
Abstract
Objectives:
Pandemic-related worries and stressors were common during the COVID-19 pandemic. The objective of this study was to examine pandemic-related worries and stressors in relation to tobacco and alcohol use among postpartum women in the United States early in the COVID-19 pandemic.
Methods:
From May through June 2020, 792 postpartum women in the United States completed an electronic survey, the COVID-19: Health in Pregnancy and Postpartum Study. The survey assessed pandemic-related worries by using a summary score of 10 items and pandemic-related stressors by using 4 items. The primary outcomes were tobacco and alcohol use. Secondary outcomes were increased amounts of tobacco and alcohol during the pandemic among participants who used tobacco and/or alcohol. We used logistic regression models to examine the association of pandemic-related worries and stressors with each outcome.
Results:
Among postpartum women, 24.4% used tobacco and 27.8% used alcohol. Pandemic-related worries were associated with higher odds of tobacco use (adjusted odds ratio [AOR] = 1.08; 95% CI, 1.04-1.13), alcohol use (AOR = 1.09; 95% CI, 1.05-1.13), and using both tobacco and alcohol postpartum (AOR = 1.13; 95% CI, 1.07-1.20). Both worries and stressors were associated with increased tobacco use (AOR for worries = 1.08; 95% CI, 1.01-1.16; AOR for stressors = 2.00; 95% CI, 1.33-3.00) but not with increased alcohol use.
Conclusions:
The association between pandemic-related worries and stressors and tobacco use underscores the need for health promotion interventions among postpartum women to reduce tobacco use. Developing pandemic-related interventions now for use in future pandemics to alleviate pandemic-related worries and stressors experienced by postpartum women is warranted.
Levels of pandemic-related worries and stressors were high at the start of the COVID-19 pandemic, 1 with women experiencing higher levels of stress and worry than men.2,3 The postpartum period is the time following childbirth, lasting up to 1 year.4,5 This period is a unique life stage during which women recover from childbirth4,6 and provide care for the newborn and other family members. Mental health among women during the postpartum period has been identified as a major public health issue. 7 Furthermore, the COVID-19 pandemic resulted in higher stress levels among postpartum women during the pandemic than before the pandemic.8,9 These stress levels are consistent with observations of increased pandemic-related worries about COVID-19 infections among family and friends, inability to provide appropriate childcare, and reduced visits with family after childbirth. 10
During the COVID-19 pandemic, people in the general US population were observed to use tobacco and alcohol to cope with pandemic-related worries and stressors.11-17 Purchases of tobacco and alcohol in all US regions increased during this period. 18 In the United States, pandemic-related worry was positively associated with coping motives to smoke among adults who smoked daily, 14 and at least 1 study found that worry due to financial problems was associated with increased cigarette smoking. 11 High perceived stress was associated with increased cigarette smoking among adults who currently or formerly smoked.11-13 Several studies showed that higher levels of COVID-19–related stress were associated with greater alcohol consumption.15-17
Studies on pandemic-related worry and stress and the use of tobacco and alcohol have primarily focused on the general population. These studies have often underrepresented postpartum women, an important population group because it faces unique and particularly intense or disruptive stressors and worries8-10 during the time of recovery from childbirth.4-6 These studies leave a critical gap in understanding how postpartum women navigate these challenges. Substantial bodies of evidence document that tobacco and alcohol use increase risks among women for hypertension, cardiovascular diseases, and several malignancies. 19 Furthermore, postpartum tobacco use increases maternal morbidity and mortality and adversely affects children’s health due to secondhand smoke exposure.20,21 Postpartum alcohol misuse increases the risk of neglecting and abusing children and worsening the mother–child relationship.22,23 Drinking up to 1 alcoholic drink per day does not show harm to infants,24,25 but guidance from the Centers for Disease Control and Prevention (CDC) indicates the safest approach for breastfeeding mothers is to abstain from alcohol drinking. 25 While the health outcomes of tobacco and alcohol use are well-established, their simultaneous use and how these behaviors changed during an unprecedented public health emergency, the COVID-19 pandemic, potentially compounding health risks for both mothers and infants, remain understudied.
The COVID-19 pandemic was a unique period during which people faced increased worries and stressors 1 ; the effects of the pandemic may have been especially acute among postpartum women. Increasing understanding of how worries and stressors might influence health behaviors such as tobacco and alcohol use among postpartum women during the COVID-19 pandemic can provide insights to help prepare for future pandemics or crises. For these reasons, we conducted the current study among postpartum women to examine how pandemic-related worries and stressors were associated with tobacco and alcohol use early in the COVID-19 pandemic, and to further assess their association with the joint and increased use of tobacco and alcohol.
Methods
Study Population
Data came from the COVID-19: Health in Pregnancy and Postpartum (CHIPP) study. CHIPP was a cross-sectional electronic survey designed to examine how the COVID-19 pandemic influenced pregnancy and postpartum health, health behaviors, and access to perinatal care in the United States.26,27 The postpartum survey was conducted from May 21 through June 11, 2020. To recruit a diverse sample, CHIPP advertised the study through community health programs serving predominantly racial and ethnic minority or low-income women and through group Facebook accounts focused on people in racial and ethnic minority populations. The recruitment cap limited the target sample size to 50% African American women. The inclusion criteria for the survey were being a US resident, being aged 18 to 44 years, and having delivered a singleton baby in a US hospital at any time from March 2020 through the survey date. Among 865 survey participants, we excluded 4 participants for not meeting inclusion criteria and 69 participants for missing values for key variables, such as tobacco use and alcohol use, resulting in 792 participants in our analysis.
This study’s protocol was approved by the institutional review board at the University of South Carolina (exempt status), and all respondents gave informed consent to participate in the study.
Measures
The primary independent variables were pandemic-related worries and stressors. The CHIPP study modified the Cambridge Worry Scale 28 for postpartum women and the pandemic setting. Ten questions assessed pandemic-related worries: (1) giving birth in the hospital setting; (2) changing birth plans; (3) their new baby; (4) friends and family; (5) stigma or discrimination from other people; (6) having enough basic supplies; (7) not getting baby supplies; (8) getting emotional or social support from family, friends, partners, a counselor, or someone else; (9) getting financial support from family, friends, partners, and organizations; and (10) other difficulties or challenges. Responses were measured on a 5-point Likert scale ranging from not at all (0) to all the time (4). The total score of the pandemic-related worries (range: 0-40) was the sum of responses to the 10 items on worries. The survey used the Pandemic Stress Index 29 to measure pandemic-related stressors, which included the following 4 items: (1) participants getting tested for COVID-19, (2) losing income due to COVID-19, (3) family members testing positive for COVID-19, and (4) family deaths in or outside the household due to COVID-19 or related complications. We examined each stressor individually and as a composite measure by summing the 4 pandemic-related stressors (range: 0-4).
The primary dependent variables were tobacco and alcohol use. The term “tobacco use” refers to using combustible and noncombustible tobacco products and electronic nicotine delivery systems. Questions asked participants about using combustible tobacco cigarettes and other tobacco/nicotine products such as electronic cigarettes (e-cigarettes), hookahs, smokeless tobacco, and cigars, cigarillos, or little filtered cigars. We measured the postpartum use of combustible tobacco cigarettes in the following categories: never used, used throughout the pregnancy, or resumed smoking in 0 to 1 month, 2 to 3 months, or ≥4 months after childbirth. Additionally, the survey asked participants about their use of other tobacco products at survey time. We classified participants as negative for tobacco use if they did not use any tobacco products and positive for tobacco use if they reported any tobacco product use during the postpartum period.
We assessed the number of alcoholic drinks participants consumed in an average week since the new baby was born during the pandemic by using the following survey categories: no drinking and <1, 1 to 3, 4 to 6, 7 to 13, and ≥14 drinks per week. We considered use of ≥1 drink per week to be positive for alcohol use. We classified joint use of tobacco and alcohol by using the following categories: nonuse, tobacco use only, alcohol use only, and use of both tobacco and alcohol. We based these analyses on the consideration of alcohol drinking as a health behavior, rather than a health risk, according to CDC guidelines for alcohol drinking among breastfeeding postpartum women. 25
Participants who reported they used tobacco and/or alcohol were also asked if they increased their postpartum use of these products during the pandemic. We used 2 categories to assess any changes in tobacco use among participants who used tobacco since the start of the pandemic: increased tobacco use and no increased tobacco use. We used the same classification for participants who consumed alcohol.
Besides the independent variables of pandemic-related worries and stressors and dependent variables of tobacco and alcohol use, the survey collected data on the following variables for assessment for potential confounding30,31: maternal age, race and ethnicity, education, health insurance, parity, annual household income, chronic health conditions, completion of a postpartum checkup, and preterm birth.
Statistical Analysis
We used Pearson χ2 tests of independence to determine if characteristics of participants differed significantly according to use and nonuse of tobacco and alcohol. We used multiple logistic regression models to measure the associations of pandemic-related worries and stressors with 2 outcomes for postpartum tobacco use: (1) tobacco use among all postpartum women and (2) increased use among tobacco users. We used the same approach for alcohol use. Furthermore, we used multinomial models to assess the association between the joint use of tobacco and alcohol. For each model, we simultaneously considered pandemic-related worries and stressors by adjusting for worries while studying the independent association of stressors with postpartum tobacco use, and vice versa. In these analyses, we assessed the associations for both individual items and total scores of worries and stressors when we evaluated worries or stressors as the primary independent variable, whereas we used only the total scores for the adjustment when adjusting for worries/stressors. We conducted sensitivity analyses that modeled pandemic-related worries and stressors separately to assess their independent association with tobacco and/or alcohol use. We estimated adjusted odds ratios (AORs) and 95% CIs. We used SAS version 9.4 (SAS Institute, Inc) to perform all analyses.
Results
Overall, most participants were aged 25 to 34 years (80.1%), had a bachelor’s degree or higher (70.6%), were nulliparous before their recent pregnancy (73.7%), and had postpartum checkups (77.7%) (Table 1). The percentage of women who self-identified as non-Hispanic African American, non-Hispanic White, and Other was 45.5%, 38.4%, and 16.2%, respectively. More than one-fourth (29.3%) of participants were enrolled in Medicaid and 48.5% had an annual household income <$50 000. The prevalence of chronic diseases was 11.9%. Preterm deliveries accounted for 15.7% of all deliveries.
Characteristics of postpartum women early in the COVID-19 pandemic, by tobacco use and alcohol use, United States, May–June 2020 a
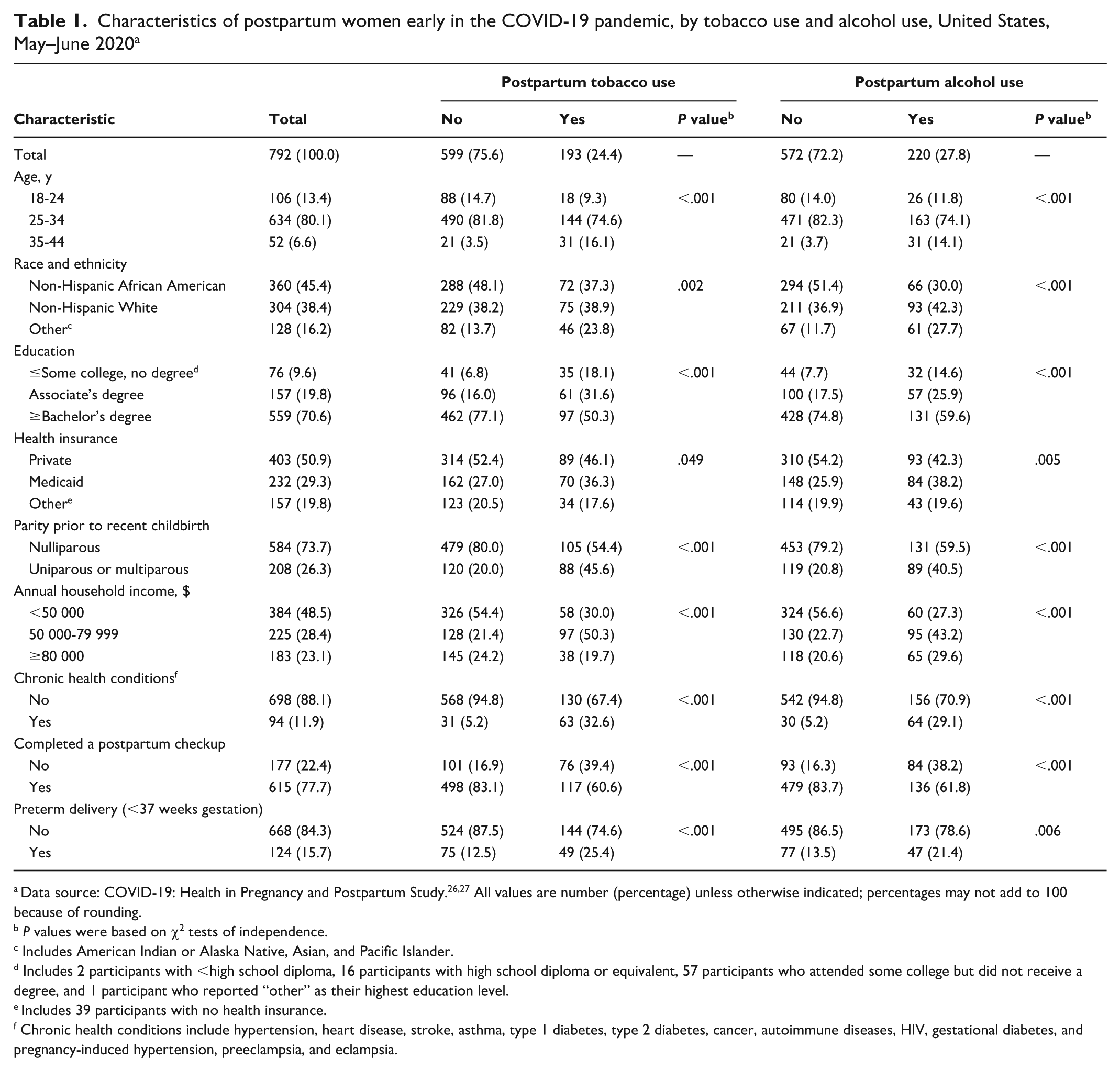
Data source: COVID-19: Health in Pregnancy and Postpartum Study.26,27 All values are number (percentage) unless otherwise indicated; percentages may not add to 100 because of rounding.
P values were based on χ2 tests of independence.
Includes American Indian or Alaska Native, Asian, and Pacific Islander.
Includes 2 participants with <high school diploma, 16 participants with high school diploma or equivalent, 57 participants who attended some college but did not receive a degree, and 1 participant who reported “other” as their highest education level.
Includes 39 participants with no health insurance.
Chronic health conditions include hypertension, heart disease, stroke, asthma, type 1 diabetes, type 2 diabetes, cancer, autoimmune diseases, HIV, gestational diabetes, and pregnancy-induced hypertension, preeclampsia, and eclampsia.
The prevalence of tobacco use was 24.4%. Among those who used tobacco, the prevalence of using e-cigarettes, cigarettes, smokeless tobacco, hookahs, and cigars/cigarillos/little filtered cigars was 85.0%, 74.6%, 64.3%, 61.7%, and 54.4%, respectively. All maternal characteristics were significantly associated with postpartum tobacco and alcohol use (Table 1).
The mean score of pandemic-related worries was significantly higher among participants who used tobacco compared with those who did not (20.4 vs 18.0; P < .001) (Table 2). For every point increase in pandemic-related worry score, the odds of using tobacco increased by 8% (AOR = 1.08; 95% CI, 1.04-1.13). The mean of pandemic-related stressors was significantly higher among those who used tobacco than among those who did not (1.6 vs 1.2; P < .001). The total number of pandemic-related stressors did not significantly differ between those who did versus did not use tobacco postpartum, and the only stressor significantly associated with postpartum tobacco use was a COVID-19–related family death (AOR = 1.92; 95% CI, 1.04-3.56).
Associations of COVID-19–related worries and stressors with tobacco use and alcohol use among postpartum women early in the COVID-19 pandemic, United States, May–June 2020 a
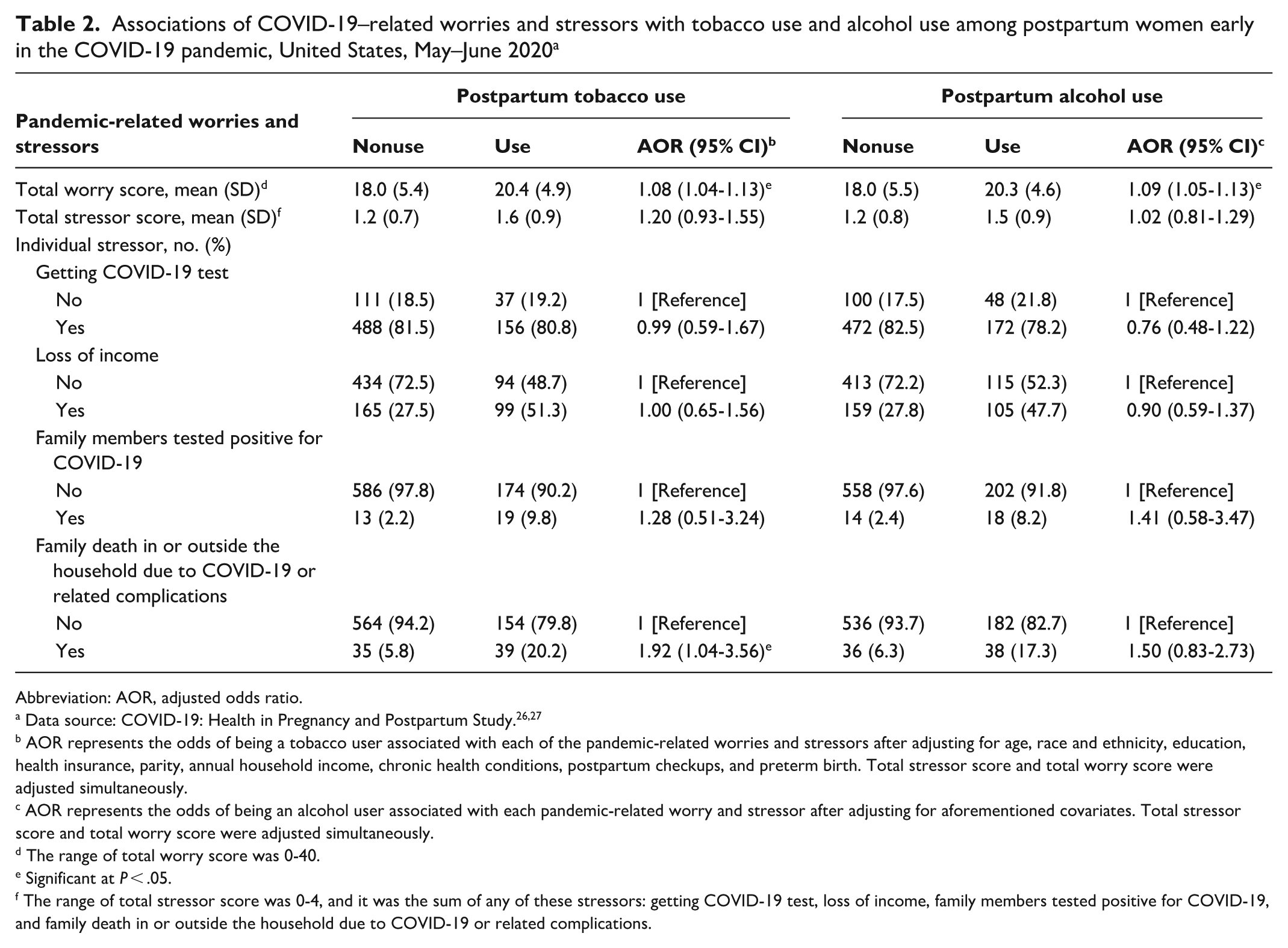
Abbreviation: AOR, adjusted odds ratio.
AOR represents the odds of being a tobacco user associated with each of the pandemic-related worries and stressors after adjusting for age, race and ethnicity, education, health insurance, parity, annual household income, chronic health conditions, postpartum checkups, and preterm birth. Total stressor score and total worry score were adjusted simultaneously.
AOR represents the odds of being an alcohol user associated with each pandemic-related worry and stressor after adjusting for aforementioned covariates. Total stressor score and total worry score were adjusted simultaneously.
The range of total worry score was 0-40.
Significant at P < .05.
The range of total stressor score was 0-4, and it was the sum of any of these stressors: getting COVID-19 test, loss of income, family members tested positive for COVID-19, and family death in or outside the household due to COVID-19 or related complications.
Most participants (72.2%) reported no alcohol consumption (Table 1). Among participants who consumed alcohol postpartum (27.8%), the prevalence of number of drinks per week was 7.7% for <1 drink per week, 14.7% for 1 to 3 drinks per week, 5.1% for 4 to 6 drinks per week, and 0.4% for 7 to 13 drinks per week. The mean pandemic-related worry score was significantly higher among those who used alcohol compared with those who did not (20.3 vs 18.0; P < .001) (Table 2). For every point increase in the pandemic-related worry score, the adjusted odds of using alcohol increased by 9% (AOR = 1.09; 95% CI, 1.05-1.13). The mean number of pandemic-related stressors was significantly higher among those who used alcohol compared with those who did not (1.5 vs 1.2; P < .001). However, after adjusting for covariates, postpartum alcohol use was not associated with the total number of stressors or any individual stressor.
In the assessment of pandemic-related worries in relation to the joint use of tobacco and alcohol, the total worry score was associated with higher odds of using alcohol only (AOR = 1.07; 95% CI, 1.02-1.13) and using both tobacco and alcohol postpartum (AOR = 1.13; 95% CI, 1.07-1.20) (Table 3). The total number of pandemic-related stressors was not associated with the joint use of tobacco and alcohol. The only stressor associated with higher odds of combined use of tobacco and alcohol was a COVID-19–related family death (AOR = 2.28; 95% CI, 1.06-4.91).
Pandemic-related worries, stressors, and joint use of tobacco and alcohol among postpartum women early in the COVID-19 pandemic, United States, May–June 2020 a
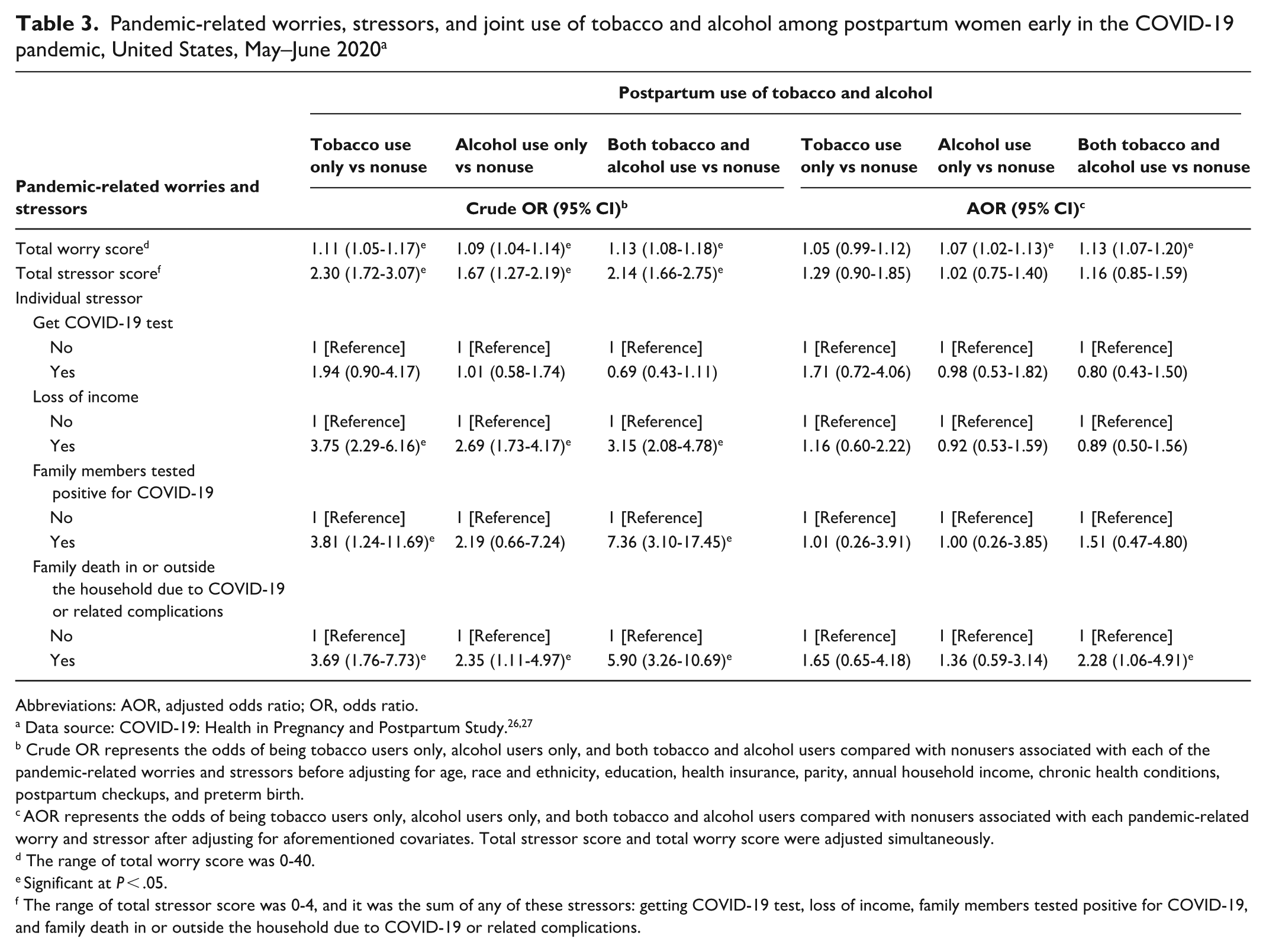
Abbreviations: AOR, adjusted odds ratio; OR, odds ratio.
Crude OR represents the odds of being tobacco users only, alcohol users only, and both tobacco and alcohol users compared with nonusers associated with each of the pandemic-related worries and stressors before adjusting for age, race and ethnicity, education, health insurance, parity, annual household income, chronic health conditions, postpartum checkups, and preterm birth.
AOR represents the odds of being tobacco users only, alcohol users only, and both tobacco and alcohol users compared with nonusers associated with each pandemic-related worry and stressor after adjusting for aforementioned covariates. Total stressor score and total worry score were adjusted simultaneously.
The range of total worry score was 0-40.
Significant at P < .05.
The range of total stressor score was 0-4, and it was the sum of any of these stressors: getting COVID-19 test, loss of income, family members tested positive for COVID-19, and family death in or outside the household due to COVID-19 or related complications.
Among participants who reported postpartum tobacco use (n = 193), a 1-point increase in the pandemic-related worry score was associated with higher odds of increased tobacco use during the pandemic (AOR = 1.08; 95% CI, 1.01-1.16) (Table 4). Every additional pandemic-related stressor was associated with higher odds of increased tobacco use (AOR = 2.00; 95% CI, 1.33-3.00). Compared with participants who did not experience a COVID-19–related family death, those who did had 5.17 times higher odds of reporting increased tobacco use (AOR = 5.17; 95% CI, 1.99-13.46). Among participants who reported using alcohol (n = 220), those who experienced a COVID-19–related family death had higher odds of reporting increased alcohol use than those who did not experience such a death (AOR = 2.47; 95% CI, 1.12-5.45). Pandemic-related worries and other pandemic-related stressors were not associated with a change in alcohol use.
Correlates of changes in tobacco use and alcohol use among postpartum women early in the COVID-19 pandemic, United States, May–June 2020 a
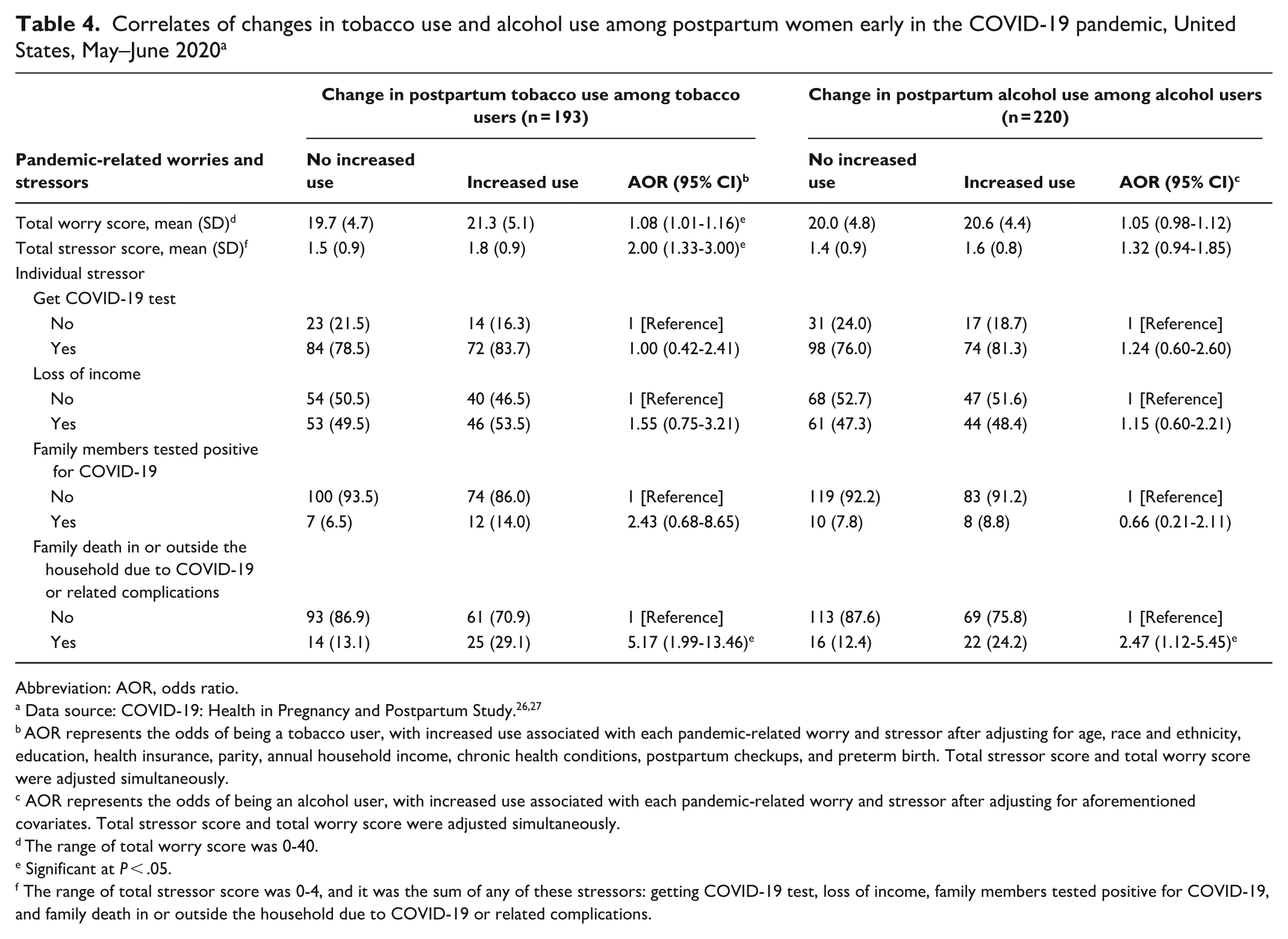
Abbreviation: AOR, odds ratio.
AOR represents the odds of being a tobacco user, with increased use associated with each pandemic-related worry and stressor after adjusting for age, race and ethnicity, education, health insurance, parity, annual household income, chronic health conditions, postpartum checkups, and preterm birth. Total stressor score and total worry score were adjusted simultaneously.
AOR represents the odds of being an alcohol user, with increased use associated with each pandemic-related worry and stressor after adjusting for aforementioned covariates. Total stressor score and total worry score were adjusted simultaneously.
The range of total worry score was 0-40.
Significant at P < .05.
The range of total stressor score was 0-4, and it was the sum of any of these stressors: getting COVID-19 test, loss of income, family members tested positive for COVID-19, and family death in or outside the household due to COVID-19 or related complications.
Sensitivity analyses modeling pandemic-related worries and stressors separately for all outcomes yielded results consistent with the main analyses, suggesting that the analytic approach of including worries and stressors in the same model did not meaningfully affect results.
Discussion
This study was conducted among postpartum women in the United States early in the COVID-19 pandemic to assess the potential effect of the pandemic on tobacco and alcohol use. Approximately one-fourth of the study population used tobacco (24.4%) and a similar proportion used alcohol (27.8%). The prevalence of tobacco use was substantially higher than the national estimate for women in 2020 (13.9%), 32 which is concerning. Electronic nicotine delivery systems were the most commonly used tobacco products and the prevalence of high-risk drinking (>7 drinks per week or >3 drinks in 1 day) was rare in this study population. 33
The most notable associations were for pandemic-related worries rather than stressors and for tobacco use or the combined use of tobacco and alcohol but not alcohol alone. Pandemic-related worries were associated with tobacco use and increased tobacco use. Total pandemic-related stressors were also associated with increased tobacco use, largely driven by the strong association between a COVID-19–related family death and increased tobacco use. Additionally, pandemic-related worries were significantly associated with alcohol use but not with increased alcohol use. Postpartum women with higher pandemic-related worry scores had significantly greater odds of using alcohol alone or both tobacco and alcohol than those with lower pandemic-related worry scores.
The overall study results suggest that postpartum women might have used tobacco to cope with worries and stressors early in the COVID-19 pandemic. These findings are consistent with results in the general population.12-17 In addition to pandemic-related worries and stressors, postpartum women routinely face worries and stressors unique to the postpartum period, including postpartum depression, infant feeding, and postnatal care.
Strengths and Limitations
Our study had several strengths. For one, our study, to our knowledge, is the only study to report on pandemic-related worries and stressors in relation to tobacco and alcohol use among postpartum women, a population frequently overlooked in pandemic-related behavioral research, early in the COVID-19 pandemic, when COVID-19 caused large spikes in disease and death and led to widespread lockdowns. 34 Our study was unique in that it examined tobacco use, alcohol use, and pandemic-related changes in use. Our findings provide evidence that external crises may be associated with changes in health behavior among postpartum women. The study population resided throughout the United States and was diverse, with a high proportion of African American women (45.5%).
Our study also had several limitations. First, tobacco and alcohol use were self-reported, but prior studies found that self-reported smoking history was valid and strongly correlated with actual smoking status. 35 Second, the study adapted the Cambridge Worry Scale 28 and the Pandemic Stress Index 29 to assess pandemic-related worries and stressors among postpartum women, which were commonly used among the general population but had not been validated among postpartum women. Third, the cross-sectional design meant we could not definitively determine the temporal sequence between pandemic-related worries and stressors and postpartum tobacco and alcohol use. Fourth, our convenience sampling method yielded a sample primarily composed of women aged 25 to 44 years, with high proportions of African American and non-Hispanic White women, often associated with greater tobacco use than other groups of women,36,37 and individuals with higher socioeconomic status, typically related to less use of tobacco compared with those with lower socioeconomic status. 37 Fifth, the higher prevalence of tobacco use observed in our study, compared with other studies, may be due to pandemic-related stress11-13 and differences in measurement compared.36,37 Our study used online surveys of a sample population to examine any tobacco use during the postpartum period. Consequently, our prevalence estimates should be interpreted cautiously as specific to this sample. Sixth, we conducted the study early in the pandemic, when pandemic worries and stressors were very high, so the findings are most relevant to the early phase of the COVID-19 pandemic. Finally, we did not adjust for preexisting depression or anxiety. Preexisting anxiety-related disorders are associated with elevated pandemic-related worries and stressors. 38 However, considering the low prevalence of respondents diagnosed with depression or anxiety during pregnancy in our sample (3.5%) and that survey participants may have been motivated by higher (or lower) worries or stressors, the influence of preexisting depression or anxiety on perceived worries and stressors is likely limited.
Conclusions
Tobacco and alcohol use are risk factors for cardiovascular diseases, hypertension, and multiple malignancies. 19 The high prevalence of tobacco and alcohol use among postpartum women early in the COVID-19 pandemic indicates that preventing tobacco and alcohol use among postpartum women should be considered a high public health priority. The high prevalence also implies the psychosocial effect of a pandemic, suggesting that investing in developing interventions now would be helpful to prepare for future pandemics or crises. Observed associations between pandemic-related worries and stressors and postpartum tobacco and alcohol use suggest the need for educational interventions to increase the awareness of mothers and their families of the health risks associated with postpartum tobacco and alcohol use. Educating family members to be aware of the mental health of postpartum mothers resulting from the usual stressors of the postpartum period as well as from any pandemic- or trauma-related worries would likely be beneficial. 7 Postpartum health care providers should support not only the physical well-being of postpartum women but also their social and psychological well-being, 39 particularly when worries and stressors are elevated, such as during pandemics. Bettering the delivery of health care to postpartum women (eg, by improving access to virtual assessments of substance use and well-being) is worthy of future evaluation.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Office of the Vice President for Research, University of South Carolina. The time of coauthors J. Liu and P. Hung was partially supported by the National Institutes of Health (NIH) under award no. 3R01AI27203-5S2. The content is solely the responsibility of the authors and does not necessarily reflect the official views of NIH or the Office of the Vice President for Research, University of South Carolina.