
Abstract
This study developed a formula for calculating the predicted VO2 max value using a prototype model of foot-based cardiorespiratory exercise. Forty sedentary workers (20 men and 20 women) were enrolled via consecutive sampling. They underwent direct measurement of VO2 max using spiroergometry as the gold standard; the predicted VO2 max value was calculated using a prototype model of foot-based cardiorespiratory exercise, which was performed on consecutive days. Multivariate linear regression analysis was used to formulate the equation for the predicted VO2 max value by including potential contributing variables: gender, body height, body weight and heart rate. Bland–Altman test was used for assessing the agreement level for the predicted VO2 max value. The equation for the predicted VO2 max value was formulated as 3.2 + 0.15 optimal exercise heart rate −5.5 sexes (0 for men, 1 for women). The agreement level for the formula was acceptable in all measurement result ranges. The formula developed in this study can be used to measure the predicted VO2 max value with an acceptable agreement level.
Keywords
Introduction
Sitting workers comprise a productive age group that is at a high risk of developing health problems due to sedentary activity, stress, alcohol consumption, smoking and irregular dietary habits. 1 Based on the Indonesian Basic Health Survey/Riset Kesehatan Dasar (Riskesdas) conducted in 2018, the seven noncommunicable diseases (NCDs) with the maximum incidence in Indonesia are hypertension, type 2 diabetes mellitus, chronic obstructive pulmonary disease, cancer, central obesity, coronary heart disease and stroke. All these NCDs were found to be strongly associated with lack of physical activity.2,3 Inactive behaviour is a common problem encountered by several workers, especially those in service sectors because fixed working hours require them to spend most of the time in performing a sedentary activity in the form of sitting. Various efforts have been made to increase the workers’ awareness about active, healthy lifestyle, but in fact, this awareness is still lacking. 4 Approximately 78% of workers in the UK feel that they are sitting too long at work and are concerned about the adverse effects of this situation. 5 In addition, 66% of workers in the Asia Pacific feel that they perform only <30 min of physical activity. 6 In Indonesia, 26.1% of the population can be categorised as being less active. 1 Habibi et al. 7 emphasised that determination of cardiorespiratory capacity is essential in the discussion of health promotion and the prevention of physical problems at the workplace. They suggested using the heart rate as prediction measure to estimate the VO2 max. The VO2 max is widely used to express the cardiorespiratory endurance.8,9
Physical activity is one of the most important determining factors of cardiorespiratory fitness levels. Workers who do not perform any physical activity have 6.3 times lower physical fitness than active workers. 10 No available simple tools combine both for doing physical exercise and measuring VO2 max, especially for doing those while sitting. The prototype of a foot-based cardiorespiratory exercise (Kinesia®) has been developed, which can be used to measure the predicted VO2 max value among workers without requiring them to leave the work desk; furthermore, the prototype is ergonomically sound.
The aim of this study was to formulate an equation for calculating the predicted VO2 max value using the prototype of the foot-based cardiorespiratory exercise.
Patients and methods
Study subjects
This study recruited sedentary workers in Jakarta in 2018. The study subjects comprised both female and male adults of working age, registered as active workers for 3 months, sitting during work for more than 4 h continuously in a day, willing to follow the entire study and undergo screening requirements for physical exercise. The study used the Physical Activity Readiness Questionnaire (PAR-Q) to do health risk screening of Physical exercise. 11
The sedentary category was identified by using international Physical Activity Questionnaire (IPAQ). 12 Prospective participants who had contraindications for physical activity or were pregnant were excluded. Subjects were selected using the sequential sampling method (consecutive sampling). In this study aimed at determining the formula used to calculate the predicted VO2 max value, with the value of the minimum difference detected (δ) being 0.5, the sample size was determined to be 32 subjects; however, considering the possibility of drop out, a sample size of 10% (three study subjects) was added. Therefore, the minimal sample size was 35 subjects. The study considered the equal number of gender and then recruited 20 male and 20 female study subjects.
Cardiorespiratory exercise
The cardiorespiratory endurance was measured with the direct measurement as a gold standard (measuring test 1). The gold standard measurement results were compared to the measurement results of the prototype model of foot rest-based cardiorespiratory exercise (measuring test 2). The gold standard of cardiorespiratory endurance measurement used the spirometry device Metalyzer 3B-R3 (Cortex Biophysics GmbH, Leipzig, Germany) and MetaSoft Studio Software (Cortex Biophysics GmbH, Leipzig, Germany). Cortex Metalyzer 3B (CM3B) is a stationary respiratory gas analysis system using Breath-by-Breath technology.13–16 This technology enables a precise and accurate determination of the individual maximum oxygen uptake rate and the energy expenditure and has thus been used in various scientific studies in sports medicine. The estimation of energy expenditure is based on the ratio of inhaled oxygen to exhaled carbon dioxide. During the diagnostics, the participant wore a breathing mask that is connected via a tube to a respiratory gases analyser.
The study used the built in echocardiography to measure the heart rate as well as a part of exercise safety monitoring. The comparison of the two devices was made to add functions to the exercise tool model, not only as a physical exercise tool but also as an alternative measurement to predict the VO2 max value. This idea was based on the similarity of modalities and the methods of operating both tools, that is, by sitting and pedalling. The examination procedures were conducted in two phases, that is, the initial preparation and the implementation of the protocol. Correlation Coefficients between the measured and predicted VO2 max values had been reported to differ from r = 0.82–0.94.
Data analysis
All data were recorded on the research subject data sheet that was provided with an identification number and contained all the research data. Data were processed and analysed using the IBM Statistics programme for Mac 24.0 version. The analysis was performed in the form of descriptive analysis to describe the general characteristics of the study subjects, and then a multivariate analysis was performed using multiple linear regression backward method to obtain a formula for the predicted VO2 max value. Then, the assumption test was performed to determine the prediction of the results of cardiorespiratory endurance measurements using a training model to measure the value of VO2 max. Existence assumptions, independence assumptions, linearity assumptions, homoscedasticity assumptions, normality assumptions and multicollinearity diagnostics were conducted on assumption tests. The statistical significance value was p < 0.05. The agreement level for the predicted VO2 max value calculated using the developed formula of cardiorespiratory endurance using the prototype model was analysed using the Bland–Altman test.
Results
The developed foot rest-based cardiorespiratory exercise tool model was tested and compared with the gold standard for predicting theVO2 max value.
Stage of determining the validity of the exercise tool model
For determining the validity of the exercise tool model, a comparison was made between the exercise tool model and spiroergometry as the gold standard to predict the VO2 max value. The study included forty sitting workers with an equal number of male and female workers. All of the study subjects have no health risk condition based on the Physical Activity Readiness Questionnaire (PAR-Q) and physical examination by the researcher as a physician. Regarding the characteristics of the subjects, their age was 20–35 years (24/40) with an age range of >35–45 years, and they had a sedentary type of work (34/40) and already in the preparation stage for physical exercise (26/40)]. A total of 13 of the 40 study subjects had a normal body mass index (BMI) and obesity level I. In total, 20 of the 40 study subjects had an average health risk, and 14 subjects had an increased health risk. The characteristics of the study subjects are presented in Table 1.
Characteristics of the study subjects.

After the subjects were declared ready and identified to be safe based on screening for prerequisite requirements, a cardiorespiratory endurance test was conducted using the two comparison measurements. The results of the cardiorespiratory endurance test are presented in Table 2.
Subjects’ physical conditions during the cardiorespiratory endurance test using the exercise tool model and the gold standard.
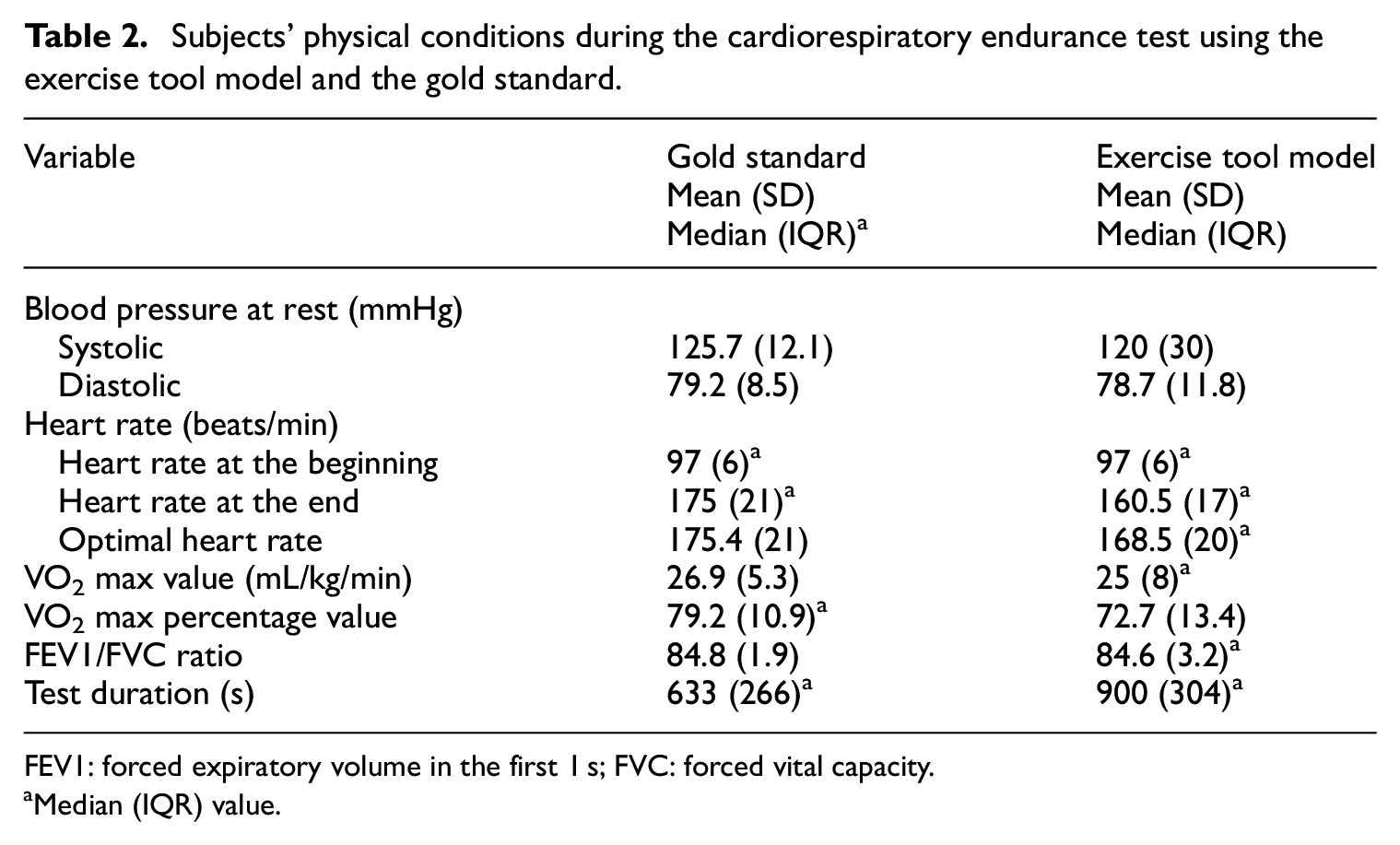
FEV1: forced expiratory volume in the first 1 s; FVC: forced vital capacity.
Median (IQR) value.
The multiple linear regression analysis was performed to determine the factors that influence the results of the cardiorespiratory endurance test. The study found that the predicted VO2 max using the exercise tool model was formulated to the following equation: VO2 max = 3.2 + 0.15 optimal exercise heart rate − 5.5 sexes (0 for men, 1 for women), with the coefficient of determinant R2 = 0.40; p < 0.05 (Table 3).
The determinant factors of the cardiorespiratory endurance using the exercise tool model.

The optimal heart rate value was ranged of 60%–85% of Maximum Heart Beat as an intermediate intensity of cardiorespiratory endurance exercise.
17
Based on the factors that influence the cardiorespiratory endurance test using the training tool model, the predicted VO2 max value can simply be determined using the following formulae: a) Predicted VO2 max value (male) = 0.15 optimal exercise heart rate + 3.2 b) Predicted VO2 max value (female = 0.15 optimal exercise heart rate − 2.36
The Bland–Altman analysis (Figure 1) showed that the VO2 max value derived from the prediction formula using the exercise tool has a good level of agreement with minimal bias compared with the measurement made using the gold standard.
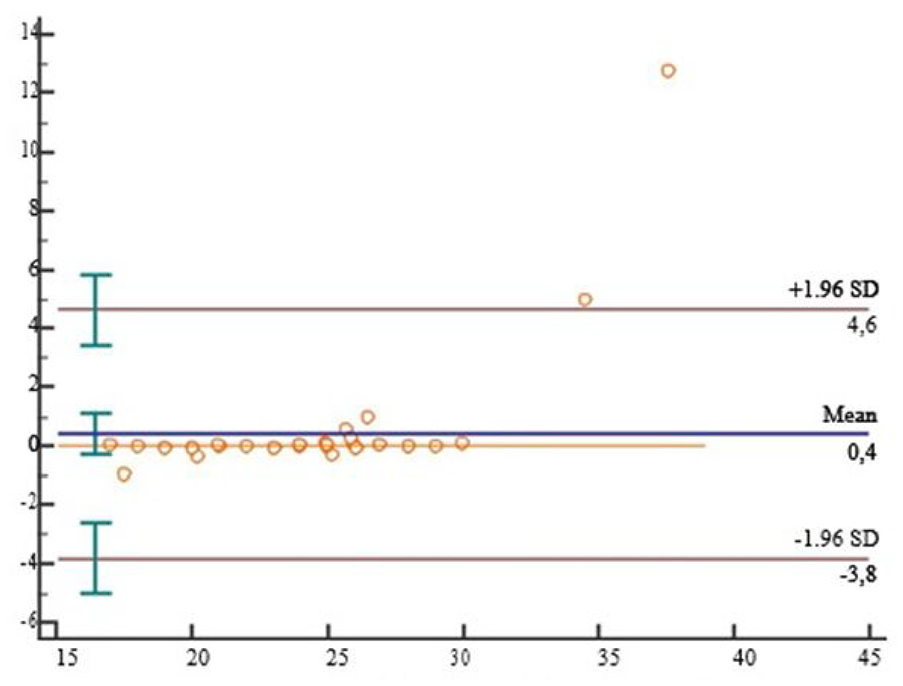
Bland–Altman plot for VO2 max value the gold standard and the predicted VO2 max value the foot rest-based cardiorespiratory exercise device model.
The average discrepancy between the methods (the bias) was close to zero (0.4 mL/kg/min), and the limits of agreement were −3.8 to 4.6, indicating that the two methods were essentially equivalent. In addition, the variability was consistent across the graph.
Discussion
In this study, the exercise tool model was compared with spiroergometry as the gold standard for measuring cardiorespiratory endurance. This comparison was done to add functions to the exercise tool model, not only as a physical exercise tool but also as an alternative measurement to predict the VO2 max value. This idea was based on the similarity of modalities and the methods of operating both tools, that is, by sitting and pedalling.
The linear regression model obtained from the measurement of cardiorespiratory endurance using the exercise tool model was able to explain 40.3% of the variation of the measured VO2 max value (R2 = 0.403; p < 0.05). In addition, sex and optimal heart rate measured during the exercise using the tool model could significantly predict the VO2 max value with p < 0.05. In this study, the load in the exercise tool model was increased gradually, starting from 25 W (female) and 50 W (male) with the addition of 25 W every 3 min.
Similar studies have been conducted using other developed exercise tool models in less mobile population or sitting workers. The results of the present study demonstrated that the predicted VO2 max value obtained from the measurement using our exercise tool model is better than those obtained in Yoopat et al. 18 study that has been conducted using similar modalities and population. They evaluated the Thai Ethics Committee volunteers in Thailand who performed the cycle ergometer exercise test and the step test and obtained the predicted VO2 max values using a linear regression analysis of the optimum heart rate response.
The results of the present study also showed no association among age, weight and BMI with the cardiorespiratory endurance represented by the VO2 max value measured using the exercise tool model (p > 0.05). A similar result has also been reported in some studies. 18 Hosseini et al. 19 study evaluated workers in Tehran, Iran, using the indirect measurement method in the form of step test and Tuxworth and Shahnawaz method, which also did not indicate a relationship of the mean predicted VO2 max value with age, weight and BMI. Furthermore, the optimal heart rate and gender were observed to have a significant association with the VO2 max value measured using the prototype tool model (p < 0.005). The gender effect was because the body composition in men is significantly greater than that in women; anatomically, the male chest and lung cavities are larger so that their lung capacity and the resulting VO2 max value could be higher.
Despite the advantage of this study in finding the predicted VO2 max formulae using the simple prototype device, the limitation is the research has not identified the safety aspects of this tool as the physical exercise device yet.
Conclusion
The cardiorespiratory exercise tool model developed in this study was valid for measuring cardiorespiratory endurance in the form of the predicted VO2 max value. This tool may be useful for improving the physical fitness level of sitting workers, and further study is necessary.
Footnotes
Acknowledgements
We (the authors) express our gratitude to the Universitas Indonesia staff for their valuable support for participating in this study as study subjects. The model of foot rest-based exercise has been registered as Kinesia®.
Author’s Note
Muchtaruddin Mansyur is currently affiliated with SEAMEO-RECFON/Regional Research Center for Food & Nutrition, Universitas Indonesia, Jakarta, Indonesia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a final assignment from the Universitas Indonesia doctoral students in the fiscal year 2019 [grant number NKB-0122/UN2.R3.1/HKP.05.00/2019].
Ethics approval
Ethical approval for this study was obtained from the Health Research Ethics Committee of the Faculty of Medicine, Universitas Indonesia, No: 0014/UN2.F1/ETIK/2018 (protocol no. 18-01-0017).
Informed consent
Written informed consent was obtained from all subjects before the study.