
Abstract
Acquired brain injury (ABI) affects the whole family unit, significantly shifting family roles and relationships, with communication disabilities associated with ABI further compounding these difficulties. Family therapy is offered in situations where family roles have been disrupted, but research on the application of family therapy to families affected by ABI has not been synthesized. This study systematically maps the research on the use of family therapy for people with ABI, identifying to what extent people with communication disabilities (PWCD) are included in the evidence base. A scoping review of primary research was conducted through a systematic search of five multidisciplinary academic databases. A consultation process, involving a person with aphasia, ran alongside the entire research process. Twenty-four studies were included in the final review with four categories of interventions identified. Twelve studies excluded PWCD, 10 potentially doing so due to the communication demands of the study. Twelve studies included PWCD, five of which included speech and language therapists to support the delivery of family therapy. A small evidence base exists for the use of family therapy within an ABI population. However, PWCD are frequently excluded from this research due to the communication demands of the study designs. More research is needed to guide appropriate intervention for PWCD.
Acquired brain injury (ABI) affects the whole family unit, not just the individual (Dawes et al., 2022). ABI can significantly shift family roles and relationships causing an intense effect on emotional, mental, and social well-being within the family system (McDermott & McDonnell, 2013). These difficulties are likely to be compounded where the ABI is associated with a communication disability. Communication disability is defined as an impairment in the functions of speech, language, or cognition, which affects a person’s ability to understand others or to be understood by others (adapted from Washington Group on Disability Statistics, 2016). Communication is one of the core components of family life, with family functioning being reliant on the successful communication of emotions and information. Therefore, disruptions to this communicative process affect how relatives interact with one another (Olson & Gorall, 2003).
Impact of ABI on Family Life
Family members play a crucial role in assisting and aiding their loved ones after an ABI. They often provide emotional care and support for the psychosocial aspects of ABI (Klonoff, 2014). When a person sustains an ABI, families encounter a multitude of difficulties throughout each stage of recovery. It can have an intense effect on the immediate and extended family unit and has substantial consequences on emotional, mental, and social well-being within the family system (McDermott & McDonnell, 2013). Family members may be required to take on new roles such as assisting the person with ABI to complete daily activities and providing financial support (Larøi, 2003). These changes are an important consideration as family is structured around the assistance, management, care, and socialization of each individual in the unit (Galvin et al., 2016). Unfortunately, emotional support is often not available for people with ABI or their family (Larøi, 2003).
Research on the impact of ABI on families has primarily concentrated on primary caregivers. The limited research which has been conducted on children of parents with ABI has shown that children have increased emotional and behavioral difficulties. Children have identified feelings of grief, loss, and worries surrounding familial breakdown, while also having additional responsibilities and independence. They often find it difficult to process and manage these emotions (Charles et al., 2007). Families have identified disparities in supports offered after ABI (Dawes et al., 2022), and affected families have emphasized the necessity of emotional support such as family support groups or family therapy (Bellon et al., 2015).
As family life is based on communication, roles are discussed and negotiated between family members. Disruptions to this communicative process affect how relatives interact with one another (Olson & Gorall, 2003). The limited literature exploring acquired communication disabilities and family relationships focuses on aphasia. Aphasia is a communication disability, primarily caused by stroke, that affects language comprehension and expression, which may impact a person’s interactions, relationships, and quality of life (Berg et al., 2022). For example, people with aphasia often experience adjustments to their role as a parent. The role of parenting is reliant on parent–child communication (Cava et al., 2014; Levin et al., 2012; Romero-Abrio et al., 2019) and effective parent–child communication is associated with increased life satisfaction and emotional well-being for the entire family (Levin et al., 2012). The nature of communication disability means that parents with aphasia may have difficulty reasserting their role as a parent to support their children and alters the allocation of parenting responsibilities between the people with the communication disability (PWCD) and their partners (Manning et al., 2021). Similar difficulties in navigating other family roles may also be experienced, including the relationship between spouses (Stead & White, 2019) and adult siblings (Barrow, 2008).
Limited research in the area of family roles and communication disability has highlighted the disruption of roles within families. Family therapy has the potential to address these adjustments in roles. However, a synthesis of existing evidence is overdue.
Family Therapy
Family therapies are grounded in systems theory. A system, in the context of family, is a collection of people who each have a unique role which is sustained by their interaction with one another (Smith-Acuña, 2010). If there is a change to the structure or roles within the family, such as the impact of a traumatic event (in this case ABI), it can impact significantly on each member. In response, each person’s behavior and role may be altered, shifting the family dynamic. Consequently, intervention is required when one or more roles in the family have changed and disrupted the family dynamic (Walker & Akister, 2004).
Family therapy can occur in different formats, including therapy for the main caregiver, marriage counseling, individual family therapy (for all members), and group therapy where several families are present (Florian & Katz, 1991; Klonoff & Koberstein, 2010; Kreutzer et al., 2002; Rosenthal & Young, 1988). Family therapy is most traditionally provided by family therapists (Klonoff & Koberstein, 2010). However, in some contexts, it may be within the scope of practice for other healthcare providers to support the readjustment of roles (Hodgson et al., 2014; Marlowe, 2011; Rolland & Walsh, 2005; Tyndall et al., 2012). The involvement of speech and language therapists (SLTs) in the delivery of family therapy may be particularly relevant in the context where a family member has a significant communication disability.
To date, there has been no systematic synthesis of how family therapy interventions have been applied to an ABI population. Furthermore, it is unknown to what extent PWCD, associated with ABI, have been included in family therapy interventions. This study systematically maps the research on family therapy for people with ABI, identifying to what extent PWCD are included in the evidence base. The review was guided by the following research questions: (a) What evidence exists for the use of family therapy in an adult ABI population? and (b) are PWCD included in the evidence base?
Method
The research questions were addressed through a scoping review using the six-step framework developed by Arksey and O’Malley (2005). The broad research questions and the large amount of evidence in this area, in addition to the wide variety of variables, suggested the use of a scoping review. This methodology allowed the researchers to scope the breadth of the literature, allowing for an overview of the prominent concepts and theories that act as the foundation to a research area (Mays et al., 2001). Additionally, the evidence synthesis that is the result of a scoping review can inform both evidence-based practice and clinical practice (Gough et al., 2020).
First, the six-step framework began with “identifying the research question,” as the research questions directed the manner in which search strategies were created. Second, “identifying relevant studies” involved finding research which appropriately addressed the research questions. This step required the identification of key databases and the generation of search strategies to find relevant studies. Third, “study selection” comprised identifying inclusion and exclusion criteria which enabled the exclusion of research which did not answer the research questions. The fourth step involved “charting the data” by synthesizing the results according to key information presented in each study. The fifth step, “collating, summarizing, and reporting the results,” provided readers with a narrative overview of the results. Finally, an optional sixth step of a “consultation process” utilizing stakeholder groups to provide professional experience was adapted and used (Arksey & O’Malley, 2005). Further details on how these steps were carried out are described in each section below.
Additionally, the PRISMA-ScR guidelines (a 20-step checklist detailing reporting steps for scoping reviews) were consulted and reported against in this research. These guidelines aim to provide methodological transparency and replicability (Tricco et al., 2018).
Consultation Process
The optional consultation process used in this research was not the traditional broad stakeholder group as described by Arksey and O’Malley (2005). Instead, consultation was sought and received from a co-researcher who is a psychologist and has aphasia post-ABI. The inclusion of a researcher with professional and living experience in this research area affords an opportunity for a unique perspective to be included. Consequently, this method ensures that research is both relevant and meaningful to those whom it is centered on (Hersh et al., 2021). The co-researcher was involved throughout the entire scoping review process. Starting with the question formulation, the co-researcher provided a degree of initial consultation, acting as a sounding board and describing their own experience of a communication disability and role changes within their family system. Once the research questions had been formulated, the co-researcher completed title/abstract screening and piloting data extraction forms with the primary researcher. As the co-researcher is an expert in their own right in this area, they were consulted during the results and discussion sections to provide a unique and personal insight. Finally, the co-researcher was consulted about directions for future research to highlight the issues that PWCD may face when accessing these interventions.
Identifying Relevant Studies
In accordance with the PRISMA-ScR guidelines, search strings were developed to identify significant evidence and articles related to the research questions (Tricco et al., 2018). The initial search string was devised with the assistance of a subject librarian and was comprised of title/abstract keywords and controlled vocabulary. The search strings were piloted and modified using key concepts from the research questions (e.g., family therapy, brain injury, etc.). To ensure that any papers focusing on communication diagnoses associated with ABI were not missed, the three most common diagnoses were included in the search strings, namely: aphasia, dysarthria, and cognitive communication disorders.
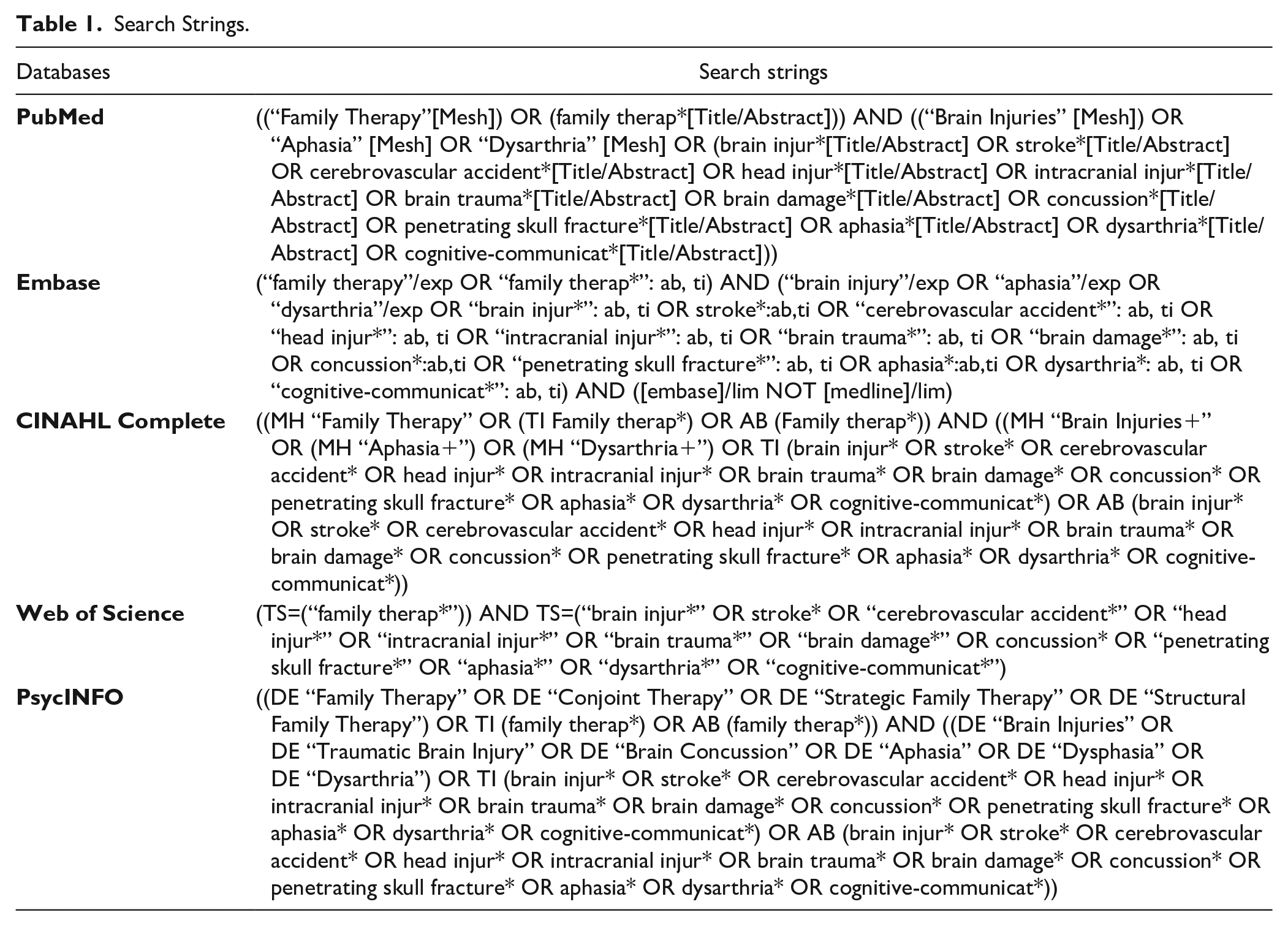
Searches were completed across five databases (PubMed, Embase, CINAHL Complete, Web of Science, and PsycINFO), reflecting the multidisciplinary nature of the research questions. All published articles were included with no restrictions on publication date. The final search strings for each database are shown in Table 1.
Search Strings.
Study Selection
The final search was completed on October 5, 2021. The search results were imported to the systematic review manager Covidence (2021), and duplicates were removed. Title and abstract screening was conducted by reading through all abstracts and assessing their relevance in relation to the inclusion and exclusion criteria (see Table 2). To ensure replicability, 10% (n = 52) of the articles were also screened by a co-researcher. No disagreements occurred.
Inclusion and Exclusion Criteria for Scoping Review.
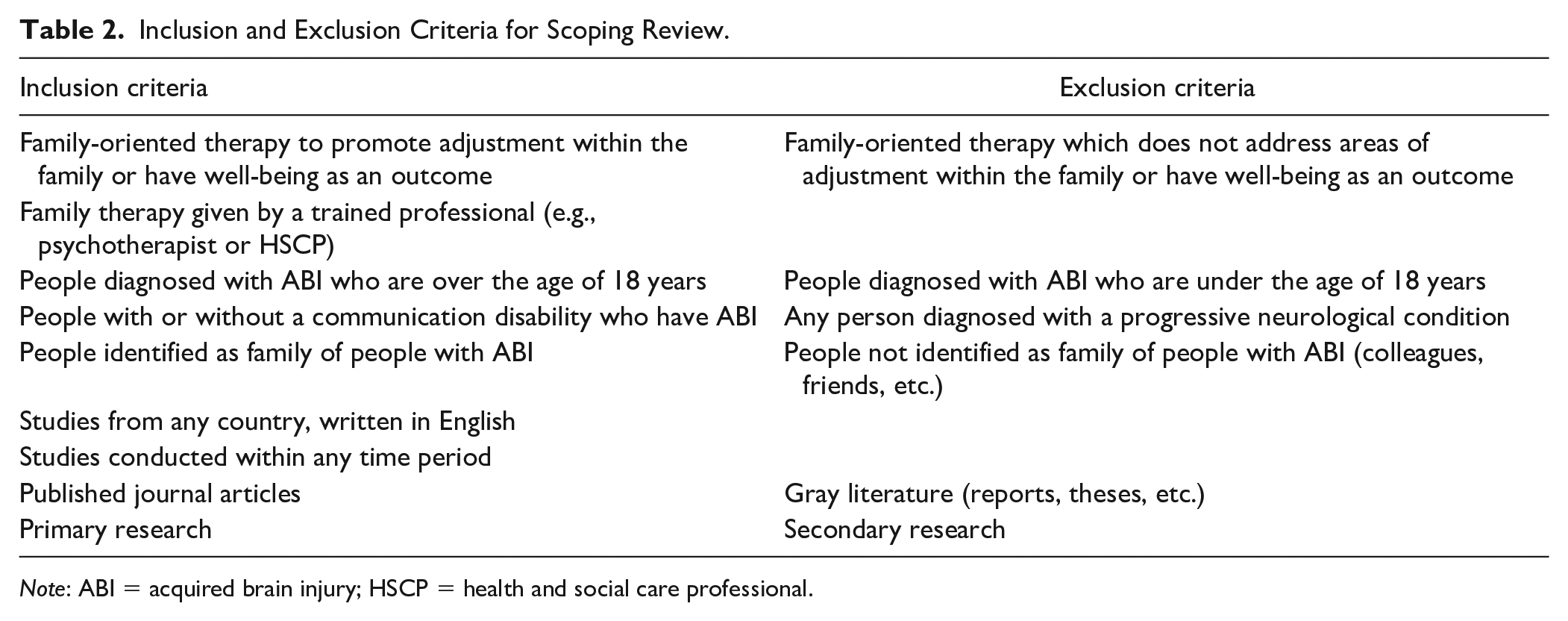
Note: ABI = acquired brain injury; HSCP = health and social care professional.
Study participants had to meet the criteria of (a) an adult with a diagnosis of ABI or (b) people identified as family of people with an ABI. Studies that included people with a progressive neurological condition were excluded. For the purposes of this study, an adult with ABI was defined as above the age of 18, but family members could be of any age (see Table 2). Interventions within the area of family-oriented therapy, whether given by a trained family therapist or given by another healthcare professional, were included in the review (see Table 2). Articles that reported on outcome data, such as well-being or adjustment within the family as a result of family therapy, were included (see Table 2).
The screened articles were subjected to full-text screening to decide whether they met the inclusion criteria for the review. Full-text articles that met the eligibility criteria were included in the final review. To locate articles not found in the initial search, all reference lists of articles included in the final review were manually searched. This was completed by reading each article title and using inclusion/exclusion criteria to assess its suitability for inclusion. No additional articles were identified through reference list searching.
Charting the Data
This stage of the scoping process required the extraction and charting of significant areas of data from articles that were included in the final review. The researcher developed a data extraction form a priori. Two members of the research team trialed the data extraction form using 25% (n = 6) of the articles, to assess its suitability to answer the research questions (Daudt et al., 2013; Levac et al., 2010). Each article was picked in random order and the data was extracted according to the sequence outlined on the data extraction form. No adjustments were made following the piloting of the form.
The data extraction form organized the data according to central themes. A narrative review approach was used for synthesis, as it allowed the researcher to note information about the process of an intervention, so context could be provided when describing the outcome (Arksey & O’Malley, 2005). The data extracted from each article included:
I. Study characteristics (Author(s), year of publication, study location, study design, aims, methodology, language, no. of participants, age, and gender);
II. Intervention and outcomes (Intervention type, focus of the intervention, frequency of sessions, professions delivering the intervention, study populations, outcome measures, and intervention outcomes);
III. Presence/absence of PWCD (Nature and severity of communication disability, and rationale for inclusion/exclusion of PWCD).
To ensure that the presence or absence of PWCD was accurately recorded for each study, the use of three labels, similar to the ones used by Jagoe et al. (2021), was considered. The label “included” was used when a study explicitly stated that PWCD were involved. Second, “excluded” was utilized when a study explicitly stated the exclusion of PWCD. For studies that did not explicitly state the exclusion of PWCD, but where a critical review of the communication demands in the study implied that they were likely to be excluded, the label “potentially excluded due to the communication demands of the study” was used.
Collating, Summarizing, and Reporting the Results
This step involved organizing, summarizing, and discussing the results (Arksey & O’Malley, 2005). First, a quantitative analysis of the amount, description, and distribution of the evidence was collated. Second, a synopsis of all the studies reviewed was created. Third, evidence was reported according to the types of therapy intervention, the professionals providing the therapy, and the outcomes of the intervention.
Findings
The search process identified 668 articles through electronic database search, with 516 articles remaining after de-duplication. In total, 24 studies met the criteria for inclusion in the scoping review (see Figure 1).
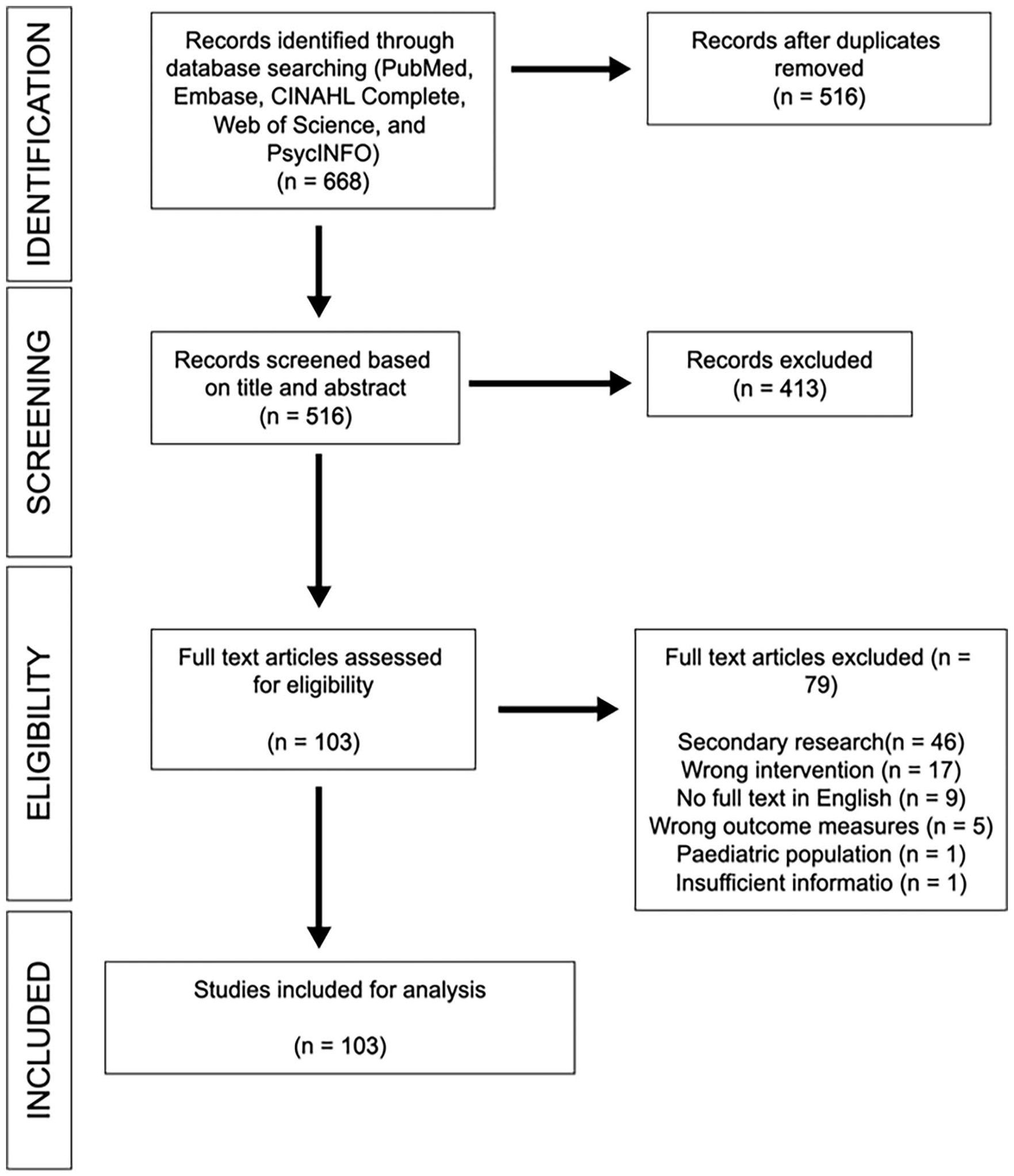
PRISMA Diagram.
Study Characteristics
The 24 studies were published between 1952 and 2019. The articles were published across four countries: 58.3% (n = 14) in the United States, 20.8% (n = 5) in Australia, 12.5% (n = 3) in Sweden, and 8.3% (n = 2) in the United Kingdom (see Figure 2). The majority of articles had a case study design (n = 15; 62.5%), followed by mixed methods (n = 3; 12.5%), and then focus groups (n = 2; 8.3%). The remaining four articles had differing study designs (n = 4; 16.7%) which included a randomized control trial, a time series, a qualitative descriptive study, and a pilot study (see Figure 3). All the articles were written in English with the majority of interventions being conducted through English too. Swedish was used as the main language for intervention in three studies (Studies 2, 5, and 21; see Appendix). One study did not report the number of people participating in the intervention with the remaining studies reporting between 2 and 152 participants.

Distribution of Studies Across Countries.
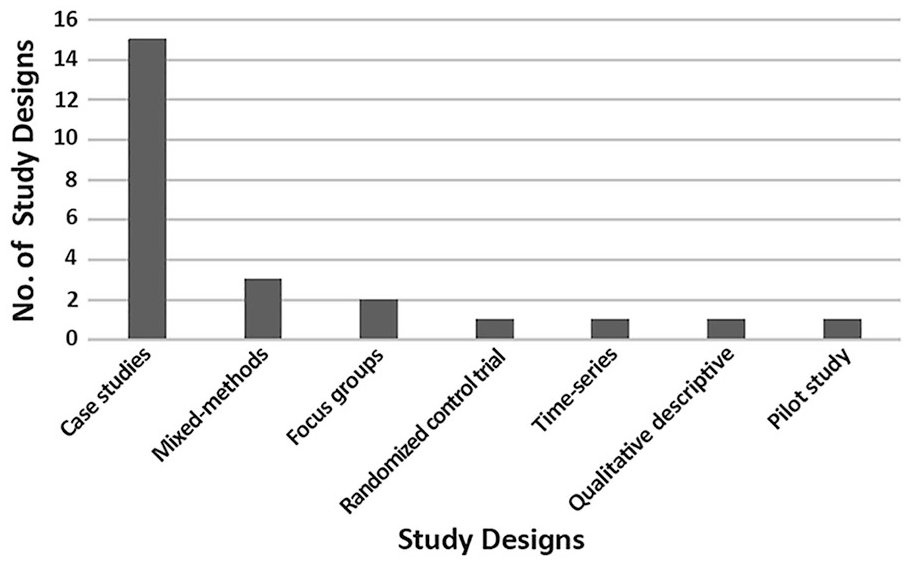
Study Designs.
Family Therapy Interventions
The included articles in this review centered on four main types of family therapy interventions for people with ABI and their family, namely: psychoeducation (n = 4; 16.7%), traditional family therapy (n = 8; 33.3%), family therapy adapted for people with ABI (n = 10; 41.7%), and psychosocial interventions (n = 2; 8.3%).
Psychoeducation Interventions (Studies 1–4):
provided information on the nature and rehabilitation process of ABI including acquired communication disorders associated with ABI (see Appendix). These studies provided emotional support to deal with adjustment of roles and responsibilities and to improve family functioning. Professionals who were involved in delivering this style of intervention included: joint working between a psychologist and SLT (Study 1), an SLT working independently (Study 2), a social worker working independently (Study 3), and a multidisciplinary team (Study 4; see Table 3). The frequency of sessions was recorded in three of the studies (Studies 2–4). The frequency ranged from weekly sessions over 6 weeks (Study 2), to 3 sessions over 5 months (Study 3), and bimonthly sessions over 5 months (Study 4). Outcome measures used included: self-reported measures (Study 1), the McMaster Family Assessment Device (Epstein et al., 1983) (Study 3), and questionnaires (Studies 2 and 4). These four studies showed improvements in the participants’: (a) awareness of the impact of ABI and communication disabilities (Studies 2 and 4); (b) understanding of family roles and responsibilities (Studies 1–3); (c) ability to advocate for family members with ABI (Study 4); (d) ability to recognize the importance of emotional support during this time (Studies 2 and 4); and (e) attitudes toward healthcare professionals (Study 4). One of the studies reported a reduction in feelings of anxiety and guilt associated with ABI (Study 1). Another study showed that family therapy had no substantial effects on depression for the person with ABI (Study 3; see Appendix).
Range of Professionals Delivering Family Therapy.
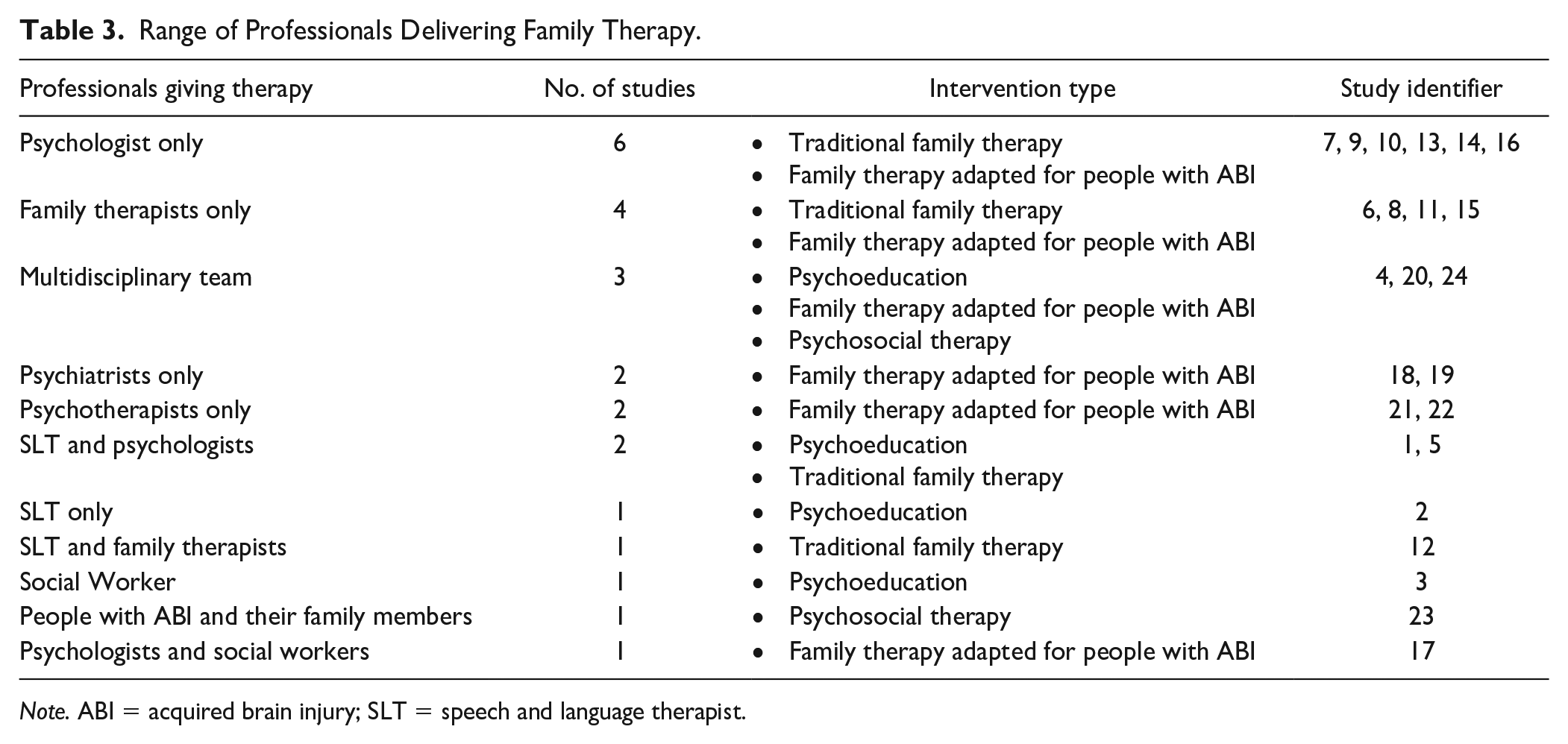
Note. ABI = acquired brain injury; SLT = speech and language therapist.
Traditional family therapy interventions (Studies 5–12):
enabled people with ABI to acknowledge their injury, educated their family on the injury, improved interpersonal relationships within the family, and identified and redefined roles and responsibilities. Additionally, these studies explored the shifts in relationships caused by ABI and aphasia and provided skills to cope with these shifts (see Appendix). Professionals who were involved in delivering traditional family therapy included: joint working between a psychologist and SLT (Study 5), a family therapist working independently (Studies 6, 8, and 11), a psychologist working independently (Studies 7, 9, and 10), and joint working between a family therapist and SLT (Study 12; see Table 3). The frequency of sessions was recorded in six of the studies (Studies 5, 6, 8, 9, 11, and 12). There were a range of frequency of sessions which included: a 5-day course (Study 5), unlimited sessions for the duration of the research (Studies 6 and 8), biweekly sessions over 12 months (Study 9), 21 sessions over 9 months (Study 11), and 5 therapy sessions over the study period (Study 12; see Appendix). Outcome measures used to evaluate intervention efficacy included: self-reported outcomes (Studies 7–11), questionnaires (Studies 5 and 12), and the Family Environment Scale (Moos & Moos, 1981) (Study 6). Traditional family therapy: (a) improved quality of life, family cohesion, negotiation of parental roles/experiences, emotional skills, sense of pride and accomplishment with hope for the future (Studies 5–10) and (b) reduced distress, caregiver burden, and family conflict (Studies 6, 11, and 12; see Appendix).
Family therapy adapted for people with ABI (Studies 13–22):
provided psychological support to manage the effects of ABI, improved communication within families across all levels of interaction, and helped the family to adjust their expectations of roles and responsibilities. Professionals who were involved in delivering family therapy adapted for people with ABI included: a psychologist working independently (Studies 13, 14, and 16), a family therapist working independently (Study 15), joint working between psychologists and social workers (Study 17), a psychiatrist working independently (Studies 18 and 19), a multidisciplinary team (Study 20), and a psychotherapist working independently (Studies 21 and 22; see Table 3). The frequency of sessions was recorded in seven of the studies (Studies 13, 14, and 16–20). There were a range of frequency of sessions which included: biweekly sessions over 10 weeks (Study 13), weekly sessions over 12 weeks (Study 14), 5 sessions over the duration of the study (Study 16), 20 sessions over 2 years (Study 17), bimonthly sessions over 9 months (Study 18), 3 sessions over the duration of the study (Study 19), and unlimited sessions over 7 months (Study 20; see Appendix). Outcome measures utilized involved: self-reported outcomes (Studies 15–17, 20, and 22), focus groups (Studies 14 and 19), the Family Empowerment Scale (Koren et al., 1992) (Study 18), and questionnaires (Studies 13 and 21). These studies showed that: (a) patients and caregivers benefited from these interventions (Studies 13–22); (b) there were improvements in the negotiation and reclamation of familial roles and responsibilities, and improved success, pride, and empowerment (Studies 14–18 and 21); (c) there was increased acceptance of the effects of ABI (Study 20); and (4) there was reduced conflict, caregiver burden, and isolation (Studies 14 and 17–19). Overall, these interventions greatly improved the participant’s quality of life.
Psychosocial therapy interventions (Studies 23 and 24):
focused on community support for people with ABI and their families and strengthening romantic relationships. Professionals involved in delivering psychosocial therapy included: people with ABI and their family members (Study 23), and a multidisciplinary team (Study 24; see Table 3). The frequency of sessions varied from unlimited sessions over 1 year (Study 23), to 15 sessions over 24 weeks (Study 24). Outcome measures addressing these aims included retrospective structured interviews (Study 23) and self-reported outcomes (Study 24). The outcomes of these interventions demonstrated: (a) an increased knowledge of the effects of ABI (Studies 23 and 24); (b) an improved quality of life, family mood, and cohesion (Study 23); (c) increased pride in accomplishments (Study 24); and (d) strengthened bond between couples, increasing their affection and appreciation of one another (Study 23; see Appendix).
Communication Disabilities and Family Therapy
PWCD were included in 50% (n = 12) of the studies (1, 2, 4, 5, 9, 12, 15–17, and 20–22). Aphasia was the most common communication disability present in the studies, with 29.3% (n = 7 of the 24 studies) of all the studies including people with aphasia (Studies 1, 2, 5, 12, 17, 20, and 21). The study designs which included people with aphasia were case studies or time-series designs. These studies delivered psychoeducation (n = 2), traditional family therapy (n = 2), and family therapy adapted for people with ABI (n = 3). People with dysarthria were included in 8.3% (n = 2 of the 24 studies) of the studies (Studies 16 and 22). These studies were case study designs and delivered family therapy adapted for people with ABI. People with cognitive communication disorders were included in one study with a case study design and delivered family therapy adapted for people with ABI (Study 9). One study included people with aphasia, dysarthria, and cognitive communication disorders (Study 15) and utilized a mixed-method study design. This study delivered family therapy adapted for people with ABI. Another study explicitly stated the inclusion of people with any communication disability (Study 4; see Figure 4). Using a case study methodology, this research provided psychoeducation as its intervention to support families post-ABI.

Types of Communication Disabilities Represented in Study Participants/Focus.
This scoping review identified that half of the total studies (n = 12) did not include PWCD, with 2 studies explicitly excluding these participants (Studies 3 and 24) and 10 studies potentially excluding this cohort due to the communication demands of the study (Studies 6–8, 10, 11, 13, 14, 18, 19, and 23). The study designs employed were case studies (n = 5), mixed-method design (n = 3), focus groups (n = 2), pilot studies (n = 1), and a randomized control trial (n = 1). The majority of these interventions utilized traditional family therapy (n = 5), followed by family therapy adapted for people with ABI (n = 4), psychosocial interventions (n = 2), and psychoeducation (n = 1).
Discussion
The aim of this scoping review was to systematically map the research that has been conducted on family therapy in the context of ABI, identifying the extent to which PWCD are included in the evidence base. This review highlights how the specific needs of those who have communication disabilities are underrepresented in the literature, thereby risking inequality of evidence-based care.
The scoping review process identified 24 studies providing family therapy for families where one person has ABI. Despite the prevalence of communication disability after ABI, half of the studies did not include families where one member had a communication disability. Only two of these studies explicitly reported the exclusion of PWCD (Clark et al., 2003; Glass et al., 2000). The remaining 10 studies were recorded as potentially excluding PWCD due to the communication demands of the study, thereby supporting the assertion that there remains a lack of evidence-based psychological interventions for PWCD (Baker et al., 2019). These findings also resonate with Townend et al.’s (2007) results which found that only 3% of studies using interventions to address stroke and depression explicitly stated the exclusion of people with aphasia.
Overall, the studies reported that participants’ quality of both personal and family life was improved post-intervention. The majority of outcome measures used in the studies were self-reported outcomes from either participants or clinicians. When formal measures were utilized in the studies, there was variability in the type of measures used. Consequently, it was difficult to draw similarities and differences between studies. Reporting of the inclusion or exclusion of PWCD in family therapy research should be clearer, with disaggregated data provided within published articles to increase the generalizability of the results. Providing this type of data will support the application of these results to clinical practice with PWCD.
There were a wide range of professionals who delivered family therapy interventions for people with ABI, with psychologists and family therapists delivering the majority of interventions. While half of the studies included PWCD, only five studies included an SLT (Blom Johansson et al., 2013; Borenstein et al., 1987; Lauer-listhaus, 1991; Nichols et al., 1996; Turnblom & Myers, 1952), with one study involving an SLT delivering the intervention independently (Blom Johansson et al., 2013). Where SLTs were involved in family therapy including PWCD, the studies reported on the use of specific interventions which did not solely rely on verbal communication for participation. The dearth of SLTs included in this research process may be attributed to a lack of understanding of their role by other healthcare professionals. This gap in SLT involvement has been recognized in the literature addressing the role of SLTs in palliative care (Hawksley et al., 2017), dementia care, (Dooley & Walshe, 2020), and the collaboration of educational psychologists and SLTs (Dunsmuir et al., 2006), suggesting that this issue is prevalent across a range of multidisciplinary contexts.
Implications for Practice
Families of PWCD are entitled to the same high-quality therapy as any other family. The communication barriers in these instances may necessitate the involvement of SLTs (Sekhon et al., 2015), a collaborative practice that is underrepresented in the literature reported in this scoping review. Existing research in the field of neurorehabilitation suggests that coworking is a productive way to engage people post-ABI as they work toward meaningful goals (Clarke & Forster, 2015). Similar principles could be applied, whereby family therapists and SLTs work together to deliver family therapy to PWCD.
Limitations and Future Research
The methodology used for this research was a scoping review, meaning that the study is limited in the evaluation of the quality of included papers. In addition, limiting the search to publications in the English language may have excluded other relevant literature. Research in the area of family therapy and ABI should purposively include PWCD, given the frequency of communication disability after brain injury. To achieve inclusion, communication-accessible research practices are required (Dee-Price et al., 2020; Jagoe et al., 2023; Luck & Rose, 2007; Shiggins et al., 2022). Future research should publish disaggregated data which includes reporting of the outcomes of interventions that are specific to PWCD. This transparency in outcomes could then be applied to clinical practice with PWCD. Establishing core outcome measures related to family therapy outcomes, including patient-reported outcome measures that are appropriate for PWCDs, is an important step that would allow a more robust comparison of studies and decisions about best practice in relation to family therapy and PWCD.
Conclusion
This scoping review has identified that a small evidence base exists for the use of family therapy after ABI. The studies included in this review demonstrated that people with ABI and their family members can benefit from family therapy. However, the paucity of research on the use of family therapy with PWCD after ABI, risks creating or perpetuating an inequality of evidence-based care, when compared with people with ABI without a communication disability. Research that is representative of PWCD is an imperative if equal access to interventions is to be achieved.
Footnotes
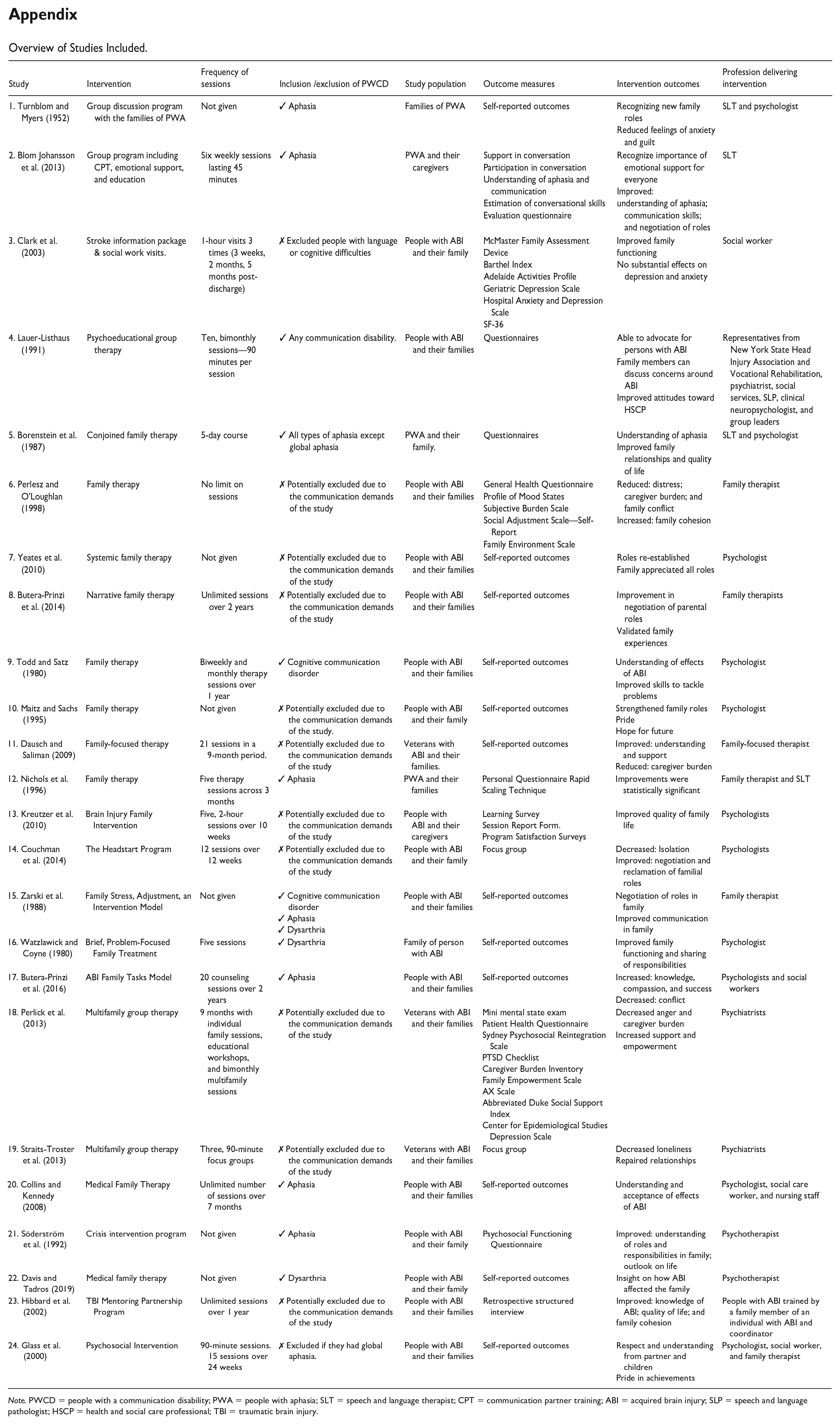
Appendix
Overview of Studies Included.
| Study | Intervention | Frequency of sessions | Inclusion /exclusion of PWCD | Study population | Outcome measures | Intervention outcomes | Profession delivering intervention |
|---|---|---|---|---|---|---|---|
| 1. Turnblom and Myers (1952) | Group discussion program with the families of PWA | Not given | ✓ Aphasia | Families of PWA | Self-reported outcomes | Recognizing new family roles Reduced feelings of anxiety and guilt |
SLT and psychologist |
| 2. Blom Johansson et al. (2013) | Group program including CPT, emotional support, and education | Six weekly sessions lasting 45 minutes | ✓ Aphasia | PWA and their caregivers | Support in conversation Participation in conversation Understanding of aphasia and communication Estimation of conversational skills Evaluation questionnaire |
Recognize importance of emotional support for everyone Improved: understanding of aphasia; communication skills; and negotiation of roles |
SLT |
| 3. Clark et al. (2003) | Stroke information package & social work visits. | 1-hour visits 3 times (3 weeks, 2 months, 5 months post-discharge) | ✗ Excluded people with language or cognitive difficulties | People with ABI and their family | McMaster Family Assessment Device Barthel Index Adelaide Activities Profile Geriatric Depression Scale Hospital Anxiety and Depression Scale SF-36 |
Improved family functioning No substantial effects on depression and anxiety |
Social worker |
| 4. Lauer-Listhaus (1991) | Psychoeducational group therapy | Ten, bimonthly sessions—90 minutes per session | ✓ Any communication disability. | People with ABI and their families | Questionnaires | Able to advocate for persons with ABI Family members can discuss concerns around ABI Improved attitudes toward HSCP |
Representatives from New York State Head Injury Association and Vocational Rehabilitation, psychiatrist, social services, SLP, clinical neuropsychologist, and group leaders |
| 5. Borenstein et al. (1987) | Conjoined family therapy | 5-day course | ✓ All types of aphasia except global aphasia | PWA and their family. | Questionnaires | Understanding of aphasia Improved family relationships and quality of life |
SLT and psychologist |
| 6. Perlesz and O’Loughlan (1998) | Family therapy | No limit on sessions | ✗ Potentially excluded due to the communication demands of the study | People with ABI and their families | General Health Questionnaire Profile of Mood States Subjective Burden Scale Social Adjustment Scale—Self-Report Family Environment Scale |
Reduced: distress; caregiver burden; and family conflict Increased: family cohesion |
Family therapist |
| 7. Yeates et al. (2010) | Systemic family therapy | Not given | ✗ Potentially excluded due to the communication demands of the study | People with ABI and their families | Self-reported outcomes | Roles re-established Family appreciated all roles |
Psychologist |
| 8. Butera-Prinzi et al. (2014) | Narrative family therapy | Unlimited sessions over 2 years | ✗ Potentially excluded due to the communication demands of the study | People with ABI and their families | Self-reported outcomes | Improvement in negotiation of parental roles Validated family experiences |
Family therapists |
| 9. Todd and Satz (1980) | Family therapy | Biweekly and monthly therapy sessions over 1 year | ✓ Cognitive communication disorder | People with ABI and their families | Self-reported outcomes | Understanding of effects of ABI Improved skills to tackle problems |
Psychologist |
| 10. Maitz and Sachs (1995) | Family therapy | Not given | ✗ Potentially excluded due to the communication demands of the study. | People with ABI and their family | Self-reported outcomes | Strengthened family roles Pride Hope for future |
Psychologist |
| 11. Dausch and Saliman (2009) | Family-focused therapy | 21 sessions in a 9-month period. | ✗ Potentially excluded due to the communication demands of the study | Veterans with ABI and their families. | Self-reported outcomes | Improved: understanding and support Reduced: caregiver burden |
Family-focused therapist |
| 12. Nichols et al. (1996) | Family therapy | Five therapy sessions across 3 months | ✓ Aphasia | PWA and their families | Personal Questionnaire Rapid Scaling Technique | Improvements were statistically significant | Family therapist and SLT |
| 13. Kreutzer et al. (2010) | Brain Injury Family Intervention | Five, 2-hour sessions over 10 weeks | ✗ Potentially excluded due to the communication demands of the study | People with ABI and their caregivers | Learning Survey Session Report Form. Program Satisfaction Surveys |
Improved quality of family life | Psychologists |
| 14. Couchman et al. (2014) | The Headstart Program | 12 sessions over 12 weeks | ✗ Potentially excluded due to the communication demands of the study | People with ABI and their family | Focus group | Decreased: Isolation Improved: negotiation and reclamation of familial roles |
Psychologists |
| 15. Zarski et al. (1988) | Family Stress, Adjustment, an Intervention Model | Not given | ✓ Cognitive communication disorder ✓ Aphasia ✓ Dysarthria |
People with ABI and their families | Self-reported outcomes | Negotiation of roles in family Improved communication in family |
Family therapist |
| 16. Watzlawick and Coyne (1980) | Brief, Problem-Focused Family Treatment | Five sessions | ✓ Dysarthria | Family of person with ABI | Self-reported outcomes | Improved family functioning and sharing of responsibilities | Psychologist |
| 17. Butera-Prinzi et al. (2016) | ABI Family Tasks Model | 20 counseling sessions over 2 years | ✓ Aphasia | People with ABI and their families | Self-reported outcomes | Increased: knowledge, compassion, and success Decreased: conflict |
Psychologists and social workers |
| 18. Perlick et al. (2013) | Multifamily group therapy | 9 months with individual family sessions, educational workshops, and bimonthly multifamily sessions | ✗ Potentially excluded due to the communication demands of the study | Veterans with ABI and their families | Mini mental state exam Patient Health Questionnaire Sydney Psychosocial Reintegration Scale PTSD Checklist Caregiver Burden Inventory Family Empowerment Scale AX Scale Abbreviated Duke Social Support Index Center for Epidemiological Studies Depression Scale |
Decreased anger and caregiver burden Increased support and empowerment |
Psychiatrists |
| 19. Straits-Troster et al. (2013) | Multifamily group therapy | Three, 90-minute focus groups | ✗ Potentially excluded due to the communication demands of the study | Veterans with ABI and their families | Focus group | Decreased loneliness Repaired relationships |
Psychiatrists |
| 20. Collins and Kennedy (2008) | Medical Family Therapy | Unlimited number of sessions over 7 months | ✓ Aphasia | People with ABI and their families | Self-reported outcomes | Understanding and acceptance of effects of ABI | Psychologist, social care worker, and nursing staff |
| 21. Söderström et al. (1992) | Crisis intervention program | Not given | ✓ Aphasia | People with ABI and their family | Psychosocial Functioning Questionnaire | Improved: understanding of roles and responsibilities in family; outlook on life | Psychotherapist |
| 22. Davis and Tadros (2019) | Medical family therapy | Not given | ✓ Dysarthria | People with ABI and their family | Self-reported outcomes | Insight on how ABI affected the family | Psychotherapist |
| 23. Hibbard et al. (2002) | TBI Mentoring Partnership Program | Unlimited sessions over 1 year | ✗ Potentially excluded due to the communication demands of the study | People with ABI and their families | Retrospective structured interview | Improved: knowledge of ABI; quality of life; and family cohesion |
People with ABI trained by a family member of an individual with ABI and coordinator |
| 24. Glass et al. (2000) | Psychosocial Intervention | 90-minute sessions. 15 sessions over 24 weeks | ✗ Excluded if they had global aphasia. | People with ABI and their families | Self-reported outcomes | Respect and understanding from partner and children Pride in achievements |
Psychologist, social worker, and family therapist |
Note. PWCD = people with a communication disability; PWA = people with aphasia; SLT = speech and language therapist; CPT = communication partner training; ABI = acquired brain injury; SLP = speech and language pathologist; HSCP = health and social care professional; TBI = traumatic brain injury.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The first author received a monetary award, in the form of the Tavistock Trust for Aphasia Student Prize, for the dissertation on which the paper was based.