
Abstract
Given that the complications of type 2 diabetes can start at an early stage, early detection and appropriate management of prediabetes are essential. We aimed to develop an expert opinion on prediabetes in Lebanon to pave the way for national guidelines tailored for the Lebanese population in the near future. A panel of seven diabetes experts conducted a thorough literature review and discussed their opinions and experiences before coming up with a set of preliminary recommendations for the detection and management of prediabetes in Lebanon. Lebanese physicians employ multiple tests for the diagnosis of prediabetes and no national cut-off values exist. The panel agreed that prediabetes screening should be focused on patients exceeding 45 years of age with otherwise no risk factors and on adults with risk factors. The panel reached that fasting plasma glucose (FPG) and HbA1c should be used for prediabetes diagnosis in Lebanon. FPG values of 100–125 mg/dL or HbA1c values of 5.7%–6.4% were agreed upon as indicative of prediabetes. For the management of prediabetes, a three-step approach constituting lifestyle modifications, pharmacological treatment and bariatric surgery is recommended. There should be more focus on research on prediabetes in Lebanon. This preliminary report will be further discussed with the Lebanese Society of Endocrinology, Diabetes and Lipids in 2021 in order to come up with the first Lebanese national guidelines for the detection and management of prediabetes in Lebanon.
Introduction
The term “prediabetes” is used by the American Diabetes Association (ADA) and the American Association of Clinical Endocrinologists (AACE) to define a condition characterized by a slightly elevated blood glucose level, not high enough to be considered as diabetes but outside the normal range.1,2 Prediabetes is defined by an impaired fasting glycemia (IFG) or impaired glucose tolerance (IGT) or raised hemoglobin levels. It is also called “non-diabetic hyperglycemia” by the World Health Organization (WHO), and “intermediate hyperglycemia” by the International Diabetes Federation (IDF).3,4 It is considered a risk factor for the onset of type 2 diabetes increasing its short-term risk by 3–10 folds. 5 Indeed, the yearly conversion rate of prediabetes to diabetes is 5%–10%. 6 A recent meta-analysis found that people with prediabetes have an increased risk of all-cause mortality (relative risk (RR) 1.13), composite cardiovascular disease (RR 1.15), coronary heart disease (RR 1.16), and stroke (RR 1.14). 2 In addition, prediabetes was also associated with an increased risk of cancer (RR 1.15). 4
In 2019, the IDF estimated that 374 million people had IGT especially those aged 50 years or less. By 2045, IGT is expected to affect 548 million adults between 20 and 79 years old representing 8.6% of the adult population. These worldwide rising numbers are also coupled with an increase in the global rate of diabetes-related morbidity and mortality. 3
The high prevalence of prediabetes is a growing problem in the Middle East. In the Arab region, 13.7 million people aged between 20 and 79 years old were reported to be living with prediabetes. 7 According to the IDF, 364,000 people lived with IGT in 2019 in Lebanon; and the age-adjusted comparative prevalence of IGT was 8.4%. 8
Observational studies have revealed that diabetes complications can develop early at the stage of pre-diabetes. 6 Thus, early detection and proper management of prediabetes are beneficial in delaying its progression9–11 and reducing the aforementioned complications.12–14
Although prediabetes has a high global prevalence and is correlated with diabetes complications, national policies toward its prevention and management are only available in a few countries. 5 Worldwide, countries are beginning to recommend lifestyle programs and, in some cases, pharmacological intervention with metformin. 15
Although several drugs have been assessed in trials for prediabetes, the Food and Drug Administration (FDA) has not approved any medications for its treatment or for the prevention of type 2 diabetes. 16 The ADA recommends (as outlined in its 2019 Standards of Medical Care in Diabetes) that “Metformin therapy for prevention of type 2 diabetes should be considered in those with prediabetes, especially for those with body mass index (BMI) ≥ 35 kg/m2, those aged <60 years, and women with prior gestational diabetes mellitus.” 17 In this expert opinion, we aimed to develop a consensus on the screening, diagnosis, and management of prediabetes in Lebanon.
Methodology
A panel comprising seven reputable experts in diabetes and endocrinology; six of which are Lebanese with clinical experience in the public and private healthcare sectors in Lebanon ranging from 20 to 30 years, met on the 24th 5 of September 2018 to understand the current status of prediabetes screening, diagnosis and treatment in Lebanon. A literature review was conducted in PubMed database using the following terms: prediabetes, impaired glucose tolerance, impaired fasting glycemia, non-diabetic hyperglycemia, Middle East, Lebanon, screening, diagnosis, prevention, management, guidelines, and recommendations. The experts selected articles that best suited the purpose of the project. The retrieved articles were discussed along with the professional opinions and experiences of the panel. No formal system was used to provide levels of evidence of the recommendations of the panel. All the recommendations mentioned herein were accepted and approved by all the experts in the panel.
Results
The current situation of prediabetes in Lebanon
There is no agreement among Lebanese physicians on the tests (nor their cut-off values) that should be employed for the diagnosis of prediabetes.
Prevalence of prediabetes in Lebanon
During the last 30 years, a lot of studies have been undertaken in Lebanon but the majority of them have had limitations either in the study design or in the population of the studied sample. Most of the studies gathered data from a specific region in Lebanon and not across the country. A study was conducted in 1997 on 2518 Lebanese subjects aged more than 30 years old. It showed that the prevalence of IGT was 6% (cut-off point: 110–125 mg/dL). 18 In 2005, another study was undertaken in Beirut using the ADA 1997 criteria. This study included 3000 patients and showed that IGT prevalence was 5.1%. 19 Another study conducted in 2017 in Greater Beirut included 500 patients aged around 45 years old and showed that diabetes prevalence was 15% compared to 40% for prediabetes. 20
Screening for prediabetes
Several factors may influence the onset of prediabetes including genetics, peripheral insulin resistance, defects in insulin secretion, glucotoxicity, lipotoxicity, impaired incretin release, amylin accumulation, inflammation, oxidative stress, and decreased beta cell mass leading to beta cell dysfunction. 21
The ADA, in a recent statement, stated that prediabetes is linked to obesity (abdominal or visceral), dyslipidemia, high triglycerides and/or low high-density lipoprotein (HDL)-cholesterol, and hypertension. The ADA considers the screening criteria for prediabetes cited in the Supplemental Appendix Table 1. 22
The United States Preventive Services Task Force (USPSTF) recommends screening for abnormal blood glucose as part of cardiovascular risk assessment in adults aged 40–70 years who are overweight or obese. Clinicians should offer or refer patients with abnormal blood glucose to intensive behavioral counseling interventions to promote a healthy lifestyle and physical activity (Grade B). 23
According to the AACE, people who have any of the clinical risk criteria cited in the Supplemental Appendix should get tested for prediabetes. 24 The AACE recommends repeating prediabetes testing every 3 years in the case of a normal range of glucose values but on an annual basis in subjects with two or more risk factors (Supplemental Appendix Table 2).
FINDRISC Diabetes Risk Calculator is a prediction tool to identify patients at risk of developing diabetes. It estimates the risk of developing diabetes and the required frequency of screening. It requires no laboratory testing and has been validated in multiple populations. FINDRISC uses age, BMI, physical activity, vegetable and fruit intake, medical treatment of hypertension, history of hyperglycemia, and family history to determine the risk of developing diabetes. Using FINDRISC to identify high-risk people and apply an educational intervention, has led to a reduction in the incidence of diabetes. 25
The Lebanese expert panel recommends that all people older than 45 years without risk factors and adults with risk factors should be screened for prediabetes. Upon comparing the risk factors mentioned by the ADA and the AACE, the Lebanese expert panel agreed that the risk factors in Table 1 should be considered on a nationwide scale in Lebanon.
Lebanese consensus on prediabetes risk criteria.
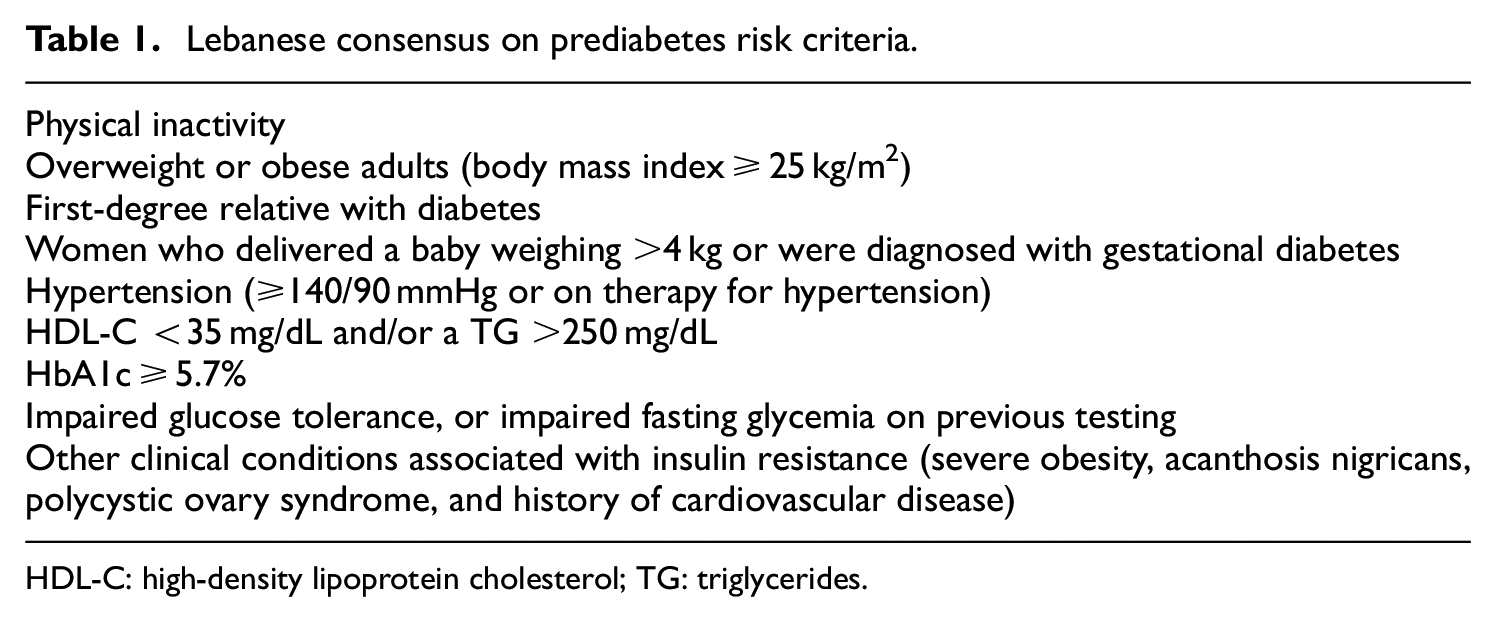
HDL-C: high-density lipoprotein cholesterol; TG: triglycerides.
The Lebanese expert panel recommended that testing should be repeated at a minimum of 3-year intervals with normal results, and should be done more frequently with abnormal findings depending on initial results (e.g. those with prediabetes should be tested yearly).
Prediabetes diagnostic tests, fasting plasma glucose, and HbA1c cut-off values
Several blood tests and biomarkers can be used to diagnose prediabetes. The WHO uses the IFG defined as fasting plasma glucose (FPG) levels of 110–125 mg/dL and IGT as 2-h PG of 140–200 mg/dL after ingestion of 75 g of oral glucose. 26 The ADA has the same cut-off value for IGT (2-h plasma glucose of 140–200 mg/dL) but a lower cut-off value for IFG (FPG of 100–125 mg/dL) and additionally considers HbA1c to diagnose prediabetes with levels ranging from 5.7% to 6.4%. 22 The IDF has set the following cut-off points for prediabetes diagnosis: FPG between 100–125 mg/dL or 2-h glucose following ingestion of 75-g glucose load levels between 140 and 199 mg/dL. The IDF also recognizes an increased level of HbA1c as a tool to diagnose those with prediabetes. 27
In this regard, the panel agreed on FPG and HbA1c as the preferred tests for the diagnosis of prediabetes in Lebanon and the adopted cut-off points were as follows:
FPG for prediabetes diagnosis: 100–125 mg/dL as per the IDF guidelines
HbA1c 5.7%–6.4% as per the ADA guidelines
Behavioral lifestyle programs should be the cornerstone of all efforts to reduce the risk of conversion from prediabetes to type 2 diabetes. No pharmacologic agents are currently approved for the management of prediabetes. However, pharmacotherapy targeted at managing non-diabetic hyperglycemia may be considered in high-risk patients after individual risk-benefit assessment. 8
Lifestyle intervention in prediabetes should aim to reduce weight by 5% to 10% and maintain it for long periods of time. To achieve this objective, a program of regular moderate-intensity physical activity for 30–60 min daily is recommended at least 5 days per week along with a diet that includes caloric restriction, increased fiber intake, and (in some cases) carbohydrate intake limitations. 8 Many studies demonstrated the positive effects of lifestyle intervention during a period ranging from 2.8 to 6 years.10,28–30
Diabetes self-management education (DSME) and diabetes self-management support (DSMS) programs are appropriate for people with prediabetes to help prevent or delay the onset of diabetes. 31 Therefore, during the Diabetes Prevention Program (DPP) (N = 3234), intensive lifestyle intervention effectively prevented progression from IGT to type 2 diabetes by 58% compared to 31% with pharmacotherapy with metformin. 10 Maintenance of long-term weight loss was assessed in a study that included 2766 patients; results showed a regain in weight in the lifestyle arm, with weight change being the same at 10 years for both lifestyle and metformin. Over this time period, the decrease in the incidence of type 2 diabetes was almost the same for both groups. 32
In the SCALE obesity and prediabetes study, patients treated with liraglutide showed an 8.4 kg weight reduction compared to a loss of 2.8 kg in patients receiving placebo. Among patients who were normoglycemic at screening, 7.2% of those treated with liraglutide had prediabetes after 56 weeks of follow-up compared with 20.7% of those receiving placebo. Among patients who were already prediabetic with prediabetes at screening, 30.8% of those treated with liraglutide continued to exhibit prediabetes at 56 weeks of follow-up compared with 67.3% of patients receiving placebo. 33
A study conducted in Lebanon combining liraglutide and metformin showed a significant improvement versus metformin alone in weight loss, HbA1c values, plasma lipids, and the percentage of subjects who reverted to normoglycemia or remained in a state of prediabetes. 34 Bariatric surgery is the most effective way to decrease weight. It induces a significant and sustainable improvement in the metabolic profile of obese patients and decreases the incidence of type 2 diabetes. There are many types of laparoscopic surgery including laparoscopic adjustable gastric banding (LAGB), laparoscopic sleeve gastrectomy (LSG), and laparoscopic gastric bypass surgery (LRYGB). The best results and outcomes are obtained with LRYGB. 35 The three-step approach for prediabetes management agreed upon by the Lebanese expert panel is summarized in Table 2.
Lebanese consensus on prediabetes management.

Metformin dose in prediabetes
In the DPP study, subjects were randomly assigned to 850 mg metformin twice daily (n = 1073) or placebo (n = 1082) and followed for 2.8 years. The results showed excellent adherence to metformin—despite gastrointestinal side effects—and a 31% decrease in the risk of developing diabetes with metformin. The optimal benefit was observed in patients with BMI ≥ 35 kg/m2—a 50% reduction in the risk of progression to type 2 diabetes. A reduction of 1.7 kg was observed in the metformin group versus 0.3 kg weight gain in the placebo group. The weight reduction leading to improved insulin sensitivity and pancreatic function is viewed as a possible mechanism for reducing the risk of progressing to frank diabetes.10,36,37
Similarly, in the Canoe trial where metformin (500 mg) twice daily was combined with rosiglitazone (2 mg) in 103 patients, there was a beneficial effect in preventing the conversion of IGT subjects to type 2 diabetes. 38
The Lebanese expert group concluded that management of prediabetes should be as follows:
Therapy should be initiated with one tablet of metformin XR 500 mg once daily with the evening meal.
After 10–15 days, dose uptitration should be considered if the glycemic profile (in terms of FPG, 2-h PG following 75 g OGTT, and HbA1c) did not change; in order to drive values into the normal range.
A gradual uptitration of the metformin dose may improve gastrointestinal tolerability. The maximum recommended dose is 2000 mg XR once daily with the evening meal.
If metformin XR is not available, then metformin immediate release (IR) can be used as an alternative formula. In such a case, the dose should be divided with meals.
Limitations
There are some limitations to this consensus; it was not based upon a systematic review of the literature, and the expert panel was not multidisciplinary.
Conclusions
A literature review of the existing data on prediabetes and a thorough professional discussion between seven diabetes experts resulted in a consensus on screening, diagnosis, and management of prediabetes in Lebanon (Figure 1).

Lebanese algorithm for prediabetes management and screening.
The panel agreed that FPG and HbA1c are the preferred tests for the diagnosis of prediabetes in Lebanon. All people older than 45 years without risk factors and adults with risk factors should be screened for prediabetes. Due to the lack of local studies, the panel agreed that Lebanese physicians should adopt cut-off points of international guidelines in their diagnosis of prediabetes. These are as follows:
FPG: 100–125 mg/dL as per the IDF guidelines
HbA1c: 5.7%–6.4% as per the ADA guidelines
The panel agreed on a three-step approach for prediabetes management; lifestyle modifications, pharmacotherapy (metformin is the drug of choice in case of failure of lifestyle intervention), and bariatric surgery.
The panel concluded that research data on diabetes and prediabetes in Lebanon is lacking and that this preliminary report needs to be further discussed with the Lebanese Society of Endocrinology, Diabetes and Lipids in 2021 in a quest to bring forward the first Lebanese national guidelines for the detection and management of prediabetes in the Lebanese population.
Supplemental Material
sj-pdf-1-sci-10.1177_00368504211029439 – Supplemental material for Experts’ opinion on the detection and management of prediabetes in Lebanon
Supplemental material, sj-pdf-1-sci-10.1177_00368504211029439 for Experts’ opinion on the detection and management of prediabetes in Lebanon by Emile Andari, Paola Atallah, Sami Azar, Akram Echtay, Selim Jambart, Charles Saab, Harry CS Howlett and Murad Al-Naqshbandi in Science Progress
Footnotes
Declaration of conflicting interests
The authors received fair market honorarium from Merck KGaA Middle East Ltd. for their time spent participating in an advisory board.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financially supported by Merck KGaA Middle East Ltd., an Affiliate of Merck KGaA, Darmstadt, Germany.
Ethical approval
Ethical approval was not sought for the present study because this was a review article and did not involve any patients.
Informed consent
Informed consent was not sought for the present study because this was a review article and did not involve any subjects.
Supplemental material
Supplemental material for this article is available online.
Author biographies
![]() ). He was also a past president of the Lebanese Society of Endocrinology, Diabetes and Lipids, and is currently the vice president of the Society. He is a principal investigator of multiple clinical trials in Lebanon.
). He was also a past president of the Lebanese Society of Endocrinology, Diabetes and Lipids, and is currently the vice president of the Society. He is a principal investigator of multiple clinical trials in Lebanon.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.