
Abstract
The rehabilitation counseling profession, as an essential career, has been facing unforeseen and unprecedented complications as a result of the coronavirus-19 pandemic. As practitioners were required to begin completing their work virtually or using telehealth modalities, it became apparent that may be gaps in preparation for such a shift. It is as yet unknown what implication these changes have on employment rates of people with disabilities, in addition to other markers for independence (e.g., independent living). Implications of the sudden shift to virtual practice are especially of interest following the changes to the comprehensive system of personnel development legislated by the Workforce Innovation and Opportunity Act reauthorization of 2014. Decreased educational requirements may lead vocational rehabilitation (VR) employees to navigate a national crisis without the essential knowledge domains required for qualified provider status. The current study asked VR personnel to indicate their comfort and preparedness in various areas, in light of the pandemic and virtual service provision (N = 88). Items were assessed at three levels: Counselor, Agency, and Client. Taken together, the results indicate that the sample feels able to maintain evidence-based services, and that supervisors have been regularly available during this uncertain time. Implications for rehabilitation researchers, supervisors, and educators are discussed.
Keywords
Needs of Vocational Rehabilitation Agencies in the Wake of COVID-19 Pandemic
In March of 2020, there was a massive change to the health and safety of the globe (World Health Organization, 2020). The coronavirus-2019 (COVID-19) was officially designated as a pandemic by the World Health Organization, affecting millions of lives across the world. To combat the extreme contagiousness of the virus, it became imperative that changes be made to inhibit the transmission of COVID-19 from person-to-person. Such changes included a massive shift to remote work and learning, shelter-in-place orders, social distancing and mask mandates, limits on in-person services—including dining, health care, and shopping—and furloughs for millions of workers (especially those deemed nonessential).
Early in the pandemic, shelter-in-place orders were implemented for the majority of U.S. businesses, except those deemed essential. The definition of essential varied by state but states also received general guidance from the federal government. In a review of the definitions of essential by states and the federal government, the National Conference of State Legislatures (2020) determined the following sectors as being considered essential: energy, child care, water and wastewater, agricultural and food production, critical retail (i.e., grocery, hardware stores, mechanics), critical trades (construction, plumbers, electricians, etc.), transportation, and nonprofits and social service organizations.
As social service organizations, state–federal vocational rehabilitation (VR) employees were deemed essential, and rapid shifts were taken to adopt remote work setups, to maintain social distancing in office buildings, and to navigate resources and employment for disabled people in a time of unprecedented unemployment rates. The effects of the pandemic on the important work that takes place at VR agencies continue to permeate all aspects of the rehabilitation counseling process. In addition, as VR agencies are run by state governments, each state has implemented policies and practices differently (Adolph et al., 2021), leaving no uniform way to assess the impact of the pandemic on VR workers and clients. Of particular interest is the way that VR counselors are managing not only their ability to provide services to their clients but also the ways in which they are experiencing the effects of the pandemic themselves. As helping professionals, one’s own mental health and well-being are vulnerable to the tumultuous and demanding work; self-care and burnout are ever-present concerns for supervisors and educators alike (Tabaj et al., 2015; Templeton & Satcher, 2007). Mental health concerns have been raised related to the impact of the pandemic at varying levels, including the population-level mental health (Galea et al., 2020), the trauma experienced by health care workers (Armitage & Nellums, 2020), the stress and trauma being experienced by disabled people (Godfrey, 2020; Lund et al., 2020), and the disproportionate trauma of the pandemic to individuals from marginalized groups who work in essential jobs (Litam et al., 2021; Strauser et al., 2021). However, absent from the literature at present are data revealing the impact of COVID-19 on VR counselors.
The purpose of the current study was to understand the pandemic-related needs and experiences of VR counselors at an agency in the southeastern United States. Specifically, the researchers sought to identify counselors’ needs and experiences related to increased reliance on technology for rehabilitation services, implementing universal design (UD) principles, providing support to clients during the pandemic, and their perception of agency-level management of the COVID-19 pandemic.
Method
The current study utilized a cross-sectional quantitative method via a survey that was distributed to VR counselors at a VR agency in the Southeast region of the United States.
Participants and Procedures
The survey was distributed to approximately 400 employees at the VR agency, yielding a response rate of about 22% (N = 88). Participant demographics mirror the makeup of the counseling profession, primarily White and female. Most participants held a master’s degree, either in rehabilitation counseling (48.9%) or in a related area (31.8%). About half of the participants indicated that they held a Certified Rehabilitation Counselor (CRC) credential (48.9%). The majority of participants indicated that they have been working at the VR for 10 or more years (29 people or 33%), while the second largest group indicated that they had been working at the VR for 0 to 2 years (22 people or 25%). Participants’ job titles were VR or OVR counselor (n = 74), manager, branch manager, supervisor (n = 5), and two miscellaneous not indicated to protect privacy. Seven left this item blank. Demographic details can be found in Table 1.
Participant Demographics for the VR Counselors and COVID-19 Study Sample
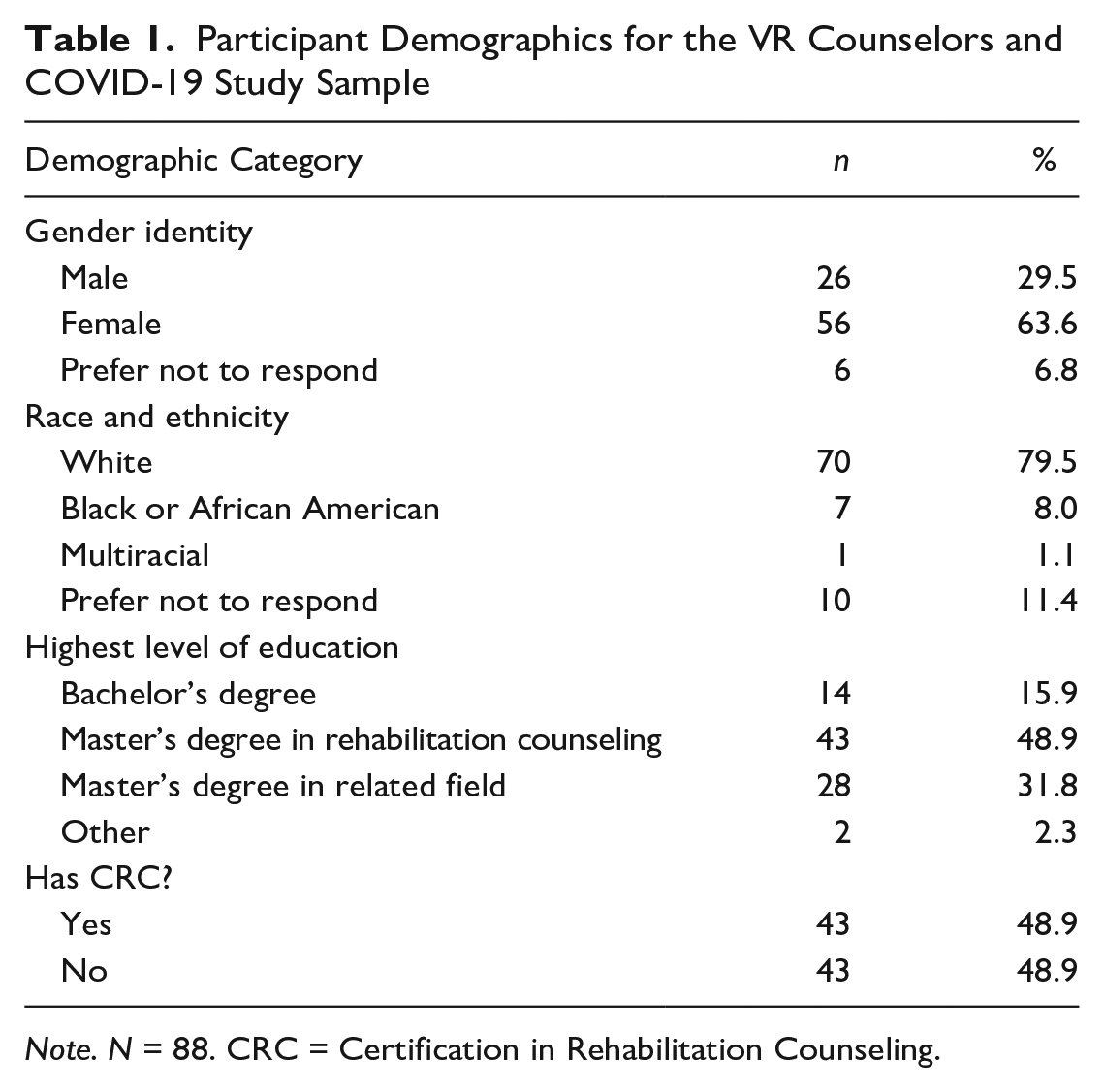
Note. N = 88. CRC = Certification in Rehabilitation Counseling.
After obtaining the Institutional Review Board (IRB) approval and in collaboration with the VR office’s administration, emails were distributed to employees for recruitment purposes. Emails were distributed with reminders at 2-week intervals, for a 2-month period. Participants were not incentivized for participating in the study and were reassured that participation was entirely anonymous and individual responses would not be reviewed by any administrative or managerial personnel.
Measures
A survey was developed by the researchers for the purpose of this study. Items were framed around three main areas of interest related to the needs of VR counselors and agencies: the counselor level (i.e., individual’s experiences and needs of counselors), the agency level (i.e., counselors’ experiences of things going on at the agency around them), and the client level (i.e., counselors’ actual work with clients and their perception of clients’ needs). To begin item development, researchers collated a list of presenting issues related to the pandemic and service provision in rehabilitation counseling at the three aforementioned levels. The list was informed by the researchers’ expertise in rehabilitation counselor education, UD and accessible online learning, and VR. Certain items were directly informed by the first and third authors’ experience of teaching a counseling techniques course during the first spring semester of the pandemic (i.e., March 2020–May 2020). For example, students often requested support with phone-based counseling services and shared that they were requesting training but not receiving it from their supervisors. As such, items were developed around using UD and technology (e.g., I create accessible documents electronically, I seek out opportunities to become more proficient with technology, I am aware of telehealth procedures).
A draft version of the survey was shared with the division director and the director of training at the VR agency with requests for modifications and recommendations based on their perception of the agency’s needs. Upon receiving and completing the recommended edits, the survey was developed into a final document consisting of 39 items: 20 counselor-level items, 12 agency-level items, and 7-client level items. Items were presented using a Likert-type scale from 1 (Strongly Disagree) to 5 (Strongly Agree) with a neutral option at 3 (Neither Agree nor Disagree). In addition, the demographic section included six questions related to race/ethnicity, gender identity, education level, job title, length of time at the agency, and CRC status.
Data Analysis
The data were analyzed using the Statistical Package for the Social Sciences, Version 27. Data were analyzed for frequencies and descriptive statistics to identify the levels of need of particular items.
Results
Counselor-Level Needs
Responses to items on the counselor-level needs subscale ranged from means of 4.57 (SD = .74), I am proficient with basic office technology (word processing, email, internet) to 2.60 (SD = 1.17), I aid clients with stimulus check availability. Highest rated items were related to service provision skills and evidence-based practice including I apply counseling skills during virtual sessions (M = 4.48, SD = .81), I am able to talk with my supervisor regularly about my concerns (M = 4.42, SD = .97), I keep up-to-date on the daily changes in policies, demand-side needs, and other movements that have happened since March (M = 4.35, SD = .82), and I implement evidence-based practices in virtual service provision (M = 4.20, SD = .99). The lowest rated items ranged in topic and included the following items: I consult the universal design principles when developing materials for my clients (M = 3.18, SD = 1.09), I seek out information about telehealth and tele-counseling to improve my practice (M = 3.68, SD = 1.19), I discuss the psychosocial aspects of sheltering in place with my clients (M = 3.73, SD = 1.14), and I experienced increased stress as a result of sheltering in place (M = 3.74, SD = 1.23). The entirety of item-level means can be found in Table 2.
Counselor-Level Needs by Mean (high to low).
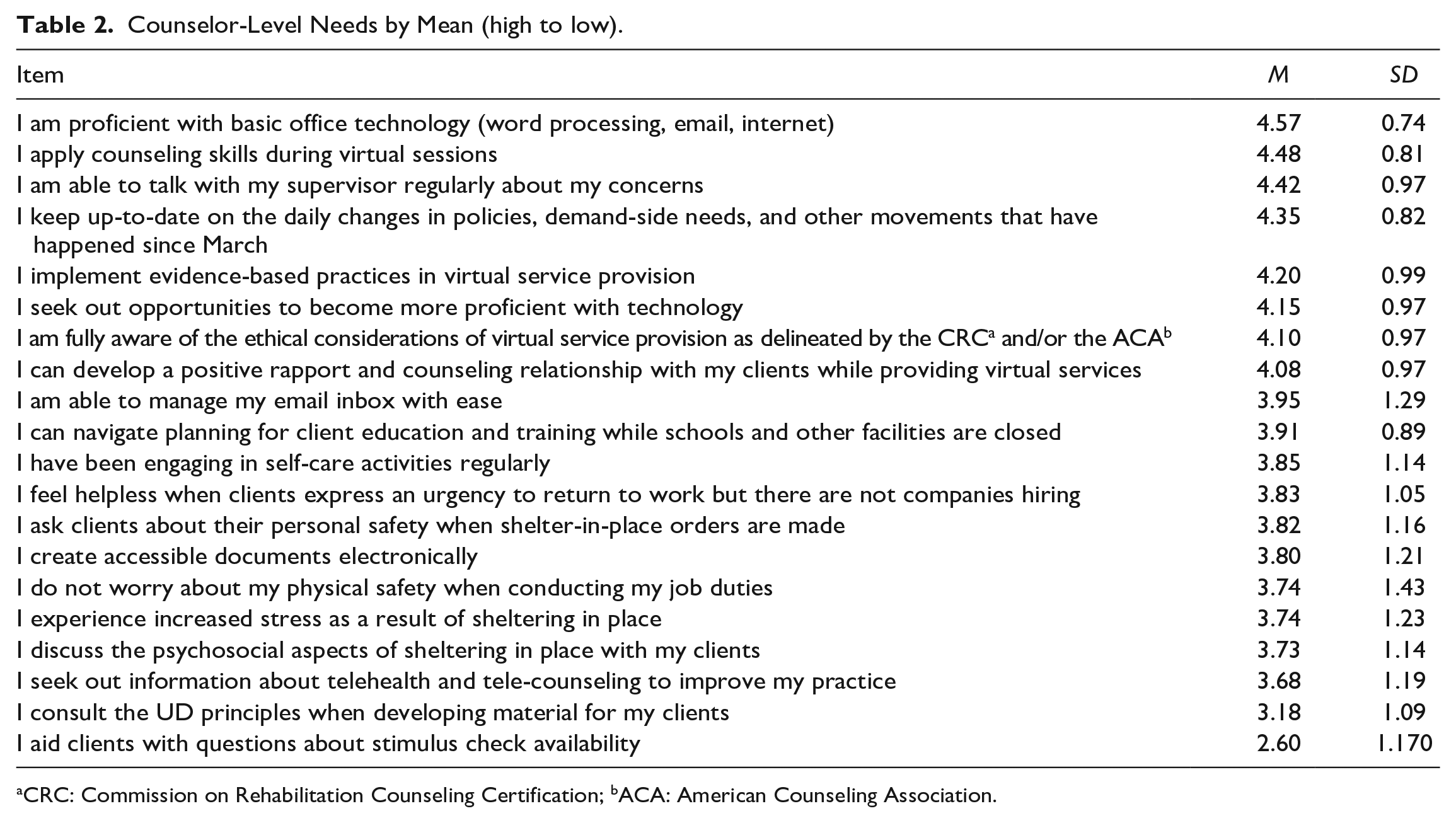
aCRC: Commission on Rehabilitation Counseling Certification; bACA: American Counseling Association.
Agency-Level Needs
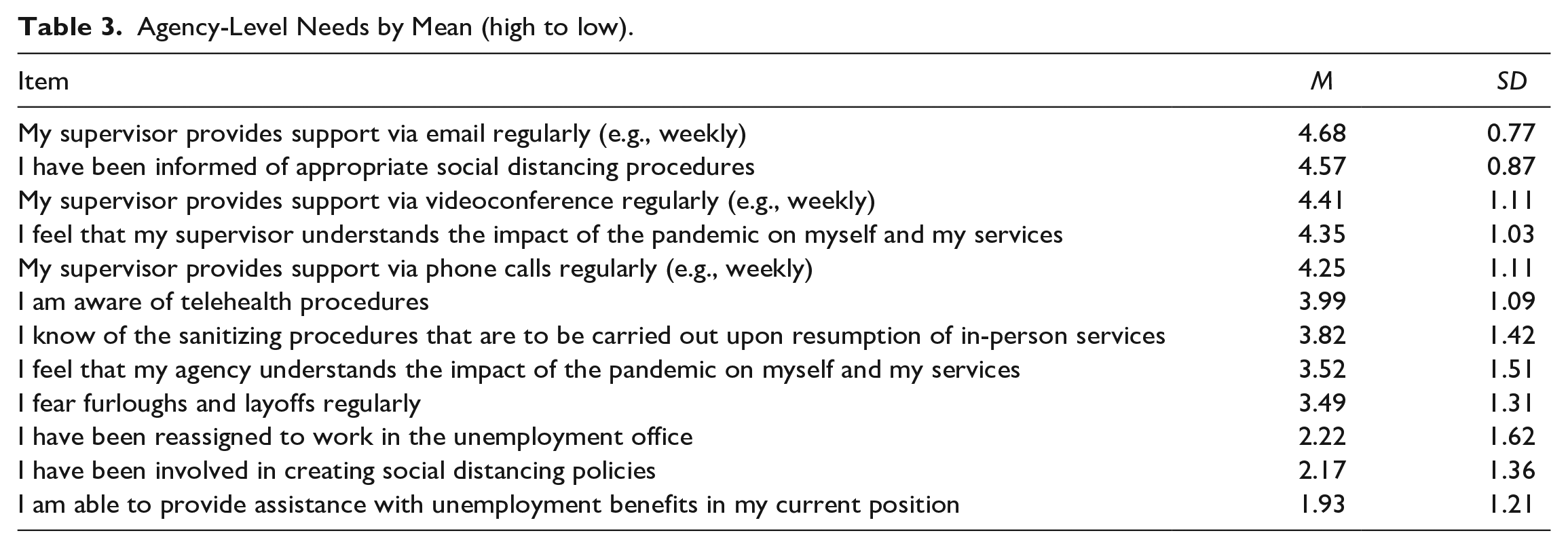
Means on agency-level items were, in general, lower than those found on the counselor-level items. Means ranged from My supervisor provides support via email regularly (e.g., weekly), M = 4.68 (SD = .77) to I am able to provide assistance with unemployment benefits in my current position, M = 1.93 (SD = 1.21). The highest rated items included I have been informed of appropriate social distancing procedures, M = 4.57 (SD = 0.87) My supervisor provides support via videoconference regularly (e.g., weekly), M = 4.41 (SD = 1.11), and I feel that my supervisor understands the impact of the pandemic on myself and my services, M = 4.35 (SD = 1.03). Items with the lowest agreement included I have been involved in creating social distancing policies, M = 2.17 (SD = 1.36), I have been reassigned to work in the unemployment office, M = 2.22 (SD = 1.62), I fear furloughs and layoffs regularly,M = 3.49 (SD = 1.31), and I feel that my agency understands the impact of the pandemic on myself and my services, M = 3.52 (SD = 1.51). The entirety of agency-level results can be found in Table 3.
Agency-Level Needs by Mean (high to low).
Client-Level Needs
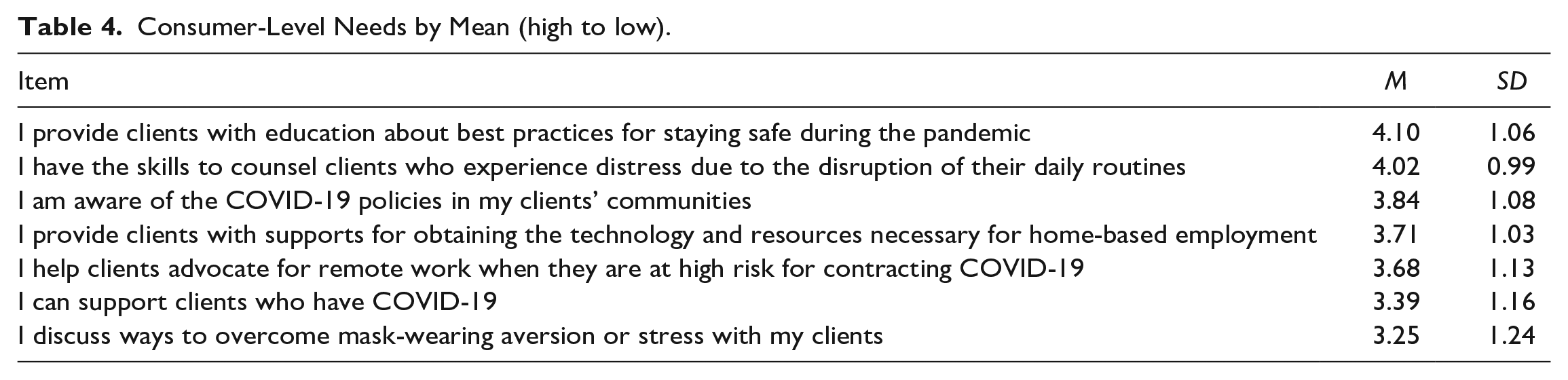
Client-level items received the lowest levels of agreement of all three subscales. The item with the least agreement was I discuss ways to overcome mask-wearing aversion or stress with my clients (M = 3.25, SD = 1.24), while the item with the most agreement was I provide clients with education about best practices for staying safe during the pandemic (M = 4.10, SD = 1.06). Items with the lowest agreement included I can support clients who have COVID-19 (M = 3.39, SD = 1.16), I help clients advocate for remote work when they are at high risk for contracting COVID-19 (M = 3.68, SD = 1.13), and I provide clients with supports for obtaining the technology and resources necessary for home-based employment (M = 3.71, SD = 1.03). All client-level results can be found in Table 4.
Consumer-Level Needs by Mean (high to low).
Discussion
The current study appears to be the first empirical investigation into the perceived needs of VR counselors relative to the COVID-19 pandemic. Although vaccine rollouts are currently in place, it is unclear when, if ever, we will return to pre-pandemic practices in our personal and professional lives. Overwhelmingly, the results of the current study demonstrate that the counselors in the current study felt well prepared and indicated that they were well trained, even as they were providing services amid a global pandemic. Notably, the participants sampled in this study revealed a high level of support from their supervisors, which may be a contributing factor to their perceptions of preparedness.
More broadly, the current study may reveal agency-level or systematic needs necessary for supporting VR counselors during the pandemic, and it also may prepare agencies to more readily respond to a future crisis situation, should one arise. For example, participants noted that they felt that their supervisors understood the impact of the pandemic on their work and lives, but by comparison did not feel as strongly that the agency in general understood those same factors. Should another crisis arise, agencies may find that it is important to be more transparent and supportive of their workforce or they may find themselves losing employees. Findings inform the field about COVID-19–specific needs at the counselor, client, and agency levels, as well as broader needs related to monitoring counselor well-being and turnover intentions, and considerations for improved use of UD in rehabilitation.
COVID-19–Specific Needs
An area of concern raised in the findings of the current study is that participants indicated that they provided education about staying safe during the pandemic but did not specifically discuss or support clients experiencing mask-wearing aversion and indicated low agreement with the ability to help clients who had COVID-19. Confounding factors for these findings potentially include the politicization of mask wearing and the COVID-19 pandemic in general. The findings may then reflect counselor’s own opinions about mask wearing (i.e., anti-mask wearing), or may have caused counselors to avoid discussing these topics with clients (i.e., fear of bringing up a divisive topic). While it is not possible to determine the cause of these findings at this time, supervisors and leaders in VR must be aware that divisive rhetoric impacts client-level interactions. Such results underscore that it is increasingly important for rehabilitation counselors to be aware of the inherent political nature of rehabilitation as a profession and a system of belief (Harley et al., 2008).
Counselor Well-Being
At the counselor level of the study, more than half of participants agreed strongly or somewhat that they experience increased stress as a result of the pandemic, and strongly or somewhat agreed that they feel a sense of helplessness when clients express an urgency to return to work but companies are not hiring. Simultaneously, participants overwhelmingly agreed that they were also being sure to implement evidence-based practice, establishing therapeutic relationships, and engaging appropriately with technology. This dichotomy of counselor’s personal needs and emotions with their professional output and service delivery is of interest. The pandemic has created an untenable labor supply and demand inequity, which contributes to feelings of helplessness on the part of counselors that may translate into decreased job satisfaction.
Pre-pandemic studies reveal that occupational stress is a significant factor in the turnover intentions of rehabilitation counselors (Layne et al., 2004). More detailed and recent findings indicate that, specifically, “too much work and too many administrative tasks” contribute to increased stress among rehabilitation professionals (Tabaj et al., 2015, p. 119). Results of the current study indicate that counselors are indeed experiencing unique and significant stressors and that agencies should remain vigilant about monitoring the job satisfaction climate within their states and attending to those factors that are currently working. In the sample studied, one such factor was supervision.
Supervisor relationships
In the current study, questions pertaining to supervisor availability and understanding were among the highest rated across all items. This finding cannot be overlooked in contextualizing the experiences of the participants in this study. Both conceptual (e.g., Bezyak et al., 2010) and empirical (e.g., Herbert & Trusty, 2006; McCarthy, 2013; Schultz et al., 2002; Schultz, 2007) articles have drawn attention to the importance of supervision in VR, which seems to be underscored by the findings of this study. While examining the quality and type (e.g., administrative or clinical) of supervision provided was outside the scope of the current study, it is possible that the regular availability of supervisors and their ability to empathize with counselors during this trying time had an impact on counselor’s feelings of preparedness.
Findings from McCarthy (2013) indicate a positive relationship between regularly scheduled supervision and a positive supervisory working alliance (SWA). Further, a meta-analysis of 27 articles examining the relationship of SWA to various outcomes revealed that there is a positive relationship between SWA and counselor self-efficacy, as well as between the counselor’s perception of the counselor–client relationship (Park et al., 2019). Taken together, one may hypothesize that the sample of the current study experienced positive SWA and as a result demonstrated positive self-efficacy in their service provision, which served as a protective factor from the negative effects of the pandemic.
Toward a Universal Design for Rehabilitation
Moving toward UD in rehabilitation practice is an inescapable need for the future of the rehabilitation profession. Much literature and research about UD has centered on Universal Design for Learning; however, the principles of UD apply handily to counseling environments, and particularly VR (Sheppard-Jones et al., 2021). The principles of UD lend themselves to applicability across all domains, which is a hallmark of the goals of UD (Story, 1998). Most succinctly, using UD in any arena ensures the usability of a given product or service by the most people possible, especially and intentionally, disabled people. For example, participants of a current study by Anderson, Hergenrather, and Jones (2021) regarding the experiences of marginalized groups using VR services indicated that they are often late to appointments as a result of public transportation issues; a UD approach to this would be to allow all consumers the option to elect to meet with their counselor remotely, and to have the accommodations available for them to do so without issue.
In the current study, while there was very high agreement among participants that they are able to use accessible technology and to create accessible Portable Document Format (PDFs) for clients, there was primarily neutral and disagreement when asked directly about UD. This finding is potentially due to the fact that rehabilitation counselors may be unaware of UD. The two most recent essential competency studies in rehabilitation counseling do not include UD nor competence with using or creating accessible materials for counseling or case management purposes ( Leahy et al., 2013, 2019). Universal design is also absent from the CRC Code of Ethics and the Council for Accreditation of Counseling and Related Educational Programs (CACREP) Standards (2016). Including UD as a component of VR would not only improve the services provided to clients, but it will also allow counselors to navigate the increasing reliance more adequately on technology in VR (Sheppard-Jones et al., 2021). The spirit of UD is the same as that which rehabilitation counseling has been built upon: improving inclusion and accessibility for all people. As such, this is an avenue that clearly needs to be built upon in post-pandemic service provision.
Limitations
Unfortunately, data collection for this study took place during a global pandemic, during which time it was difficult to secure a more significant sample size thus limiting the ability to analyze the data in more depth. In addition, although the researchers attempted to contact additional VR offices for participation in the current study, it was not possible to secure a site for additional distribution. These factors can be attributed to the pandemic: the pandemic created an increase in reliance on email communication, thus the sample recruited may be those who had an easier time managing their inboxes as compared with their peers who did not respond. Similarly, it was necessary for the study to capture a moment in time when regulations were not in flux and state-level guidance had not yet been changed due to a decrease in cases or the introduction of the vaccine. It may have benefited researchers to sample counselors at multiple points in time during the pandemic which would have demonstrated the changes in how the pandemic impacted rehabilitation counselors’ perceptions over time and to illustrate the impact of such an acute shift in work format affected their experiences with supervisors and clients.
Implications
The current study reveals that the sample of VR counselors who participated was well trained and well prepared to navigate the myriad effects of the pandemic on their work roles. However, given that the pandemic and its effect on social programs such as VR are still ongoing and unknown, future research may reveal more detailed information about the impact of COVID-19 on VR service provision. The current study was an investigation into one state VR agency; replication studies to identify needs across the country must be done to better understand the nuances of needs identified by counselors, and to determine next steps such as training, resources, and interventions. Additional research should also seek to understand if the SWA is indeed a protective factor during a time of crisis, as well so to explore the effect of the SWA on counselor’s perceived preparedness and self-efficacy specifically in VR.
Responses in the current study generally indicated a lack of issue with providing services remotely. Researchers must uncover if this same finding can be replicated when surveying clients receiving those services, especially regarding the working alliance. Understanding client needs at this time is essential to effectively overcome this global crisis. Employer attitudes about remote work may have changed due to the pandemic, and data about the impact of the pandemic on those attitudes would likely help counselors and clients secure remote accommodations in the future. In addition, disabled academics have placed a call to action to draw attention to the additional trauma and stress experienced by disabled people as a result of factors such as the rationing of care, ableism, and isolation which occurred during the pandemic (Lund et al., 2020).
For Supervisors
Supervisors must be aware of the findings of the current study to potentially avoid increases in turnover intentions among counselors. Perhaps even more importantly, throughout VR agencies, it is essential for leadership to acknowledge the impact of divisive social rhetoric and the spreading of misinformation on conversations that counselors may (or may not) be having with clients. Difficult conversations must be happening during VR counseling processes or clients are not adequately being prepared for success in an inclusive, competitive environment. Not only do counselors need to be able to navigate and critically consume media, but they must also be able to support and guide vulnerable clients in doing the same. Supervisors can scaffold opportunities for learning and perfecting microskills such as confrontation, to support counselors in developing these skills.
The results of the current study indicate the importance of supervisor availability and presence during uncertain times. While the delineation of administrative and clinical supervision is certainly important (e.g., as described by Sabella et al., 2021), capturing that detail fell outside the scope of the current study. However, the consistent availability of supervisors, as indicated by the current sample, may be related to the high levels of comfort with a shift to telehealth and remote work indicated by participants. Supervisors must be mindful of maintaining their availability to their supervisees, in whatever format possible (e.g., phone, email, video call).
For Educators
Results of the current study indicate that the sample felt highly prepared to shift to virtual service provision. Although several items may have been aspirational (e.g., proficiency in technology and the use of UD), the high levels of overall comfort with virtual service provision underscore the importance for educators to be infusing technology across program domains. A large proportion of responses indicated that the counselors surveyed seek out additional opportunities to learn about technology; training programs are the starting point for developing these skills and providing those training opportunities. Hartley and Bourgeois (2020) also draw attention to important factors educators must be mindful of as there is an increase in technology as a component of VR service delivery. For example, ethical considerations related to using social media, text messaging, protecting client privacy, and ensuring client safety are all increasingly of concern during remote, or technology-centered service provision. Awareness of and the ability to assess such issues must be included in the content students are learning in CACREP-accredited rehabilitation counseling programs.
Conclusions
More than revealing the needs of VR counselors during the COVID-19 pandemic, the current study revealed the resilience of VR counselors during this trying time. Counselors reported being able to maintain the implementation of evidence-based practices and building positive rapport with clients, even while living through a global pandemic themselves. The sample overwhelmingly indicated that their supervisor was readily available and understood what they were going through. This study’s findings additionally may indicate that the role of the supervisor becomes even more significant during a time of heightened stress and uncertainty. Leadership in all spaces throughout the field should not simply wait to “return to normal,” rather should use the current situation as a means to reinvigorate professional development opportunities and training that will ultimately improve services provided and prepare current and future counselors for any such situation that may arise again in the future.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.