
Abstract
As the coronavirus disease 2019 (COVID-19) epidemic spreads around the world, the demand for imaging examinations increases accordingly. The value of conventional chest radiography (CCR) remains unclear. In this study, we aimed to investigate the diagnostic value of CCR in the detection of COVID-19 through a comparative analysis of CCR and CT. This study included 49 patients with 52 CT images and chest radiographs of pathogen-confirmed COVID-19 cases and COVID-19-suspected cases that were found to be negative (non-COVID-19). The performance of CCR in detecting COVID-19 was compared to CT imaging. The major signatures that allowed for differentiation between COVID-19 and non-COVID-19 cases were also evaluated. Approximately 75% (39/52) of images had positive findings on the chest x-ray examinations, while 80.7% (42/52) had positive chest CT scans. The COVID-19 group accounted for 88.4% (23/26) of positive chest X-ray examinations and 96.1% (25/26) of positive chest CT scans. The sensitivity, specificity, and accuracy of CCR for abnormal shadows were 88%, 80%, and 87%, respectively, for all patients. For the COVID-19 group, the accuracy of CCR was 92%. The primary signature on CCR was flocculent shadows in both groups. The shadows were primarily in the bi-pulmonary, which was significantly different from non-COVID-19 patients (p = 0.008). The major CT finding of COVID-19 patients was ground-glass opacities in both lungs, while in non-COVID-19 patients, consolidations combined with ground-glass opacities were more common in one lung than both lungs (p = 0.0001). CCR showed excellent performance in detecting abnormal shadows in patients with confirmed COVID-19. However, it has limited value in differentiating COVID-19 patients from non-COVID-19 patients. Through the typical epidemiological history, laboratory examinations, and clinical symptoms, combined with the distributive characteristics of shadows, CCR may be useful to identify patients with possible COVID-19. This will allow for the rapid identification and quarantine of patients.
Introduction
On December 31, 2019, several patients with idiopathic pneumonia were hospitalized in Wuhan, Hubei Province, China. The disease quickly spread throughout the entire country. It was on February 12, 2020, when the World Health Organization (WHO) officially named the virus as coronavirus disease 2019 (COVID-19), and named the pneumonia caused by the virus as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). The virus is believed to have originated from a wet market in Wuhan, yet additional studies are needed to verify this hypothesis. 1 As COVID-19 aggressively spread throughout China, researchers confirmed the virus exhibited human-to-human transmission. 2 It was only weeks before COVID-19 was declared a global endemic.3,4
According to the latest guidelines from the National Health Commission, the definite diagnosis of COVID-19 is primarily through high-throughput sequencing or real-time reverse-transcriptase polymerase-chain-reaction (RT-PCR) testing of respiratory specimens. 5 However, nucleic acid detection methods are timely and dependent on the availability of specialized test kits and reagents, making this approach suboptimal in emergent situations. More importantly, the accuracy of these diagnostic approaches relies on the stage of the disease (i.e. patients with low viral loads may be undetectable) and the successful extraction of the specimen from the patient. Considering these inherent limitations, the current detection rates of COVID-19 by RT-PCR ranges from 30% to 71%.6–8
Diagnostic imaging is a major tool used in the clinic for the detection of pulmonary diseases. Several studies have reported the value of chest computed tomography (CT) in the diagnosis of SARS-CoV-2. Ground-glass opacities, solid lesions, interstitial changes, and subpleural distribution suggest that SARS-CoV-2 has a certain specificity.9–11 Conventional chest radiography (CCR) is the most widely available, rapid, and popular imaging tool for the detection of pulmonary inflammatory diseases.12,13 However, there is limited information about the value of CCR in diagnosing COVID-19. For this reason, in the current study, we aimed to explore the value of CCR in the early diagnosis of COVID-19 through a comparative analysis of CCR and CT.
Materials and methods
Patients
CCR and CT images of 49 patients from Honghu People’s Hospital, Southern Hospital of Southern Medical University, and Maoming People’s Hospital were retrospectively collected and analyzed. This study was approved by the institutional review committee of each participating agency, and written informed consent was waived for the study. From the 49 patients, 23 were confirmed to have COVID-19 infection through nucleic acid testing, while 26 were suspected of COVID-19 but tested negative (non-COVID-19) by nucleic acid testing. The clinical data, epidemiological characteristics, and laboratory data were collected for each patient. The time intervals of CCR and CT examinations were shorter than 48 h.
The inclusion criteria were as follows: (1) patients were diagnosed as having COVID-19 infection or non-COVID-19 infection by nucleic acid testing and clinical confirmation; (2) patients were ≥18 years old; and (3) the intervals between CCR and chest CT examinations were less than 48 h. The exclusion criteria were as follows: (1) a large amount of pneumothorax or pleural effusion that affects the observation of pulmonary lesions; (2) patients with missing clinical or laboratory data; and (3) poor quality of chest CT or CCR that could impact the observation of lesions.
A total of 49 patients were evaluated, including 23 patients (10 men and 13 women; average age, 51 ± 16 years) with COVID-19 infection. From the 23 patients, 18 had the common type of disease, one had the mild type, and two had the severe or critically severe cases. All 49 patients underwent both CCR and chest CT examinations, with an interval less than 48 h. Among these patients, three cases repeated the CCR and chest CT examinations within 4–10 days.Therefore, the study included 52 CCR and chest CT examinations.
Imaging techniques
Several systems were used for CCR examinations, including a mobile X-ray machine (DRX-Revolution) with chest X-ray frame, mobile digital radiography (XR220amx, GE), mobile X-ray machine (DRX-Ascend), digital radiography (security Angell-1600). The imaging conditions were as follows: 120 kV and 300 mA, except for the bedside machine with IP board (65 kV and 100 mA). The chest X-ray radiographs (CXRs) ranged from 1800 × 1800 to 2022 × 2022 pixels, and pixel sizes ranged from 0.1931 to 0.1943 mm.
The chest CT scans were obtained using one of these CT systems (Brilliance-64, Philips; Ingenuity, Philips; ScintCare CT16, Mingfeng; OptimaCT680, GE; Somatom Go Now, Siemens). The CT images were obtained according to the local imaging protocol.
Imaging analysis
Two radiologists (W.S.N. and Z.F.X. with 8 and 6 years of experience in chest imaging, respectively) reviewed all CCRs and CT images independently. They were blinded to the clinical data, laboratory findings, and RT-PCR results of the patients. The analysis was performed using the commercial DICOM image viewer (RadiAnt-64 bit-1.8.8), and adjustment of the windowing pan was allowed. They reviewed the CCR before the chest CT image, and they were not allowed to change the results of the CCR after reviewing the CT image.
While reviewing the CCRs, the observers were asked to locate the abnormal shadow and mark its location. For each image, the observers scored the likelihood of abnormal shadow of each lung on a continuous scale (1–5), with the following ratings: 1, very low likelihood of abnormal shadow; 2, low likelihood of abnormal shadow; 3, moderate likelihood of abnormal shadow; 4, high likelihood of abnormal shadow; 5, confirmed abnormal shadow. The location of each abnormal shadow was divided into upper, middle, and lower lung fields. Next, the nature of the abnormal shadows was evaluated, including solid lesions, flocculent shadows, reticular changes, and cord-like shadows.
While reviewing the CT image, the two radiologists independently evaluated the signs of lesions on each side of the CT image. The main observations included ground-glass opacities, solid lesions, and ground-glass opacities combined with solid lesions. Simultaneously, the readers evaluated the distribution of lesions and pulmonary lobe localization. The distribution included diffuse or localized distribution, and localized distribution, including subpleural or non-subpleural distribution. The two radiologists reviewed the images independently, and they reached an agreement via consensus for any disagreement.
Statistical analysis
The statistical analysis was performed using R-software version 3.3.6 (www.r-project.org). Using the chest CT images as references, the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of abnormal shadow detection were calculated for the chest X-rays. A true-positive finding was defined as a lesion correctly assessed as having abnormal shadows, with a confidence score 4 or 5. A true-negative finding was defined as abnormal shadows with a detection confidence score of 1 or 2 or indeterminate (confidence score 3). Categorical variables were expressed as number (%), and the Chi-square test or Fisher’s exact test were used for inter-group comparisons with RT-PCR results as a reference. p-Values <0.05 were considered statistically significant.
Results
Baseline patient characteristics
A total of 49 patients were evaluated, including 23 patients (10 men and 13 women; average age, 51 ± 16 years) with COVID-19 infection. From the 23 patients, 18 showed the common type, one showed the mild type, and two showed the severe or critically severe type. There were 26 cases (15 men and 11 women; average age, 48 ± 16 years) of non-COVID-19 infection. From a total of 49 patients, 38 had a history of contact with confirmed personnel or resided within an epidemic area, while 11 patients had no related history. Of the 38 patients, there were 19 cases with related history in the COVID-19 group and 19 cases in non-COVID-19 group. The patients in the COVID-19 and the non-COVID-19 group infection often experienced the following symptoms, including fever, cough, sputum, fatigue, dyspnea, or shortness of breath.
In the laboratory tests, 91.3% of cases (21/23) exhibited normal or decreased leukocytes, 39.1% of cases (9/23) had decreased lymphocytes, and 73.9% of cases (17/23) had elevated C-reactive protein in the COVID-19 group. The non-COVID-19 group showed normal or decreased leukocytes in 77% of cases (20/26), decreased lymphocytes in 38.4% of cases (10/26), and increased C-reactive protein in 65.4% of cases (17/26). No significant differences in age, sex, age, history of exposure, leukocyte, neutrophil, lymphocyte, or C-reactive protein, were identified. The details of all above information were shown in Table 1.
Patient demographics and baseline characteristics.

CRP: C-reactive protein.
Diagnostic performance of abnormal shadows detected by CCRs
Two radiologists performed 105 separate scores (52 × 2 + 1, with two independent abnormal shadows found in one lung), of which 64.7% scored ≥4 (68/105), and 35.3% scored ≤3 (37/105). In the corresponding chest CT images, 73.3% lesions (77/105) were positive, 26.7% lesions (28/105) were negative, of which 37 lesions were ground-glass opacities, 27 lesions were ground-glass opacities combined with consolidation, and 11 lesions were consolidations alone. For each abnormal shadow on CT images, 12 abnormal shadows were false negatives not detected on CCRs (Figure 1), and 65 were true positives (Figure 2). The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of CCRs to detect abnormal shadows were 84%, 89%, 96%, 68%, and 87%, respectively.

Chest radiography and CT images of a 35-year-old man with fever and cough. The patient was found to be positive for SARS-CoV-2 by RT-PCR on February 1, 2020: (a) the radiograph obtained on January 23, 2020, is negative and (b) the CT images on January 24, 2020, showed consolidation in the lower lobe of the right lung near the diaphragm.
Chest radiography and CT images of a 43-year-old man who presented with a fever. The patient was found to be positive for SARS-CoV-2 by RT-PCR on February 7, 2020: (a–b) the radiograph shows a flocculent shadow in the middle field of the left lung and (c–d) the CT images on January 31, 2020, show ground-glass opacity in the upper lobe of the left lung.
Thirty-nine showed positive findings on CCRs, while 13 were negative. However, 42 chest CT images showed positive, and 10 were negative. The CCR achieved a sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of 88%, 80%, 95%, 62%, and 87%, respectively. In the COVID-19 group, 23 were positive on CCRs (Figures 3 and 4), and 25 were positive on CT images. The CCR can achieve sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of 92%, 100%, 100%, 33%, and 92%, respectively. In the non-COVID-19 group, 16 were positive on CCRs (Figure 5), and 17 were positive on CT images. The CCR can show a sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of 82%, 78%, 88%, 70%, and 81%, respectively. All above information were shown in Table 2.

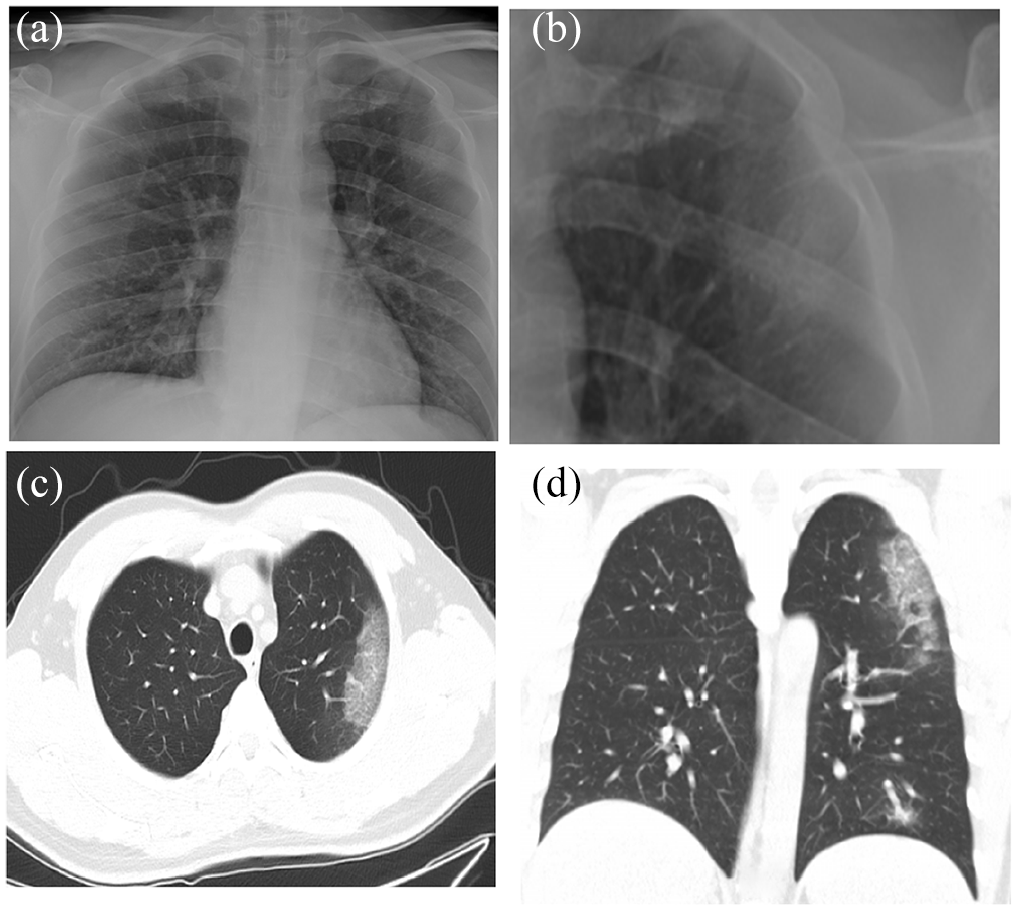
Chest radiography and CT images of a 44-year-old woman with a fever. The patient was found to be positive for SARS-CoV-2 by RT-PCR on February 6, 2020: (a–b) the radiograph obtained from January 29, 2020, showed flocculent shadows in the middle and lower field of the right lung and (c–d) CT images on January 29, 2020, showed consolidation combined with ground-glass opacity in the right lung and small ground-glass opacity in the left lung, which is negative on the radiograph.
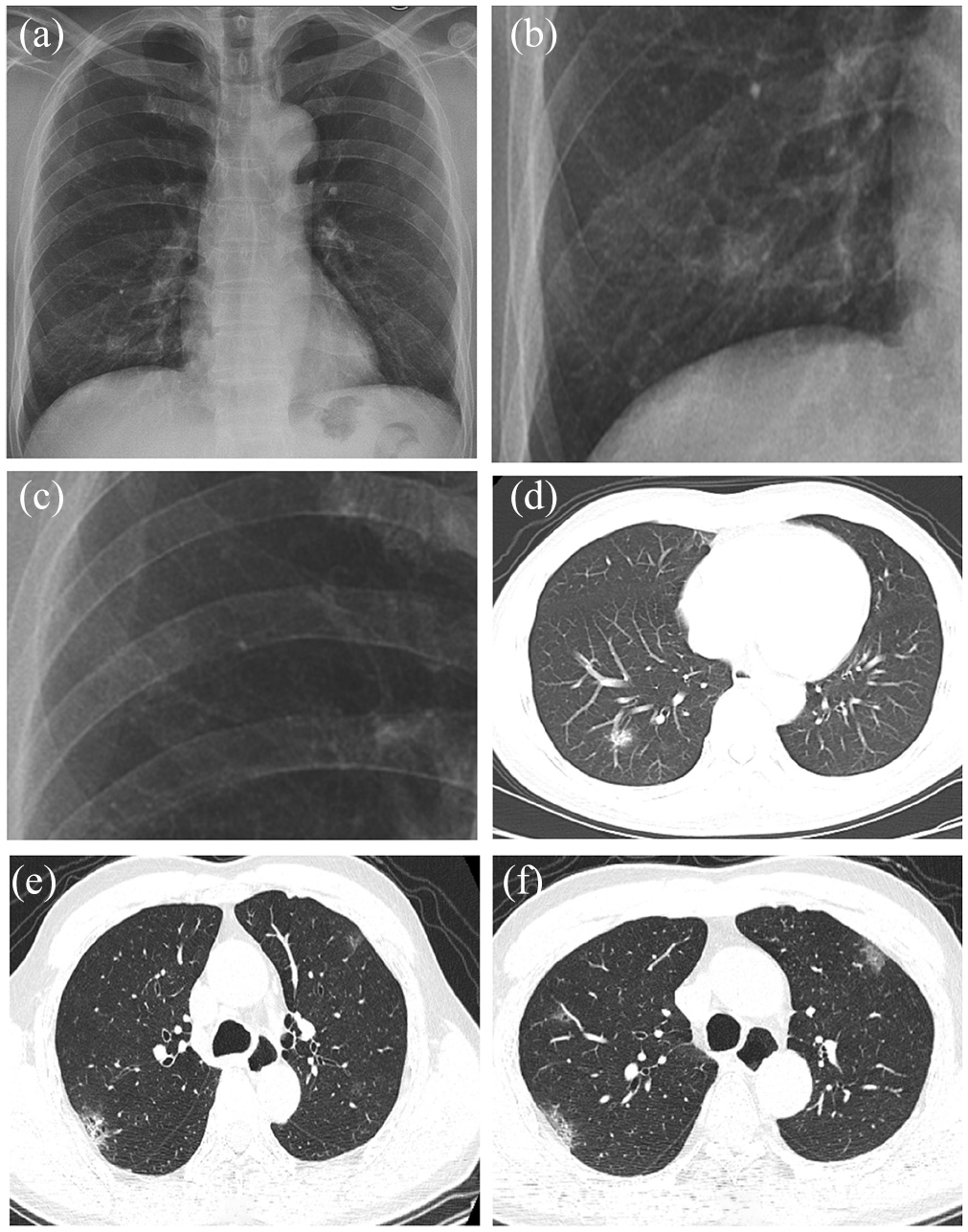
Chest radiography and CT images of a 60-year-old man with a fever. The patient was found to be positive for SARS-CoV-2 by RT-PCR on February 1, 2020: (a–c) the radiography obtained from January 23, 2020, showed flocculent shadows in the upper field rated as 4 and lower field rated as 5 of the right lung. However, the left lung was negative and rated as 1 and (d–f) the CT images on the same day showed consolidation combined with ground-glass opacity in the right lung and small ground-glass opacity in the upper lobe of the left lung.

Chest radiography and CT images of a 30-year-old woman with cough and expectoration of phlegm. The patient was found to be negative for SARS-CoV-2 by RT-PCR: (a–b) the radiograph showed flocculent shadows in the middle and lower field of the left lung, but the right lung was negative and (c–d) the CT images on the same day showed consolidation in the left lung and small ground-glass opacity and consolidation with a scattered distribution in the right lung.
Diagnostic performance of chest X-ray with chest CT as the standard of reference.
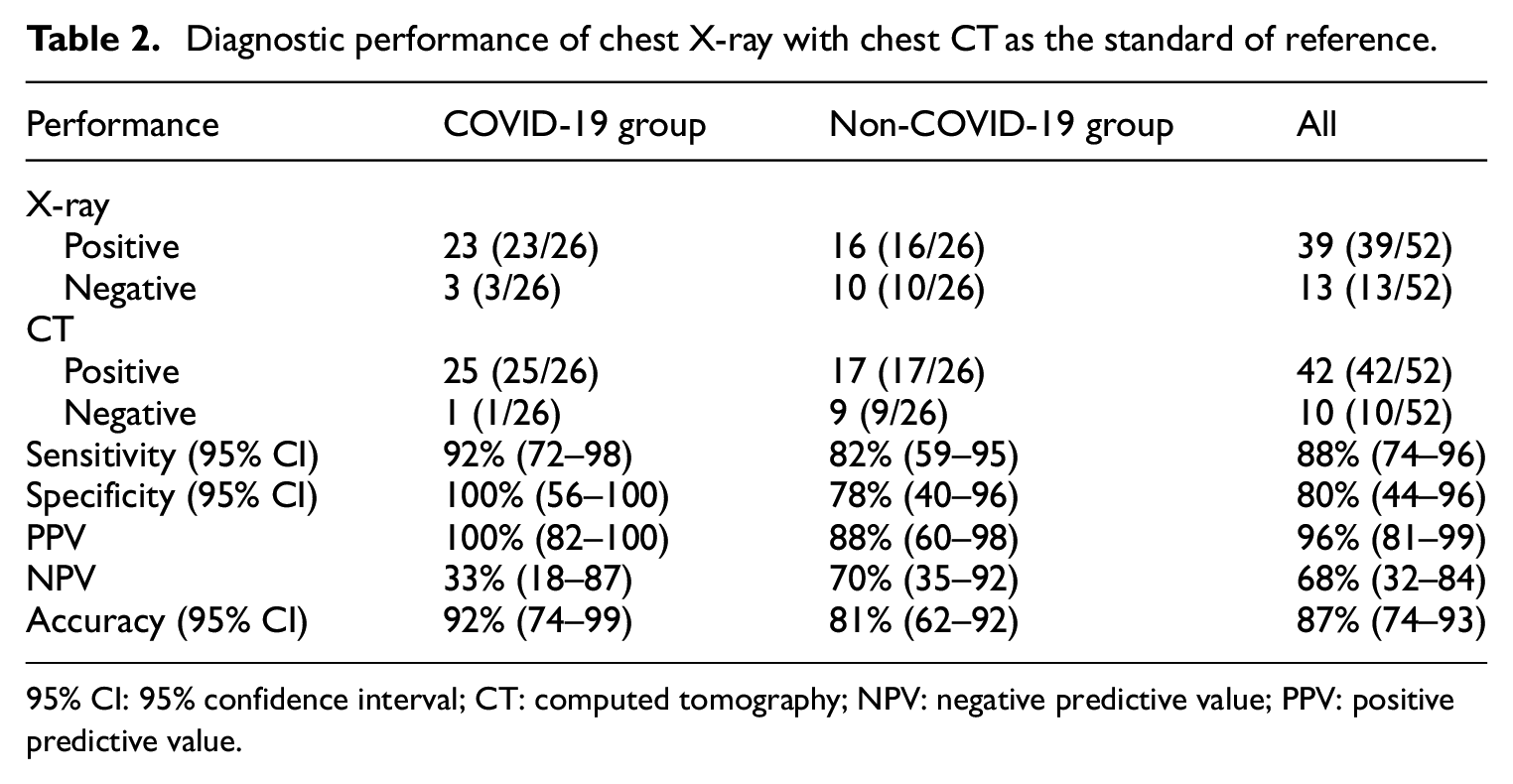
95% CI: 95% confidence interval; CT: computed tomography; NPV: negative predictive value; PPV: positive predictive value.
Comparative analysis findings of CCR between the COVID-19 and non-COVID-19 groups
The evaluation of abnormal shadows showed that 88.5% of CCRs (23/26) in COVID-19 group showed positive characteristics, of which 7 showed consolidation lesions, 20 showed flocculent shadows, 1 showed reticulated shadows, and 4 showed strip shadows. In the non-COVID-19 group, 16 CCRs showed positive findings, such as solid lesions, floppy shadows, net-like shadows, and stripe shadows with 6 cases, 13 cases, 3 cases, and 3 cases, respectively. There were no significant differences in the natures of these lesions.
Most CCRs (19/23) with COVID-19 showed bilateral lung involvement. In the non-COVID-19 group, the focus was primarily in the bilateral lung or single lung with 62.5% CT images (10/16) and 37.5% CT images (6/16), respectively. The difference was statistically significant (p = 0.03). Among the abnormal findings on CCR, 56.5% (13/23) CCRs in the COVID-19 group showed abnormal finding involving both the upper, middle, and lower lung fields, while 31.2% (5/16) in the non-COVID-19 group showed both upper, middle, and lower lung fields, and the difference was statistically significant (p = 0.008). All above information were shown in Table 3.
Comparison of radiological findings between the COVID-19 and non-COVID-19 groups.

CT: computed tomography.
Comparative analysis of CT findings between the COVID-19 and non-COVID-19 groups
There were 25 chest CT images were positive in the COVID-19 group, while 17 were positive in the non-COVID-19 group. The most common CT findings (13/25, 52%) in the COVID-19 group were multiple subpleural ground-glass opacities. In the non-COVID-19 group, the main lesions (7/17, 41.2%) were ground-glass opacities with consolidations. The difference was statistically significant (p = 0.002). In the COVID-19 group, most of the lesions (23/25, 92%) were involved in both of the lungs, and the whole lung lobe was most involved in most images (p = 0.0001). Also, the distribution of the lesions was peripherally (60% vs 47%, p = 0.01). In the non-COVID-19 group, bilateral and single lung involvement were more common with nine cases (9/17, 52.9%) and eight cases (8/17, 47.1%), respectively. The difference was statistically significant (p = 0.001). All above information were shown in Table 3.
Discussion
Due to the rapid and global spread of COVID-19, methods for the early detection, diagnosis, and isolation are of critical importance in the control of the virus. As there are several limitations to current nucleic acid-based laboratory tests, diagnostic imaging has become an important tool for the early diagnosis of COVID-19. The diagnostic value of chest CT has been confirmed in several studies.14–16 However, the value of CCR in the early detection of COVID-19 remains unclear. As chest CT is the current “gold standard,” we aimed to explore the diagnostic value of CCR in COVID-19 in the current study.
CCR is considered to be the most common diagnostic tool for detecting abnormal shadows due to its wide accessibility, low cost, and low radiation dose.17,18 However, due to the limited contrast of soft tissues, CCR is rarely used in the early diagnosis and screening of COVID-19. In this study, we found that the sensitivity, specificity, and accuracy of chest X-rays for detecting abnormal shadow of the lung were 84%, 89%, and 87%, respectively. In the 12 false-negatives on CCRs, 3 lesions were solid, 4 were ground-glass opacity, and 5 were ground-glass opacity combined with consolidations on chest CT images. Nine shadows could not be shown on CCRs because the focus lesions on the chest CT images were too small or the density was too weak. The rest could not be displayed because of their overlap with the heart shadow or diaphragm. In conclusion, CCRs have shown good diagnostic performance in detecting abnormal shadows. However, as reported in previous studies, CCR were restricted by various factors, such as the size and density of the lesions and the overlap between the lesions and soft tissue. For this reason, CCRs are subject to a certain degree of false negatives.17–19
In the clinical, as long as the abnormal shadow is found on the CCR, it is possible to diagnose the positive case. In the COVID-19 group, the sensitivity, specificity, and accuracy of chest X-rays in the positive cases were 92%, 100%, and 92%, respectively. Only two cases were found to be false negatives.
Our study enrolled two patient groups, including those diagnosed with pathogen-confirmed COVID-19 group and the non-COVID-19 group. These are consistent with the common epidemiological characteristics, clinical symptoms, and routine tests in patients with COVID-19. There was no significant difference in age, sex, epidemiological history, clinical symptoms, or laboratory results between the two groups, which made it difficult to differentiate between the two groups. Most of the cases in the two groups showed flocculent shadows on CCRs, followed by consolidations, which had no significant significance in the differential diagnosis. In terms of the distribution, the lesions in the COVID-19 patients primarily involved both lungs, while non-COVID-19 patients experienced involvement of one or both lungs. Moreover, in the COVID-19 group, the lesions involved the upper, middle, and lower lung fields at the same time. In addition, the changes in the middle and lower lung fields were more evident. The distribution characteristics of the lesions are consistent with COVID-19 patients reported in most studies, with multiple lesions in both lungs, but the changes in the lower lungs are the most obvious.15,16,20
In addition, our study further confirmed the diagnostic value of chest CT in both groups of patients. Our results showed that the primary signs of chest CT in the COVID-19 group were ground-glass opacities, mainly in both lungs, with a wide range of lesions. In the non-COVID-19 group, the involvement of one and both lungs were more common, primarily manifested as solid lesions combined with ground-glass opacities.
Chest CT imaging is a convenient, non-invasive modality with high accuracy. In the epidemic areas, CT can be used as a routine modality for suspected patients, and even as a screening tool in the general population to detect and isolate suspicious patients. However, the use of CT for COVID-19 screening can be costly and expose people to unnecessary doses of radiation. The radiation dose of standard chest CT is about 4.7 mSv, and a single CT scan produces a cancer risk of approximately 0.05%. For patients who undergo multiple CT scans, the risk may be as high as 2.7%. However, the radiation dose of the chest X-ray is about 0.05 mSv, which is only 1/80–1/140 of the radiation dose of chest CT.21,22 Regarding the target population of COVID-19 is all over the world, it is impossible to perform CT as a screening tool, which may lead to overuse of CT and unnecessary irradiation of healthy people. 23 In addition, for some lower-level medical institutions, not equipped with CT scanners, chest X-ray examinations may help screen suspicious patients.
There are some limitations to our study: (1) First, the detection performance of normal shadows is limited as we lack a “gold standard.” We only have a reference standard, which was represented by the chest CT images within 48 h and the consensus readings by the radiologists. (2) The number of cases diagnosed with COVID-19 by both CCRs and CT images within 48 h was insufficient, the early diagnostic value of CCR in COVID-19 needs to be further investigated in larger patient populations. (3) The non-COVID-19 group had patients with other types of viral and bacterial infections that could interfere with the differential diagnosis. However, we strongly encourage future studies to assess the potential value of CCR in COVID-19, ideally with multiple radiologists of various expertise levels and more cases so that meaningful variability can be obtained and reported.
In conclusion, the detection of inflammatory lesions on chest X-ray examinations in patients with COVID-19 showed good sensitivity, specificity, and accuracy, and has a certain value for screening patients. However, its importance in differentiating COVID-19 patients from non-COVID-19 patients is limited. Through the typical epidemiological history, laboratory examinations, and clinical symptoms, combined with the distribution characteristics of shadows, X-rays examinations allow for the rapid identification of possible COVID-19 cases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by National Key R&D Projects (No. 2019YFC0121903), High-level Hospital Construction Research Project of Maoming People’s Hospital (Yueweihan (2018) 413).
Data availability
Some or all data, models, or code generated or used during the study are proprietary or confidential in nature and may only be provided with restrictions.