
Abstract
Objectives:
Although federal funding for COVID-19 pandemic response measures has ended, opportunities remain to understand the needs of public health departments and the potential use of infectious disease models in the postacute pandemic response. We conducted semistructured interviews with public health representatives representing state, local, and regional/tribal public health departments in the Rocky Mountain West in summer 2022 to understand their COVID-19 priorities, decision-making needs, and data resources.
Methods:
We interviewed representatives from 6 organizations representing 3 state, local, and regional/tribal public health departments in the Rocky Mountain West.
Results:
From interviews, priorities included having timely information on vaccines, being able to anticipate COVID-19 demands on hospitals, understanding the potential effects of emerging variants, and communicating immunity concepts to the public. Decisions focused on making public health recommendations as opposed to mandates. Multiple interviewees reported limited access to timely COVID-19 data, challenges tracking COVID-19 hospitalizations, and a desire for communication tools on vaccinations and immunity.
Conclusion:
Although COVID-19 models can provide forecasts on hospital demand and project the effects of vaccines and variants in the endemic period, major gaps in data continue to challenge the public health response. Continued investments are needed in data and surveillance resources to respond to COVID-19 and to prepare for future pandemics.
Many local, state, national, and tribal public health departments partnered with academic institutions to develop COVID-19 models that informed decision-making during the COVID-19 pandemic.1-3 These partnerships brought together complementary expertise: public health departments guided the development of critical questions, and academic institutions used their expertise in infectious disease modeling to generate estimates to address priority questions. The processes that drive decision making during pandemics and how best to communicate evidence to decision makers during public health emergencies are areas of active research.4-7 Previous work in the early phase of the COVID-19 pandemic documented a range of needs among public health decision makers, including improved granularity of data and model outputs, timely information flow from research teams to decision makers, and strategies to rapidly process evolving and, at times, conflicting evidence.1,4,6 Recent outbreaks of mpox (formerly known as monkeypox) and highly pathogenic avian influenza have underscored the urgency of research on understanding the needs of public health leaders to improve decision-making during emerging infectious disease events. 8
By summer 2022, basic clinical and biological characteristics of SARS-CoV-2 were known, COVID-19 disease surveillance systems were established, and COVID-19 vaccines were widely available. Modeling efforts at the national level were used to generate scenario-based projections of variant emergence and vaccine uptake and near-term forecasts of clinical demand,9,10 and some US jurisdictions have continued to consult with academic modeling groups. However, with priorities and efforts now shifted from an intensive pandemic response to routine surveillance, this period, which has not been well-studied, has offered a unique opportunity to understand the needs of public health departments and the potential uses of infectious disease models in the postacute pandemic response. In summer 2022, we conducted semi-structured interviews with public health representatives from state, local, and regional/tribal (including nongovernment based) public health departments in the Rocky Mountain West (RMW) region, a region of rural and frontier locations connected by large cities. These interviews were designed to assess the decision-making needs of public health leaders, the types of data that they used, and any gaps in data that affected their situational awareness.
Methods
From June through August 2022, we identified a sample of public health representatives in the RMW region (Colorado, Idaho, Montana, New Mexico, Utah, and Wyoming) to interview about their current COVID-19 priorities and data and decision-making needs for the purpose of tailoring COVID-19 modeling tools to current and emerging needs. For the purpose of this study, we defined COVID-19 modeling broadly, to include both mechanistic and statistical approaches for scenario-based modeling and forecasting. We used targeted recruitment and snowball sampling. 11 We created an initial list of representatives with affiliations at state, local, and regional/tribal public health departments across the RMW region. We followed up on potential participants by email and/or telephone call. We asked both those interviewed and those unable or unwilling to participate to recommend other participants.
We conducted virtual, semistructured, 30-minute interviews from June through August 2022. If multiple people from the same organization agreed to participate, we scheduled a single interview and captured all responses with consensus not required. We developed interview questions to solicit open-ended responses on (1) the COVID-19–related priorities for each organization, (2) the types of decisions related to COVID-19 that an organization was currently making and the types of decisions that they anticipated making, (3) the concerns about imported infections and variants, and (4) the data sources that organizations used to track SARS-CoV-2. After conducting interviews, we performed a descriptive analysis of responses. We consolidated interview notes from 2 independent notetakers into a single document. We then paraphrased the responses to identify common responses for each interview question. We grouped topics that emerged among responses to multiple questions.
The Colorado Multiple Institutional Review Board (IRB) classified this project as exempt from IRB review and waived the need for consent. To protect privacy, we omitted participant names and affiliate institutions; redacted versions of interviews can be made available upon request to the corresponding author.
Results
We identified and contacted 13 public health organizations in 6 states in the RMW region. Overall, we interviewed 6 groups, representing local (n = 1), state (n = 3), and regional/tribal (n = 2) levels. Despite repeated outreach to multiple groups (30 individuals), we were unable to recruit participants from 3 states (Idaho, New Mexico, and Utah). Our organizational response rate was 46% (6 of 13). The number of participants per interview ranged from 1 to 3. The participants represented a range of positions, including state epidemiologists, surveillance program managers, COVID-19 response managers, and data analysts. The ability for decision-making also varied among participants: some held leadership roles and were directly involved in decision-making, whereas others contributed to the monitoring and interpretation of surveillance trends that informed the decision-making process.
Participants described a shift in decision-making away from mandates that characterized the early response to SARS-CoV-2 and were, instead, in “recommendation mode,” often following guidelines from the Centers for Disease Control and Prevention. Several participants noted that face mask mandates and closures were no longer options.
From interviews, we found that COVID-19–related public health priorities and decision-making centered on 3 themes: vaccination and immunity, hospital capacity and health care needs, and effects of emerging variants (Table). The most common vaccination priorities were identifying individuals in need of catch-up vaccination and understanding the present level of immunity in various regions. Hospital priorities included understanding when and if hospital capacity might be exceeded. The ability to time potential hospitalization surges that could exceed hospital capacity was seen as important to potentially help with staffing adjustments, change licensing requirements, and improve health facility preparedness. Emerging variants were identified as a challenge closely related to health care needs: one participant asked, “How bad would a variant have to be to see an increase [in hospitalizations] this fall?” Although some participants were interested in tracking when new, high-priority variants arrived in their region, few were interested in tracking travel patterns, noting “everyone is traveling.” Representatives of tribal entities highlighted concerns about the ability to continue testing for COVID-19 and new variants and concerns about transporting tribal members to facilities equipped with testing resources.
Summary of responses to COVID-19 interview questions from public health practitioners in the Rocky Mountain West region, June–August 2022
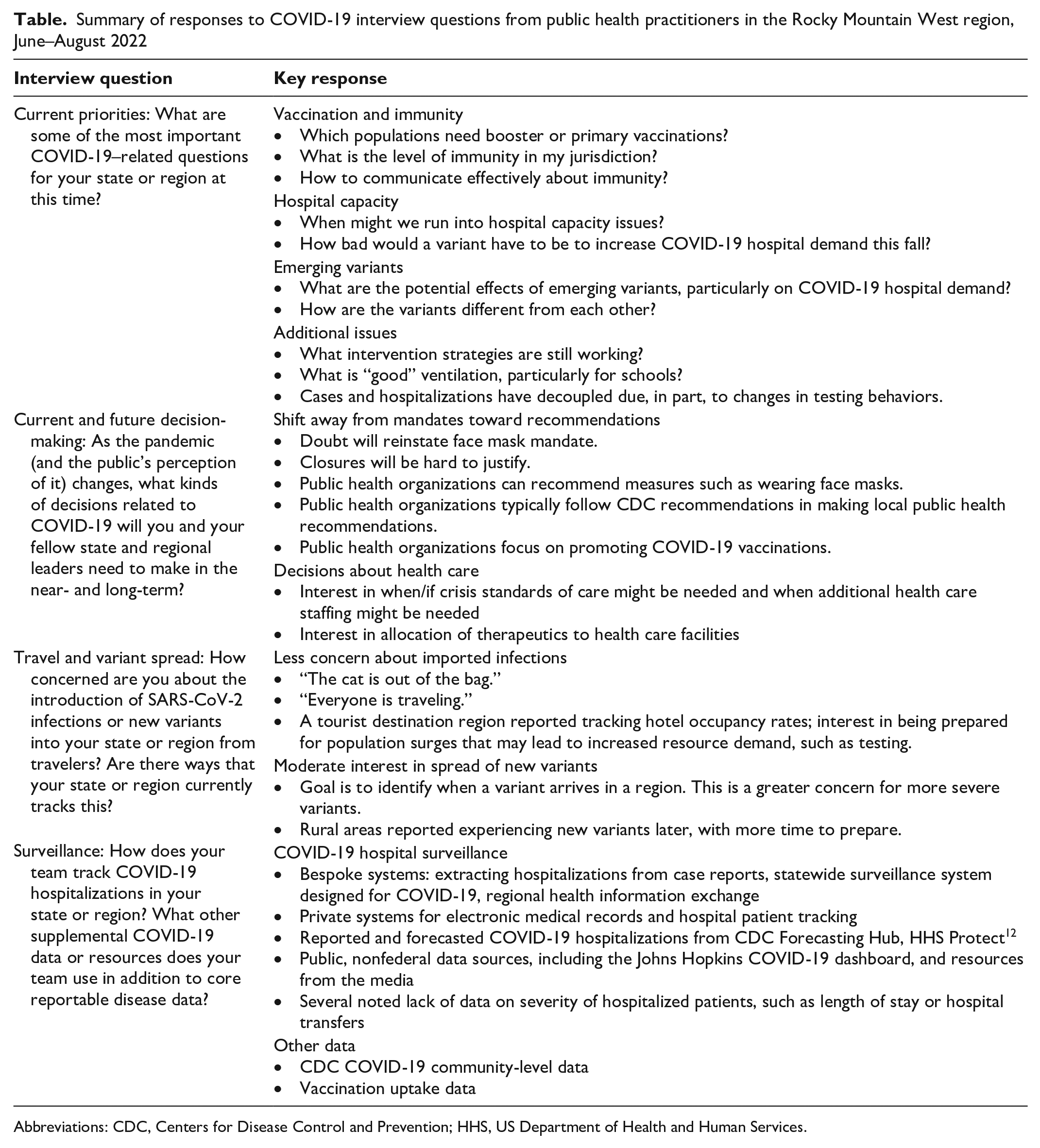
Abbreviations: CDC, Centers for Disease Control and Prevention; HHS, US Department of Health and Human Services.
Science communication emerged as a common challenge among participants (Box). Participants described challenges in communicating the health risks from new variants to the public, translating complex concepts of immunity to simple public health messaging, and addressing misinformation about COVID-19 vaccines and treatments and general public disengagement. Some participants described wanting educational materials to explain “how variants are different from each other.” Other participants described feeling ill-prepared to answer questions such as “My young child had COVID-19; why get them vaccinated?” Participants stated that communication toolkits on these topics were needed for public health leaders.
COVID-19–related challenges raised by public health representatives in the Rocky Mountain West region during interviews, June–August 2022
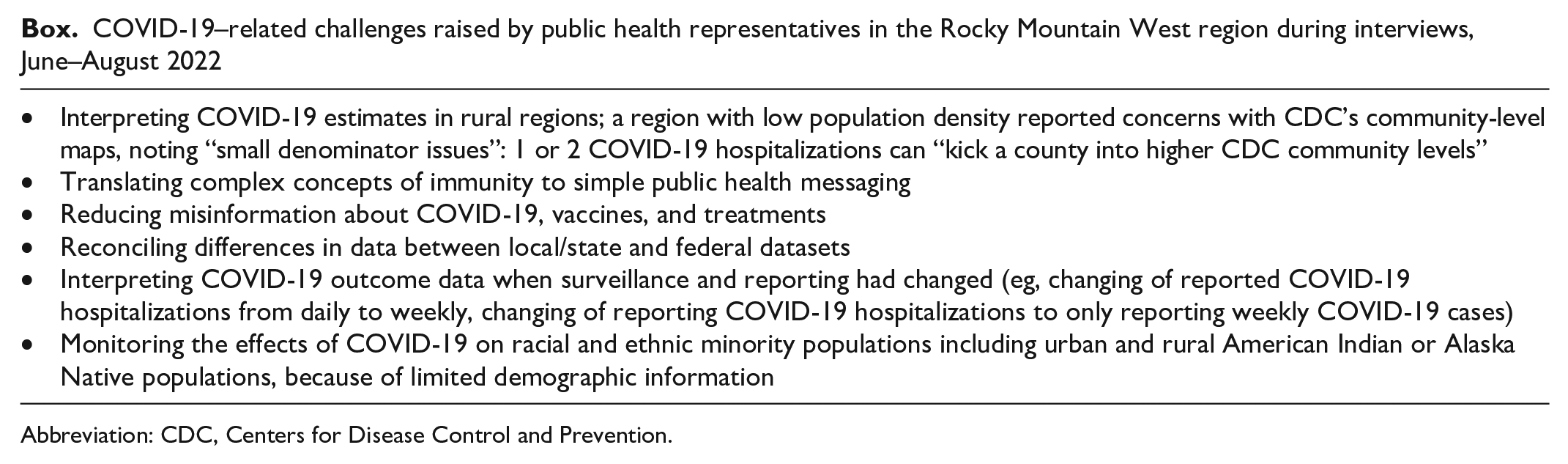
Abbreviation: CDC, Centers for Disease Control and Prevention.
Participants used a range of sources for surveillance of COVID-19 hospitalization, including bespoke state hospital reporting systems, federal data, 12 and public and private sources. Bespoke systems included hospitalization data extracted from case reports, a statewide COVID-19 hospital surveillance system created during the pandemic, and a regional health information exchange that predated the COVID-19 pandemic. Participants also described other metrics, including reported and forecasted COVID-19 hospitalizations and COVID-19 community-level maps from Centers for Disease Control and Prevention (CDC) 13 and publicly available nonfederal data sources, such as the Johns Hopkins COVID-19 dashboard. 14 A key data challenge described by participants was limited demographic information, including missing data on race and ethnicity needed to identify and monitor the effects of COVID-19 on racial and ethnic minority populations, including urban and rural American Indian or Alaska Native (AI/AN) populations. This challenge was mentioned a few times as a limitation in reporting and access for tribal participants. Some participants could not identify the county of residence for hospitalized patients and were limited in determining disease severity at fine spatial scales. Some participants noted that COVID-19 hospitalization estimates differed between state and federal data sources, and the discordance led the participants to have low trust in federal data sources. Tribal participants also mentioned that they used data sources similar to other participants to monitor hospital trends but also mentioned that they receive some hospital data annually, limiting the utility and timeliness of such data. Nearly all participants wanted more information, including mortality rates, length of hospitalization, and hospitalization rates of patients with and without COVID-19.
Discussion
Our semistructured interviews with representatives from public health organizations in the RMW region in summer 2022 identified common COVID-19–related priorities, such as increasing vaccine uptake, monitoring emerging variants, and anticipating increases in COVID-19 hospital demand but also showed that capacity to meet these priorities varied among organizations. Participants reported shifts in the scope of COVID-19–related decision-making, from public health mandates to making recommendations based on CDC guidelines, identified needs for improved scientific communication and support to reduce misinformation, and called for educational outreach on topics such as vaccination and immunity.
Our findings point to several potential uses of COVID-19 models at the point of transition from acute pandemic to endemic transmission. Participants mentioned that they continued to use CDC forecasts and modeled scenarios to track COVID-19 trends, providing evidence that these sources continue to be useful during the transition period of the pandemic, as available surveillance data shifted. Models that can estimate future COVID-19 hospital demands and models that can simulate potential effects of emerging variants on hospital capacity continue to have utility. Local forecasting of hospitalizations and timely access to leading hospitalization indicators can help public health organizations plan for future surges in hospital admissions.15-17 Simulations of various intervention scenarios, such as vaccine uptake, can show potential effects of interventions and provide results that can be used to tailor communication tools for vaccination and immunity, as has recently been shown for mpox. 18 Knowing that disease forecasts and modeling projections are of use to public health practitioners can help to delineate the application of modeling for future epidemics and pandemics. 19
Although studies on the use of infectious disease models among state, local, and regional/tribal public health departments are limited, we observed consistency with other studies. Public health leaders in Arizona expressed similar concerns about data access issues, including the timeliness of data and the limited availability of community-level data, and tribal participants echoed similar concerns about data quality, specifically highlighting the lack of information about community demographic characteristics and social determinants of health. 20 These concerns on timeliness and access to data for tribal organizations underscore the ongoing challenge that many tribal public health organizations have when evaluating the effects of COVID-19 on their community.21,22 In a North Carolina study, public health decision makers stated that modeling helped inform decisions on resources and employees during the COVID-19 pandemic, but they also expressed hesitancy to use modeling to inform decisions, as a result of concerns about underlying data precision and the desire for more locally focused models. 1
Although we had originally intended for these interviews to inform how infectious disease modeling can better aid public health departments more than 2 years into the COVID-19 pandemic, our participants consistently highlighted the need for access to timely COVID-19 hospital data, including data on racial and ethnic populations that have historically been neglected. Responses from participants underscored how challenges of interoperability, lack of timeliness, and changing reliability of data continued well into the pandemic. These gaps in surveillance can directly affect emergency preparedness and response and can delay identification of health inequities and evaluations of trends over time. The inclusion of a tribal public health department was critical to understanding the unique jurisdictional considerations for implementing public health measures on tribal lands—which can often cross multiple county and state lines—and highlighted the continued challenges of tribal public health departments to acquire adequate local- and state-level health data on AI/AN communities. Of note, we conducted these surveys approximately 9 months before the 2023 termination of the public health emergency for COVID-19, 23 which marked a shift from response-based activities and changed many surveillance mechanisms of COVID-19. 16
Limitations
Our study had several limitations. First, we had a limited sample size; our sample may not be representative of the RMW region because not all states in the region participated. One recruitment challenge was the large number of public health officials who were either out of the office or had left their position. This noted challenge also speaks to the larger issue of politicization of public health, safety risks, 24 and burnout experienced by public health officials during the COVID-19 pandemic.25,26 Despite this challenge, a strength of our study was our ability to include representatives from state, local, and regional/tribal public health departments. Second, we did not record interviews in an effort to promote candid responses and did not apply formal qualitative approaches to our analysis. Therefore, we did not transcribe responses and may have missed important findings.
Conclusions
Infectious disease modeling tools can aid in response planning and decision-making during public health emergencies, such as the COVID-19 pandemic. A number of participants in our study reported that they have continued to use CDC data and models. However, such tools are limited in their effectiveness when surveillance capacity is limited or when organizations lack access to timely data. The representatives from public health organizations we interviewed were resilient to many challenges experienced during the COVID-19 pandemic but continue to need investments in data and surveillance resources to respond to COVID-19 and prepare for future pandemics.
Footnotes
Acknowledgements
The authors thank the public health practitioners who gave their time to participate in these interviews.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by cooperative agreement no. NU38OT000297 from the Centers for Disease Control and Prevention and the Council of State and Territorial Epidemiologists.
Disclaimer
The findings in this study do not necessarily represent the views of the Centers for Disease Control and Prevention or the Council of State and Territorial Epidemiologists.