
Abstract
This work is a qualitative exploratory survey that aims to identify healthcare workers and skilled professionals’ perceptions of the Food and Nutrition Surveillance System in the Zona da Mata Mineira region of Brazil. Data analysis was carried out through content analysis; testimonials were extracted from semi-structured interviews via the qualitative data processing software Interface de R pour lês Analyses Multidimensionnelles de Textes et de Questionnaires version 0.7 alpha 2. A total of 41 people were interviewed, including primary healthcare center coordinators, and technical consultants at the Food and Nutrition Surveillance System, as well as nutritionists and data entry clerks. The issues most mentioned during interviews were related to lack of anthropometric equipment, absence of transportation, and inadequate facilities. Regarding the work process, professionals identified scarce training and nonuse of the data collected for healthcare decision-making as factors that compromise desired system outcomes. System qualities were also recognized, especially the mapping of main nutritional issues in the region. The participants reported the need for greater efforts to raise awareness of the importance of Food and Nutrition Surveillance actions at all levels of the public healthcare system. They also highlighted the need for human resources training, higher quality data recording, and suitable facilities. Investments in the entire system are essential to strengthen the information–decision-making–action triad, which would result in the improvement of users' health indicators.
Keywords
Introduction
In 1990, the Healthcare Organic Law (Law n. 8080/90) officially implemented the Brazilian Food and Nutritional Surveillance (SISVAN). Currently, it is a health information system (HIS) and consolidates the data resulting from monitoring the nutritional situation and food consumption indicators of users receiving primary healthcare services of the Unified Health System (SUS).1,2 Its aim is to assist in the management of Food and Nutrition Surveillance (VAN) information, from recording to reporting, which in turn contributes to the political decision-making process that determines methods to improve health conditions. 3
SISVAN has continuously evolved – from creating more localized versions 3 to the current version, which includes an online tool that enables the communication between HIS staff to avoid staff rework and establishes an information recording integrated model. 3 It is managed by primary healthcare center (PHC) coordinators, run by front desk clerks, and powered by nutritionists who feed the system data collected by primary healthcare workers and other skilled professionals.
Healthcare workers and skilled professionals are aware that Food and Nutrition Surveillance Systems are an important asset to fight malnutrition and other nutritional problems; nevertheless, these systems are largely undeveloped in most developing countries. Reasons for this include a lack of consensus on the best methods to implement nutritional surveillance, a lack of confidence in surveillance data, and insufficient data to compare the costs of different effective systems to justify such investments. 4 These findings demonstrate a gap in understanding between monitoring nutritional status and using system information. The greatest challenges are addressing the failures of data processing and promoting the active use of information. Those responsible for SISVAN have not utilized the information to guide decision-making, and many do not recognize the importance of the collected data for guiding city management. 5 Thus, a distance remains between the system and the solution to existing nutritional problems. According to the Global Nutrition Report, 6 the national average of monitoring nutritional status is insufficient to accurately identify vulnerable groups and enable open dialog, partnerships, action, and assignment of responsibility necessary to solve most prevalent nutritional problems.
It is no different in Brazil; despite the evolution of SISVAN as a HIS, daily practices have limitations related to communication with VAN. 5 Since the initial implementation attempts in 2004, this surveillance has not always been effective in the cities. The main problems relate to the operation of the system and the use of data to elaborate actions and can generally be identified in one or more dimensions.5,7,8 In addition to poor integration and communication between government sectors, there are issues with facility infrastructure, personal training, interactivity, and system intelligence; 9 poor system coverage and representativeness;10,11 lack of integration between information systems; 12 and poor geographical and population coverage.5,10,13–15 Finally, research has shown the need for better system integration with assistance program funding 7 and the underutilization of SISVAN information by city management of SUS primary care. 5
Incorporating VAN practices into daily healthcare services does not rely only on financial resources. In fact, it depends on other aspects, such as political commitment to public health, especially by those advocating for food and nutrition actions within cities. 16 Nevertheless, this is not a current Brazilian government priority, due to political instability that could result in setbacks for social and health policies.17,18
Food and Nutrition Security comprises the realization that everyone has the right to regular and permanent access to quality food, in sufficient quantity, without compromising access to other essential needs, and is based on health-promoting food practices that respect cultural diversity and are environmentally, culturally, economically, and socially sustainable. 2
Healthcare quality relies on different elements: management, financial, and organizational devices; aspects related to the care provided; and professional capability and outcome suitability. If one element fails, the entire process may be impaired. 19 Thus, quality control assessment of information systems must consider the workers’ perceptions and preferences – what measures could improve satisfaction – with the aim of system optimization.19,20 To improve system quality, it is crucial to share experiences with Food and Nutrition Security, provide insights into what works (and does not) in real life, and identify system challenges, potentials, and perceptions. 21
This work aims to identify healthcare workers and skilled professionals’ perceptions of SISVAN performance in the Zona da Mata Mineira region of Brazil.
Methods
This is a qualitative exploratory study using semi-structured interviews for data collection, 22 one of several studies conducted as part of the project “Food and Nutritional Surveillance in the cities from the Zona da Mata Mineira region,” which has already applied three different assessment methods to evaluate SISVAN in this area. The first study analyzed the bias in the coverage of population nutritional status evaluation in cities located in this region registered on SISVAN Web from 2008 to 2017. Specifically, it mapped the correlation between socioeconomic, demographic, and healthcare system organization variables and concluded that the coverage of the nutritional status evaluation was low throughout the period under consideration. 15 In this context, given that the previous research only employed quantitative measurements, it was necessary to analyze healthcare workers’ and skilled professionals’ perceptions of SISVAN. There is currently another exploratory study in progress, which relies on a structured SISVAN evaluation process. Our study is the third attempt to assess SIVAN's efficacy in this region.
Study area location
The Brazilian Institute of Geography and Statistics (IBGE) divides Minas Gerais State into 12 mesoregions covering 66 micro-regions. The mesoregion of the Zona da Mata Mineira comprises 42 cities, with an estimated population of 2,175,254 inhabitants and a demographic density of 60.0 inhabitants/km2. It covers an area of 35,726 km2, approximately 6% of the State of Minas Gerais. This region has seven geographical micro-regions: Ponte Nova, Manhuaçu, Viçosa, Muriaé, Ubá, Juiz de Fora, and Cataguases. 23
The selected cities are healthcare references for each micro-region of the Zona da Mata Mineira, with which the research team has had a partnership for more than four years resulting in contributions to this work. A healthcare reference city serves as an appropriate representation of the population of its micro-region. Therefore, such cities are used as the base population linked to a particular territory in order to calculate the healthcare planning and network organization. This delimitation provides guided criteria as to the flow, accessibility, service provision, and clinic supply profiles, which are related to the level of technological density according to the typology initially established. 24
Participants and recruitment
To investigate the different workers and skilled professionals’ perceptions regarding VAN's performance, 41 interviews were carried out with healthcare workers and skilled professionals involved in the VAN work process, including PHC city coordinators, technical consultants, and nutritionists and data entry clerks. The interviews took place at the participants’ workplaces.
This study applied convenience sampling, which selects participants according to interest and willingness to participate. Workers and skilled professionals in contact with SISVAN were invited to participate in the study after a project presentation in which researchers explained the objectives and methods to be employed. All participants voluntarily agreed to participate in this study after signing the informed consent form.
The work team went to the aforementioned cities on prearranged dates after confirming availability via telephone. A group of experienced researchers conducted the individual interviews at a location provided by each city. All interviews were conducted in Brazilian Portuguese, the official language of Brazil, lasted approximately 60 min each.
After an analysis of the results and construction of the study, an experienced professional translator and specialist in Food and Nutritional Surveillance translated the work into English. Data collection was carried out between November 2017 and March 2018.
Conceptual framework and study tools
To evaluate healthcare workers and skilled professionals’ perceptions and understanding of the activities developed by VAN in each city, the roles played by each actor, the organization, and the execution of surveillance actions, the functionality and use of the information system, potentials, and weaknesses, as well as the intermediate and final results produced, were investigated in individual interviews. The study questions were adapted from Vitorino et al.25,26 Interviews were guided by the questions presented in .
Guiding questions of the interview to identify the healthcare workers and skilled professionals’ perceptions regarding the performance of the Food and Nutrition Surveillance System in the Zona da Mata, Mineira region of Brazil.
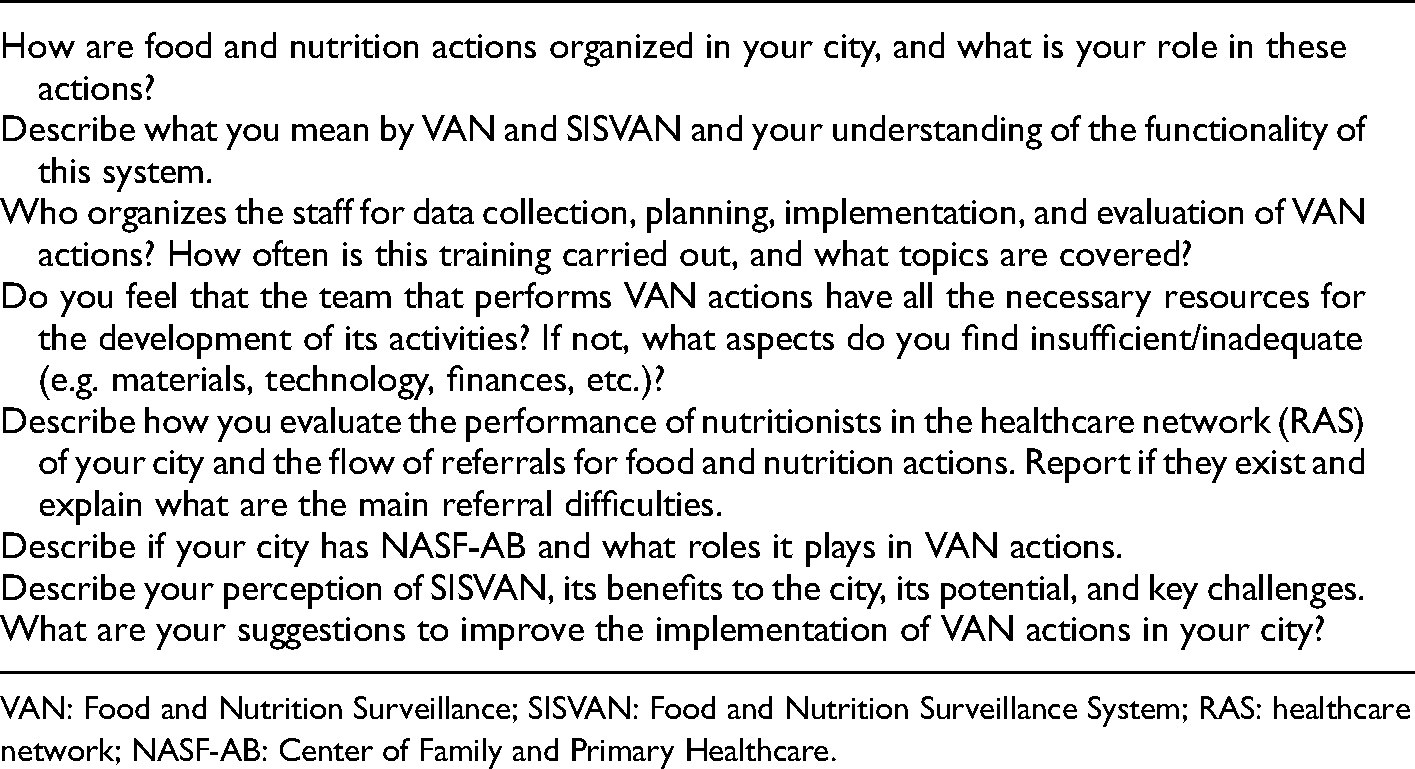
VAN: Food and Nutrition Surveillance; SISVAN: Food and Nutrition Surveillance System; RAS: healthcare network; NASF-AB: Center of Family and Primary Healthcare.
Data analysis
All interviews were recorded via Sony® digital audio equipment and later fully transcribed. Participants were referred to as P1, P2, etc. in the transcripts to preserve anonymity. The interpretive analysis of the corpus was supported by the works of Bardin 27 and Minayo, 28 through content analysis, with the support of the qualitative data analysis software Interface de R pour lês Analyses Multidimensionnelles de Textes et de Questionnaires (IRAMUTEQ) 0.7 alpha 2. IRAMUTEQ is an open-source software developed by Pierre Ratinaud,29,30 licensed by GNU general public license (v2). With this software, it is possible to carry out statistical analysis on textual corpus and charts, subjects, words. It is supported by the R software (www.r-project.org) and Python language (www.python.org).
The organization of the content analysis had three sequential steps: (1) pre-analysis; (2) exploration of the material; and (3) treatment of results, inferences, and interpretations.18,31
Credibility of the study
To ensure credibility, transcription and analysis of data were carried out by pairs of researchers. In addition, the criteria necessary to demonstrate the general quality of the research were always considered, that is, our results are not based on casuistic observations or descriptions of the obvious, or content analysis carried out without methodological clarity. The organization of content analysis followed three sequential steps: (1) pre-analytical phase; (2) exploration of the materials; and (3) treatment of results, inferences, and interpretations. The reliability of the research was ensured by the methodological criteria established for data collection and analysis. Transcripts were coded by two trained researchers. A document with the codes was developed based on the interview questions in the emerging results, which was continuously revised to ensure meaningful and consistent code definitions and definitions. An agreement was reached by discussing the initial coding and a third researcher arbitrated any differences.
Moreover, transferability was considered. This study, despite not being phenomenological, used the interview techniques of open questions and content analysis to understand and explore the perception of healthcare workers and skilled professionals. We believe that in countries with health and information systems similar to Brazil, studies like this one can assist in the analysis of the system and promote the development of more efficient and effective actions and policies on food, nutrition, and health.
Finally, the researchers considered the confirmability, that is, whether the results of the study are compatible with the results of the larger project in the same region entitled: “Evaluation of the Food and Nutrition Surveillance System in the Region of Zona da Mata in Minas Gerais.”
Ethical principles
This study was guided by the Declaration of Helsinki. Accordingly, all procedures with human beings/patients were approved by the Committee on Ethics in Research with Human Beings of the Federal University of Viçosa. This work respects ethical principles according to Resolution 466/12 of the National Health Council, and it was approved under Opinion 2.370 on November 8, 2017. Verbal consent was requested and formally registered for all interviewees.
Patient and public involvement
No patients were involved in this study.
The research group is in the process of preparing reports with the results to be presented at a conference for workers and skilled professionals from the Zona da Mata region.
Results
Table 1 summarizes the characteristics of the 41 research participants. Of these, 36 (57.1%) were female. Among those interviewed, the nutritionists had the highest education level: 5 (22.7%) had a master's degree. The mean age was 40 ± 10 years for females and 35 ± 5 years for males.
Characteristics of the research participants in Zona da Mata, Minas Gerais region of Brazil.
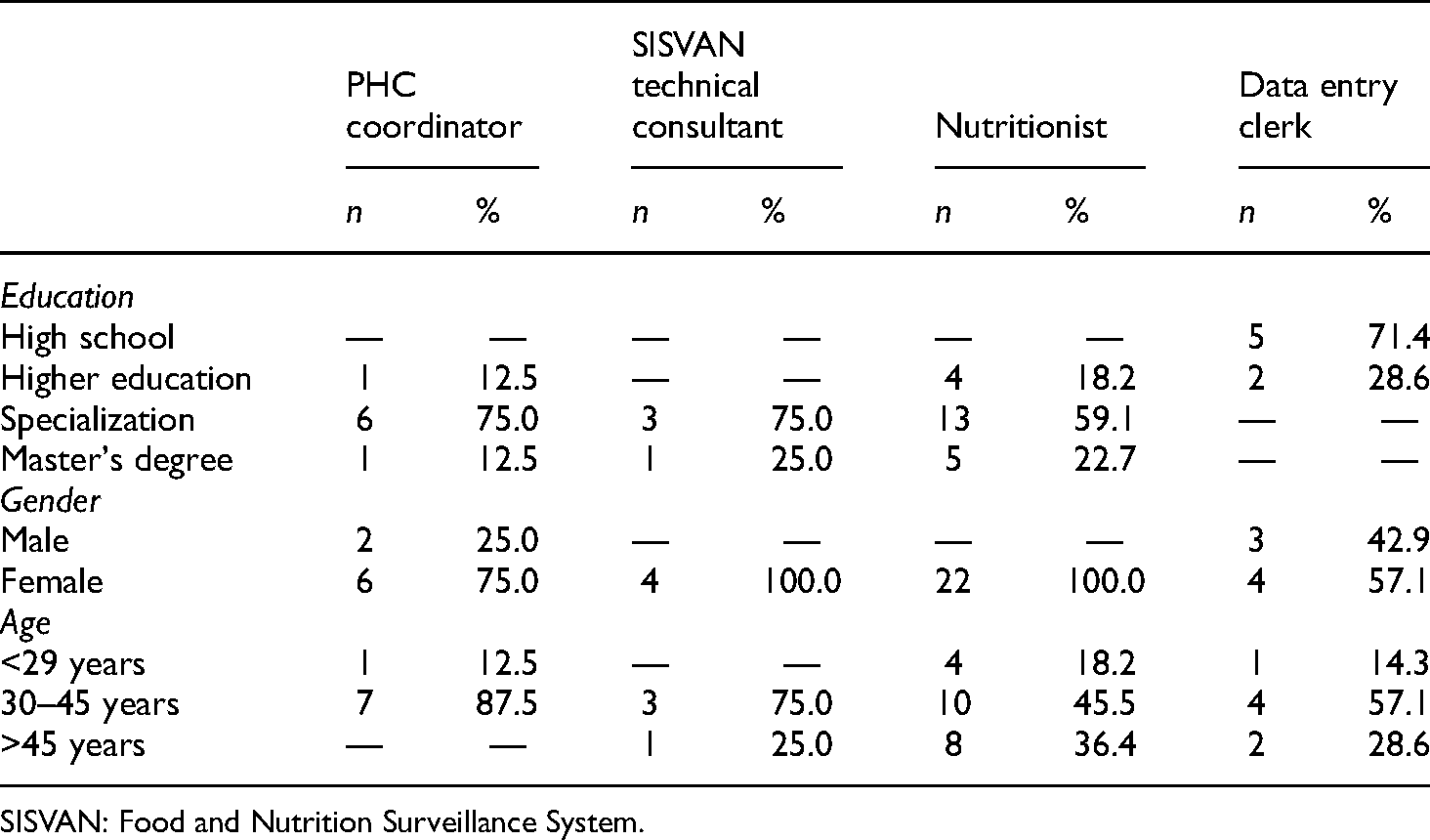
SISVAN: Food and Nutrition Surveillance System.
The corpus comprises 5522 text segments (TS), of which 4404 TSs (79.75%) were useful. The results were grouped into the following four main perception groups: (i) understanding the role of VAN and SISVAN, (ii) identification and understanding of the structural components of SISVAN, (iii) the work process, and (iv) potentials and challenges of SISVAN (see Table 2).
Summary of the perception of the SISVAN triad (information–decision-making–action), Zona da Mata, Mineira region of Brazil.

TS: Text Segment; ESF: Family Health Strategy; NASF-AB: Center of Family and Primary Healthcare; SISVAN: Food and Nutrition Surveillance System; VAN: Food and Nutrition Surveillance.
Category 1: Perceptions related to the understanding of VAN and SISVAN
Category 1, which is related to the understanding of VAN and SISVAN, had TSs related to the words “monitor,” “risk,” “disease,” “future,” “diagnosis,” and “reliable,” evaluating the participants’ perceptions of the system, its functionality, and operation. This category was responsible for identifying participants' conceptual perceptions, which involved perceptions about the relationship between the system and its goals.
Afterward, in the interviews, the words “mapping,” “evaluation,” and “verification” stood out as the main features of the system, concerning risk assessment of disease emergence, once presents a reliable assessment of the reality.
I understand that SISVAN is a tool to map food and nutrition conditions among city residents. You can identify the areas that have more obesity and the ones with the most malnutrition. (P22, SISVAN technical consultant)
The SISVAN is the basis that allows us to verify, evaluate, and identify the risk factors that can compromise one's health; for instance, high blood pressure, diabetes, and cancer. (P27, PHC coordinator)
With a system working properly, effectively, you could perform diverse interventions, which would be good for professionals, users, and management. If this system is in place and working, a primary care patient can avoid a complication that could potentially lead to bigger problem ahead, even hospitalization. (P7, PHC coordinator)
Healthcare workers and skilled professionals have recognized that as one becomes aware of the objectives and goals of the system, the interest in meeting them increases. However, not everyone has access to these goals: I wanted to know about the goals; for example, each city has the number of patients that you have to see. I have heard people saying that we have not met our goals, but we do not even know what these goals are. (P33, nutritionist)
Whereas coordinators defined VAN as a mapping system, the data entry clerks did not know how to discern these questions, as shown in the following statement: I know that SISVAN is a program to help, what I mean is, there is an efficiency, and it assesses population growth, and how every family lives, right? This program is a good way to know each family, their needs, that is, what happens to each one of them. (P13, data entry clerk)
Category 2: Perceptions of the city SISVAN structure
Category 2 comprises the main aspects related to participants’ perception of the structure of the system, highlighting a lack of resources, with an emphasis on anthropometric equipment, transportation, and a lack of qualified personnel. The interviewees reported inadequacies regarding the maintenance of anthropometric equipment and a lack of adequate facilities to practice activities in partnership with the Center of Family and Primary Healthcare (NASF-AB).
The first thing we need is a scale. I have my own scale in my car. It is the same with transportation; I have to see patients in rural areas and I have to rely on my own personal transportation to see them. (P3, nutritionist)
We need equipment maintenance to be able do a more reliable job. Because our scales have not been maintained in a long time, they sometimes display the wrong weight. We do not have a suitable anthropometer, a suitable scale to take to fieldwork; we do not have a proper means of transportation to carry the equipment. (P22, SISVAN technical consultant)
… the main difficulties I feel are lack of time at work and lack of a suitable place to do group activities. I think it would be these two. If we can have a little more time and a place to do them, I believe we can manage the rest Sometimes we do not have enough supplies, but I think we do not need much to carry out these activities; we need the essentials and these are not available sometimes. (P25, nutritionist)
Most PHC coordinators had little experience with SISVAN. One interviewee reported the following: Actually, this part of food and nutritional surveillance is not exactly my expertise; I fell from the sky and landed in this job. (P18, nutritionist)
The need for continuous health education that addresses VAN was pointed out by several interviewees, even referring to the standardization of data collection, which would result in more reliable diagnoses and actions with better outcomes.
I think there must be more training. It will improve everything, especially the outcomes. (P37, nutritionist)
Because, in fact, I think there must be training and information, “What is SISVAN?”, “Why are you going to do this?” “Do you understand it?” However, they assign you the job, without any information, “Oh, here it is; you will type this, okay? Then take it and type it.” So, you will worry about what? (P13, data entry clerk)
I think that the community health agents should be better trained because they do the data collection. They need to be confident about the issue on anthropometry, about the position of the subjects during the measurements, whether they are facing forward or facing backward when weighing, and not weighing people wearing shoes and heavy clothing. By doing so, the data will be more reliable and the system can generate better results. (P37, nutritionist)
In addition to issues with structural resources and trained personnel, a lack of a clear action plan, an absence of clear goals and results to be achieved, misdirection of actions, and a lack of clarity and knowledge of goals by workers and skilled professionals were also found. Indeed, data collection and entry in the information system are prioritized, but without informing those responsible for these activities as to what, how, and why they are being done.
What I consider to be inadequate is not only the lack of resources but also the lack of planning. There is a lack of interest as well. There is no planning of the activities in the VAN system. (P34, nutritionist)
There is no planning for SISVAN. There is no coordination; as a result, nothing is done. We continue to make our calls but without any direction. There is not any kind of planning. This was in the past. (P35, nutritionist)
Category 3: Perceptions of the work process
Participants perceived the work process as weak and fragmented for not having enough work hours, inadequate team composition, and weaknesses in nutritionists’ performance. They also pointed out that the service network was segmented regarding information and action flow between the system's points of attention.
Although the interviewees from the different cities had small differences in their epidemiological, demographic, and social scenarios, many similarities can be seen between the different scenarios, particularly in relation to weaknesses in the work process. Although some cities have a slightly better work methodology, reports show that they are isolated or incomplete, such as referencing and counter-referencing of users.
With regard to counter-referencing, I receive and issue it, but it is not 100%. If it were put it in terms of a percentage, it would be about 60%, but I do not see any problem with this; when I refer, I also receive patients. (P40, nutritionist)
Regarding PHC, we do not have any integration; we do not have any contact. There is a gap. What exists is a demand according to the user's interest, without a referral. (P10, nutritionist)
Nutritionists’ performances were reported as isolated and fragmented due to a lack of a well-defined and strengthened healthcare network (RAS); however, the role of NASF-AB as a promoter of food and nutrition actions whenever there is a nutritionist in this center was highlighted. On the other hand, interviewees reported a lack of adequate facilities for group activities promoted by the NASF-AB nutritionists.
Our performance here, in the health network, I think is fragile. I think performance is weak. However, with the implementation of more NASF-AB teams, we will have much better performance. (P32, PHC coordinator)
The interviewees have noticed some small improvements in the system, albeit isolated ones. They also attributed these improvements to the presence of a nutritionist at NASF-AB: Some time ago we made a chart flow to use the SISVAN data. We evaluated whether the child was underweight and made a cool graph. We asked the nutritionists to monitor the underweight children, to group them at NASF-AB and include more activities, but not all the teams had nutritionists, so the idea ended up being lost. (P15, SISVAN technical consultant)
Some interviewees expressed substantial concern about the inadequacy of the compositions of the health teams.
The number of nutritionists is insufficient. It is what I am telling you; we could have a professional on each team with an adequate workload. I believe that when the NASF-AB project was initiated, it could have been better structured, you know? Just as you need a doctor in primary healthcare, we also need a nutritionist, you see? (P31, PHC coordinator)
Moreover, participants voiced the need for better use of the system to guide effective actions. They stated that the information–decision-making–action triad is frail: … This is what I think is wrong: this demographic, epidemiological, and nutritional transition in the country, how can it be? You generate numbers, you feed the system, but they do not result in effective measures. (P37, nutritionist)
The difficulties related to the work process also involved the accumulation of duties and time management, as referenced below: If we had more time to closely monitor the work process, surely we could get more proposals and improve organization to have better outcomes. It would involve even more system-oriented programming. (P27, PHC Coordinator) I collect and enter the data, but I do not have time for evaluation. I have other duties, so many times, I have the data, which are particularly important, but I do nothing with them. I understand that the difficulties in performing VAN actions are related to a lack of time. I think this makes it difficult to execute (the duties). In the reality of UBS,
1
where the action happens, a professional has many attributions, so I can say from my point of view that the problem is the lack of time to do everything. (P9, technical consultant of SISVAN)
Category 4: Potentials and challenges of SISVAN
The fourth category comprises the main healthcare workers and skilled professionals’ perceptions regarding the system's potential and the main challenges in achieving the desired results. The words “directing,” “tool,” and “indicator” were highlighted as the main potentials, and the words “coverage,” “partnership,” and “training” indicated the main challenges. In addition to the absence of political willingness, interviewees also stated that it is necessary to establish partnerships with research institutes, such as universities, which would enhance the quality of the service provided. In the professionals' perception, there is no partnership between the surveillance sector and universities, but the professionals believe that it is important that this partnership be made.
Regarding the SISVAN potential, workers and skilled professionals mentioned the possibility of better targeting of the primary healthcare services and enhancing user care within the health system with an early diagnosis of food and nutrition situation for improved nutritional status. These concepts can be seen in the following interview excerpts: SISVAN can provide for all citizens, including children, more accurate services and primary care, thereby reducing hospitalizations and other health problems. (P41, data entry clerk) With SISVAN, it is possible to obtain a precise indicator of the nutritional status of the population. Then actions can be planned based on it. It is a tool for diagnosis and planning. (P2, nutritionist)
On the one hand, nutritionists, who are professionals working in the front end, raised questions related to a nutritional diagnosis, mapping, and early diagnosis as system potentialities, focusing on the possible outcomes. On the other hand, coordinators were more concerned with the challenges, such as financial constraints, the process of data entry in the information system, and its performance. This unveils the gap between the objectives and the use of the system.
The most complicated thing is that if you dońt meet a goal, you dońt get the money. (P7, PHC Coordinator)
I can see some potentials, but for us, the most important thing is to meet the goals. Our SISVAN is useful to get resources, so we do not take advantage of its potential, but in the end, the biggest challenge is to achieve the goal. (P14, PHC Coordinator)
The interviewees reported that maintaining SISVAN coverage at the same rate in all phases of life is a challenge since specific groups such as children and pregnant women are prioritized, with other groups receiving poor coverage.
A challenge would be to treat the age groups with their specificities, because I noticed that in the last report I did there were very few elderly people. There are many children and pregnant women because I use the pre-natal HIS registry, but for older people, I think I would have to do a more targeted job. (P30, data entry clerk)
The lack of clarity in system functioning was mentioned as a setback, which shows the considerable distance between the system's goals and actual practices: The challenge is to explain what the logic is, the methodology, because as far as we know, the team, including the managers, thinks it's just about data collection. (P8, nutritionist)
The lack of training was also identified as a challenge: I think training has to be part of the routine. It should not be related only to problems; I think we should be trained according to the skills required. For example, I need to be able to guide and coordinate, and we are poorly trained, especially to use specific systems. (P6, SISVAN technical consultant)
The interviewees expressed suggestions for improving the system related to partnerships and political administration: So, you must have a manager who's really worried about what's going on in the city. I think, along with that, there should be partnerships, for instance, with the universities. We could think of doing more joint work, but if the management does not support this idea, how will the university participate? It all comes down to political will. (P36, nutritionist)
Table 2 summarizes the main findings of this study based on an analysis of four evaluation-perception pillars (concept, structure, process, and result) to understand the perceptions of healthcare workers and skilled professionals in the Zona da Mata Mineira region of Brazil. Regarding the conceptual understanding, the participants identified the applicability of SISVAN as a VAN instrument, highlighting the functions of mapping, evaluation, and risk assessment of the health situation of the population. However, the working conditions are underdeveloped, revealing a poor structure in terms of insufficient equipment, facilities, and supplies. The lack of an organized and efficient RAS impairs professionals’ work process providing insufficient working time, inadequate team composition, as well as a fragmented and disjointed performance among nutritionists. Notwithstanding these issues, the performance results follow the same trend, showing inadequate direction, knowledge, and management investments, as well as a failure to envisage important and enriching partnerships. This is confirmed by analyzing the results of another study conducted by our research group in the same municipalities, in which the evolution of the coverage of the nutritional status of the population from 2008 to 2017 and the evolution of the coverage of the monitoring of food consumption markers of the population (<2 years) in the period from 2016 to 2017 showed low performance of the system. 15 Thereby, risk management is compromised, which is expressed as the inefficiency and inefficacy of food and nutrition policies.
Discussion
This research revealed that both skilled professionals and workers see SISVAN as a fragile and unstructured system in the cities evaluated, compromising the ability to control and monitor the major nutritional problems prevalent in primary care. The perceptions of this study are similar to those of an earlier evaluation of SISVAN in the management of food and nutrition actions in Minas Gerais conducted in 2015, which demonstrated the importance of the perception of healthcare workers and skilled professionals on nutritional monitoring, early diagnosis, and direction of actions. 5 In addition, there are questions regarding the potential role of this system in the elaboration of nutritional diagnosis and disease monitoring.
Concerning the structure of SISVAN, this study unveiled incipient working conditions that are not conducive to achieving the desired outcomes, namely reduced work hours and other unmet needs such as the absence of anthropometric equipment and adequate facilities. All these compromise the generation of quality information and implementation of actions, reflecting the weaknesses in the use of SISVAN as a system to manage information on food and nutritional surveillance in primary care, as has already been demonstrated by other Brazilian researchers.5,14–16
The structural and organizational issues highlighted in this study, such as inadequate facilities and lack of preventive maintenance of anthropometric equipment management, have also been reported in other developing countries, including those related to anthropometric data collection. 21 It remains critical to minimize the random errors in measurements by using standardized techniques and rigorous quality control procedures. Specifically, in attempting to achieve management goals, the number of individuals evaluated is increased. However, this may be counterproductive in anthropometric data collection, as this would increase the training and supervision requirements as well as researchers’ exhaustion, which can affect overall accuracy. 24
In 2014, it was demonstrated in Brazil that despite the implementation of SISVAN Web, the structures of the logistics and equipment for VAN actions carried out by the health team were insufficient or low quality, and thus unable to meet the emerging demand. The authors also considered it a fundamental necessity that the data collection and anthropometric equipment used by SISVAN be standardized and the workers and skilled professionals be trained on a continuous basis. They emphasized the need for adequate infrastructure and motivation of healthcare workers and skilled professionals to perform surveillance in day-to-day activities. 32
Some authors have shown that human resources feel unmotivated to work in public health, presenting little preference, few skills, and low personal stimulus for this area, 33 which was not observed in this study.
Although the interviewed professionals reported the need for training, they demonstrated aptitude and willingness to face new service challenges if structural conditions were available, which may favor an efficient and satisfactory work process. Moreover, several participants mentioned NASF-AB as an important area for a nutritionist and strengthening of VAN actions. To strengthen and broaden the scope of these actions, NASF-AB proposes to include nutritionists as staff members. Thus, despite the inclusion of nutritionists in primary healthcare services in previous efforts of Brazilian cities, 34 the NASF-AB proposal allowed great inclusion of nutritionists in this area of care, establishing an important action in Brazilian primary care. 35 However, not all evaluated cities had implemented NASF-AB, and even some towns that had the nuclei in operation did not have a nutritionist.
It is important to discuss the uncertainty of the continuity of these systems, programs, and projects related and strengthened by NASF-AB due to Ordinance 2979, instituted on November 12, 2019, 36 which extinguishes this model of healthcare, which may lead to imbalances throughout the sector.
The lack of knowledge about the use of system information and consequently the underutilization of data for the implementation of actions in the SUS were pointed out in the study by Rolim et al. 5
This is an international trend whereby few assessments of the use and value of surveillance information have been conducted and reported. 21
As a consequence of weaknesses in the information–decision-making–action triad, the surveillance system becomes fragmented in the sense of complementary health care and is characterized by professional dissatisfaction and low productivity, thus failing to respond to both the expectations of the professionals involved and the needs of the population served.
Another step in this research revealed low coverage of the nutritional status of certain population groups and demonstrated the need to obtain pertinent and reliable data to allow routine nutrition and health monitoring. This action is known to enable the detection of trends that help in decision-making and in the formulation of health actions and policies in a particular country or region. A Food and Nutrition Surveillance System should include a broad set of appropriate and quality indicators, collected with satisfactory frequency, and focused on groups vulnerable to food and nutrition insecurity. 26 Importantly, knowing the factors that influence the trend of nutrition monitoring in health services allows decision-makers to identify, prepare for, and address emergencies by developing effective strategies before the onset of a crisis.
This study proposed identifying the perceptions of healthcare workers and skilled professionals regarding the performance of the Food and Nutritional Surveillance System in the Zona da Mata Mineira region of Brazil. In the scope of this study, the results corroborate the literature, describing the health professionals’ perceptions of the system as unable to meet objectives or solve health problems prevalent in the current population, poor coverage of SISVAN,13–16 and gaps in the management of food and nutrition actions in primary health care of the SUS. 5
Despite its limitations, the results of this research corroborate the literature regarding the weaknesses found in nutritional surveillance systems of several countries. Countries such as Democratic Republic of the Congo, Somalia, and Sudan face difficulties including poorly trained or unmotivated staff, difficulty in sending data from sites to the local center in a timely and reliable manner, a lack of quality control procedures to ensure proper entry and analysis of data, and failure to produce reports in a timely manner. In addition, there are problems in the population's access to data collection services and some stakeholders do not act on the basis of the information generated by the systems.37–39 In other countries such as Ethiopia, Indonesia, Mozambique, the Palestinian Territories, and Uganda, the systems operate under unstable conditions. In Bangladesh, China, Djibouti, Guatemala, Kuwait, Nicaragua, Vietnam, and Zambia the systems operate at various stages of development. 40
Notably, the development of the system is independent of the method of data collection (whether repeated sampling surveys, community-based sentinel posts, registrations in food programs, mass collection, or collection in public health units), since countries with some of the most serious security and access problems such as Ethiopia and Somalia use a wide variety of data collection methods.
Nutritional surveillance systems that use a wider variety of data collection methods present weaknesses such as poorly trained or demotivated staff, difficulty sending data from sites to central locations in a timely and reliable manner, a lack of data quality procedures to ensure proper data entry and analysis, untimely reports, and stakeholders who do not act based on information generated by systems, which corroborates the results of this research. A major weakness of systems that use sentinel sites is that sentinel site data may be representative of the population seeking site services but are generally not representative of the general population in the country given that a portion of the population does not seek these services.
Two other major challenges encountered in most nutritional surveillance systems are the weak capacity and ownership of the national government and the uncertainty and instability of financing, which is not appropriate to discuss in this research since SISVAN does not receive funding directly. These problems have resulted in surveillance systems becoming nonfunctional for certain periods of time, as seen in Zambia. 40
The lack of proper working conditions, transportation, and adequate workload makes it difficult to achieve a high-quality nutritional diagnosis in line with SISVAN's goals. It is impossible to obtain high-quality information and implement the necessary actions without a proper structure. In this sense, it is crucial to raise awareness of the importance of VAN actions at all professional levels. Human resources training is also important for high-quality data collection and recording. Regular reports from the SUS Computer Department of the Ministry of Health (DATASUS), reinforcement of structural resources, and collaboration among government agencies will provide faster access to the information needed for proper decision-making and successful public health policy.
Limitations
This study could have benefited from other data collection methods, such as focus groups, which would broaden and enhance further discussions of this qualitative study. It is suggested that other researchers wishing to further explore this topic expand the types of data collection.
Conclusion
The perception of SISVAN by healthcare workers and skilled professionals reveals a frail and unstructured system in the cities evaluated, compromising the capacity to control and monitor the main nutritional problems persisting in primary care. Participants reported the need for great efforts to raise awareness of the importance of Food and Nutrition Surveillance actions at all levels of the public healthcare system. They further pointed out the need for human resources training, quality data recording methods, and suitable facilities. Therefore, investments in the entire system are essential to strengthen the information–decision-making–action triad, which would result in the improvement of users' health indicators.
This perception shows mismatches between the proposal of the information system produced by the Ministry of Health and the care models in which they are practiced and put into action by SUS workers and skilled professionals. This has led to discontinued and fragmented actions and impasses in health management. These mismatches are unveiled in the system's clear failure to achieve the desire results.
As a final product of the perception of deficiencies in this work, there is a compromise in risk management, an important step in the surveillance process, which can weaken the actions and policies for food and nutrition. Considering the current epidemiological profile of the Brazilian population, which presents the concomitant prevalence of overweight and obese individuals, malnutrition, and micronutrient deficiencies, it is verified that the organization of the VAN in the health services of the local territories is in urgent need of monitoring and evaluation of nutritional disorders.
In this way, it is necessary that the tools for VAN are available and the requisite conditions are created to encourage their use in an efficient and effective way.
Footnotes
Acknowledgments
The authors acknowledge the support of the funding institutions: Coordination for the Improvement of Higher Education Personnel - CAPES, National Council for Scientific and Technological Development - CNPq, Research Support Foundation of the State of Minas Gerais - FAPEMIG and the participation of all volunteers in the study.
Authors’ contribution
ISAG was responsible for planning, carrying out the study, design, methods, data collection, interview transcriptions, data analysis and interpretation, running the software, writing, proofreading, and editing the manuscript. CPD was responsible for methods, data analysis and interpretation, and running the software. TRM was responsible for the final review of this text. RMMC was responsible for data analysis and proofreading the last version of the manuscript. GDC was responsible for research supervising and coordination, planning, design, writing, proofreading, and editing the manuscript, and funding application.
Ethical aspects
This study was conducted according to the guidelines established in the Declaration of Helsinki and all procedures involving human beings/patients were approved by the Ethics Committee on Research with Human Beings of the [details omitted for double-anonymized peer review], respecting the ethical aspects, according to Resolution 466/12 of the National Health Council and approved under Opinion 2.370 on November 8, 2017. Verbal consent was requested and formally recorded for all respondents.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Minas Gerais Research Support Foundation (FAPEMIG – CDS – APQ-01201-14) and the National Council for Scientific and Technological Development (CNPq – 457912/2014-6).