
Abstract
Ethnocultural empathy is one of the most important multicultural competencies in counseling psychology. Wang et al. developed the Scale of Ethnocultural Empathy (SEE) for counseling psychology educators as an outcome variable to evaluate multicultural counseling competencies of counselors-in-training. The purpose of this study was to evaluate the measurement structure of the SEE in a sample of undergraduate and graduate students in rehabilitation. Confirmatory factor analysis results indicated that the four-factor intercorrelated model fit the data very well. The four factors are (a) empathic feeling and expression, (b) empathic perspective taking, (c) empathic awareness, and (d) acceptance of cultural differences. The SEE can be an invaluable tool for rehabilitation counselor educators to evaluate their students’ level of multicultural rehabilitation counseling competency and as an outcome variable for multicultural rehabilitation counseling training.
The coronavirus disease 2019 (COVID-19) pandemic, the Black Lives Matter movement, and the passage of the COVID-19 Hate Crimes Act of 2021 (Pub. L. 117-3, 123 Stat. 2835) revealed the broad issues of racial inequalities in the United States (Chowkwanyun & Reed, 2020; Jan et al., 2021; Lopez et al., 2021; Valderrama, 2020). Systemic discrimination against African Americans and other marginalized groups, including people with disabilities, permeates every aspect of society including government, healthcare, education, and the workplace (Centers for Disease Control and Prevention [CDC], n.d.; Harvard Graduate Council, 2020; The Lancet, 2020; Rehabilitation Act Amendments, 1992; Walsh, 2020). Corporate America, healthcare companies, and higher education institutions have pledged to narrow racial disparities in the workplace and within society (Chowkwanyun & Reed, 2020; Computer Networks, 2020; Harvard Graduate Council, 2020; Jan et al., 2021; Lancet, 2020; Lopez et al., 2021). The Council of State Administrators of Vocational Rehabilitation (CSAVR) also issued a strong statement condemning and rejecting racism and inequities in all forms and the systemic way which this is used to oppress individuals with disabilities, especially those from racial and ethnic minority backgrounds (Council of State Administrators of Vocational Rehabilitation [CSAVR], 2020).
Recognizing the importance of providing culturally sensitive and effective counseling services to individuals from racial-ethnic minority backgrounds, the Council for Accreditation of Counseling and Related Educational Programs (CACREP, 2021) 2024 standards (Draft 2) clearly indicated that counselor education programs must address culturally responsive content and strategies across the eight foundational curriculum areas including social and cultural diversity. There is a need for a psychometrically sound clinical assessment instrument for rehabilitation counselor educators in CACREP-accredited programs to evaluate and improve students’ level of multicultural rehabilitation counseling competency and as an outcome variable for multicultural rehabilitation counseling training and research.
Multicultural competence training for rehabilitation counselors-in-training in CACREP-approved rehabilitation counseling and clinical rehabilitation counseling programs and practicing rehabilitation counselors is crucial to increasing equity in rehabilitation and counseling services. However, there is strong empirical evidence to indicate that racial disparities exist in counseling (Perzichilli, 2020), health and mental health care (CDC, n.d.; Perzichilli, 2020), and the state–federal vocational rehabilitation (VR) program (Chan et al., 2005; LeBlanc & Smart, 2007; Olney & Kennedy, 2002; Rehabilitation Act Amendments, 1992; Rosenthal & Berven, 1999). Employment and health disparities are intensified for individuals with multiple intersecting identities (e.g., race/ethnicity, gender, disability, and poverty) who are at risk for experiencing high levels of stigma, unconscious bias, health issues, and employment difficulties (Purdie-Vaughns & Eibach, 2008; Shaw et al., 2012; Vera et al., 2018). Rehabilitation researchers have suggested that racial biases were at least in part responsible for the inequitable patterns of VR service delivery for African Americans and other racial and ethnic minority clients (McGinn et al., 1994; Rosenthal et al., 2005; Wilson et al., 2001; Wilson & Senices, 2005).
Propitiously, research has indicated multicultural competence training is an effective intervention to reduce racial disparities in counseling and rehabilitation services. For example, Constantine (2001) used data from transcribed intake sessions of 52 counselor–client dyads to examine the effect of academic training in multicultural counseling and self-reported multicultural counseling competence on supervisor ratings of trainees’ multicultural counseling competence. Results indicated that multicultural competence training is strongly associated with observer ratings of trainees’ effectiveness in counseling racial and ethnic minority clients. Tao et al. (2015) conducted a meta-analysis to examine the effect of client ratings of therapist multicultural competence on therapeutic processes and outcome, including (a) working alliance, (b) client satisfaction, (c) general counseling competence, (d) session impact, and (e) symptom improvement. The findings indicated a large effect size for the relationship between multicultural competence and the counseling process, and a medium effect size between multicultural competence and counseling outcomes.
Recognizing racial biases may still exist in state VR agencies, the Rehabilitation Services Administration (RSA) has recently announced a funding opportunity (Notice Inviting Applications for Activities for Underserved Populations, Assistance Listing Number 84.315C, published in the Federal Register, 2021) for rehabilitation researchers to develop and validate effective multicultural competence training curriculum for rehabilitation counselors and rehabilitation counseling students that will improve employment outcomes and quality of employment outcomes for individuals with disabilities from racial and ethnic minority backgrounds. Considering RSA’s concern about racial inequality in state VR services, it is imperative for rehabilitation researchers to develop and validate outcome measures that can be used to assess the effectiveness of in-service multicultural competence training in state VR agencies and pre-service training in master’s level rehabilitation counseling programs.
Ethnocultural Empathy
In counseling, empathy is defined as an expression of the concern and respect counselors hold for their clients whose life experiences and worldview may be different from them (Wampold, 2015). Therapist empathy is a primary “common factor” essential to a counselor–client relationship and has a robust relationship with counseling/psychotherapy outcomes (d = 0.63). The effect size of therapist empathy is appreciably higher than other common factors: positive regard/affirmation (d = 0.56) and congruence/genuineness (d = 0.49; Wampold, 2015). Corollary, it can be argued that therapist “ethnocultural” empathy will be equally important for rehabilitation counselors to develop a working alliance with racial and ethnic minority clients to improve rehabilitation outcome. Ethnocultural empathy is defined as empathy toward people of racial and ethnic backgrounds different from one’s own (Wang et al., 2003). It is one of the most important multicultural competencies in healthcare, psychological, and rehabilitation services (Chung & Bemak, 2002; Wang et al., 2003). Wang et al. (2003) developed and validated the Scale of Ethnocultural Empathy (SEE) in a large sample of college students using exploratory and confirmatory factor analysis and found strong empirical support for a four-factor measurement structure: (a) empathic feeling and expression, (b) empathic perspective taking, (c) empathic awareness, and (d) acceptance of cultural differences.
Empathic Feeling and Expression is related to concern about communication of discriminatory or prejudiced attitudes or beliefs and emotional/affective responses to the emotions and/or experiences of people from racial and ethnic minority backgrounds different from one’s own. Empathic Perspective Taking is related to effort to understand the experiences and emotions of people from racial and ethnic backgrounds by trying to take their perspectives in viewing the world. Empathic Awareness is related to the effort to focus on the awareness or knowledge that the counselor has about the experiences of people from racial and ethnic minority backgrounds different from his or her own. Acceptance of Cultural Differences is related to effort to understand, accept, and value cultural traditions and customs of individuals from racial and ethnic minority backgrounds. These ethnocultural empathy factors were found to correlate significantly with a general empathy measure (concurrent validity) and attitudes toward people’s similarities and differences (nomological validity, a form of construct validity) in the theoretically predicted direction (Wang et al., 2003). Rasoal et al. (2011) confirmed the four-factor measurement structure of the SEE in a large sample (N = 799) of undergraduate students in Sweden and the SEE subscales were significantly associated with the Empathic Concern and Perspective-Taking subscales of the Interpersonal Reactivity Index. Albiero and Matricardi (2013) validated the factorial structure of the SEE in a sample (n = 610) of Italian undergraduate students and found a positive moderate association between the SEE and a measure of general empathy as well as a negative high association with a measure of prejudice. Mallinckrodt et al. (2014) developed and validated a more comprehensive version of the SEE in a sample of White undergraduate students in introductory psychology courses (N = 602) and reported subscales of the expanded version of the SEE were significantly associated with measures of Openness to Diversity Challenge and Universal-Diverse Orientation.
Evidently, the SEE can be used in multicultural rehabilitation counseling research as an outcome measure to evaluate the effectiveness of multicultural competence training for leaders, mid-level managers, rehabilitation counselors, and support staff in state VR agencies. It can also be used by rehabilitation counselor educators to evaluate the effectiveness of multicultural competence training in their CACREP approved clinical rehabilitation counseling programs as well as to assess students’ development of multicultural competencies in clinical practicum and internship.
Purpose of the Study
The purpose of this study was to evaluate the four-factor measurement structure of the SEE in a sample of undergraduate students in rehabilitation services and graduate students in rehabilitation counseling using confirmatory factor analysis (CFA). The following research questions were investigated:
What are the underlying dimensions of the Scale of Ethnocultural Empathy?
Do the subscales of the Scale of Ethnocultural Empathy possess adequate internal consistency reliability?
What is the relationship between ethnocultural empathy and social dominance orientation?
Method
Participants
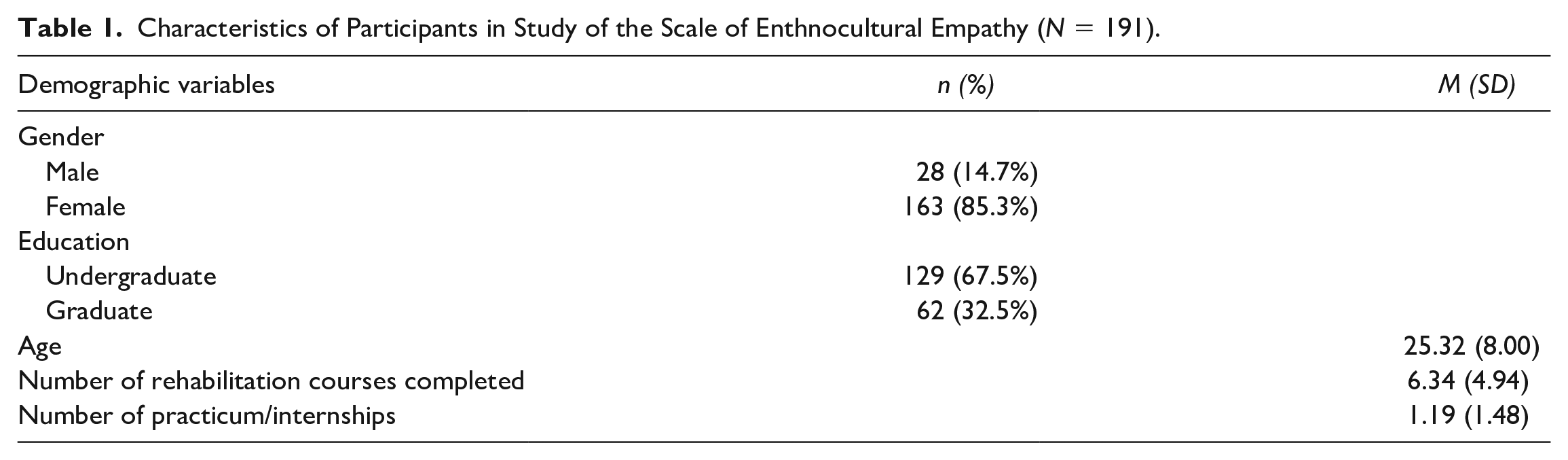
The sample is composed of 191 European American undergraduate students in rehabilitation services and master’s degree students in rehabilitation counseling. The inclusion criteria were undergraduate students majoring in rehabilitation services or master’s degree students majoring in rehabilitation counseling. The mean age of participants was 25.30 years (SD = 7.98), and 85% were women. A detailed description of the individual characteristics of the participants is presented in Table 1.
Characteristics of Participants in Study of the Scale of Enthnocultural Empathy (N = 191).
Measures
Ethnocultural empathy
The SEE, developed by Wang et al. (2003), was used to measure ethnocultural empathy. It is composed of 31 items with four subscales: (a) empathic feeling and expression (EFE; e.g., “When I hear people make racist jokes, I tell them I am offended even though they are not referring to my racial or ethnic group”); (b) empathic perspective taking (EP; e.g., “It is easy for me to understand what it would feel like to be a person of another racial or ethnic background other than my own”); (c) acceptance of cultural difference (AC; e.g., “I feel irritated when people of different racial or ethnic backgrounds speak their language around me”); and (d) empathic awareness (EA; e.g., “I can see how other racial or ethnic groups are systematically oppressed in our society”). Each item is rated on a 6-point Likert type agreement scale (1 = strongly disagree that it describes me to 6 = strongly agree that it describes me). The four-factor measurement structure was validated by Wang et al. (2003) using exploratory and then confirmatory factor analysis. Wang et al. (2003) reported internal consistency reliability coefficients (Cronbach’s alpha) for the four scales ranging from .73 to .89. In the present study, the Cronbach’s alpha was .87 for the EFE subscale, .71 for the EP subscale, .74 for the AC subscale, and .69 for the EA subscale. In general, Cronbach’s alpha .70 or higher is considered acceptable (Cortina, 1993).
Social dominance
The Social Dominance Orientation Scale (SDOS), developed by Pratto and colleagues (1994), was used to measure social dominance orientation. Social dominance orientation refers to the basic desire to have one’s own primary in-group be considered better than, superior to, and dominant over relevant out-groups. It is composed of 16 items (e.g., “Some groups of people must be kept in their place”; “We should not push for group equality”; “We should not work to give all groups an equal chance to succeed”). Each item is rated on a seven-point Likert type rating scale (1 = very negative to 7 = very positive). Pratto et al. (1994) reported that Cronbach’s alpha for the SDOS was .83. In the present study, the Cronbach’s alpha for the SDOS was .93.
Procedures
Upon receiving approval from the Institutional Review Board of a midwestern university in the United States, participants were recruited from rehabilitation programs in eight predominantly White institutions. Professors who agreed to assist with this study helped advertise for this research project to students in their classes. Prior to participation in the study, the purpose of the study was explained to participants. Students were told that participation in the study was completely voluntary. Once consent was granted from the individuals, they proceeded to complete the survey packet.
Data Analysis
The Statistical Package for the Social Sciences (SPSS, version 27.0) was used for computing descriptive statistics and correlational analysis. CFA was computed to examine the measurement structure of the SEE using the SPSS AMOS statistical software program version 22.0. Following the guidelines of Weston et al. (2008), the goodness of fit of each CFA model was assessed using chi-square, chi-square/df ratio, the goodness of fit index (GFI), the comparative fit index (CFI), and the root mean square error of approximation (RMSEA). A nonsignificant chi-square, x2/df ratio in the range of 1 to 3, and values greater than .95 for the GFI and CFI, and RMSEA less than 0.08 indicate the model is a good fit to the data.
Results
Descriptive Statistics
In this study, the average score for the SEE was 4.30 (M = 0.64). The average subscale scores were: (1) empathic feeling and expression (M = 4.53, SD = 0.72), (2) empathic perspective taking (M = 3.44, SD = 0.83), (3) empathic awareness (M = 4.88, SD = 0.76), and (4) acceptance of cultural differences (M = 4.35, SD = 1.38). Rehabilitation students rated themselves as high in empathic feeling and expression, empathic awareness, and acceptance of cultural differences but average in empathic perspective taking. The average score for the SDOS was 1.83 (SD = .85), indicating rehabilitation students in the present study do not support the social hierarchy that proclaims their in-group is superior to out-groups and their domination over lower-status groups.
Confirmatory Factor Analysis
To avoid estimating too many parameters (i.e., factor loadings and error terms) in fitting the model to the data and to decrease the likelihood of obtaining distorted results due to idiosyncratic characteristics of individual items, Wang et al. (2003) organized the 31 SEE items into 9 parcels before subjecting the scale to a CFA. We replicated this process and divided the 31 items from the four SEE subscales—EFE (15 items), EP (7 items), AC (5 items), and EA (4 items)—into 9 bundles (3 bundles for the EFE, 2 bundles for the EP, 2 bundles for the AC, and 2 bundles for the EA). Three confirmatory factor models were tested: (a) one-factor model, (b) four-factor intercorrelated model, and (c) four-factor hierarchical model (second-order factor).
The results indicated that the one-factor model was a poor fit for the data, χ2(27, N =192) = 164.15, p < .001; χ2/df = 6.08; GFI=.84; CFI = .82; RMSEA = 0.16. The model fit for the four-factor intercorrelated model was very good, as indicated by the following indices: χ2(21, N = 192) = 44.99, p < .05; χ2/df = 2.14; GFI = .95, CFI = .97; RMSEA=.0.77 (see Figure 1). In addition, all factor loadings were high (ranging from .69 to .90), suggesting that the four factors were well constructed by the bundles. The four-factor correlated model represents a significantly better explanation of the data than the one-factor model (χ2diff = 119.16, dfdiff = 6, p < .01). Finally, we fit a second-order hierarchical factor model with the second-order factor (SEE) having direct effects on each first-order factor (EFE, EP, AC, and EA). The analysis generated the following fit indices: χ2(23, N=192) = 45.01, p < .05; χ2/df = 1.96; GFI = .95; CFI = .97 (>.95); RMSEA = 0.07 (<0.08). All factor loadings were significant at the p < .01 level, suggesting satisfactory convergent validity for the first-order factors. The means and standard deviations of the SEE total and four factor scores in this study are as follows: SEE total: M = 4.46, SD = 0.62; EFE: M = 4.64, SD = 0.70; EP: M = 3.52, SD = 0.92; AC: M = 4.88, SD = 0.86; and EA: M = 4.88, SD = 0.76.
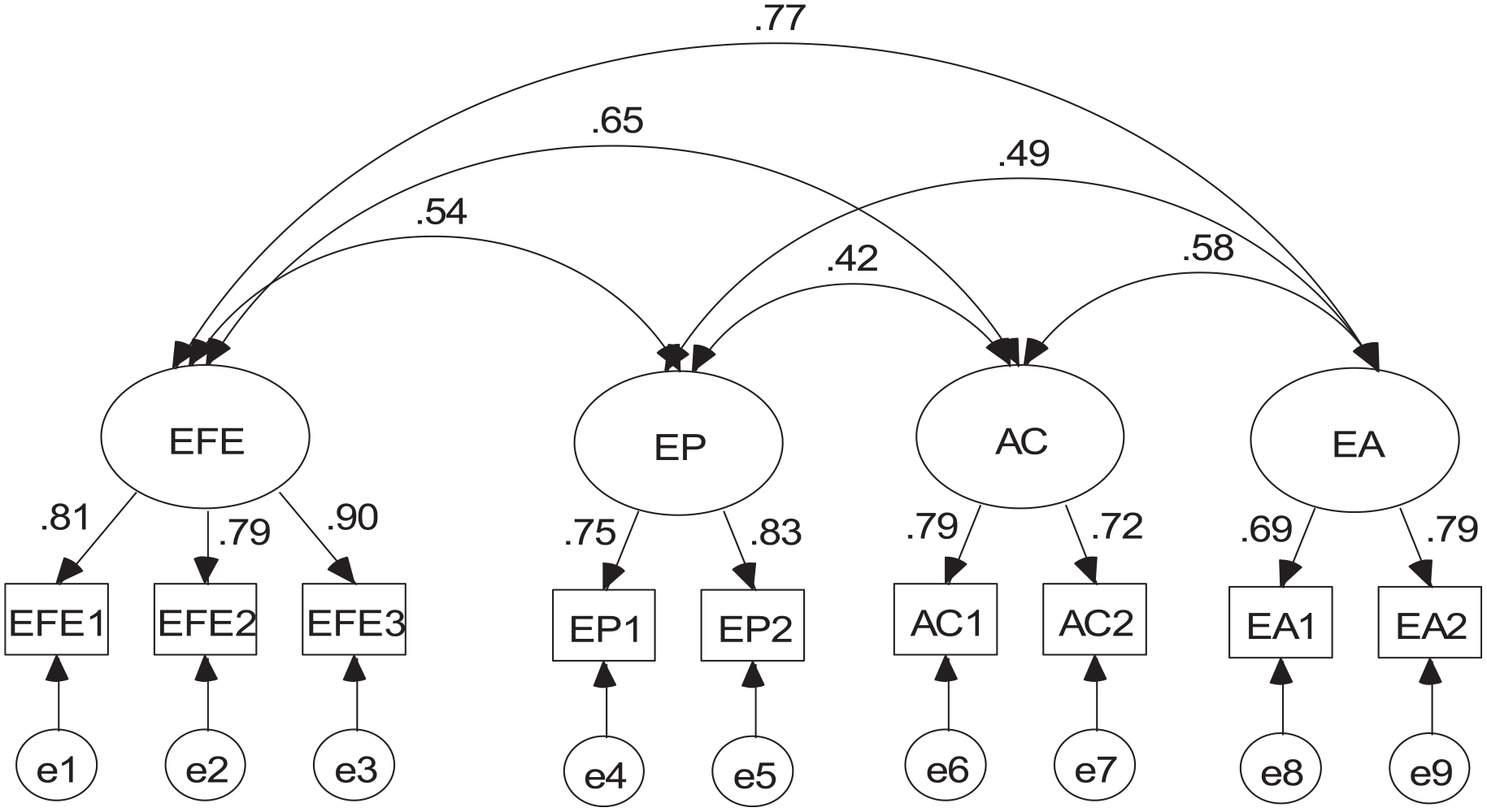
Standardized estimates for the four-factor correlated model.
External Correlates
The SEE was correlated with the SDOS. The Pearson product-moment correlation coefficient between the SEE and the SDOS was significant (r = -.45, p < .001), indicating that high SEE scores were related to lower levels of negative stereotyping of out-groups, internal and negative attributions for out-group failures, and active discrimination against out-group members.
Discussion
The aim of the present study was to validate the psychometric properties of the SEE in a sample of undergraduate and graduate students in rehabilitation. The goodness-of-fit indices for the CFA indicated a very good fit between the model and the data, supporting the factorial validity of the SEE. The significant inverse correlation between ethnocultural empathy and social dominance (a related construct) in the nomological network at the expected direction provide nomological validity of the SEE, which is a form of construct validity (Cronbach & Meehl, 1955). Except for the acceptance of cultural difference subscale (.69), the Cronbach’s alpha coefficients for the rest of the subscales were greater than .70, well within the acceptable range. The Cronbach’s alpha coefficients for the SEE in the present study are consistent with previous research validating the psychometric properties of the SEE (Albiero & Matricardi, 2013; Rasoal et al., 2011; Wang et al., 2003). As expected, compared to the normative data reported by Wang et al. (2003), students in rehabilitation services and rehabilitation counseling had appreciably higher ethnocultural empathy scores than college students in general. It can be concluded that the SEE is a psychometrically sound measure of ethnocultural empathy that can be used in multicultural competency training and research in rehabilitation.
Implications for Research and Clinical Rehabilitation Counseling Practices
Individuals with multiple intersecting identities of race/ethnicity, disability, and poverty are at elevated risk for experiencing high levels of stigma, unconscious bias, health issues, and employment difficulties (Purdie-Vaughns & Eibach, 2008; Shaw et al., 2012; Vera et al., 2018). Research has indicated that racial disparities exist in state VR agencies. The Rehabilitation Services Administration has established pre-service multicultural competency training for master’s degree students in clinical rehabilitation programs and in-service training for practicing rehabilitation counselors in state VR agencies and community-based rehabilitation organizations as a high priority goal for the agency. The SEE can be used by rehabilitation counselor educators and training specialists in VR to assess students and counselors’ level of multicultural rehabilitation counseling competency and as an outcome variable to evaluate the effectiveness of multicultural rehabilitation counseling training.
The prevalence of chronic health conditions and disabilities (e.g., obesity, high blood pressure, stroke) is significantly higher among African Americans than Whites (Centers for Disease Control and Prevention, 2017). Furthermore, African American workers and foreign-born Hispanic workers are at elevated risk for workplace injuries compared to White workers, suggesting that disparities in economic opportunities expose minorities to greater risk of workplace injury and disability (Goodman et al., 2019; Seabury et al., 2017). Rehabilitation counselors in state VR agencies are serving more African Americans with chronic disease and work-related disability than before (Pi et al., 2020). There is an urgent need to increase the knowledge, skills, abilities, and attitudes of rehabilitation counselors and counselors-in-training to understand, interact effectively, and empathize with people with disabilities from racial minority backgrounds. Helping rehabilitation counselors develop awareness of their implicit bias toward African Americans and other minorities with disabilities and provide multicultural competence training to increase their ability to work fairly and effectively with minority clients will increase their opportunity to receive skill training for in-demand occupations. The SEE can be a valuable tool for leaders in state VR agencies to evaluate the effectiveness of multicultural rehabilitation counseling training for practicing rehabilitation counselors and for rehabilitation counselor educators to gauge their students’ multicultural competencies in clinical supervision.
Limitations
There are several limitations related to this study that need to be considered. We recruited a convenience sample of undergraduate students in rehabilitation services and graduate students in rehabilitation counseling from eight cooperative White institutions, which may limit the generalizability of the research findings. Although undergraduate and graduate students in rehabilitation share commonalities because of their career interests and training in counseling, disability, and rehabilitation, future research should focus on rehabilitation counselors-in-training and practicing rehabilitation counselors (Donnel, 2008; Herbert et al., 2010; Koch et al., 2009). In addition, research has indicated that minority counselors may have the same biases against minority clients; future research should include rehabilitation students from historically Black colleges and universities. Not including a well-established measure of therapist empathy to provide evidence of concurrent validity for the SEE is another limitation of this study. The Cronbach’s alpha of .69 for the empathic awareness subscale is below .70; it may be important to conduct an item analysis to identify items that should be modified or removed from this subscale.
Conclusion
The Black Lives Matter movement revealed the broad issues of racial inequalities in the United States. Research has indicated that racism is deeply embedded as normal practice in the systems, structures and institutions that fortify society. Diversity, inclusion, and equity are fundamental values and beliefs of the counseling profession. The CACREP 2024 standards (Draft 2) clearly indicated that counselor education programs must address culturally responsive content and strategies across the eight foundational curriculum areas (CACREP, 2021). Multicultural competence training for rehabilitation counselors-in-training in CACREP-approved rehabilitation counseling and clinical rehabilitation counseling programs and practicing rehabilitation counselors is crucial to increasing equity in rehabilitation and counseling services. Ethnocultural empathy is essential for rehabilitation counselors to develop a positive working alliance with racial and ethnic minority clients with disabilities to improve rehabilitation counseling outcomes. The SEE is a psychometrically sound clinical assessment instrument that can be used by rehabilitation counseling researchers and educators to evaluate the effectiveness of multicultural competence training for rehabilitation counseling students and practitioners.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.