
Abstract
Objectives:
Pregnant people infected with SARS-CoV-2, the virus that causes COVID-19, are at increased risk for severe illness and death compared with nonpregnant people. However, population-based information comparing characteristics of people with and without laboratory-confirmed SARS-CoV-2 infection during pregnancy is limited. We compared the characteristics of people with and without SARS-CoV-2 infection during pregnancy in Massachusetts.
Methods:
We compared maternal demographic characteristics, pre-pregnancy conditions, and pregnancy complications of people with and without SARS-CoV-2 infection during pregnancy with completed pregnancies resulting in a live birth in Massachusetts during March 1, 2020–March 31, 2021. We tested for significant differences in the distribution of characteristics of pregnant people by SARS-CoV-2 infection status overall and stratified by race and ethnicity. We used modified Poisson regression analyses to examine the association between race and ethnicity and SARS-CoV-2 infection during pregnancy.
Results:
Of 69 960 completed pregnancies identified during the study period, 3119 (4.5%) had laboratory-confirmed SARS-CoV-2 infection during pregnancy. Risk for SARS-CoV-2 infection was higher among Hispanic (adjusted risk ratio [aRR] = 2.3; 95% CI, 2.1-2.6) and non-Hispanic Black (aRR = 1.9; 95% CI, 1.7-2.1) pregnant people compared with non-Hispanic White pregnant people.
Conclusions:
This study demonstrates the disproportionate impact of SARS-CoV-2 infection on Hispanic and non-Hispanic Black pregnant people in Massachusetts, which may widen existent inequities in maternal morbidity and mortality. Future research is needed to elucidate the structural factors leading to these inequities.
Keywords
Pregnant and recently pregnant people infected with SARS-CoV-2, the virus that causes COVID-19, are at increased risk for severe illness and death when compared with nonpregnant people.1-4 While the absolute risk for severe outcomes among pregnant and recently pregnant people is low, reported risk factors for severe COVID-19 in pregnancy include higher maternal age, high body mass index (BMI), non-White race, certain preexisting health conditions (eg, chronic hypertension, pre-pregnancy diabetes), and pregnancy complications such as gestational diabetes and preeclampsia.2,5,6 While many studies have reported on the characteristics of pregnant people with COVID-19 compared with nonpregnant people with COVID-19, few population-based studies have examined how the characteristics of pregnant people with and without COVID-19 differ. This comparison is critical to identify disparities and enrich our understanding of who is being most impacted by COVID-19 during pregnancy, especially as initial hospital-based and community-level studies suggest that racially and ethnically minoritized groups might experience higher rates of SARS-CoV-2 infection during pregnancy when compared with non-Hispanic White pregnant people.7-9 We compared the characteristics of pregnant people with and without laboratory-confirmed SARS-CoV-2 infection in Massachusetts.
Methods
To identify pregnant people in Massachusetts with laboratory-confirmed SARS-CoV-2 infection during pregnancy and with completed pregnancies resulting in live births, we linked data on people identified as females of reproductive age (defined as aged 11-59 years) with SARS-CoV-2 infection confirmed by positive molecular testing results obtained from infectious disease case reports 10 with data from provisional birth certificates (unpublished data, Massachusetts Department of Public Health, Registry of Vital Records and Statistics) from March 1, 2020, through March 31, 2021. This activity received a determination of not research by the Massachusetts Department of Public Health Institutional Review Board.
We performed deterministic data linkages between birth certificates and infectious disease case reports using various combinations of first, last, and maiden name; date of birth; and address; linkages were made using exact matches on date of birth, street address, and zip code, as well as the first 3 letters, SOUNDEX, and SPELLDEX 11 functions applied to first, last, and maiden names. Among people with laboratory-confirmed SARS-CoV-2 infection who linked to a provisional birth certificate, we excluded people whose SARS-CoV-2 test date occurred outside their pregnancy window. For people with data available on the date of their last menstrual period (LMP), we considered the pregnancy window as the time between LMP and their date of delivery. For pregnant people missing information on LMP, we first looked to see whether data on gestational age at delivery were available; if the duration (in weeks) between receiving a positive test result for SARS-CoV-2 and date of delivery was within 1 week of the gestational age at delivery (in weeks), then we considered the SARS-CoV-2 test to occur during the pregnancy window. For those missing data on both LMP and gestational age, we operationalized the pregnancy window as the 300-day period before their delivery date. People with provisional birth certificates that did not link to laboratory-confirmed SARS-CoV-2 case reports during the same calendar time or that linked but the SARS-CoV-2 positive test result was outside the pregnancy window were considered our comparison group (ie, pregnant people without laboratory-confirmed SARS-CoV-2). We obtained data on demographic characteristics, comorbidities, prenatal care adequacy (as determined by the adequacy of prenatal care utilization [Kotelchuck] index 12 ), and pregnancy complications from birth certificates for people with and without SARS-CoV-2 infection during pregnancy. We performed Pearson χ2 tests to determine significant differences in distributions of characteristics of pregnant people by infection status overall and stratified by race and ethnicity. We considered P < .05 to be significant.
We used modified Poisson regression to calculate crude risk ratios (RRs) and adjusted risk ratios (aRRs) and 95% CIs for SARS-CoV-2 infection for various racial and ethnic groups, with non-Hispanic White as the referent group. We top-coded Hispanic ethnicity over other race variables, and we determined non-Hispanic ethnicity for those with other non-Hispanic ethnicities and those missing ethnicity information. We excluded people with unknown or missing data before conducting Pearson χ2 tests and modified Poisson regression. We adjusted for all potential covariates (ie, age, education level, preferred spoken language, health insurance type at delivery, nativity status, pre-pregnancy BMI, pre-pregnancy and gestational diabetes, pre-pregnancy and gestational hypertension, receipt of prenatal care, and adequacy of prenatal care) in our fully adjusted model. In our parsimonious model, we used backward deletion to identify confounders that changed our estimates >10% (nativity status and health insurance type). We conducted all data linkages and analyses using SAS version 9.4 (SAS Institute, Inc).
Results
We identified 69 960 completed pregnancies resulting in a live birth during the study period, of which 3119 (4.5%) had laboratory-confirmed SARS-CoV-2 infection during pregnancy. We found significant differences by SARS-CoV-2 infection status for race and ethnicity, age, education level, preferred spoken language, health insurance at delivery, nativity, pre-pregnancy BMI, pre-pregnancy diabetes, gestational hypertension, and prenatal care adequacy. Compared with pregnant people without infection, a higher proportion of pregnant people with SARS-CoV-2 infection were Hispanic or non-Hispanic Black, Spanish speaking, non–US-born, or aged <30 years (Table 1). A higher proportion of people with infection (vs no infection) during pregnancy had <high school education, public health insurance, or inadequate prenatal care. We found no significant differences by infection status for many of the comorbidities or pregnancy complications examined; however, when compared with pregnant people without infection, a higher proportion of people infected with SARS-CoV-2 during pregnancy had pre-pregnancy diabetes, gestational hypertension, and BMI ≥30 kg/m2.
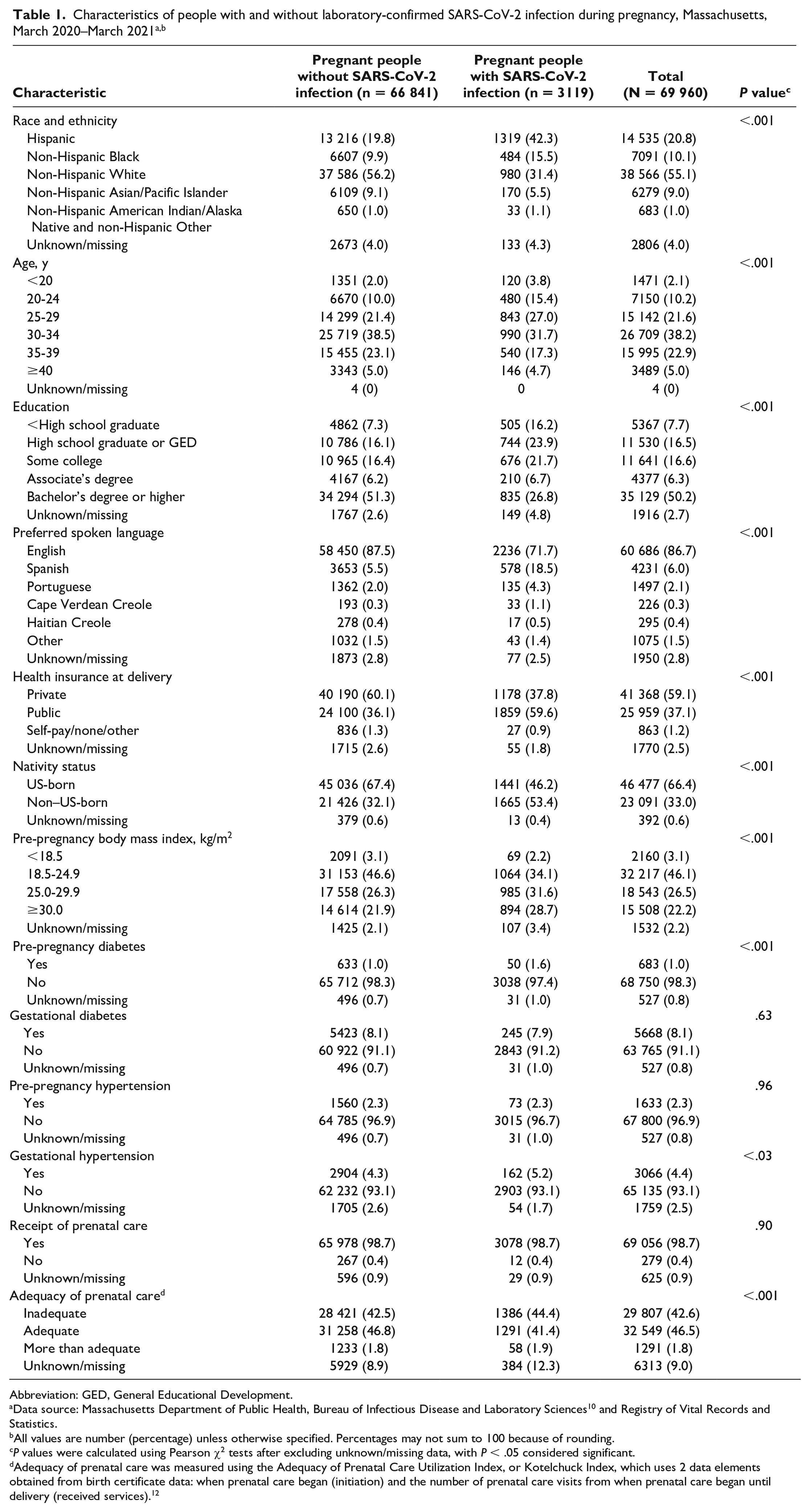
Abbreviation: GED, General Educational Development.
Data source: Massachusetts Department of Public Health, Bureau of Infectious Disease and Laboratory Sciences 10 and Registry of Vital Records and Statistics.
All values are number (percentage) unless otherwise specified. Percentages may not sum to 100 because of rounding.
P values were calculated using Pearson χ2 tests after excluding unknown/missing data, with P < .05 considered significant.
Adequacy of prenatal care was measured using the Adequacy of Prenatal Care Utilization Index, or Kotelchuck Index, which uses 2 data elements obtained from birth certificate data: when prenatal care began (initiation) and the number of prenatal care visits from when prenatal care began until delivery (received services). 12
When stratified by race and ethnicity (Table 2), data were available for 96.0% of our sample (n = 67 154). We observed significant differences in characteristics associated with infection status by race and ethnicity. Compared with people without infection belonging to the same racial and ethnic groups, a higher proportion of pregnant people with SARS-CoV-2 infection had fewer years of education, spoke a preferred language other than English, were non–US-born, and had a pre-pregnancy BMI ≥30 kg/m2. We observed additional differences by SARS-CoV-2 infection status within racial and ethnic groups. Higher proportions of people with infection had public health insurance among Hispanic (81.8% vs 73.0%), non-Hispanic White (31.6% vs 21.7%), and non-Hispanic Asian/Pacific Islander (38.8% vs 23.0%) pregnant people, but this difference was not significant among non-Hispanic Black and non-Hispanic American Indian/Alaska Native and non-Hispanic Other pregnant people. In addition, among non-Hispanic White pregnant people only, higher proportions of people with SARS-CoV-2 infection were aged <30 years (35.1% vs 25.9%) and had pre-pregnancy diabetes (1.8% vs 0.8%). Finally, among Hispanic pregnant people, a significantly lower proportion of pregnant people with SARS-CoV-2 infection had adequate or more than adequate prenatal care (38.1% vs 44.8%) compared with pregnant people without infection in the same racial and ethnic group.
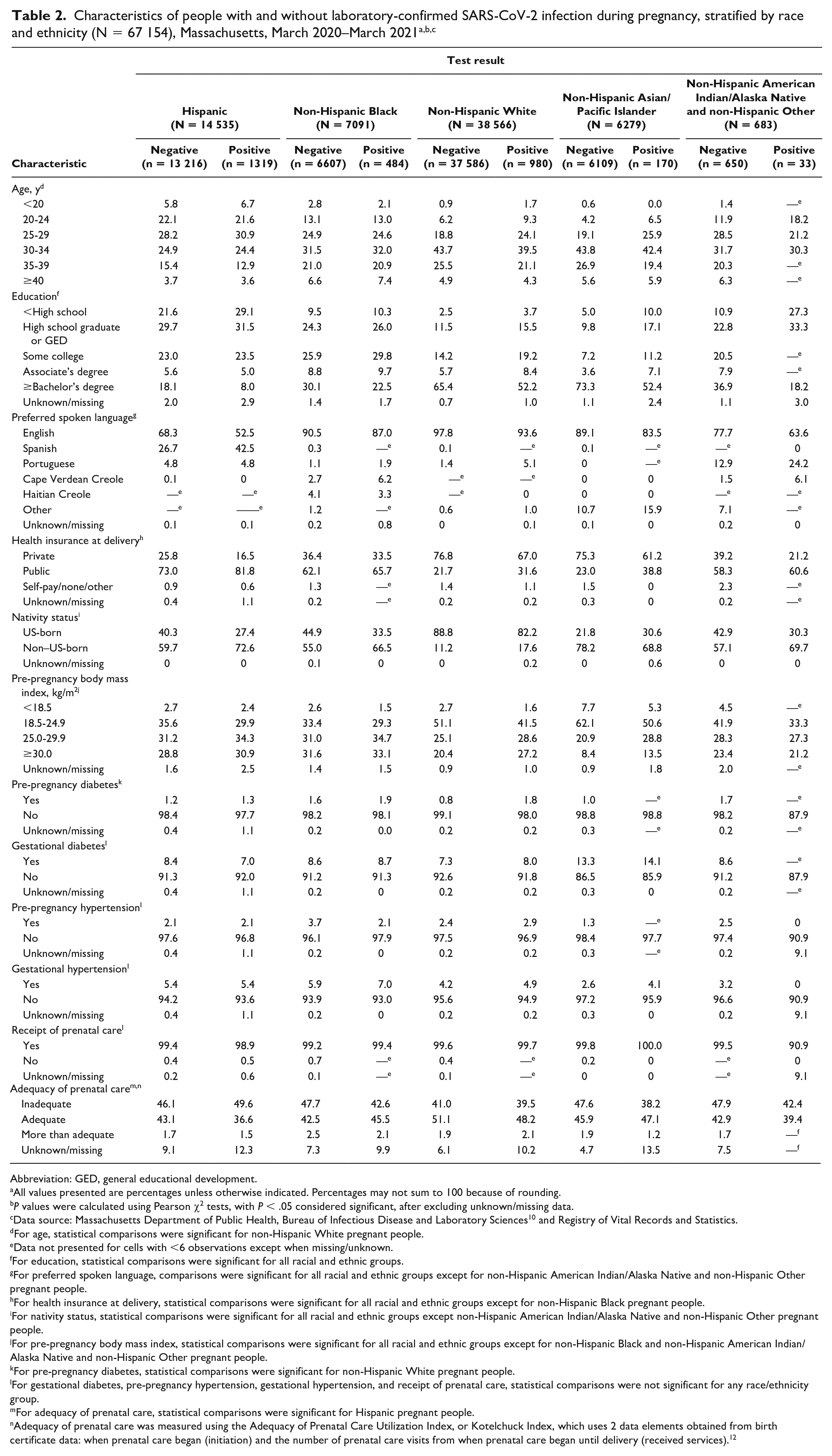
Abbreviation: GED, general educational development.
All values presented are percentages unless otherwise indicated. Percentages may not sum to 100 because of rounding.
P values were calculated using Pearson χ2 tests, with P < .05 considered significant, after excluding unknown/missing data.
Data source: Massachusetts Department of Public Health, Bureau of Infectious Disease and Laboratory Sciences 10 and Registry of Vital Records and Statistics.
For age, statistical comparisons were significant for non-Hispanic White pregnant people.
Data not presented for cells with <6 observations except when missing/unknown.
For education, statistical comparisons were significant for all racial and ethnic groups.
For preferred spoken language, comparisons were significant for all racial and ethnic groups except for non-Hispanic American Indian/Alaska Native and non-Hispanic Other pregnant people.
For health insurance at delivery, statistical comparisons were significant for all racial and ethnic groups except for non-Hispanic Black pregnant people.
For nativity status, statistical comparisons were significant for all racial and ethnic groups except non-Hispanic American Indian/Alaska Native and non-Hispanic Other pregnant people.
For pre-pregnancy body mass index, statistical comparisons were significant for all racial and ethnic groups except for non-Hispanic Black and non-Hispanic American Indian/Alaska Native and non-Hispanic Other pregnant people.
For pre-pregnancy diabetes, statistical comparisons were significant for non-Hispanic White pregnant people.
For gestational diabetes, pre-pregnancy hypertension, gestational hypertension, and receipt of prenatal care, statistical comparisons were not significant for any race/ethnicity group.
For adequacy of prenatal care, statistical comparisons were significant for Hispanic pregnant people.
Adequacy of prenatal care was measured using the Adequacy of Prenatal Care Utilization Index, or Kotelchuck Index, which uses 2 data elements obtained from birth certificate data: when prenatal care began (initiation) and the number of prenatal care visits from when prenatal care began until delivery (received services). 12
In the crude Poisson regression model, Hispanic (RR = 3.6; 95% CI, 3.3-3.9), non-Hispanic Black (RR = 2.7; 95% CI, 2.4-3.0), and non-Hispanic American Indian/Alaska Native and non-Hispanic Other (RR = 1.9; 95% CI, 1.4-2.7) pregnant people were at higher risk for SARS-CoV-2 infection during pregnancy compared with non-Hispanic White pregnant people (Table 3). In the parsimonious adjusted model, the risk of SARS-CoV-2 infection among Hispanic (aRR = 2.3; 95% CI, 2.1-2.6) and non-Hispanic Black (aRR = 1.9; 95% CI, 1.7-2.1) pregnant people was higher than the risk among non-Hispanic White pregnant people. Estimates were similar to RRs obtained from the fully adjusted model, although 95% CIs were wider.
Crude and adjusted risk ratios for laboratory-confirmed SARS-CoV-2 infection during pregnancy, by race and ethnicity, Massachusetts, March 2020–March 2021 a
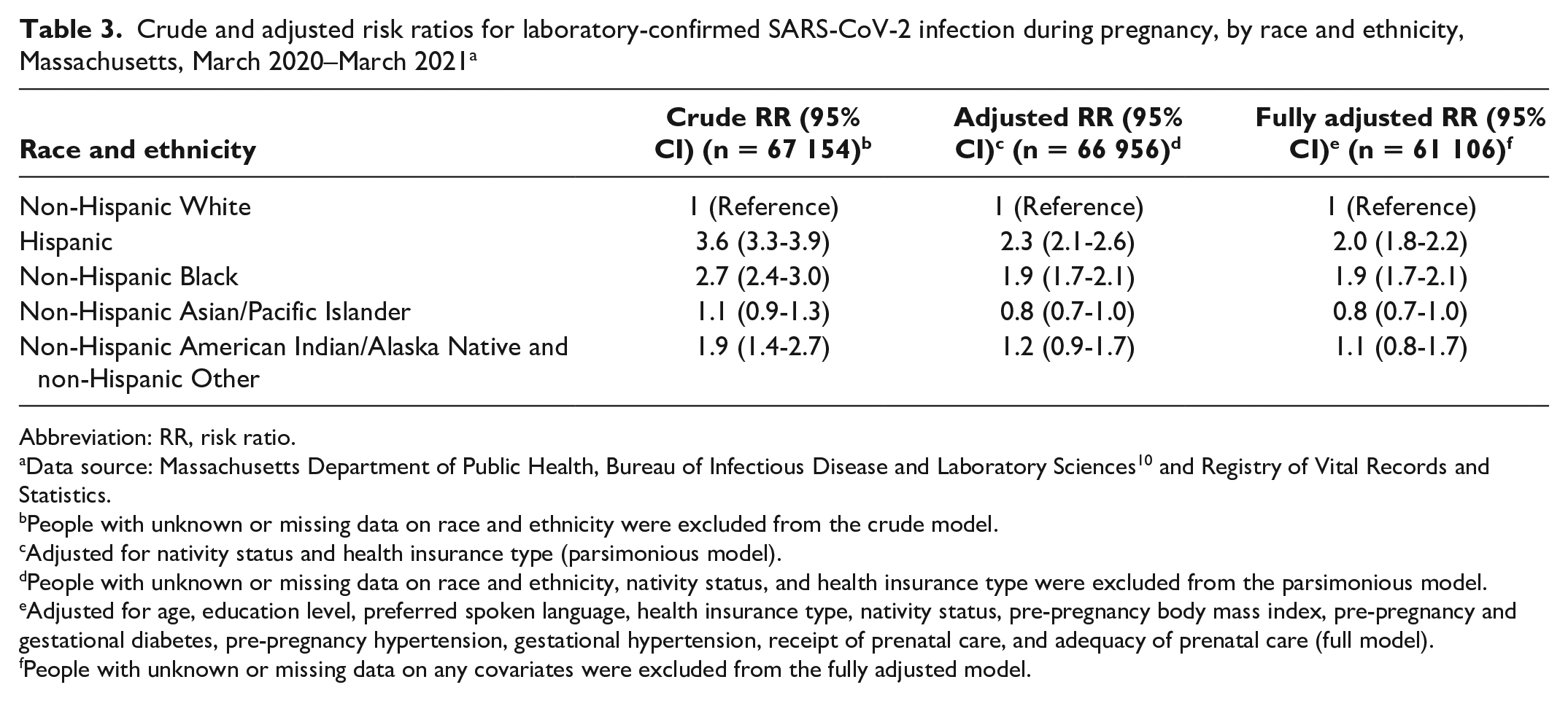
Abbreviation: RR, risk ratio.
Data source: Massachusetts Department of Public Health, Bureau of Infectious Disease and Laboratory Sciences 10 and Registry of Vital Records and Statistics.
People with unknown or missing data on race and ethnicity were excluded from the crude model.
Adjusted for nativity status and health insurance type (parsimonious model).
People with unknown or missing data on race and ethnicity, nativity status, and health insurance type were excluded from the parsimonious model.
Adjusted for age, education level, preferred spoken language, health insurance type, nativity status, pre-pregnancy body mass index, pre-pregnancy and gestational diabetes, pre-pregnancy hypertension, gestational hypertension, receipt of prenatal care, and adequacy of prenatal care (full model).
People with unknown or missing data on any covariates were excluded from the fully adjusted model.
Discussion
Given the more severe health implications of COVID-19 for pregnant and recently pregnant people than for nonpregnant people, it is important to understand the characteristics associated with the greatest incidence of infection among pregnant people. We sought to identify and describe any inequities among pregnant people by SARS-CoV-2 infection status by comparing pregnant people with and without SARS-CoV-2 infection in a statewide population in Massachusetts. We identified a disproportionate impact of COVID-19 on Hispanic and non-Hispanic Black pregnant people in Massachusetts.
We also observed differences in sociodemographic characteristics by SARS-CoV-2 infection status. Pregnant people who had fewer years of education, preferred speaking a language other than English, were non–US-born, had public health insurance, and had underlying health conditions were also disproportionately impacted by COVID-19. The intersection between these social determinants of health and systemic racism may further worsen maternal and child health inequities. 13 By conducting multivariable analyses, we estimated the independent association between race and ethnicity and SARS-CoV-2 infection among pregnant people. While this association was attenuated by nativity status, preferred spoken language, and health insurance type, Hispanic and non-Hispanic Black pregnant people had an elevated risk of SARS-CoV-2 infection even after adjusting for these factors. Because race is a social construct that does not biologically predispose certain groups to SARS-CoV-2 infection, we understand race and ethnicity in our analysis is a proxy for other social, environmental, and structural factors, especially systemic racism, that we could not measure with the data available in this analysis that are driving the observed association between race and ethnicity and COVID-19. 14
Limitations
This analysis had several limitations. First, to identify pregnant people with COVID-19, we relied on linkages of laboratory-confirmed SARS-CoV-2 case data to provisional birth certificates for completed pregnancies resulting in a live birth; therefore, we were unable to identify people with infections who experienced early pregnancy losses, terminations, or non–live births; people who might have had SARS-CoV-2 infection during pregnancy but were not tested; and people who were tested outside their pregnancy window. Moreover, although universal screening for SARS-CoV-2 was implemented before admission for labor and delivery in Massachusetts early in the pandemic, detection bias may have been introduced for people who were infected early in their pregnancy window, because those who had mild symptoms or were asymptomatic might not have sought testing. Second, we were unable to ascertain probable cases of COVID-19 during pregnancy, or pregnant people without laboratory confirmation of SARS-CoV-2 infection but with other epidemiological, clinical, or laboratory criteria 15 that may result in underreporting of SARS-CoV-2 infection among pregnant people, especially with increasing availability of at-home rapid antigen testing for which a reporting mechanism is often lacking. Third, while we aimed to capture as many linkages as possible between laboratory-confirmed SARS-CoV-2 case data and data from provisional birth certificates by developing a robust linkage algorithm using several combinations of matching variables and functions allowing for inexact matches, the linkage process might not have accurately captured the entire population of those with SARS-CoV-2 infection during pregnancy. Fourth, data from provisional birth certificates have more missing data than finalized records; however, all the variables we included had fewer than 12% of missing or unknown values. Finally, we were not able to explore several structural factors contributing to the observed racial and ethnic inequities, such as discrimination, health care access, occupation, income and wealth inequality, and housing, which drive differential risk of COVID-19 in communities of color. 16 These factors should be further investigated, explicitly defined, and addressed in COVID-19 prevention and mitigation strategies that promote health equity across race and ethnicity and address the social determinants of health for pregnant people.
Conclusion
This population-based study demonstrates the disproportionate impact of COVID-19 on Hispanic and non-Hispanic Black pregnant people in Massachusetts. The inequities we observed among pregnant people are consistent with the racial and ethnic disparities observed for COVID-19 in the general population.17,18 The unequal impact of COVID-19 on racially and ethnically minoritized groups during pregnancy deserves urgent public health attention; even before the COVID-19 pandemic, non-Hispanic Black mothers in the United States were 3 times more likely than non-Hispanic White mothers to die of pregnancy-related causes. 19 The COVID-19 pandemic may further exacerbate these inequities in maternal morbidity and mortality. 20
Footnotes
Acknowledgements
The authors thank the following for their contributions to COVID-19 Pregnancy Surveillance in Massachusetts: Anne Marie Darling, PhD, MPH (Massachusetts Department of Public Health); the COVID-19 Pregnancy Surveillance Medical Record Abstractor Team: Penny Connolly, RN; Jeanne Day, MPH; Sabrina Eagan, MSN, MPH; Nancy Reinhalter, RN; and Herman Willems (John Snow Institute, Inc.); and Kerry Fenton, RN (Massachusetts Department of Public Health).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Centers for Disease Control and Prevention (CDC) cooperative agreement “Building and Enhancing Epidemiology, Laboratory and Health Information Systems Capacity in Massachusetts” grant (NU50CK000518) and by an appointment to the Applied Epidemiology Fellowship Program administered by the Council of State and Territorial Epidemiologists and funded by CDC cooperative agreement number 1NU38OT000297-03-00.