
Abstract
Objectives:
The health status of Middle Eastern or North African (MENA) populations in Western countries is poorly understood. We assessed whether MENA infants and mothers have a greater risk of adverse pregnancy and birth outcomes than non-MENA infants and mothers in Quebec, Canada.
Methods:
We conducted a population-based observational study of 809 172 infants born to pregnant women in Quebec from 2008 through 2020. We identified infants in the MENA group based on self-reported mother tongue (Arabic or Turkish) and parents’ country of birth (North African or Middle Eastern country). We compared infant and maternal outcomes, including gestational diabetes, cesarean delivery, preterm birth, severe maternal or neonatal morbidity, and other pregnancy and birth complications between the MENA and non-MENA groups. Using log-binomial regression models, we calculated risk ratios (RRs) and 95% CIs to measure the risk of adverse pregnancy and birth outcomes for the MENA group compared with the non-MENA group, adjusting for maternal age, comorbidity, and other patient characteristics.
Results:
Compared with the non-MENA group (n = 716 387), the MENA group (n = 92 785) had an elevated risk of gestational diabetes (RR = 1.51; 95% CI, 1.48-1.55), postterm birth (RR = 1.24; 95% CI, 1.08-1.42), and short-stay neonatal intensive care unit admission (RR = 1.91; 95% CI, 1.82-1.99). However, MENA infants were 15% to 50% less likely than non-MENA infants to be born preterm, have severe neonatal morbidity, and have a mother with preeclampsia or severe maternal morbidity.
Conclusions:
Although findings among MENA infants and mothers in Quebec were reassuring overall, MENA infants and mothers may benefit from closer perinatal follow-up to improve complications of gestational diabetes.
Keywords
Race and ethnicity are social determinants of maternal and infant health,1,2 but little is known about the outcomes of Middle Eastern or North African (MENA) populations. An increasing number of MENA people have been migrating to Western countries, composing as much as 2% of the population in countries such as Canada. 3 MENA people may experience discrimination or have lifestyle characteristics that influence health outcomes during pregnancy.4,5 MENA people have elevated rates of type 2 diabetes and hyperlipidemia and tend to have low uptake of vaccination for preventable infections,4,5 all factors that may affect pregnancy. Language barriers and cultural beliefs or misconceptions about the causes of disease may affect quality or access to antenatal and perinatal care. 6 However, literature on maternal and infant outcomes in the MENA population is scant.
Reports have suggested that MENA women may be at risk of certain adverse obstetric outcomes.7-9 In a study of 207 458 US births, MENA mothers had 31% greater odds of gestational diabetes and 16% greater odds of low birth weight than non-Hispanic White mothers. 7 In a study of 165 000 singleton births in Finland, MENA mothers had 1.7 times higher rates of low birth weight and preterm birth than the general population. 8 In an analysis of 3 million births from Canada, MENA women had 1.2 times greater risk of stillbirth than other women in Canada. 9 However, at least 5 studies have suggested that MENA women tend to have low rates of preeclampsia, preterm birth, and infant mortality.10-14 These opposing patterns make it unclear whether MENA women have increased susceptibility to adverse pregnancy and birth outcomes. In this study, we compared risks of a range of adverse maternal and infant outcomes among MENA infants and mothers versus non-MENA infants and mothers in a large Canadian province.
Methods
Study Design and Population
We conducted a population-based observational study of 809 172 infants born in Quebec, Canada, from January 1, 2008, through December 31, 2020, the period when data were available. We extracted data on all births from Quebec’s registry of demographic events and obtained pregnancy and birth data from the Maintenance and Use of Data for the Study of Hospital Clientele registry.15,16 All hospitals in Quebec contribute data to these registries. The registries contain self-reported parental information on country of birth, mother tongue, and socioeconomic status, as well as characteristics such as gestational age, birth weight, intensive care unit (ICU) admission, clinical diagnoses, and procedures in infants and mothers. Because we used anonymized data, the University of Montreal Hospital Centre Review Board exempted our study from ethical review.
We divided the study group into an exposure group (MENA infants) and a comparison group (non-MENA infants), who represented the general population. After Black people, MENA people are the second largest racial and ethnic minority group in Quebec, accounting for 40% of the MENA population in Canada.3,17 Most MENA people in Quebec originate from Algeria, Morocco, Lebanon, and Syria, with 20% of all immigrants from 2016 through 2021 coming from one of these countries. 17
Exposure and Comparison Groups
We identified MENA infants on the basis of the mother tongue and country of birth of the parents. We included infants in the MENA group if at least 1 parent reported Arabic or Turkish as their mother tongue or had a North African or Middle Eastern country of birth, including Algeria, Bahrain, Egypt, Iran, Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Palestine, Qatar, Saudi Arabia, Syria, Tunisia, Turkey, United Arab Emirates, Western Sahara, or Yemen. We further accounted for the number of MENA parents (MENA mother only, MENA father only, 2 MENA parents). The comparison group included infants whose parents both reported French or English as their mother tongue and Canada as their country of birth.
Outcomes
We analyzed infant and maternal outcomes. In infants, we considered preterm birth (<37 wk gestation), postterm birth (≥42 wk gestation), low birth weight (<2500 g), high birth weight (≥4000 g), birth defects (chromosomal, nonchromosomal), birth trauma, neonatal sepsis, neonatal jaundice, hypoglycemia or hyperglycemia, severe neonatal morbidity (respiratory distress syndrome, bronchopulmonary dysplasia, intraventricular hemorrhage, necrotizing enterocolitis, periventricular leukomalacia, and retinopathy of prematurity), ICU admission (1, 2 or 3, 4-13, or ≥14 d), fetal death, and neonatal death.
For maternal outcomes, we included gestational diabetes, preeclampsia, placental abruption, placenta previa, postpartum hemorrhage, chorioamnionitis, cesarean delivery, and severe maternal morbidity (eclampsia, heart failure, myocardial infarction, cerebrovascular accidents, acute renal failure, shock, and other life-threatening morbidity). 18
We identified adverse infant and maternal outcomes using diagnostic codes from the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Canada and procedure codes from the Canadian Classification of Health Interventions, and from gestational age, birth weight, ICU admission, and death record fields (eTable 1 in the Supplement).19,20
Covariates
We accounted for maternal age; parity (0, 1, ≥2 previous deliveries); maternal comorbidity, including preexisting hypertension, diabetes mellitus type 1 or 2, obesity, dyslipidemia, and alcohol, tobacco, or other substance use disorders (yes, no, unknown); infant sex (male, female); multiple births (yes, no); self-reported maternal education (high school, vocational training, university, unknown); and birth year. We expressed age and birth year as continuous variables in splines. 21 We also accounted for socioeconomic disadvantage (yes, no, unknown), measured as the most materially deprived quintile of the population based on a composite neighborhood-level indicator of education, income, and unemployment derived from census data linked to postal codes. 13
Data Analysis
We calculated outcome rates per 1000 infants for the MENA and non-MENA groups and estimated risk ratios (RRs) and 95% CIs for the risk of adverse pregnancy and birth outcomes in the MENA group compared with the non-MENA group by using log-binomial regression models. We adjusted the models for maternal age, parity, maternal comorbidity, infant sex, multiple births, maternal education, socioeconomic disadvantage, and birth year. We accounted for patients with missing data on maternal comorbidity (34 382 of 809 172; 4.2%), maternal education (31 102 of 809 172; 3.8%), and socioeconomic disadvantage (23 837 of 809 172; 2.9%) in separate categories. We used generalized estimating equations with an exchangeable correlation structure to account for siblings in the same family.
In secondary analyses, we examined whether MENA infants and mothers had a greater risk of adverse outcomes than non-MENA infants and mothers among subgroups of the population having biological risk factors considered to contribute to increased risk of poor maternal outcomes (aged <25 y, presence of comorbidity, multiple pregnancy, high school education, and socioeconomic disadvantage). We also determined whether risks were greater when both parents were MENA as opposed to when only 1 parent was MENA. In sensitivity analyses, we excluded births that occurred during the COVID-19 pandemic. We used SAS version 9.4 (SAS Institute Inc) for statistical analyses.
Results
In our cohort of 809 172 infants, 92 785 (11.5%) were born to MENA parents (Table 1). Among MENA infants, 73 062 (78.7%) had 2 MENA parents, 6545 (7.1%) had a MENA mother only, and 13 178 (14.2%) had a MENA father only. Compared with non-MENA infants (n = 716 387), MENA infants were more likely to have a mother aged ≥35 years (32.3% vs 14.1%), with ≥2 previous deliveries (27.2% vs 18.5%), with university education (57.9% vs 36.2%), and with socioeconomic disadvantage (30.9% vs 17.2%).
Characteristics of MENA and non-MENA infants and mothers, Quebec, Canada, 2008-2020 a

Abbreviation: MENA, Middle Eastern or North African.
The MENA group included infants whose parents self-reported Arabic or Turkish mother tongue or were born in a North African or Middle Eastern country. The non-MENA group included infants whose parents had French or English mother tongue and were born in Canada. Data sources: Ministry of Health and Social Services.15,16
Preexisting hypertension, diabetes mellitus type 1 or 2, obesity, dyslipidemia, and alcohol, tobacco, or other substance use disorders.
Missing data not shown; percentages do not add to 100.
Most materially deprived quintile of the population based on neighborhood education, income, and unemployment.
Compared with non-MENA infants, MENA infants had 1.24 times the risk of postterm birth (95% CI, 1.08-1.42), 1.09 times the risk of high birth weight (95% CI, 1.06-1.11), and 1.50 times the risk of chromosomal anomalies (95% CI, 1.23-1.82) (Table 2). MENA infants were 2 times more likely than non-MENA infants to have a short stay in a neonatal intensive care unit (NICU) of 1 day (RR = 1.91; 95% CI, 1.82-1.99) or 2 or 3 days (RR = 1.84; 95% CI, 1.71-1.98). In contrast, MENA infants were 20% to 30% less likely than non-MENA infants to be born preterm or have low birth weight, birth trauma, sepsis, jaundice, or severe neonatal morbidity.
Risk of adverse birth outcomes in MENA and non-MENA infants, Quebec, Canada, 2008-2020 a

Abbreviation: MENA, Middle Eastern or North African.
The MENA group included infants whose parents self-reported Arabic or Turkish mother tongue or were born in a North African or Middle Eastern country. The non-MENA group included infants whose parents had French or English mother tongue and were born in Canada. Data sources: Ministry of Health and Social Services.15,16
Risk ratio (MENA group vs non-MENA group) is significant if 95% CI excludes 1.
Adjusted for maternal age, parity, maternal comorbidity, infant sex, multiple birth, maternal education, socioeconomic disadvantage, and birth year.
Any injury to the infant during labor or delivery.
Respiratory distress syndrome, bronchopulmonary dysplasia, intraventricular hemorrhage, necrotizing enterocolitis, periventricular leukomalacia, and retinopathy of prematurity.
Compared with non-MENA mothers, MENA mothers had an elevated risk of gestational diabetes (RR = 1.51; 95% CI, 1.48-1.55) and cesarean delivery (RR = 1.06; 95% CI, 1.05-1.08) (Table 3). We also found a greater likelihood of placental abruption, chorioamnionitis, and uterine rupture among MENA mothers. However, MENA mothers were 30% to 50% less likely to have preeclampsia, postpartum hemorrhage, and severe maternal morbidity, including acute renal failure and ICU admission.
Risk of adverse pregnancy outcomes in mothers of MENA and non-MENA infants, Quebec, Canada, 2008-2020 a

Abbreviation: MENA, Middle Eastern or North African.
Mothers had delivered in any birthing hospital of Quebec. The MENA group included infants whose parents self-reported Arabic or Turkish mother tongue or were born in a North African or Middle Eastern country. The non-MENA group included infants whose parents had French or English mother tongue and were born in Canada. Data sources: Ministry of Health and Social Services.15,16
Risk ratio (MENA group vs non-MENA group) is significant if 95% CI excludes 1.
Adjusted for maternal age, parity, maternal comorbidity, infant sex, multiple birth, maternal education, socioeconomic disadvantage, and birth year.
Compared with non-MENA infants who had the same demographic characteristics, MENA infants had a greater risk of NICU admission if their mother was socioeconomically disadvantaged (RR = 1.88; 95% CI, 1.77-1.99) or aged < 25 years (RR = 1.58; 95% CI, 1.43-1.76) (Table 4). MENA mothers were 30% to 50% more likely than non-MENA mothers to have gestational diabetes if they had only a high school education or were socioeconomically disadvantaged. However, when we compared results among the increased risk subgroups (aged <25 y, presence of comorbidity, multiple pregnancies, high school education or less, and socioeconomic disadvantage), MENA mothers had a lower risk of preterm birth, preeclampsia, severe maternal morbidity, and maternal ICU admission than non-MENA mothers.
Risk of adverse pregnancy and birth outcomes in increased risk MENA and non-MENA subgroups, Quebec, Canada, 2008-2020 a

Abbreviation: MENA, Middle Eastern or North African.
The MENA group included infants whose parents self-reported Arabic or Turkish mother tongue or were born in a North African or Middle Eastern country. The non-MENA group included infants whose parents had French or English mother tongue and were born in Canada. Data sources: Ministry of Health and Social Services.15,16
Risk ratio (MENA group vs non-MENA group) is significant if 95% CI excludes 1.
Adjusted for maternal age, parity, maternal comorbidity, infant sex, multiple birth, maternal education, socioeconomic disadvantage, and birth year unless the variable was used for stratification.
Preexisting hypertension, diabetes mellitus type 1 or 2, obesity, dyslipidemia, and alcohol, tobacco, or other substance use disorders.
Most materially deprived quintile of the population based on neighborhood education, income, and unemployment.
Among mothers who delivered in any birthing hospital of Quebec.
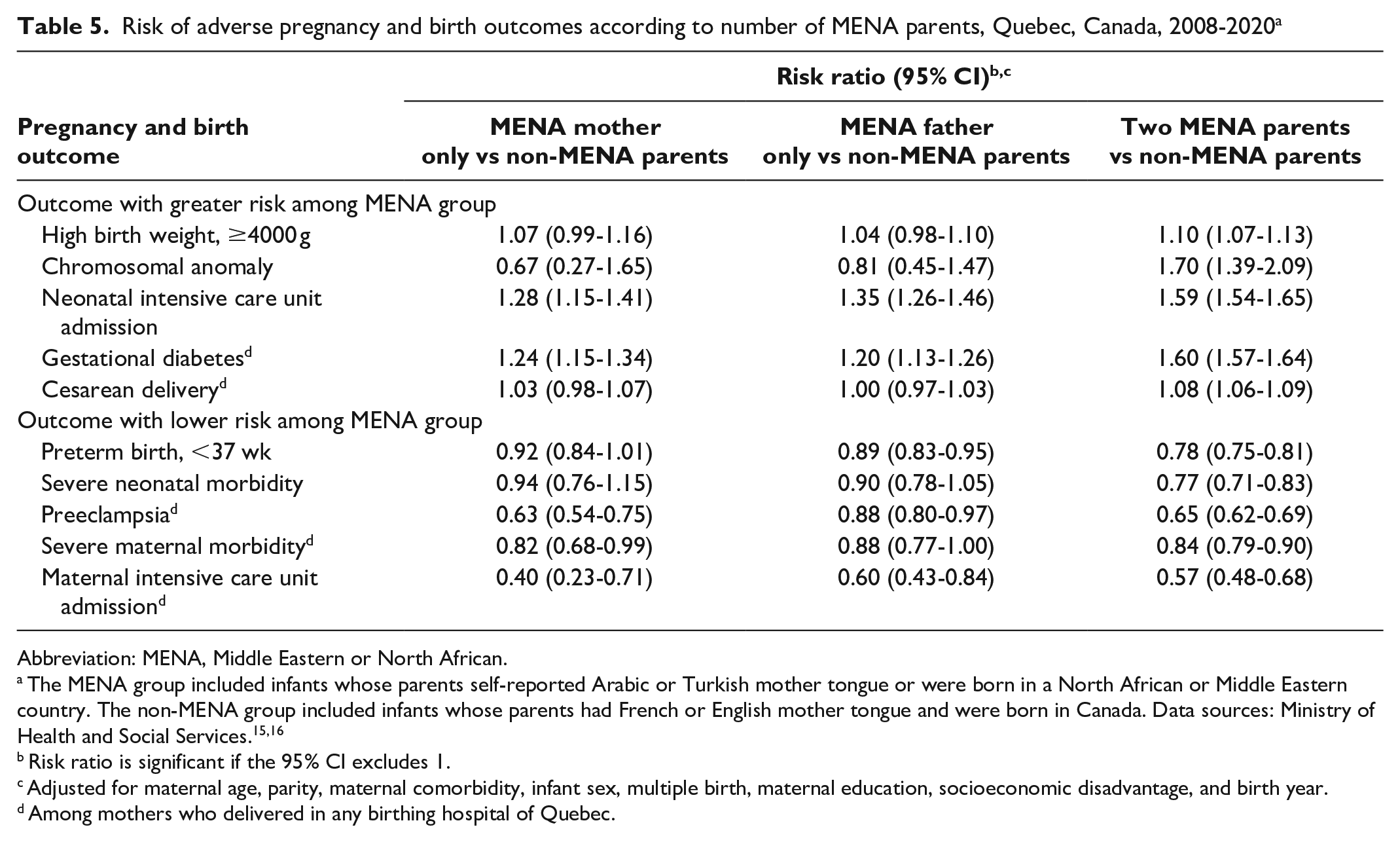
Having more than 1 MENA parent influenced the associations (Table 5). MENA infants (vs non-MENA infants) had a particularly elevated risk of chromosomal anomaly when both parents were MENA (RR = 1.70; 95% CI, 1.39-2.09). MENA infants were 1.6 times more likely than non-MENA infants to have a NICU admission (RR = 1.59; 95% CI, 1.54-1.65) and a mother with gestational diabetes (RR = 1.60; 95% CI, 1.57-1.64) when both parents were MENA. These associations were less pronounced when only 1 parent was MENA. Infants with 2 MENA parents were also less likely than infants with non-MENA parents to be born preterm (RR = 0.78; 95% CI, 0.75-0.81) and have severe neonatal morbidity (RR = 0.77; 95% CI, 0.71-0.83). Exclusion of births during the COVID-19 pandemic did not affect results (eTable 2 in the Supplement).
Risk of adverse pregnancy and birth outcomes according to number of MENA parents, Quebec, Canada, 2008-2020 a
Abbreviation: MENA, Middle Eastern or North African.
The MENA group included infants whose parents self-reported Arabic or Turkish mother tongue or were born in a North African or Middle Eastern country. The non-MENA group included infants whose parents had French or English mother tongue and were born in Canada. Data sources: Ministry of Health and Social Services.15,16
Risk ratio is significant if the 95% CI excludes 1.
Adjusted for maternal age, parity, maternal comorbidity, infant sex, multiple birth, maternal education, socioeconomic disadvantage, and birth year.
Among mothers who delivered in any birthing hospital of Quebec.
Discussion
Our observational study of 809 172 infants born in Canada from 2008 through 2020 suggested that MENA infants and mothers have elevated risks of several birth complications compared with non-MENA infants and mothers. Risks were elevated for gestational diabetes, high birth weight, cesarean delivery, chromosomal anomaly, and short-stay NICU admission. MENA infants and mothers had a generally lower risk of other adverse outcomes than non-MENA infants and mothers, including preeclampsia, preterm birth, severe maternal morbidity, and severe neonatal morbidity. For most conditions, these patterns were present whether the mother or father was MENA, although associations were more pronounced when both parents were MENA. Overall, the findings indicated that disparities in maternal and infant health between MENA and non-MENA infants and mothers may be concentrated in outcomes that can be readily managed with prenatal care. Our study suggested that MENA infants and mothers had outcomes similar to or more favorable than non-MENA infants and mothers, except for a few pregnancy complications that may require closer obstetric follow-up.
Some evidence has suggested that MENA mothers may be predisposed to developing gestational diabetes.7,10,22 In a study of 207 458 US births, MENA mothers were 1.31 times more likely to have gestational diabetes than non-Hispanic White mothers. 7 Cohort studies from France and Sweden showed that MENA immigrant women have twice the risk of gestational diabetes than women who are not immigrants.10,22 However, the reason for these associations is unclear, as MENA women tend to have a low prevalence of risk factors for gestational diabetes, including obesity, hypertension, smoking, and a Western diet.5,23 Even after adjustment for several of these factors, MENA mothers in our data had a 50% higher risk of gestational diabetes than non-MENA mothers.
In contrast, MENA mothers in our population had a 30% lower risk of preeclampsia, a hypertensive disorder of pregnancy that frequently clusters with gestational diabetes. 24 Studies from other countries have tended to align with our findings, including an analysis suggesting that migrants from Syria, Iraq, Somalia, Eritrea, and Afghanistan have a 30% lower risk of preeclampsia than Swedish-born mothers. 10 In an analysis of more than 9 million infant deliveries from 6 high-income countries, MENA immigrants had 38% lower odds of preeclampsia than other women in the population. 25 Because risk factors for preeclampsia are frequently similar to those for gestational diabetes,24,26 MENA women may have genetic traits or other unique characteristics that are specific to gestational diabetes. Type 2 diabetes mellitus has a genetic component, 27 and MENA people are known for having a high risk of type 2 diabetes mellitus. 4
Only a few studies have examined surgical outcomes of pregnancy among MENA mothers.10,28-30 An analysis of 287 000 women from Sweden suggested that the risk of cesarean delivery, whether planned or unplanned, was 50% higher for migrants from MENA countries than for other women, 10 whereas a population-based study of 500 000 live births from Norway found that the rate of cesarean delivery was similar among MENA and non-MENA mothers. 28 The available literature has also suggested that MENA women may have risks of uterine rupture and hysterectomy similar to non-MENA women,29,30 although we found elevated risks. Why associations are not present in the literature is not clear, as cesarean delivery is common in patients with gestational diabetes and macrosomia. 31 MENA mothers in our study had an elevated risk of macrosomia.
MENA infants were more likely than non-MENA infants to be admitted to a NICU. Although outcomes of MENA infants have received limited attention in the literature, a study of 192 527 term infants from Israel found that MENA infants were more frequently admitted to a NICU than non-MENA infants. 32 In our study, we found that MENA infants had mainly short stays in intensive care, suggesting that transient complications from which infants quickly recovered were the most likely underlying reasons for admission. Pregnancy complications that are common among MENA mothers, such as gestational diabetes and cesarean delivery, may be contributing factors, as these morbidities have been associated with risk of NICU admission. 32 MENA infants and mothers in our population had a low risk of preterm birth, low birth weight, and severe neonatal morbidity, factors associated with prolonged stays in NICUs. 33
We found that the risk of admission to NICUs was particularly pronounced for MENA infants from increased risk subgroups, suggesting that social conditions may explain some of the disparities in maternal and infant health. Stigma and discrimination may have negative effects on maternal health during pregnancy. 34 Stigma and discrimination may also be associated with mistrust in the health care system and reduced use of prenatal care services.4,5 In the United States, MENA women are 60% less likely than non-Hispanic White women to seek prenatal care in the first trimester of pregnancy. 7 Cultural and religious beliefs may also influence access and quality of antenatal and perinatal care. MENA women may have preferences in the sex of their health care providers or misconceptions related to illness causation 6 ; thus, providing culturally sensitive care may help improve maternal and infant outcomes. Language barriers, transportation barriers, lack of social support or health literacy, and lack of knowledge of services available to pregnant women may also prevent adequate care.4,6
Studies of birth defects among MENA people are sparse. In a study of 1.6 million live births in the United States, MENA infants had a similar risk of birth defects as non-MENA infants 35 ; however, chromosomal anomalies were an exception, as MENA infants had slightly higher rates of Down syndrome and Edwards syndrome. 35 In a study of 3 million Canadian births, MENA women were 1.5 times more likely than non-MENA women to have stillbirths due to congenital anomalies. 9 Up to 20% of stillbirths can be attributed to chromosomal anomalies. 36 MENA infants and women in our study had elevated risks of both chromosomal anomalies and stillbirth. Although the reason for these risks is unclear, advanced maternal age is a strong risk factor for Down syndrome. Religious beliefs may also discourage pregnancy terminations among MENA people. 37 The risk of having an infant with a chromosomal anomaly was greater when both parents were MENA and more likely to share the same cultural and religious background than when only 1 parent was MENA.
We found that MENA infants and mothers had low risks of severe maternal morbidity, severe neonatal morbidity, and preterm birth. Although few studies have examined severe maternal and neonatal morbidity among MENA infants and mothers, evidence has shown that preterm birth may be infrequent in this population. 12 In a study of 617 451 US births, MENA mothers were up to 25% less likely than non-Hispanic White mothers to have a preterm birth. 12 MENA mothers also had lower rates of infant mortality and obstetric hemorrhage than non-MENA mothers.10,13,14,29 Some of these patterns may relate to lifestyle.5,7 In the United States, MENA mothers are 80% less likely than non-Hispanic White mothers to consume alcohol and tobacco during pregnancy. 7 MENA women in the United States have low rates of obesity and hypertension. 5 A healthy immigrant effect, caused by policies that encourage the selection of immigrants who have high education levels and are generally healthy, may also contribute to these low rates. 38 In Canada, immigrants are up to 40% less likely than nonimmigrants to be overweight, have heart disease, or have other chronic conditions. 38 However, acculturation may attenuate these differences over time.7,39
Limitations
This study had several limitations. First, nondifferential misclassification may have attenuated associations, as language and country of birth were self-reported and potentially miscoded. Second, we could not account for MENA parents born in Canada whose primary language was not Arabic. Third, we could not stratify the analysis by country of birth due to low sample sizes. Fourth, outcomes and other covariates may have been nondifferentially miscoded. Fifth, we could not determine the underlying reason for NICU admission. Sixth, we could not examine planned versus unplanned cesarean deliveries. Seventh, we could not determine whether residual confounding, as a result of lack of data on self-reported race, religion, immigration status, length of stay in Canada, acculturation, and language proficiency, led to overestimated or underestimated associations. We also lacked information on diet, physical activity, medication use, and vaccination status. Confounders such as maternal obesity and substance use may have been underreported. We had no information on the number, timing, and quality of prenatal visits or the delivery hospital. Eighth, the cohort is representative of MENA people in Quebec, but the findings may not generalize to MENA populations in other provinces or countries. Further research is needed to determine how outcomes in MENA people compare with outcomes in other racial and ethnic minority groups.
Conclusions
Despite findings of an elevated risk of gestational diabetes, chromosomal anomaly, high birth weight, and short stays in NICUs among MENA infants and mothers in our population, MENA infants and mothers were less likely than non-MENA infants and mothers to have preeclampsia, severe maternal or neonatal morbidity, and preterm birth. Improved understanding is needed to explain these patterns, as findings may help improve pregnancy and birth outcomes in this population. In the meantime, MENA patients may benefit from early prenatal interventions to improve outcomes of gestational diabetes.
Supplemental Material
sj-docx-1-phr-10.1177_00333549251314304 – Supplemental material for Pregnancy and Birth Outcomes Among Middle Eastern or North African Infants and Mothers in Quebec, Canada, 2008-2020
Supplemental material, sj-docx-1-phr-10.1177_00333549251314304 for Pregnancy and Birth Outcomes Among Middle Eastern or North African Infants and Mothers in Quebec, Canada, 2008-2020 by Gabriel Côté-Corriveau, Nicole Silva-Lavigne, Méloë Maigné, Aimina Ayoub, Thuy Mai Luu, Olivier Drouin and Nathalie Auger in Public Health Reports
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Quebec Population Health Research Network (266659) and the Fonds de recherche du Québec-Santé (296785).
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.