
Abstract
While the 2017 version of the Commission on Rehabilitation Counselor Certification (CRCC) Code of Ethics engrained diversity considerations across the 12 main sections of professional practice, more explicit ethical expectations related to multicultural competence are needed to govern the future of rehabilitation counseling practice. The 2023 revised CRCC Code of Ethics will include a newly added unit labeled, Section D: Multicultural Considerations, which seeks to reduce bias, minimize discrimination, and prevent harm in practice. This section infuses cultural competencies introduced to the profession and tenets of advocacy as more than just aspirational directives but also as enforceable tenets of conduct. This article provides an overview of the changes made to Section C: Advocacy and Accessibility and explains the significance of Section D across the principles that instruct professional behavior. The authors will describe best practices for operationalizing the ethics code to ensure that services are comprehensive, equitable, and inclusive. Finally, we will present strategies for becoming a culturally competent and ethically conscientious Rehabilitation Counselor.
The Commission on Rehabilitation Counselor Certification (CRCC, 2021) remains a leader in the unification of the rehabilitation counseling profession and in the standards of excellence maintained through the credentialing of certified rehabilitation counselors (CRCs). Since the inception of the CRCC in 1974, the primary mission of the assembly has been to sustain a “dedication to the excellence of rehabilitation counseling and services for individuals with disabilities by setting national standards in certification, providing leadership, education, advocacy, and supporting research” (CRCC, 2021, para 1). Over the past 20 years, CRCC has blazed a trail of accountability for rehabilitation counselors and other counseling professions, such as the American Counseling Association (Kaplan et al., 2009), through a commitment to regularly revise the professional code of ethics. Revisions to the ethics code have been conducted across five review cycles beginning in 2001. Today, CRCC assumes a decades-long history of revising the ethics code to reflect ongoing changes within the field as quintessential standards of behavior and practice.
Historical Perspectives and Milestones
Formalized codes for ethical behavior began to rise in prominence in corporations and government in the 1980s in response to increasing instances of corruption and wrongdoing on the part of such institutions. Concurrently, the first Code of Professional Ethics for CRCs was developed and administered by the CRCC in 1987. Before 2001, “the rehabilitation profession lacked a clear, normative statement elucidating appropriate, culturally competent professional conduct” (Middleton et al., 2000, p. 223). The ethics code, standards of practice, and scope of practice revealed no mention of multicultural and cross-cultural counseling issues or skills. As such, building on the work of Atkins (1988) and Arredondo et al. (1996), Middleton and colleagues presented “A Call to Action” to the CRCC and the rehabilitation counseling profession to “recognize the needs of culturally diverse consumers/clients” (Middleton et al., 2000, p. 222). Harley et al. (1996) also made the case that, by omitting multicultural considerations in previous versions of the code, the ethics code may encourage unethical behavior during engagement with culturally diverse populations. Indeed, some well-meaning professionals (Weinrach & Thomas, 1996) had expressed confusion and doubt regarding the value of the profession in promoting diversity. However, the revised ethics code of 2001 sought to address some of these concerns.
The 2010 revision included a statement on respecting diversity (A.2. The Counseling Relationship), nondiscrimination (D. The Professional Responsibility), and developmental and cultural sensitivity (I. Research and Publication). The revised ethics code of 2017 strengthened the statements regarding the rehabilitation profession’s commitment to cultural diversity and considerations. Specifically, the 2017 version (D.2. Cultural Competency/Diversity) addressed expectations regarding the need for cultural competence, adaptation of interventions, and nondiscrimination (CRCC, 2017). A review of the historical codes reveals a need for more explicit ethical expectations related to multicultural counseling competence to govern certified rehabilitation counseling practice.
Racial and Ethnic Disparities in Vocational Rehabilitation Services
The fifth revision of the ethics code began in July 2021 with the formation of an ad hoc task force of CRCs in good standing who were selected to provide recommendations for principles that communicate professional behaviors and “demonstrate beliefs, attitudes, knowledge, and skills to provide competent rehabilitation counseling services and . . . work collaboratively with a diverse group of individuals” (CRCC, 2017, p. 1). Discussions emerged among the task force members surrounding racial and ethnic health disparities concerning the gaps in services and trends of vocational outcomes for diverse consumers (Matrone & Leahy, 2005; Moore et al., 2009; Wilson, 2002). Discussions about such inequities in our backyard inspired the development of a new section of the Code that seeks to transform multicultural competencies (Arredondo et al., 1996; Atkins, 1988; Middleton et al., 2000) into enforceable standards of practice for all counselors to uphold. Decreasing the racial and ethnic disparities across acceptance, service provision, closure types, and employment outcomes (Moore et al., 2009; Wilson et al., 2001; Wilson, 2002) was a vital element of focus throughout the revision of the ethics code. The new section, along with overall revisions to the ethics code, has been generated to hold rehabilitation counselors accountable for the ongoing gaps in services to many underserved groups.
Diversity Considerations in the New Code of Professional Ethics for Rehabilitation Counselors
Through the formation of the new Section D: Multicultural Considerations and comprehensive updates to Section B: Advocacy and Accessibility, we acknowledge that the rehabilitation counseling profession, and society-at-large, is more diverse with non-White racial and ethnic groups predicted to be the new majority by 2055 (Pew Research Center, 2015). The CRCC’s willingness to spearhead this movement of operationalizing ethical responsibility of cultural competence supports the changes in the larger society. One might reflect that this illustration speaks to the fact that our society can no longer ignore systemic disparities. The new section on Multicultural Considerations is housed directly following the updated Section C: Advocacy and Accessibility. This layout and design intentionally emphasize the understanding that advocacy and social action are skills intrinsic to the multicultural counseling competencies and comprise the new standards of professional conduct (Middleton et al., 2000; Sue et al., 1992).
Streamlining Section C of the Code: Advocacy and Accessibility
The 2023 revised ethics code has extended Section C: Advocacy and Accessibility to illuminate principles of diversity, equity, and inclusion, and describe the ethical obligation of CRCs to address systemic oppression that disproportionally affects members of marginalized groups (Lund et al., 2020). Waldmann and Blackwell (2010) introduced ethical implications surrounding advocacy skills and attitudinal barriers that affect access and referral accessibility of clients. In parallel, the 2017 version of Section C articulated the three major conditions of advocacy across individual, group, institutional, and societal levels. These included (a) promoting opportunity and access, (b) improving quality of life for individuals with disabilities, and (c) removing potential barriers to the provision of or access to services (CRCC, 2017). The updated section explicitly presents the professional responsibility of CRCs to be aware of the juncture that exists between disability and social justice. Examples were deliberately integrated to highlight the scope of social justice from poverty to homelessness, trauma, and systemic racism (CRCC, 2023). Furthermore, the new section adds two additional conditions of advocacy: (d) addressing stigma, and (e) fostering systems change when appropriate (CRCC, 2023). The following discussion will summarize modifications surrounding the inclusion of affirming language, clarify ethical behaviors, and provide an elaborate description of the newly added conditions of advocacy.
Advocacy
Consistent with previous versions of the ethics code, Section C maintained the layout marked by two main subsections: (a) Advocacy, and (b) Accessibility. The revised advocacy segment has increased from seven to nine standards, labeled C.1.c. Empowering the Client, and C.1.e. Adequacy of Services. The first new standard (C.1.c. Empowering the Client) targets client autonomy and encourages rehabilitation counselors to empower clients to make informed choices in decision-making and treatment planning. Credence is given to self-advocacy as a fundamental skill to achieve maximum independence and successful vocational and independent living outcomes (Schoffstall et al., 2015). The second new standard (C.1.e. Adequacy of Services) considers the concept of distributive justice, guiding CRCs to advocate for the length and quality of service that is sufficient to meet individual client needs (CRCC, 2023). Where resources are limited or inadequate, CRCs should advocate for the tools and resources needed to deliver quality services (Tarvydas & Cottone, 2000).
Accessibility
Accessibility was originally integrated into the advocacy section during the 2010 ethics code revision. The most recent review cycle classified an additional standard that functions as a reminder of the ethical obligation to protect and promote human rights and the welfare of persons with disabilities (United Nations, 2006, art. 18) by addressing systemic barriers to fair and equitable access, participation, and inclusion into society (CRCC, 2023). The theme of inclusivity is captured across these enhancements and promotes opportunity for access, improvements to the quality of life, and the removal of barriers for individuals with disabilities to community inclusion. In addition to these new standards, amendments to Section C are summarized in Table 1 and specifically address affirming language and clarification of ethical behaviors.
Summary of Amendments to Section C: Advocacy and Accessibility.
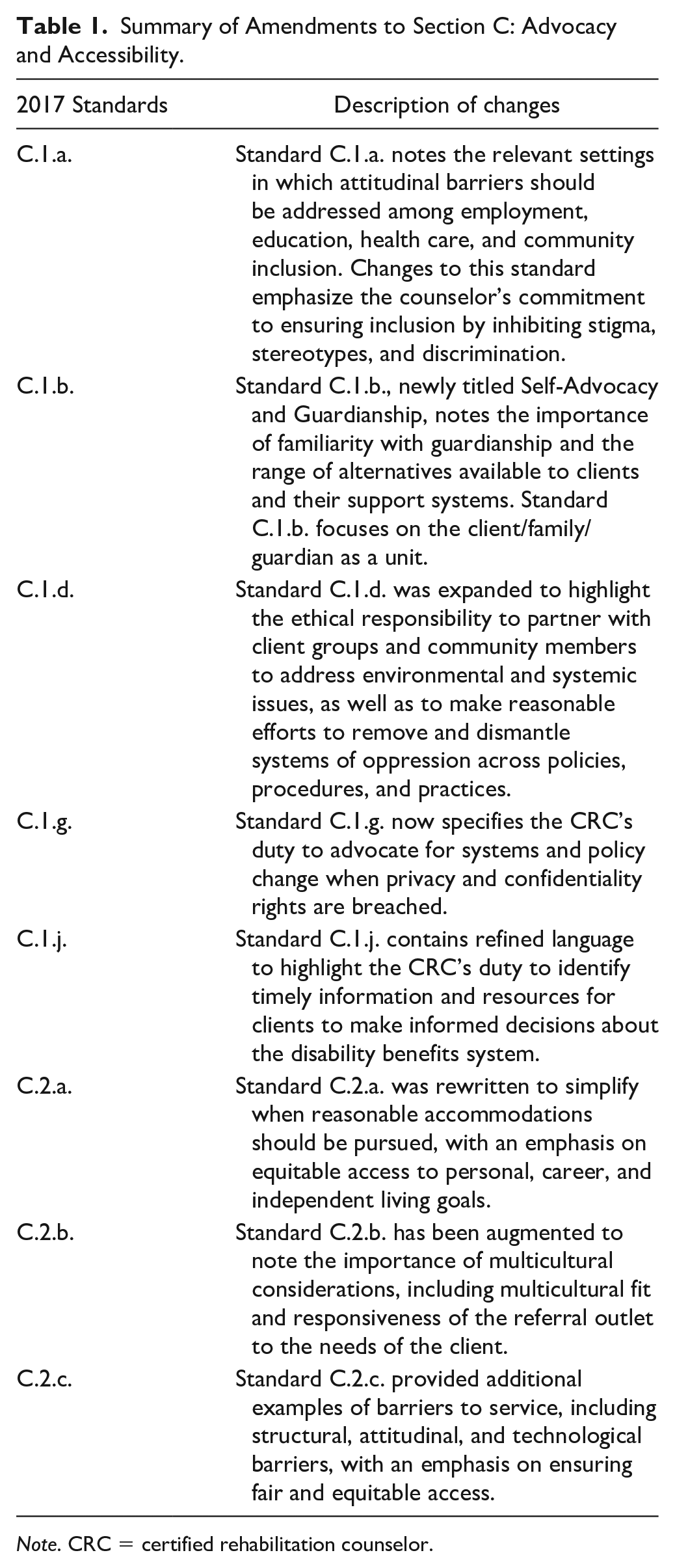
Note. CRC = certified rehabilitation counselor.
Why Section D: Multicultural Considerations, Why Now?
The foreword for Section D: Multicultural Considerations provides a comprehensive overview of counselor conduct and prioritizes multicultural competence when serving racially and ethnically diverse clients. These directives now postulate multicultural knowledge and skills as an unambiguous core value of professional conduct (CRCC, 2023). The major sentiment of the introduction outlines professional conduct that is rooted in the reduction of bias, the minimization of discriminatory practices, and the prevention of harm based on race and ethnicity (CRCC, 2023). Subsequent to the explanation of the new section, a detailed chart is offered to display how the Middleton et al. (2000) recommendations remain relevant in operationalizing these new codes.
Section D.1. Strengthening the Multicultural Counseling Relationship
The theme of Section D.1. emphasizes the impressions of diversity across the counseling relationship and guides rehabilitation counselors to honor the influences of diversity. Standard D.1.a., Establishing Constructive Multicultural Counseling Relationships, gives credence to the importance of establishing a strong working alliance with diverse clients. Lustig et al. (2002) advocated that “rehabilitation counselors may be able to improve outcomes by facilitating a strong working alliance with their clients” (p. 29), congruent with the sentiments of Bordin (1979), which highlight that the working alliance is developmental to the counseling process. Standard D.1.b., Impact of Client Intersectionality/Identity, highlights the duty of all rehabilitation counselors to consider, through continuing education and personal commitment, the intersectionality and multiple identities of the consumer. This code establishes the task of familiarizing oneself with the cultural values, attitudes, and beliefs of a consumer as a priority of professional ethical behavior.
The third standard, C.1.c. Awareness of Client Worldview, highlights the responsibility of rehabilitation counselors to advocate that the core values and assumptions of the clients are infused in practice. Furthermore, worldview and counseling, according to Ibrahim and Heuer (2016), help to reduce the “chance of oppressing the client by imposing therapist values and assumptions” (p. 54). The final standard, D.1.d. Interventions, specifies that rehabilitation counselors are expected to use, develop, or adapt interventions.
Section D.2. Avoiding Harm and Value Imposition
The second subsection communicates the expectations that all rehabilitation professionals abide by the ethical principle of nonmaleficence (to do no harm). In previous versions of the ethics code, Avoiding Value Imposition and Avoiding Harm were housed under Section A: Counseling Relationship and mentioned again in the former Section D: Professional Responsibility. Taskforce leaders felt it was important to avoid duplicity and thus value imposition was relocated to this new section.
Standard D.2.a. Avoiding Harmful Multicultural Service Provision, is the first standard under this subsection. This standard was developed to emphasize the potential adverse impacts on diverse clients when rehabilitation counselors are unaware of their attitudes, beliefs, and behaviors. The second and third standards, D.2.b. and D.2.c., address microaggressions and implicit bias in practice. It should be noted that previous versions of the ethics code do not mention the term “microaggression” across any of the ethical standards. Microaggressions were first defined by Pierce et al. (1978), a psychologist, who described the occurrences as “subtle, negative, or denigrating messages, often automatic, and nonverbal in nature” (as cited in Cartwright et al., 2009, p. 171). Furthermore, research on disability microaggressions and ableism remain prominent concerns that prevent the achievement of rehabilitation outcomes (Aydemir-Döke & Herbert, 2021). The 2017 version of the ethics code omitted the impacts of implicit bias specific to diversity, which highlighted an opportunity for the current version to explore professional standards of practice. The new ethics code highlights the responsibility of all rehabilitation counselors to make every effort to participate in self-awareness by way of supervision, consultation, and training. The final standard, D.2.d. Recognition and Respect of Client Values, summarize that, to avoid harm and value imposition, rehabilitation counselors are expected to regularly integrate the social norms of the client into the provision of services.
D.3. Personal and Professional Development and Cultural Competence
The third subsection stresses that personal and professional development and cultural competence are criteria for ethical practice. These ethical codes were developed in response to the disparities in service provision within our profession (Arredondo et al., 1996; Wilson, 2002). The significance of these codes turns what were considered suggestions of aspirational governance into enforceable tenets of professional behavior. The first and second standards, D.3.a. Personal Awareness and D.3.b. Antiracism, require that rehabilitation counselors regularly engage in personal reflection of how their cultural background and beliefs can potentially affect the working alliance (Crenshaw, 1989; Kendi, 2019). Furthermore, this code sets a professional responsibility for all counselors to assess their levels of cultural competence and continuously work to become antiracist. There are procedures in place to hold rehabilitation counselors accountable for adherence to this standard. For the first time in history, according to the ethics code, antiracism is foundational to the efficacy of the counseling relationship.
Although social justice was previously mentioned in Section B, the task force felt that moving the social justice standard to Section D set a precedence of all CRCs/CCRCs to “understand the client’s personal experience, cultural background, and the client’s awareness of and personal commitment to social justice and the impact of social justice on rehabilitation service outcomes” (CRCC, 2023, p. 15). Section D.3.d. addresses Cultural Humility. According to Tervalon and Murray-García (1998), cultural humility is an approach that can help to address the imbalance in client–provider power dynamics. The task force infused Section D.3.e. Use of Affirming Language as a method to acknowledge how language changes. It is our duty to affirm the client’s intersecting identities and refrain from imposing our values. The final two standards of the subsection, including D.3.f. Avoiding Discrimination and D.3.g. Serving Religious Cultures, are based on understanding, respect, and support for their client’s spiritual and religious beliefs, or absence thereof.
The final subsection, D.4., stipulates that diversity, equity, and belonging in coworker relationships are indicative of ethical professional standards of practice. By highlighting this responsibility in the new code of ethics, rehabilitation counselors are expected to promote diversity, equity, and belonging (CRCC, 2023) while maintaining and enhancing inclusive work environments to avoid negative indirect influences on client outcomes. This standard urges rehabilitation counselors to foster good working relationships by promoting trust, respect, self-awareness, and open communication (CRCC, 2023).
Operationalizing the New Multicultural Standards of the Code
Individual-Level Change
To ensure rehabilitation, as counselors apply the multicultural and advocacy sections of the ethics code, we must provide functional definitions of the behaviors that allow us to achieve the desired outcomes of equity and justice in service provision. Middleton et al. (2000) operationalized the multicultural competencies and standards developed more than 20 years ago and these recommendations remain relevant, even now, as CRCC endorses the new multicultural and advocacy sections. For this reason, we examine the new section of the Code, alongside the multicultural competencies developed, through the lens of the Akan (West African) principle of Sankofa (Asante & Mazama, 2009). Although there are several interpretations of this principle, which is represented by the image of a bird whose body is facing forward while the head is turned back, the literal translation is san (“return”), ko (“go back”), and fa (“fetch/retrieve”; Asante & Mazama, 2009, para. 1). We have applied this principle to a document that was essentially “forgotten, misplaced, or lost” to carve a path toward the future we seek (Asante & Mazama, 2009, para. 2).
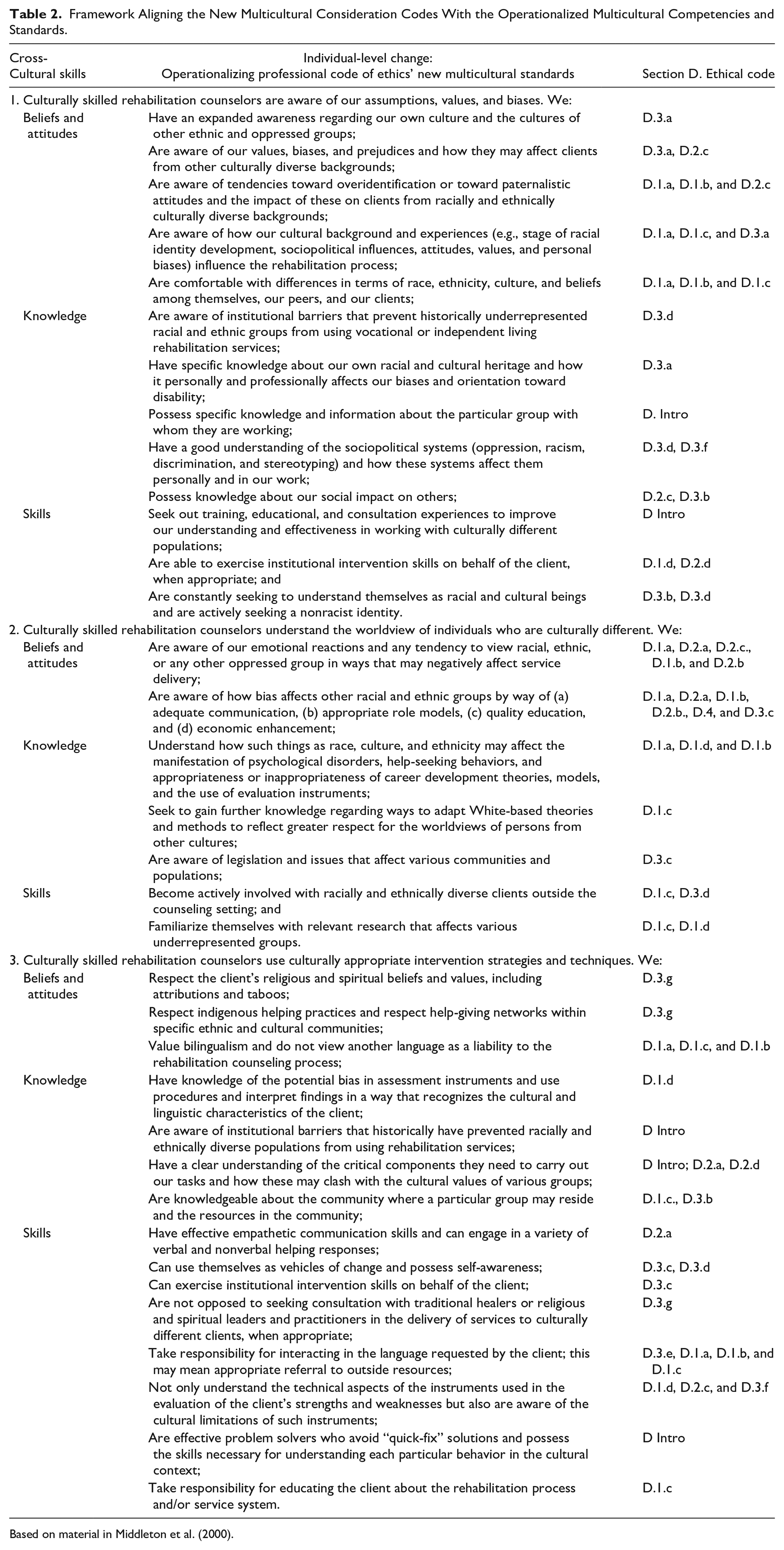
Table 2 provides a framework that aligns the new multicultural consideration codes with the operationalized multicultural competencies and standards (Middleton et al., 2000) and highlights specific strategies for reinforcement, support, and assessment of the multicultural considerations to promote change at the individual practitioner level. As we move forward to reduce bias, minimize discrimination, and prevent harm in practice, rehabilitation counselor education programs and professional organizations are encouraged to apply these standards across platforms that prepare counselors-in-training, practitioners, and educators to exhibit these skills.
Framework Aligning the New Multicultural Consideration Codes With the Operationalized Multicultural Competencies and Standards.
Institutional/Organizational-Level Change
While we acknowledge the personal factors necessary for comprehensive, inclusive, and equitable service delivery, we also note that many of the outcomes to reduce bias and prevent harm will require modifications to policy, procedures, and leadership at both institutional and organizational levels. Equity must be prioritized among our accreditation standards, CRCC examination development, and in the professional code of ethics. To better understand the role of power and privilege in this society, and at play within our profession, critical disability theory (Schalk, 2017) and critical race theory (Delgado & Stefancic, 2001) both provide a framework to challenge, dismantle, and eradicate systems of oppression. By adopting a critical disability lens at an organizational level, systems that direct how services are provided will be accountable to “reinterpret what it means to be considered disabled, bringing people who live this experience to the process as the primary agents of change in word and deed” (Reaume, 2014, p. 1249). This can be done, first, by centering the voices of those who are most affected by a policy or decision and, second, by allowing those individuals to be part of the reform and restoration process that will be necessary to repair those harms. A combination of stakeholder input from within the organization, and consultation with diversity, equity, inclusion, and accessibility (DEIA) experts from outside the organization can lead to meaningful outcomes for all parties involved.
Implications
The most recent revision of the CRCC Code of Ethics was conducted at a critical time in world history as the onset of the global COVID-19 pandemic led to forced lockdowns and ultimately affected how rehabilitation services were delivered. Members of the code revision task force were challenged to acknowledge that the method by which services were previously delivered would likely not return to normal, but rather grow to meet the unique needs of consumers like never before. One notable outcome of the COVID-19 pandemic is evidenced by an economic recession that pinpointed health inequalities of underserved communities (Bambra et al., 2020) and the “great resignation” a term coined to represent the roughly 33 million Americans who quit their jobs in 2021 in search of more fulfilling endeavors (Treffeisen, 2022). These phenomena undergirded a current and future demand for rehabilitation counselors to advocate and assist a range of diverse consumers with vocational services that resulted in job placement and retention. Data also indicate that past economic downturns prove daunting for people with disabilities as they are typically hit hardest, being considered more likely than their non-disabled peers to leave the workforce, with a less likelihood of regaining employment once the recession ends (Shaewitz & Yin, 2021).
Revisions to the code ignited conversations about racial and ethnic disparities that have gone unnoticed for far too long even within the profession. The CRCs are committed to serving diverse individuals with disabilities, highlighting their abilities, and connecting them to support/resources. Therefore, it is a priority for rehabilitation counselors to be culturally competent and serve individuals from a range of diverse backgrounds. The revised and new sections of the code are more than aspirational behaviors and, as we move forward in the profession, Sections C (Advocacy and Accessibility) and D (Multicultural Considerations) will provide both standards of practice and rigorous educational requirements for engaging in culturally competent and ethically conscientious rehabilitation service delivery (CRCC, 2023).
The codification of the multicultural competencies in the new Section D has been the result of decades of advocacy by thought leaders (Middleton et al., 2000; Sue et al., 1992). Even in a progressive and altruistic profession such as rehabilitation counseling, positive change can be slow and face resistance. While the changes to the code are anticipated to affect service delivery, there remains a need for ongoing training by way of continuing education, on-the-job and in-service training, and updates to rehabilitation counselor education that infuse the revised Code of Ethics as standards of professional practice.
While we note that ethics codes serve as guideposts for individual practitioners, we acknowledge an ever-present need for systems-level change to hold public and private sector rehabilitation institutions accountable, as well. The profession of rehabilitation counseling can follow models developed by the larger health care system in the United States. These examples include the development of standards for practice (i.e., National Standards for Culturally and Linguistically Appropriate Services [CLAS] in Health and Health Care; U.S. Department of Health and Human Services, Office of Minority Health, 2016) and ongoing research to examine the impact of cultural competence on client outcomes (Butler et al., 2016). The most recent relevant research conducted in rehabilitation counseling was conducted nearly two decades ago (Matrone & Leahy, 2005). While such discussions are outside of the scope of this article, we hope that future efforts include prioritization of systems- and institutional-level changes, in addition to the changes at the individual practitioner level, which are currently underway.
Conclusion
Understanding and commitment to decreasing racial disparities in services highlight why it is imperative that CRCC also take a stance to be more culturally competent and diversity-oriented to improve client outcomes. The CRCC’s willingness to blaze a trail in this movement is long overdue but speaks to the fact that people can no longer ignore the disparities that are systemic.
We acknowledge CRCC’s efforts to strengthen competencies, including revamping the code of ethics to meet the needs of an increasingly diverse client population. There is an increased need to develop explicit guidelines for counselors. Creating a multicultural section is timely in response to the ongoing needs in our country and provides an avenue for CRCC to reinforce the mission of advocating for diverse groups of individuals. Rehabilitation counseling professionals must apply the entire code of ethics and not solely the codes of interest as the lack of knowledge or lack of interest does not exempt one from the responsibility to practice according to the professional code of ethics, with the ultimate goal of improving rehabilitation outcomes for the clients we serve.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.