
Abstract
Objectives:
Understanding COVID-19 vaccination behavior can guide public health efforts to increase vaccination acceptance and uptake. We examined COVID-19 vaccination intention among Wisconsin residents and assessed racial and ethnic disparities in vaccine uptake.
Methods:
We assessed vaccination intention during COVID-19 testing registration in February 2021 and used the Wisconsin Immunization Registry to ascertain COVID-19 vaccination uptake by July 2022. We described differences in intention to get vaccinated and assessed the association between racial and ethnic identity and vaccination. We analyzed vaccination likelihood by using Cox proportional hazards models and presented adjusted hazard ratios (AHRs) with 95% CIs.
Results:
Of 12 196 people, 9843 (80.7%) intended to be vaccinated against COVID-19. A higher proportion of non-Hispanic Black people (21.1%) than people in all other racial and ethnic groups did not intend to get vaccinated. Adjusting for vaccination intention, age group, sex, and neighborhood Area Deprivation Index, Hispanic people were 41% (AHR = 0.59; 95% CI, 0.54-0.64) less likely than non-Hispanic White people to get vaccinated. Compared with non-Hispanic White people, non-Hispanic Black people were 24% (AHR = 0.76; 95% CI, 0.68-0.84) less likely to get vaccinated and Asian people were 18% (AHR = 0.82; 95% CI, 0.75-0.90) less likely to get vaccinated.
Conclusions:
Racial and ethnic disparities in vaccination uptake persisted despite controlling for intention. Efforts to focus public health resources on increasing COVID-19 vaccination among racial and ethnic minority groups are important.
Vaccination against COVID-19 is a major public health strategy for reducing risk for severe illness and death. As of May 2024, approximately 111 million cases of COVID-19 had been documented in the United States, including 6.8 million hospitalizations and 1.2 million deaths. 1 During 2020-2022, a disproportionate number of COVID-19–related cases, hospitalizations, and deaths were reported among non-Hispanic Black, Hispanic, and American Indian or Alaska Native populations.1-4 In December 2020, less than 1 year after the United States declared a public health emergency, 5 the first COVID-19 vaccines became publicly available. 6 The United States implemented a phased approach to prioritize vaccinating adults at elevated risk for severe disease or exposure; by May 2021, all adults were eligible. 7 As of May 2023, approximately 668 million COVID-19 vaccine doses had been administered, and 86% of people in the United States aged ≥5 years had received ≥1 COVID-19 vaccine dose; however, approximately 15% of US adults were unvaccinated.2,7
Vaccination intention (eg, vaccine hesitancy) and uptake vary by racial and ethnic identity. After the COVID-19 vaccine became publicly available, evidence of racial and ethnic disparities in vaccination were apparent in the United States. In the United States, non-Hispanic Black and Hispanic people had lower COVID-19 vaccination rates than White and Asian people.8,9 Low vaccination coverage among these racial and ethnic groups could have been related to a lack of vaccine prioritization for racial and ethnic minority groups despite support for equitable vaccine allocation. 10 Low vaccination rates posed risk for severe illness and death in these populations and perpetuated health inequities.9,11-13 Explanations for lower vaccination rates among racial and ethnic minority groups than among other racial and ethnic groups might be partially explained by vaccine hesitancy. Vaccine hesitancy is defined as refusal or delay in acceptance of vaccination despite availability and has been identified as among the top 10 threats to global health by the World Health Organization.14,15 Hesitancy toward vaccines has been growing for decades among US adults across all racial and ethnic identities and was seen during the COVID-19 pandemic.14,16 Multiple explanations for vaccine hesitancy exist among adults, including mistrust of vaccine science, fear of side effects, or perceptions that risk for disease is low.15,16 Hesitancy among racial and ethnic minority groups may be further compounded by decades of discrimination and trauma that have led to mistrust of the health care system by non-Hispanic Black, Hispanic, and American Indian and Alaska Native people, leading them to be more likely than non-Hispanic White people to express hesitancy. But the drivers of vaccination behavior can be explained by more than hesitancy, are complex, and differ greatly by population.
Although studies have identified hesitancy as a primary driver of vaccination behavior, the effect of social determinants of health (eg, health care access, transportation, other socioeconomic factors) have been less well-studied.11,12 Social determinants of health have been measured in many ways, one of which is the Area Deprivation Index (ADI),17,18 which measures socioeconomic disadvantage. Socioeconomic disadvantage is a construct reflecting experiences of poverty, lack of access to health care, and other limitations on financial and social resources, which are directly related to the likelihood a person is to get vaccinated. We hypothesized that socioeconomic disadvantage likely has a role in COVID-19 vaccination behavior even when a person intends to get vaccinated.16,19,20 The role of socioeconomic disadvantage in COVID-19 vaccination behavior might partially explain lower vaccination rates among racial and ethnic minority groups, which have a disproportionate amount of disadvantage in the United States, than among White people.15,21-24 Vaccine hesitancy and the overlapping effects of socioeconomic disadvantage can compound to further worsen vaccination outcomes.22-24
Understanding that intention is a key predictor of vaccination behavior, we described vaccination uptake throughout a 17-month follow-up period among a study cohort of heterogenous intention. We examined COVID-19 vaccination by race and ethnicity and investigated ADI at the neighborhood level as an effect modifier. We conducted this analysis among a cohort of Wisconsin residents during February 2021–July 2022.
Methods
Study Design
The Wisconsin Department of Health Services (DHS) conducted a retrospective study among a cohort of Wisconsin residents who answered a vaccination intention question when registering for a COVID-19 test at 1 of several DHS-supported community testing sites during February 7-28, 2021. We excluded children and adolescents aged <16 years who were not authorized to receive a vaccine and people who self-identified as health care workers who were already likely to have been vaccinated based on eligibility criteria. We included people who provided an answer for the intention question in the cohort and subsequently linked them to the Wisconsin Electronic Disease Surveillance System (WEDSS) for COVID-19 test results and the Wisconsin Immunization Registry (WIR) for vaccination status. We also collected data on demographic characteristics such as race, ethnicity, sex, age group, occupation, industry, and census-block group based on residential address. We gathered these data through the COVID-19 testing registration form. Data on race and ethnicity were self-reported during test registration; if data on race and ethnicity were missing, we used race and ethnicity reported in WEDSS to increase completeness. We excluded people whose information on race and ethnicity was still missing after this step. We used occupation and industry information to exclude health care workers. The registration form included a question, “Are you a healthcare worker?” and free-text industry and occupation questions that were coded through the National Institute for Occupational Safety and Health’s Industry and Occupation Computerized Coding System. 25 We considered people who responded yes to the health care worker question or whose industry subsector was ambulatory health care services, hospitals, or nursing and residential care to be health care workers, and we excluded these respondents from analysis.
Assessing Vaccine Intent
We captured responses about intent to get vaccinated through the Dynamics Testing and Registration Application (DTRA), an online registration platform used to collect and manage patient data for COVID-19 community testing sites in Wisconsin. DHS-supported community testing sites for COVID-19 served approximately 30 of 72 counties across Wisconsin. DTRA managed online registration for testing. Registration contained a supplemental questionnaire that included a single question about vaccination intention: “When a vaccine is available, how likely will you be to get it?” Answers were on a 4-point Likert scale, where 1 = definitely will not get it, 2 = probably will not get it, 3 = probably will get it, and 4 = definitely will get it. The questionnaire was provided in English and required access to the internet or an internet-capable device to access registration.
Wisconsin Immunization Registry
WIR is an online database for the report of immunizations administered in Wisconsin. WIR requires reporting of all COVID-19 vaccinations administered in the state. We extracted data on COVID-19 vaccinations for people whose testing records were located in WEDSS based on a complete match of first name, last name, sex, and date of birth. We followed this matching by manually checking all unmatched names to increase accuracy. All positive and negative COVID-19 test results are reported in WEDSS; we excluded from analysis people who could not be matched to a COVID-19 test record in WEDSS. Data obtained from WIR included the name of the vaccine, number of doses, and administration date. We defined vaccination as a single dose of Janssen (Johnson & Johnson), Pfizer-BioNTech, or Moderna COVID-19 vaccine during March 2, 2021–July 30, 2022. We considered first doses of vaccination in this analysis to evaluate the specific follow-up action because it was associated with original intention. We considered people without a vaccination record during the study period to be unvaccinated but understand it was possible that people might have been vaccinated out of state. We assessed vaccination status as of July 31, 2022, giving a 17-month observation period.
Area Deprivation Index
The 2020 ADI is a validated tool used to measure socioeconomic disadvantage at the census-block group level (ie, neighborhood level). ADI uses 4 domains from the American Community Survey 26 : income, education, employment, and housing quality.17,18 We obtained census-block group levels from WEDSS and linked them with the corresponding ADI state decile. A decile ADI score of 1 corresponds with a neighborhood experiencing the least disadvantage, and a decile ADI score of 10 corresponds with a neighborhood experiencing high socioeconomic disadvantage. We categorized ADI deciles into 3 groups: low ADI (ADI decile 1-4), middle ADI (ADI decile 5-7), and high ADI (ADI decile 8-10).
Statistical Analysis
We described COVID-19 vaccination among 3 separate intention groups (high intention, no intention, and unsure intention). The high intention group included people who reported they would definitely get the vaccine, the no intention group included those who reported they would definitely not get the vaccine, and the unsure intention group included those who answered that they “probably will get it” or “probably will not get it.” We measured intention to get vaccinated once at the beginning of the study period during February 7-28, 2021. We used SAS version 9.4 (SAS Institute, Inc) for all analyses. The observation time for each person started at completed registration and concluded at vaccination date; those who were not vaccinated during the study period were censored at the end of the study on July 31, 2022.
Covariates for our analysis included sex (male, female, unknown), age group (18-45, 46-65, ≥66 y), and ADI group (low, middle, high). Racial and ethnic identity, the primary categorical variable of interest, included Asian, Hispanic, non-Hispanic Black, non-Hispanic White, and other or multiple races. Some racial and ethnic categories (American Indian/Alaska Native, Native Hawaiian) were too small for analysis and were combined into the other or multiple races category. We used a Cox proportional hazards model to estimate the hazard ratios for vaccination among racial and ethnic groups, adjusted for vaccination intention, sex, age group, and ADI. We calculated adjusted hazard ratios (AHRs) with 95% CIs. We tested ADI as an effect modifier of the relationship between vaccination and racial and ethnic identity and used a P value of .05 to determine significance.
The Centers for Disease Control and Prevention (CDC) Institutional Review Board reviewed this activity and determined it was public health practice and exempt. This activity was conducted consistent with applicable federal law and CDC policy (see eg, 45 CFR part 46, 21 CFR part 56; 42 USC §241[d]; 5 USC §552a; 44 USC §3501 et seq). This article was revised to comply with US Executive Order 14168. Information was collected for participant gender, not sex. For people who did not identify as male or female, sex was considered unknown.
Results
In total, 14 084 Wisconsin residents responded to the question on vaccination intention during registration for a COVID-19 test. Of those who responded to the registration questionnaire, we had complete data on race and ethnicity for 12 196 people (86.6%) (Table 1). By July 31, 2022, a total of 9031 (74.0%) respondents had ≥1 dose of COVID-19 vaccine, and 3165 (26.0%) respondents remained unvaccinated. The study population represented all but 4 of the 30 Wisconsin counties with a COVID-19 testing site, and most of the study population resided in 1 of 2 urban counties, Dane (n = 5221; 42.8%) or Milwaukee County (n = 2914; 23.9%). The study population was predominantly non-Hispanic White (80.5%; n = 9820) followed by Hispanic (7.8%; n = 951), Asian (5.2%; n = 632), non-Hispanic Black (4.6%; n = 563), and other or multiple races and ethnicities (1.9%; n = 230). Female residents represented 51.0% and male residents represented 48.0% of the study population. Sixty-nine percent of the study population was aged 16 to 45 years.
Demographic characteristics and COVID-19 vaccination intent among a cohort of adults who received COVID-19 testing a at a state-supported community testing site, Wisconsin, February 2021–July 2022
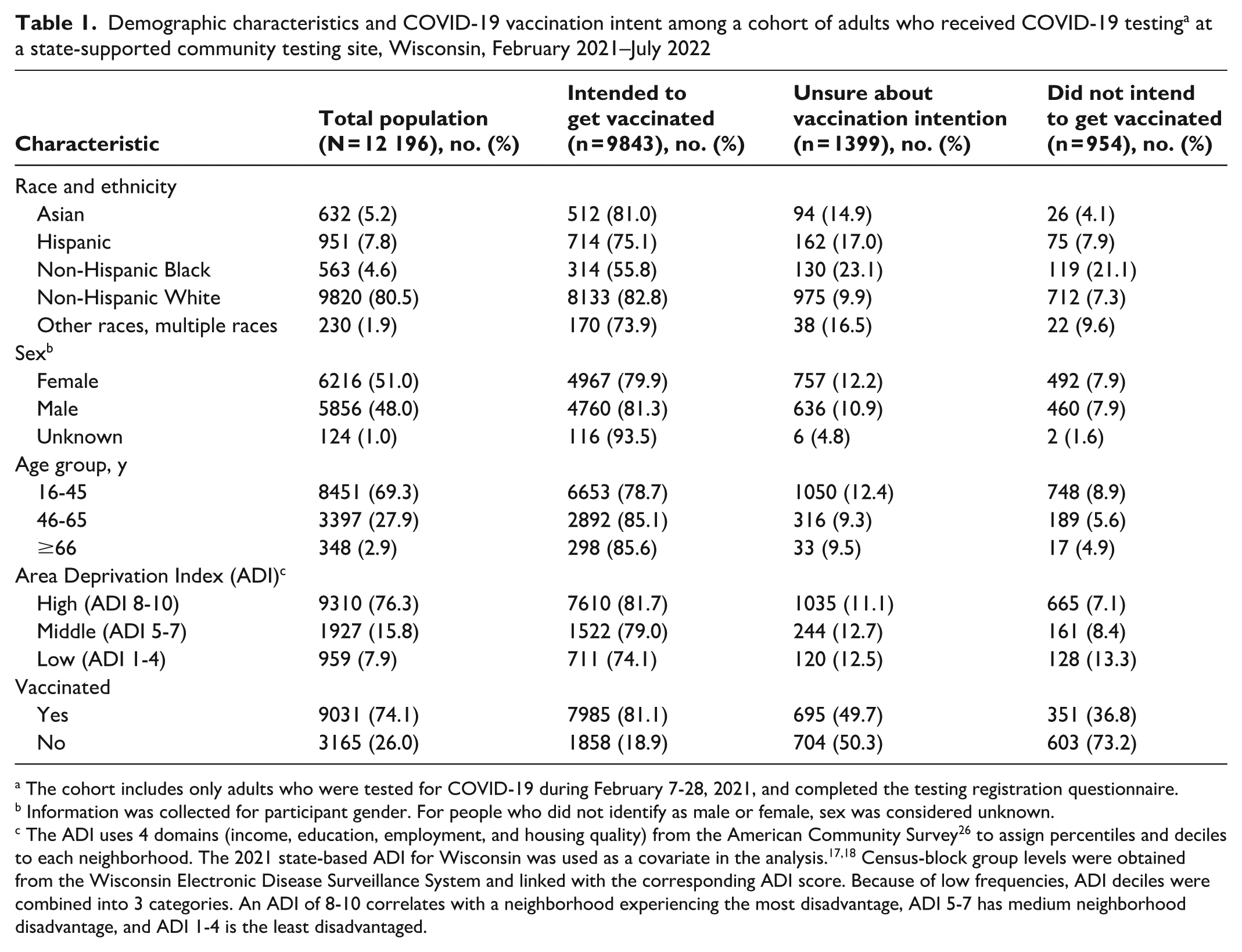
The cohort includes only adults who were tested for COVID-19 during February 7-28, 2021, and completed the testing registration questionnaire.
Information was collected for participant gender. For people who did not identify as male or female, sex was considered unknown.
The ADI uses 4 domains (income, education, employment, and housing quality) from the American Community Survey 26 to assign percentiles and deciles to each neighborhood. The 2021 state-based ADI for Wisconsin was used as a covariate in the analysis.17,18 Census-block group levels were obtained from the Wisconsin Electronic Disease Surveillance System and linked with the corresponding ADI score. Because of low frequencies, ADI deciles were combined into 3 categories. An ADI of 8-10 correlates with a neighborhood experiencing the most disadvantage, ADI 5-7 has medium neighborhood disadvantage, and ADI 1-4 is the least disadvantaged.
Most of the study population indicated they intended to get the COVID-19 vaccine when it became available (80.7%; n = 9843), 11.5% (n = 1399) were unsure, and 7.8% (n = 954) did not intend to get vaccinated (Table 1). Across racial and ethnic groups, 21.1% of non-Hispanic Black respondents, 9.6% of respondents from other or multiple races, 7.9% of Hispanic respondents, 7.3% of non-Hispanic White respondents, and 4.1% of Asian respondents did not intend to get vaccinated. By sex, male respondents had a higher intention to get vaccinated than female respondents (81.3% vs 79.9%). Vaccination intention was highest among people aged ≥66 years (85.6%), followed by people aged 46 to 65 years (85.1%) and 16 to 45 years (78.7%). A higher proportion of people living in a neighborhood with an ADI of 1 to 4 (low socioeconomic disadvantage) did not intend to get vaccinated (13.4%) compared with 7.1% of people living in neighborhoods with an ADI score of 8 to 10 (high socioeconomic disadvantage) and 8.4% of those living in the middle ADI tercile neighborhoods (ADI score 5-7).
The multivariable Cox proportional hazards model found a significant association between racial and ethnic identity and vaccination (Table 2). Effect modification between ADI and race and ethnicity was not significant (P = .13). A racial and ethnic disparity persisted in COVID-19 vaccination despite controlling for vaccination intention, age group, sex, and ADI group.
Adjusted hazard ratios for COVID-19 vaccination in a multivariable Cox proportional hazards model, Wisconsin, February 2021–July 2022
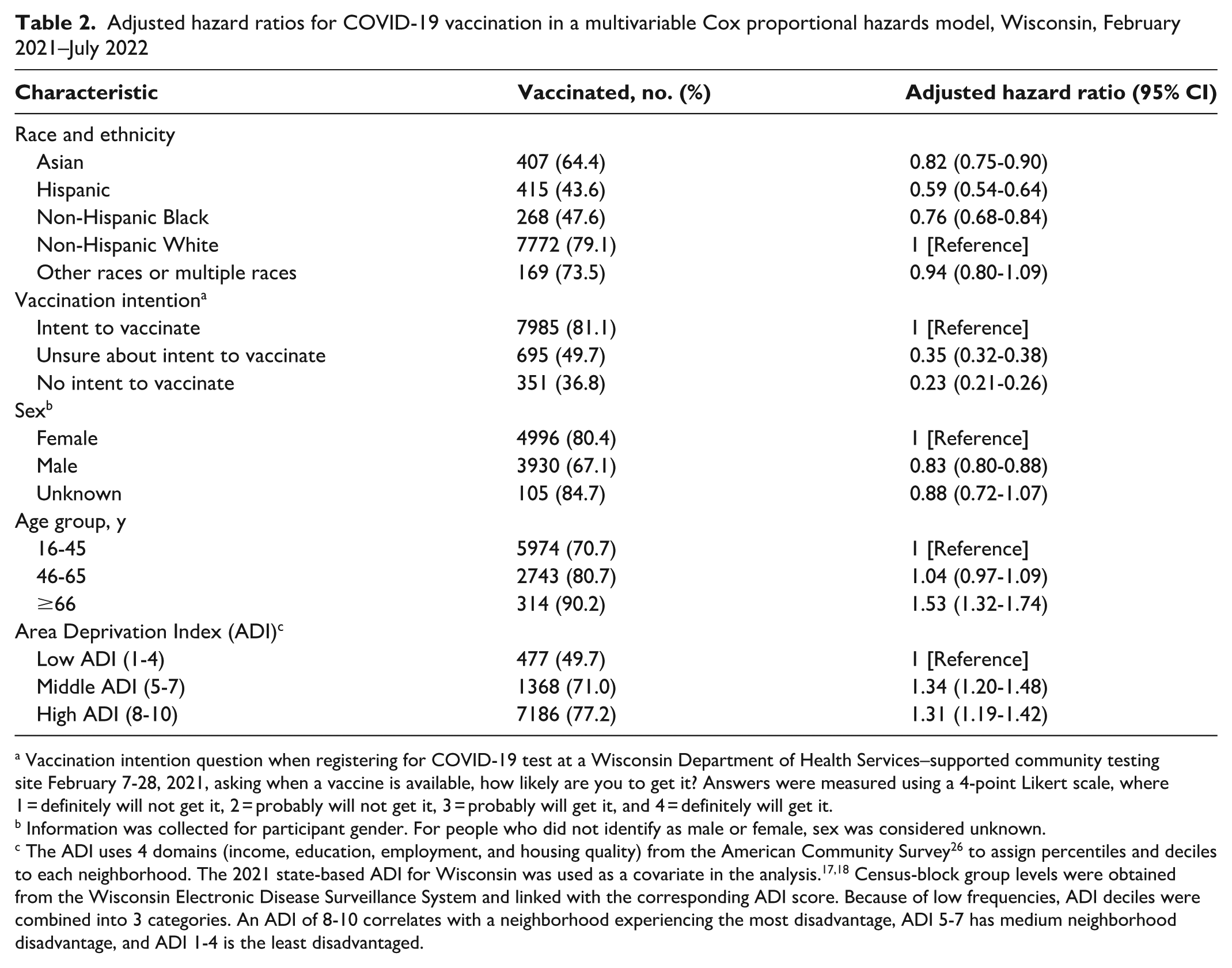
Vaccination intention question when registering for COVID-19 test at a Wisconsin Department of Health Services–supported community testing site February 7-28, 2021, asking when a vaccine is available, how likely are you to get it? Answers were measured using a 4-point Likert scale, where 1 = definitely will not get it, 2 = probably will not get it, 3 = probably will get it, and 4 = definitely will get it.
Information was collected for participant gender. For people who did not identify as male or female, sex was considered unknown.
The ADI uses 4 domains (income, education, employment, and housing quality) from the American Community Survey 26 to assign percentiles and deciles to each neighborhood. The 2021 state-based ADI for Wisconsin was used as a covariate in the analysis.17,18 Census-block group levels were obtained from the Wisconsin Electronic Disease Surveillance System and linked with the corresponding ADI score. Because of low frequencies, ADI deciles were combined into 3 categories. An ADI of 8-10 correlates with a neighborhood experiencing the most disadvantage, ADI 5-7 has medium neighborhood disadvantage, and ADI 1-4 is the least disadvantaged.
Hispanic people were 41% (AHR = 0.59; 95% CI, 0.54-0.64) less likely to get vaccinated than non-Hispanic White people were (Table 2). Non-Hispanic Black people were 24% (AHR = 0.76; 95% CI, 0.68-0.84) less likely and Asian people were 18% (AHR = 0.82; 95% CI, 0.75-0.90) less likely to be vaccinated than non-Hispanic White people.
Discussion
This large multidata source study in Wisconsin found racial and ethnic disparities in vaccination uptake despite the intention to get vaccinated. In addition, we found that a higher proportion of respondents in racial and ethnic minority groups than non-Hispanic White respondents were unsure or did not intend to get the COVID-19 vaccine. Findings from our study suggest that public health efforts could focus resources to increase acceptance of and access to the COVID-19 vaccine among racial and ethnic minority groups in the United States.
Our findings of racial and ethnic differences in vaccination intention support findings from other COVID-19 vaccination studies that highlighted the increased hesitancy among racial and ethnic minority groups in the United States.9,11,27-29 High rates of vaccine hesitancy have also been noted in American Indian or Alaska Native populations, which we were unable to assess because of low representation in the study population. 30 These findings might indicate gaps in vaccine education tailored to racial and ethnic minority groups such as Black and Hispanic people in the United States. Studies have reported that conversations with health care providers and education of patients about COVID-19 vaccine were effective in changing the minds of people who were hesitant to be vaccinated, but a lack of health care access or poor health care quality might affect the likelihood of this type of provider–patient education in some communities. 22 Another study by Nguyen et al 29 found that mistrust in science and the COVID-19 vaccine is significantly higher among Black and Hispanic people than among White people and might be a significant predictor of vaccination. Mistrust of government and health care in Black populations is rooted in a long history of abuse and mistreatment by these establishments, and these relationships have yet to be adequately repaired.31,32 Contemporary discrimination and stigma continue to sow mistrust in these institutions among racial and ethnic minority groups in the United States. 33 Concerns about COVID-19 vaccine in these populations should be addressed, and efforts to address education gaps should be culturally appropriate, taking into consideration the roots of mistrust, cultural and social sensitivities, and structural racism that has harmed and continues to harm these populations. Such programs have proven effective in overcoming vaccine hesitancy and increasing COVID-19 vaccination rates among racially diverse populations.34-36
Our study found that neighborhood-level socioeconomic disadvantage measured by ADI was not associated with worse vaccination rates among racial and ethnic minority groups. Our findings differ in that respect from other studies that have reported associations of higher COVID-19 vaccine hesitancy among people of low socioeconomic status and worse vaccination rates among some racial and ethnic minority groups, although many of those studies do not include vaccination behavior.37,38 For example, a study by Nguyen et al 11 highlighted significant associations among vaccination intention, race and ethnicity, and household income in a large US survey, but the actual receipt of COVID-19 vaccination was not assessed. We did not find an association between vaccination uptake and socioeconomic disadvantage in this sample of Wisconsin residents, which could be a result of an effective community vaccination strategy for low-income communities. 39 This strategy, which included awarding more than $8 million in grants to community-based organizations to promote outreach and serve as trusted messengers to medically underserved communities, may have led to increased vaccination rates among the lowest ADI group in the study cohort. These strategies may not have had an effect on the racial and ethnic disparities seen in vaccination behavior because ADI did not correlate with race and ethnicity (ie, the socioeconomic experiences of racial and ethnic minority groups were diverse). We originally hypothesized that vaccine hesitancy and social determinants of health (ie, socioeconomic disadvantage as measured by ADI) together would explain vaccination behavior. Our study found that even when controlling for vaccination intention, non-Hispanic Black, Hispanic, and Asian people were still less likely than non-Hispanic White people to get vaccinated, and this association could not be explained by ADI. Alternatively, it is possible the ADI did not adequately capture social determinants of health that directly related to health care experiences or access among this study cohort. Such factors would include transportation needs or access to high-speed internet or a smartphone. Access to these resources could have been distributed unequally across racial and ethnic groups and affected vaccination behavior. Although we do not know what other barriers affected vaccination behavior among those who intended to get the vaccine, an investigation of these factors would be beneficial because these factors may be more easily overcome than vaccine hesitancy.
Limitations
Our study had several limitations. First, we assessed vaccination intention in February 2021. Vaccination intention during the early dissemination of the COVID-19 vaccine might have inflated the number of those with little intention to vaccinate because of unfamiliarity with the vaccine. We recognize vaccination intention can change as the attitudes and perceptions of individual and community risk change. For this reason, we cannot be certain about the reason someone chose to receive or forgo the COVID-19 vaccine. Second, the study population might be more likely to seek and get to health care than the general population because the cohort was selected from people who were mostly from urban centers in Wisconsin who generally have more access to health care than rural residents. Also, they were people who sought a COVID-19 test, suggesting that vaccination intent and vaccination rates might be higher among this population than among the general population. Third, we were able to assess vaccination only in Wisconsin, but it is possible that people in this cohort received their vaccination in a neighboring state (Illinois, Minnesota, or Michigan). Fourth, data on race and ethnicity were unknown for approximately 13% of the study population, and we were unable to make meaningful interpretations for this group because they were excluded. In addition, because the DTRA registration questionnaire was provided in English only, the study population was limited to people who were comfortable enough to read and answer in English. Fifth, the probabilistic matching algorithm between DTRA and WIR is not definite, and some people who registered for a COVID-19 test and indicated some level of intent were unable to be linked and assessed. We believe this was a limited proportion of the overall source population (ie, <5%). Finally, findings from this study might not be generalizable to states or regions with different geopolitical and demographic compositions. Despite these limitations, our findings contribute to understanding intention as an indicator of vaccination behavior in ways previous research has not explored.
Conclusion
Understanding COVID-19 vaccination intention is important, and assessing other factors such as race and ethnicity and neighborhood socioeconomic status might play an important role when assessing vaccination behavior. We linked data from a questionnaire administered during COVID-19 test registration to a state-run immunization registry to longitudinally assess vaccination during a 17-month follow-up period. Racial and ethnic disparities in vaccination uptake persisted despite controlling for vaccination intention. Vaccination continues to be an important public health tool because of continued elevation in COVID-19–related morbidity, mortality, and hospitalizations. Vaccination strategies tailored to the needs of racial and ethnic minority groups in the United States remain crucially important.
Footnotes
Acknowledgements
For their review of previous versions of this article, the authors acknowledge the contributions of Stephanie Schauer, PhD, and Jon Meiman, MD, of the Wisconsin Department of Health Services and Kristine Bisgard, DVM, at the Centers for Disease Control and Prevention.
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.