
Abstract
Objective:
To investigate the correlation between placental characteristics and the onset of selective intrauterine growth restriction (sIUGR) and to explore the influence of placental characteristics on sIUGR onset.
Methods:
A retrospective cohort study was conducted at our hospital from April 2013 to April 2019. The pregnancy data and placental perfusion of 114 sIUGR patients who had received conservative treatment and delivered in our hospital were included. Correlation analysis was conducted between the total diameter of placental anastomoses, placental territory discordance, umbilical cord insertion point distance ratio, and the onset time of sIUGR.
Results:
The prevalence of AA anastomoses was 88.6% (101/114), with an average total diameter of 2.8 ± 1.5 mm, the prevalence of AV anastomoses was 93.9% (107/114), with an average diameter of 5.4 ± 3.6 mm, and the prevalence of VV anastomoses was 18.4% (21/114), with an average diameter of 4.0 ± 1.9 mm. There was a significant negative correlation between the time of sIUGR onset and the placental territory discordance ratio with a Spearman correlation coefficient of −0.306 (P = 0.001).
Conclusions:
The larger the placental territory discordance, the earlier onset time of sIUGR.
Keywords
Introduction
Selective intrauterine growth restriction (sIUGR) in monochorionic diamniotic (MCDA) twin pregnancies is complicated with an incidence of 10–26%.1,2 The current understanding of sIUGR is that it arises when the monochorionic diamniotic twin pair share one placenta and the allocation of placental sharing between the two fetuses is unequal. Marginal and velamentous insertion of the umbilical cord may also cause unequal nutritional supply to the fetuses and sIUGR.1,3–5 The placenta of MCDA pregnancy has unique vascular anastomoses between the twin pairs. Previous studies have demonstrated that these placental anastomoses could affect the progression and prognosis of sIUGR. 6 Lewi et al. 7 found in a study with 28 sIUGR placental samples that if sIUGR occurred before 20 gestational weeks, the placental share discordance was greater than when sIUGR occurred after the 26th gestational week. However, their sample size was insufficient and they simply compared the difference between the two groups without conducting a correlation analysis based on the sIUGR onset time and placental characteristics. So, the relationship between the sIUGR onset time and placental characteristics is unclear. We conduct this study to explore the relationships between placental superficial anastomoses, placental share discordance, umbilical cord insertion, and the time of sIUGR onset.
Methods
In this retrospective cohort study, we included sIUGR patients with monochorionic diamniotic twin pregnancy after live birth of both twins at our center from April 1, 2013, to April 1, 2019. Patients with twin-to-twin transfusion syndrome, twin anemia polycythemia sequence, fetal reduction, fetal demise during pregnancy were excluded, ruptured placentas after delivery that could not be perfused completely with dye were also excluded. The study was approved by the Ethics Committee of this hospital and placentas were collected after informed consent from patients.
All the MCDA pregnancies were followed up every two weeks since 16 weeks of gestational age in our center. sIUGR was diagnosed in monochorionic diamniotic twin pregnancies where the ultrasound-estimated weight of any fetus was less than the 10th percentile of weights in the corresponding gestational age, and the other fetus present normal growth, cases with both fetuses < 10th centile were excluded. 1 The classification criteria were based on the Doppler status of the umbilical arterial blood flow to the smaller fetus, with the following three classifications 8 : Classification I: the end-diastolic spectrum of umbilical arterial blood flow was positive. Classification II: there was persistently absent or reversed end-diastolic blood flow in the umbilical artery. Classification III: the presence of intermittently absent or reversed end-diastolic blood flow in the umbilical artery. TTTS was diagnosed based on the combined presence of a maximum vertical pocket (MVP) of ≥8 cm in one sac and ≤2 cm in the other before 20 weeks and a MVP of ≥10 cm in one sac and ≤2 cm in the other after 20 weeks. 9 Antenatal twin anemia polythemia sequence (TAPS) diagnosis was based on the discordant measurements of the middle cerebral artery peak systolic velocity (MCA-PSV) being greater than 1.5 the multiples of the median [MoM] in donors, and less than 1.0 in recipients, or wiht a Delta MCA-PSV > 0.5 MoM. 10
The gestational age at first diagnosis of sIUGR, and classification status were recorded, as were the treatments and prognoses of patients during the pregnancy. Gestational age was confirmed by last menstrual period and with ultrasound measurement of crown-rump length at the first trimester.
This hospital conducted routine examinations of the placentas of the monochorionic diamniotic twin pairs after delivery to verify the chorionic diagnosis. Placentas without a confirmed chorionic diagnosis were sent for pathological examination. All complete placentas of monochorionic diamniotic twin pairs were perfused with dye (white, green, red and yellow) to determine placental superficial vascular anastomoses, placental share, and umbilical cord insertion, and digital photographs were kept for subsequent data analysis (Figure 1). The type, extent, and diameter of each placental anastomosis were recorded. The distance between the umbilical cord insertion points was measured between the centers of the two umbilical cord insertion sites, as for velamentous umbilical cords, the margin of the adjacent placental parenchyma was chosen as the center of the insertion point. The longest diameter of the placenta was the maximum distance towards the placental margin. The umbilical cord insertion point distance ratio was defined as the ratio between the umbilical cord insertion point distance to the longest diameter of the placenta. The placental sharing of the two fetuses was determined according to the intersection of anastomoses, and the area of the shared placenta was measured for each fetus. The placental territory discordance ratio = (the larger placental area - the smaller placental area)/the larger placental area.

Image of the placenta after the injection of dyes. (Blue arrow, AA anastomosis; Red arrow, AV anastomosis; Black curve, vascular equator.).
The SPSS statistical analysis software package (Version 24.0; IBM Corp, Armonk, NY, USA) was used for statistical processing. The measurement data fitting the normal distribution were described as mean ± standard deviation, while data not fitting the normal distribution were described by the median (maximum, minimum). Spearman rank correlation analysis was used for non-normally distributed data. A Scatter plot was used to descript the association between placental territory discordance, umbilical insertion ratio, AV diameter and the gestational age of TTTS diagnosis respectively. Spearman's rank correlation coefficients for them were calculated. For the reason that some placentas of sIUGR have no AA or VV anastomoses, a probability density curve was used to present the probability density distribution of the gestational age of TTTS diagnosis in the groups with and without AA or VV anastomoses. Mann-Whitney U tests were used to compare the gestational age median of TTTS diagnosis between the two groups. A two-tailed probability value of P < 0.05 represented statistical significance.
Results
A total of 217 sIUGR patients with monochorionic diamniotic twin pregnancy, admitted to the Obstetrics Department of Peking University Third Hospital between April 2013 and April 2019, were retrospectively analyzed. We excluded 20 patients who were diagnosed as sIUGR complicated with TTTS, 9 patients who were diagnosed as TAPS, 41 patients who chose fetal reduction, and 31 patients who suffered fetal demise during pregnancy. We also excluded 2 placentas that were too fragmented to allow effective perfusion. The remaining 114 placentas with complete dye injection were the final sample of the study (Figure 2).
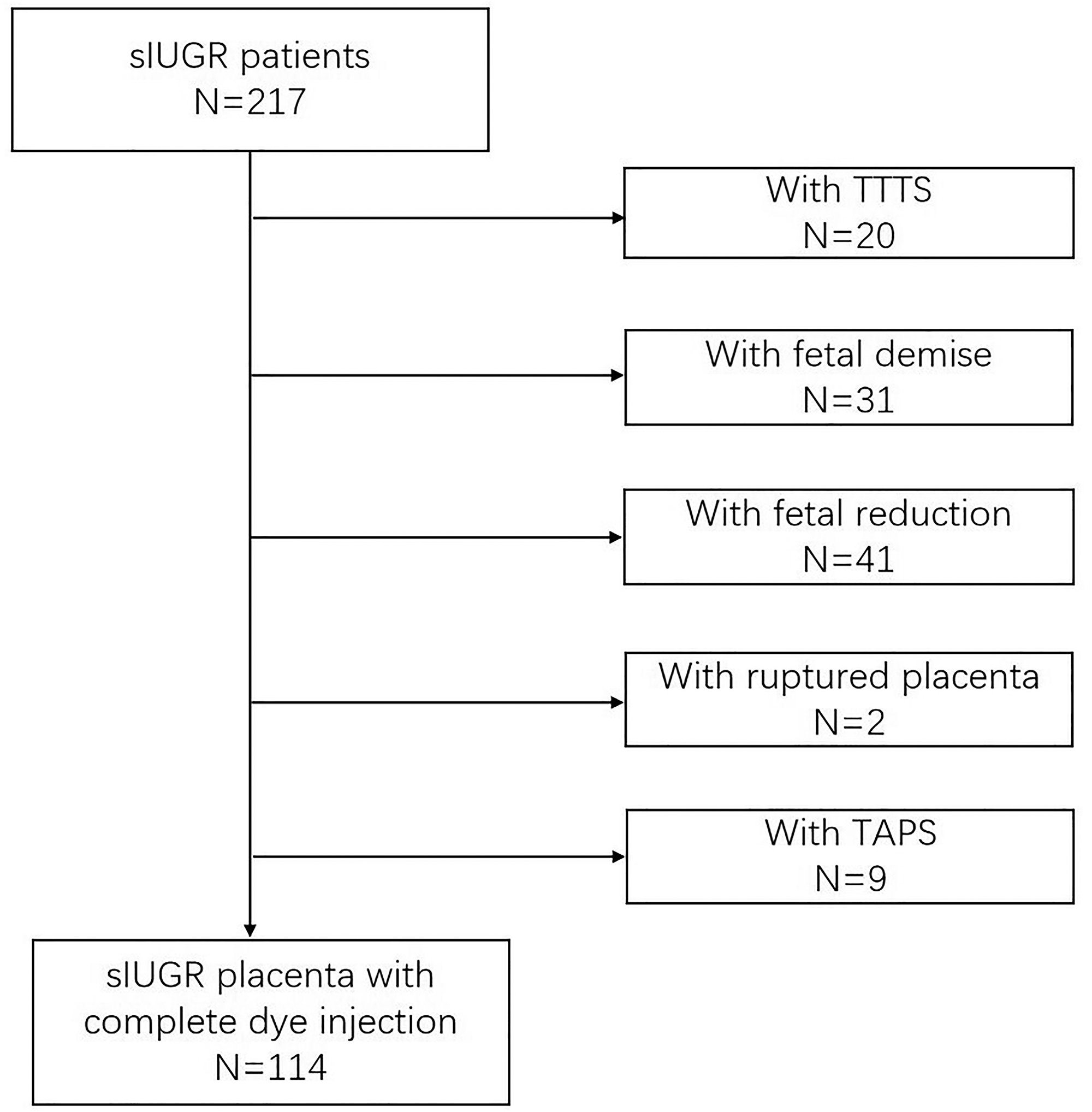
Flowchart of placentas included in the study (sIUGR: selective intrauterine growth restriction, TTTS: twin to twin transfusion syndrome, TAPS: twin anemia polythemia sequence).
The median age of all patients was 29 (20,41) years old. There were 53 patients that were confirmed as sIUGR type I, 37 patients as sIUGR type II, and 24 patients as sIUGR type III. The median gestational age at first diagnosis of sIUGR was 23.7 (16.9,36.3) weeks, the distribution of gestational age at first diagnosis of sIUGR was shown in Figure 3(a). The average delivery time was 33.2 ± 2.1 weeks. A total of 218 infants were born alive. Fetuses with normal development had an average weight of 2095 ± 517 g while growth-restricted fetuses had an average weight of 1451 ± 488 g.

Distribution of gestational age at first diagnosis of sIUGR and its correlation with placental characteristics.
Spearman correlation analysis of every indicator of placentas is presented in Table 1. Among the 114 placentas, the prevalence of artery to artery (AA) anastomoses was 88.6% (101/114) with an average total diameter of 2.8 ± 1.5 mm, the prevalence of artery to vein (AV) anastomoses was 93.9% (107/114) with an average total diameter of 5.4 ± 3.6 mm, and the prevalence of vein to vein (VV) anastomoses was 18.4% (21/114) with an average total diameter of 4.0 ± 1.9 mm. The umbilical cord insertion distance ratio was 0.57 ± 0.23 and the placental territory discordance ratio was 0.60 ± 0.12.
Spearman rank correlation coefficients between placental characteristics.

Correlation analysis of the gestational age of the first diagnosis of sIUGR and placental characteristics is shown in Figure 3. As can be seen, the gestational age of the first diagnosis of sIUGR was negatively correlated with the placental territory discordance ratio with a Spearman correlation coefficient = -0.306(P = 0.001) (Figure 3(b)). There was no significant correlation between umbilical cord insertion ratio, AA, AV, VV anastomoses and the gestational age of the first diagnosis of sIUGR (Figure 3c,d,e,f).
Discussion
The present study showed that the placental territory discordance is negatively correlated with the gestational age of the first diagnosis of sIUGR, which means the larger the placental territory discordance in MCDA pregnancies, the earlier sIUGR onset. The finding seems to provide some ideas for earlier prediction and intervention of sIUGR.
sIUGR is characterized by unequal placental sharing with the marginal or velamentous insertion of the umbilical cord. 11 Various studies have demonstrated that the greater the inequality of placental sharing, the greater the difference in the birth weights of the two fetuses.3,4,12,13 Additionally, uneven allocation of placental share is often accompanied by the abnormal insertion of the umbilical cord,14,15 which all could cause insufficient supplies of nutrients and oxygen required by the fetuses during development, leading to intrauterine growth restriction. However, relevant studies are lacking on whether the uneven placental allocation influences the onset time of sIUGR. The present study showed a negative correlation between the gestational age of the first diagnosis of sIUGR and the placental territory discordance ratio (r = -0.336, P < 0.001). These results show that the larger the placental territory discordance between two fetuses, the earlier the onset of sIUGR probably, consistent with the findings of Lewi et al. early-onset sIUGR is a consequence of a greater placental territory discordance. More importantly, it was also found that this is a continuous linear relationship. In other words, the larger the placental territory discordance, the earlier the onset time of sIUGR. This result reveals that the ultrasound examination should become more frequent in order to diagnose sIUGR earlier if we could identify larger discordance in placental sharing in MCDA in the future.,
Vascular anastomoses are seen on most placentas of MCDA twin pregnancy, with two-way blood flow in the A-A and V-V anastomoses. The direction of the blood flow can be adjusted based on the hemodynamic pressure between fetuses. A-V anastomoses occur deep in the placenta, with blood flow in a single direction in the capillaries below the placental chorionic plate arteries. Currently, it is thought that A-A anastomoses could compensate for the imbalance in blood flow caused by A-V anastomoses, thus protecting monochorionic diamniotic twin pregnancies.16,17 The prevalence of V-V anastomoses is small, and their role is unclear. It is possible that they may be associated with a decreased survival rate of perinatal infants as the sudden venous reflux may lead to intrauterine fetal death. 17 Two fetuses can exchange blood with each other by these anastomoses. The bigger fetus with sufficient blood supply could transfuse blood in a protective way to the smaller fetus in need of blood so that the impact of insufficient placental sharing on the smaller fetus can be reduced. Hence, whether anastomoses influence the onset time of sIUGR is unknown. Theoretically, larger total anastomosis diameters are associated with larger volumes of exchanged blood, suggesting that greater compensation of blood nutrients and oxygen from the bigger fetus to the smaller one could delay the onset of sIUGR. Lewi et al. in their study of 28 early- and late-onset sIUGR placentas, 7 observed significant differences in the total diameter of AA anastomoses (3.66 ± 1.83 and 1.34 ± 1.15 mm for early- and late-onset sIUGR, respectively, P < 0.01) and the total diameter of anastomoses (13.97 ± 7.07 and 5.83 ± 5.24 mm, respectively, P = 0.01), indicating that both values were larger in the early-onset placentas, contrary to the theoretical speculation. De Paepe et al. 3 reported a study of 36 sIUGR placentas and found that there was no difference in the diameters of placental superficial vascular anastomoses in placentas with and without sIUGR. Hence, they speculated that placental anastomoses were not involved in the pathogenesis of sIUGR. In the present study, no correlation was found between the total diameters of VV, AA, and AV anastomoses and the total diameter of anastomoses in each placenta and the gestational age of the first diagnosis of sIUGR. Hence, although anastomoses were certainly relevant with the different classifications of sIUGR, 9 it is deduced that anastomoses may have negligible effects on the onset time of sIUGR.
This study had several limitations as it was performed retrospectively, since sIUGR can only be diagnosed by ultrasound, the time of initial ultrasound diagnosis cannot absolutely represent the onset time. Although we found a few statistically significant correlations between the gestational age of the first diagnosis of sIUGR and the placental territory discordance ratio, the correlations (Spearman's rank) are relatively weak, so the conclusion should be treated with caution. It is hoped that this preliminary result will lay the foundation for future research.
Conclusion
In conclusion, we found that the larger the placental territory discordance, the earlier the onset time of sIUGR.
Footnotes
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
This work was funded by grants from the National Key Research and Development Program of China (2018YFC1002900).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent to participate
All patients signed informed consent before participation.
Consent for publication
All authors provide formal written consent to publish before publication of the work.
Author contribution
All authors contributed to the study conception and design. Study design and project development were performed by Yuan Wei and Xueju Wang. Material preparation, data collection and analysis were performed by Xueju Wang, Luyao Li, Pengbo Yuan, Yangyu Zhao and Yuan Wei. Data analysis check and consultation was performed by Huifeng Shi. The first draft of the manuscript was written by Xueju Wang and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.