
Abstract
Objectives:
Alaska has among the highest traumatic brain injury (TBI) mortality rates in the United States. We characterized the epidemiology of TBIs in the country’s largest and most sparsely populated state to guide prevention efforts.
Methods:
This cross-sectional study analyzed TBI-associated hospitalization and mortality rates in Alaska from 2016 through 2021. Data included people with TBI-associated hospitalization or death in Alaska. We compared age-adjusted rates using national data, with analysis by age, sex, race and ethnicity, and injury mechanism. Logistic regression explored factors influencing mortality among hospitalized patients with TBI.
Results:
TBI-associated hospitalization rates per 100 000 population in Alaska were highest among adults aged ≥75 years (310.4), by sex among males (123.3), and by race among American Indian and Alaska Native (AI/AN) people (186.7). Patients with TBI-associated hospitalizations due to self-harm were approximately 8.6 times as likely to die as patients with unintentional injuries. Alaska’s age-adjusted TBI-associated mortality rate per 100 000 population was twice the national rate (36.2 vs 17.3). TBI-associated mortality rates in Alaska exceeded national averages across all demographic characteristics and injury mechanisms. Adults aged ≥75 years, males, and AI/AN people in Alaska had TBI-associated death rates that were 1.3, 1.9, and 2.0 times higher, respectively, than national rates. Alaska’s TBI-associated mortality rate from suicide was 2.6 times the national average, with notable racial disparities for AI/AN people.
Conclusions:
TBIs are a considerable source of morbidity and mortality in Alaska, with disproportionate effects observed among population groups. These findings underscore the need for increased focus on mechanism-specific TBI prevention activities, particularly for older adults and AI/AN people.
Of all common neurologic disorders, traumatic brain injury (TBI) has the highest incidence, presenting a substantial yet preventable public health burden worldwide. In the United States, TBIs account for approximately 30% of all annual injury deaths and contributed to approximately 1 million deaths in the past 2 decades.1,2 Moreover, TBIs can result in substantial morbidity, contributing to approximately 214 000 hospitalizations in 2020 alone. 3 Although most TBIs are not fatal, they can lead to lifelong health problems (and associated medical costs) that can result in increased mortality risk from other causes.4,5
Residents of rural states have a disproportionately higher incidence of TBI-associated morbidity than nonrural states and are at increased risk for TBI-associated mortality. 6 The causes of this disparity include higher rates of suicide and unintentional motor vehicle crashes in rural areas and decreased access to prehospital care, high-level trauma services, neurosurgical services, and postdischarge rehabilitative services.6-9
Alaska is the largest and most sparsely populated state and is recognized for having among the highest rates of TBI-associated mortality nationwide. 6 Nevertheless, characterization of the epidemiology of TBI-associated morbidity and mortality among Alaska residents has been limited. In this study, we assessed and characterized the epidemiology of TBIs in Alaska. Our objectives included calculating TBI-associated hospitalization and mortality rates in Alaska, analyzing demographic and injury-specific risk factors associated with TBI mortality among hospitalized patients, and comparing Alaska’s TBI-associated mortality rates with national rates for the corresponding period.
Methods
We obtained statewide hospitalization data from 2016 through 2021 (6 calendar years) from the Alaska Trauma Registry (ATR), 10 which covers all 24 acute-care hospitals in Alaska. ATR collects data on seriously injured patients admitted to or held for observation in Alaska hospitals, declared dead in the emergency department, or transferred to another acute-care hospital. The International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) 11 documents injury diagnoses and external causes of injury. Additional variables collected in the ATR for analysis comprised patient age, sex, race and ethnicity, date of injury, outcome at discharge (death or survival), number and type of preexisting comorbidities, hospital length of stay, Glasgow Coma Scale 12 upon emergency department arrival, and Injury Severity Score 13 upon hospital admission.
We used ATR data to identify TBI-associated hospitalizations with the following criteria: (1) Alaska residency, (2) injuries sustained from 2016 through 2021, and (3) a primary ICD-10-CM injury diagnosis code and a Centers for Disease Control and Prevention (CDC)–referenced ICD-10-CM code indicative of a TBI 14 (S02.0-S02.1, S02.8-S02.91, S04.02-S04.04, S06, S07.1, and T74.4) in any diagnosis fields. Injuries could include initial hospitalization following a TBI and subsequent hospitalizations due to head injury sequalae. We categorized injuries by the underlying mechanism of injury, as defined by the ICD-10-CM External Cause of Injury Matrix 15 grouped into the following principal mechanisms of injury: unintentional falls, unintentional motor vehicle crashes, self-harm, assault, and other or unspecified. We classified injuries attributed to all-terrain vehicles or snow machines as unintentional motor vehicle crashes for all analyses due to their extensive use in Alaska as a primary form of motor vehicle.
We calculated age-adjusted hospitalization rates by sex, age, race and ethnicity, and principal mechanism of injury by using midyear population data from the Alaska Department of Labor and Workforce Development as denominators. 16 To assess demographic and injury-specific factors associated with mortality among hospitalized patients with TBI, we categorized nonsurvivors as prehospital deaths (patients declared dead in the emergency department) or in-hospital deaths (admitted but died before discharge); we categorized people who were discharged alive as survivors. Univariate comparisons between survivors and nonsurvivors analyzed demographic and injury-specific characteristics by using a Pearson χ2 test or t test as appropriate. We considered differences to be significant when P < .05. We used logistic regression to quantify observed associations between patient characteristics and mortality odds. We obtained a full model by adding covariates in a forward selection process, keeping variables that significantly improved the model fit according to tests of differences between log-likelihoods of nested models. We calculated unadjusted odds ratios and adjusted odds ratios (AORs) and corresponding 95% CIs to determine predictive factors linked to increased mortality odds after a TBI among hospitalized patients.
To characterize TBI-associated mortality among Alaska residents, we collected death certificates from Alaska’s vital records system 17 during the study period. We identified TBI-associated deaths by the presence of 2 codes from the International Classification of Diseases, Tenth Revision 18 : an injury-associated underlying cause-of-death code (V01-Y36, Y85-Y87, Y89, U01-U03) and a TBI-associated code aligned with the established TBI death surveillance definition 19 in the sequence of conditions contributing to death. For determining the principal mechanism of injury, we categorized underlying cause-of-death fields based on external causes, including unintentional motor vehicle crashes, unintentional falls, suicide, homicide, and other or unspecified codes for infrequent or nonspecific cases. To enable accurate comparison with corresponding national TBI-associated mortality rates, we obtained a death record dataset for the study period from the “mortality multiple cause” files of CDC’s National Vital Statistics System. 20 These files, sourced from state registries through a partnership with the National Center for Health Statistics, include death records for all US residents. Alaska rates were based on population data from the Alaska Department of Labor and Workforce Development, 16 while national rates used US Census Bureau estimates. 21 We calculated age-adjusted rates by using the 2000 US standard population weighting. We determined 95% CIs to account for random variation in the number of deaths and hospitalizations each year. We identified significant differences in age-adjusted rates of TBI-associated mortality between Alaska and the national average by examining nonoverlapping 95% CIs.
We further characterized mortality rates by age, sex, race and ethnicity, year of death, and mechanism of injury. For race-based calculations, categories included American Indian or Alaska Native (AI/AN), White, and a combined category, “another race.” We used the combined category because of low population counts in Alaska for the following races: Asian, Native Hawaiian or other Pacific Islander, and Black or African American. We obtained data for denominators for each race-based calculation for Alaska from the Alaska Department of Labor and Workforce Development. 16 We computed national race-specific rates by using identical single-race population denominators obtained from the National Center for Health Statistics. 22 For ethnicity, we classified all people with Hispanic ethnicity as Hispanic, regardless of race, allowing identification as Hispanic and any race (eg, Hispanic White). Hispanic counts are therefore not mutually exclusive in race counts.
This study was reviewed by CDC and conducted consistent with federal law and CDC policy (45 CFR part 46, 21 CFR part 56; 42 USC §241d; 5 USC §552a; 44 USC §3501 et seq). CDC determined that this work did not constitute human subjects research because data were collected and analyzed as part of routine public health surveillance.
Results
From 2016 through 2021, a total of 3846 Alaska residents were hospitalized with TBIs (Table 1), resulting in an age-adjusted hospitalization rate of 109.6 (95% CI, 105.7-113.5) per 100 000 population. The median (IQR) age at hospitalization was 46 (25-66) years, with the highest rate per 100 000 population observed among those aged ≥75 years (310.4; 95% CI, 284.8-336.1). Males represented 64.8% of TBI hospitalizations, with an age-adjusted rate 1.8 times that of females (123.3 [95% CI, 118.3-128.4] vs 70.4 [95% CI, 66.7-74.4]) per 100 000 population. AI/AN people, who represent 15.7% of Alaska’s population, accounted for 31.0% of all TBI-associated hospitalizations. AI/AN people also had an age-adjusted hospitalization rate 2.4 times that of White people in Alaska (186.7 [95% CI, 175.7-198.5] vs 77.3 [95% CI, 74.0-80.8]) per 100 000 population. Unintentional falls constituted the largest single mechanism of injury, representing 43.4% of all TBI hospitalizations, with an age-adjusted rate of 155.0 (95% CI, 142.3-168.6) per 100 000 population, approximately 5 times higher than the latest national estimate. Unintentional motor vehicle crashes were next, with a rate of 31.8 (95% CI, 27.1-37.2) per 100 000 population in Alaska.
Rate of traumatic brain injury–associated hospitalizations, by patient demographic and injury-specific characteristics, Alaska, 2016-2021 a

Data sources: Alaska Department of Health, 10 Alaska Department of Labor and Workforce Development. 16
Apart from age, variables were age standardized to the 2000 standard US population.
Race and ethnicity are not mutually exclusive categories.
Includes Black or African American, Native Hawaiian or other Pacific Islander, and Asian.
During the study period, 370 patients died, representing 9.6% of all TBI-associated hospitalizations. Of these, 56 were in-hospital deaths and 314 were prehospital deaths, representing 1.5% and 8.2% of hospitalizations, respectively. Univariate analysis found significant demographic and injury-specific differences between surviving patients with TBI and those who died (Table 2). Patients who died after a TBI were significantly older, had lower median Glasgow Coma Scale scores, and had higher median Injury Severity Scores than those who survived. By mechanism of injury, patients whose mechanism was self-harm accounted for 77 deaths out of 370 (20.8%) and 43 cases of survival out of 3476 (1.2%). We found no significant differences in the type or number of preexisting comorbidities between patients who died and those who survived their TBI.
Characteristics of hospitalized patients with fatal and nonfatal TBIs, Alaska, 2016-2021 a

Abbreviations: GCS, Glasgow Coma Scale; ISS, Injury Severity Score; TBI, traumatic brain injury.
Data sources: Alaska Department of Health, 10 Alaska Department of Labor and Workforce Development. 16
All nonsurvivors, including prehospital deaths (n = 314) and in-hospital deaths (n = 56).
Determined by Pearson χ2 test or t test as appropriate; P < .05 considered significant.
Scale ranges from 3 to 15; a higher score indicates better neurologic function. 12
Scale ranges from 0 to 75, with 1 representing a minor injury and 75 representing a fatal injury; a score ≥15 indicates a major traumatic injury. 13
Includes Black or African American, Native Hawaiian or other Pacific Islander, and Asian.
Race and ethnicity are not mutually exclusive categories.
Injuries attributed to self-harm (International Classification of Diseases, Tenth Revision, Clinical Modification code X71-X83). 11
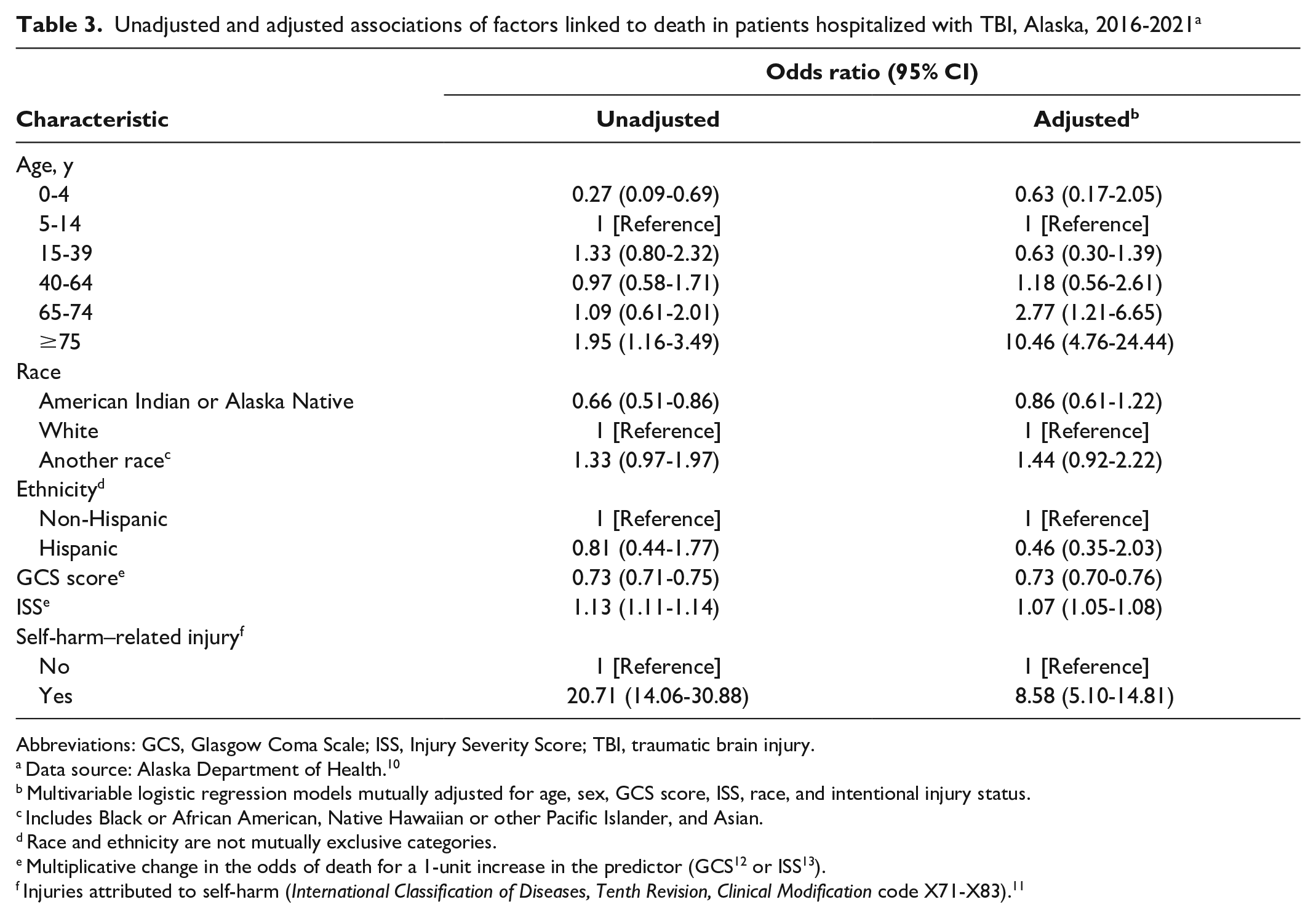
After adjusting for factors significantly associated with mortality (Table 3), age was the strongest independent risk factor for death after a TBI. Patients aged ≥75 years were 10.5 times as likely to die after a TBI as patients aged 5 to 14 years (AOR = 10.46; 95% CI, 4.76-24.44). A self-harm–related TBI was also a significant independent risk factor for death among hospitalized patients. Patients with a self-harm–related TBI were 8.6 times as likely to die as patients with an unintentional or accidental injury (AOR = 8.58; 95% CI, 5.10-14.81). Notably, 77% of self-harm–related TBI cases were attributable to a firearm, with a 90% fatality rate among patients with TBI who had firearm-related injuries. Patients who died after a TBI were also more likely than those who survived to have a lower Glasgow Coma Scale score on arrival to the emergency department (AOR = 0.73; 95% CI, 0.70-0.76) and a higher Injury Severity Score on admission (AOR = 1.07; 95% CI, 1.05-1.08).
Unadjusted and adjusted associations of factors linked to death in patients hospitalized with TBI, Alaska, 2016-2021 a
Abbreviations: GCS, Glasgow Coma Scale; ISS, Injury Severity Score; TBI, traumatic brain injury.
Data source: Alaska Department of Health. 10
Multivariable logistic regression models mutually adjusted for age, sex, GCS score, ISS, race, and intentional injury status.
Includes Black or African American, Native Hawaiian or other Pacific Islander, and Asian.
Race and ethnicity are not mutually exclusive categories.
Multiplicative change in the odds of death for a 1-unit increase in the predictor (GCS 12 or ISS 13 ).
Injuries attributed to self-harm (International Classification of Diseases, Tenth Revision, Clinical Modification code X71-X83). 11
From 2016 through 2021, Alaska reported 1527 TBI-associated deaths, resulting in an age-adjusted mortality rate of 36.2 (95% CI, 31.8-40.6) per 100 000 population, approximately twice that of the corresponding national average of 17.3 (Table 4). Notably, during this period in Alaska, we found that 1 in 4 deaths among people aged <30 years followed a TBI. Consistent with national patterns, the TBI-associated mortality rate per 100 000 population was highest by race and ethnicity among AI/AN people (65.9; 95% CI, 59.6-72.9), by sex among males (53.3; 95% CI, 50.1-56.6), by mechanism of injury among those with injuries attributed to suicide (17.3; 95% CI, 16.0-18.7), and by age among people aged ≥75 years (97.8; 95% CI, 82.9-115.3).
Number and rate of traumatic brain injury–associated deaths in Alaska and United States, by selected characteristics, 2016-2021 a

Data sources: Alaska Department of Health, 17 Alaska Department of Labor and Workforce Development, 16 Centers for Disease Control and Prevention. 20
Apart from age, variables were age standardized to the 2000 standard US population.
Race and ethnicity are not mutually exclusive categories.
Includes Black or African American, Native Hawaiian or other Pacific Islander, and Asian.
In national-level data, 27 death records were missing data on age.
For every sex, race, and age-specific subgroup, Alaska’s TBI-associated mortality rates surpassed the corresponding national rates (Table 4). Among people aged 15 to 24 years in Alaska, the rate of TBI-associated mortality per 100 000 population was approximately 4 times higher than the corresponding national average for the same age group (62.6 [95% CI, 55.7-70.3] vs 16.2 [95% CI, 16.1-16.4]). Similarly, children in Alaska aged 5 to 14 years had a rate of TBI-associated mortality per 100 000 population approximately 4 times higher than the national average (8.3 [95% CI, 6.1-11.3] vs 1.9 [95% CI, 1.9-2.0]).
TBI-associated mortality rates in Alaska exceeded national rates across all injury mechanisms. Apart from TBI-related mortality from unintentional falls, the rates of TBI-associated mortality in Alaska were consistently twice as high as the corresponding national averages for all other injury mechanisms (Table 4). Suicide was the predominant mechanism of injury for TBI-associated mortality in the nation and in Alaska. However, the suicide-attributed TBI-associated mortality rate per 100 000 population in Alaska was more than double the corresponding national average (17.3 [95% CI, 16.0-18.7] vs 6.7 [95% CI, 6.7-6.8]).
Rates of TBI-associated mortality were significantly higher in Alaska among White and AI/AN people than in the nation. Disparities in TBI-associated mortality rates between racial groups were more pronounced in Alaska, where AI/AN people had approximately double the TBI-associated mortality rate per 100 000 population of White people (65.9 [95% CI, 59.6-72.9] vs 33.0 [95% CI, 30.9-35.3]). National rates showed relatively less between-race disparity: the TBI-associated mortality rate per 100 000 population was 32.6 (95% CI, 31.5-33.6) among AI/AN people and 19.9 (95% CI, 19.9-20.0) among White people.
TBI-associated mortality rates among AI/AN people in Alaska exceeded the rates for AI/AN people nationally across all mechanisms of injury (Table 5). For TBI-associated mortality attributed to homicide, the rate per 100 000 population among AI/AN people in Alaska was 3.8 times higher than among AI/AN people nationally (11.1 [95% CI, 8.6-14.2] vs 1.9 [95% CI, 1.7-2.1]). The TBI-associated mortality rate per 100 000 population attributed to suicide was also significantly higher among AI/AN people in Alaska than among AI/AN people nationally (28.9 [95% CI, 24.5-34.1] vs 6.4 [95% CI, 6.0-6.8]).
Rate of traumatic brain injury–associated deaths in Alaska and United States, by race and mechanism of injury, 2016-2021 a

Data sources: Alaska Department of Health, 17 Alaska Department of Labor and Workforce Development, 16 Centers for Disease Control and Prevention. 20
Age standardized to the 2000 standard US population.
Race and ethnicity are not mutually exclusive categories.
Includes Black or African American, Native Hawaiian or other Pacific Islander, and Asian.
Discussion
Alaska’s TBI-related mortality rate per 100 000 population was more than double the corresponding national average (36.2 [95% CI, 31.8-40.6] vs 17.3 [95% CI, 17.3-18.4]) during 2016 through 2021. One in 4 deaths among people aged <30 years occurred following a TBI. Suicide was the most common mechanism of TBI-associated mortality among Alaskans, with AI/AN people being disproportionately affected. Consistent with national findings, we found notable disparities in TBI mortality and morbidity among population groups. Older adults in Alaska had the highest rates of hospitalization and mortality due to TBIs, aligning with the established association between older age and an increased risk for, and severity from, such injuries.14,23,24 We identified older age (≥75 y) as the most significant independent risk factor for mortality among patients in Alaska with TBI-associated hospitalization. This finding underscores the need for focused injury prevention programs in this age group, particularly considering its high rate of TBI-associated hospitalizations primarily from unintentional falls and its increased risk for mortality after hospitalization. Additional interventions addressing injury mechanisms such as unintentional falls, the leading cause of TBI-associated hospitalizations in older adults, are crucial. 14
In Alaska, males had significantly higher rates than females of TBI-associated hospitalization and mortality, mirroring a national trend where TBI hospitalization and death rates are 2 and 3 times higher, respectively, among males than among females. 3 This sex gap is attributed to factors such as increased involvement in physical altercations, military service, contact sports, and firearm-related suicides. Underreported and undetected TBIs among women, especially those related to intimate partner violence and assault, may contribute to an underestimated rate of TBI among women in Alaska. This point is particularly notable given the high prevalence of intimate partner violence, especially among AI/AN women in Alaska.25,26
Our study highlights the link between self-harm–related injuries and mortality among hospitalized patients with TBI in Alaska. After older age, self-harm–related injuries, primarily through firearms, emerged as an independent risk factor for mortality among hospitalized patients with TBI in Alaska. With firearms contributing to 98% of self-harm–related TBI-associated deaths in Alaska and 77% of self-harm–related TBI hospitalizations and with the absence of a level 1 trauma center in the state, the opportunity for lifesaving interventions diminishes substantially. Addressing this issue may involve integrating community-based interventions with real-time suicide surveillance to effectively monitor and respond to ongoing trends.
Racial disparities in TBI-associated mortality and hospitalizations have been reported nationally, with AI/AN people consistently having the highest rates.27-29 This disparity is even more pronounced in Alaska, where the gap in TBI-associated mortality rates between racial groups exceeds the national average. The TBI-associated mortality rate among AI/AN people in Alaska is twice as high as that of White people, largely due to TBI-related deaths from suicide and unintentional motor vehicle crashes, which account for 64% of all TBI-related fatalities and disproportionately affect AI/AN populations. When compared with White people, AI/AN people have 2.3 times higher rates of TBI-related suicides and 2.5 times higher rates of TBI-related motor vehicle crashes. The high rates of suicide among AI/AN populations are likely influenced by factors such as historical trauma, community violence, and exposure to suicide in their communities, leading to some of the highest suicide rates in the country among AI/AN people in Alaska. 30 Elevated rates of substance abuse among AI/AN people as compared with other racial groups likely also contribute to higher TBI-related morbidity and mortality. These disparities should not be causally linked to race; rather, structural racism, historical exposures, and daily living conditions are key factors. Addressing these issues requires understanding complex factors such as substance misuse, mental health challenges, poverty, and health care barriers. Further research and culturally appropriate programs are essential to support AI/AN people at risk for TBI mortality, considering Alaska’s unique context.
TBI prevention initiatives in Alaska are multifaceted, addressing various safety and health concerns. Public campaigns and educational programs focus on motor vehicle safety and safety gear distribution.31-33 Specific interventions include fall prevention for older adults through free distribution of ice cleats and balance programs.34-36 Suicide prevention efforts are diverse, spanning school-based initiatives, tribal-focused programs, community-based strategies, and mental health support.37-39 Alaska’s Statewide Suicide Prevention Council also collaborates with various partners to address suicide rates, 40 while the Alaska Native Tribal Health Consortium provides education, training, and telehealth services.41,42 Injury prevention efforts also address head trauma from motor vehicle crashes. The Center for Safe Alaskans (https://safealaskans.org) promotes safe transportation practices through child passenger education, free car seat fittings, and teen driver resources. Looking ahead, the 2020-2025 Alaska State Plan for Brain Injury aims to enhance TBI prevention and management through a TBI registry. 43 This registry will track trends and identify gaps in TBI needs, leading to expanded services. Ongoing research by the Alaska Native Epidemiology Center and the Alaska Department of Health supports these efforts, contributing to a nuanced understanding of TBI in Alaska.44-46
Limitations
This study had several limitations. First, non-TBI diagnoses might have contributed to deaths and hospitalizations in cases of multiple injuries. Second, AI/AN people are often misclassified in surveillance and administrative data systems, with the lowest agreement between self-reported and recorded race. 47 Studies consistently show underestimation of mortality rates in these populations,48-50 which may lead to underestimating outcomes in our study. However, more data are needed to more fully understand the magnitude and direction of this potential source of bias in Alaska. Third, because of low population numbers and the statistical reliability of rates, additional racial groups in Alaska could not be included. Fourth, out-of-state aeromedical transport of patients with severe TBI is common in Alaska, potentially excluding some hospitalizations from our rates. Finally, substantial variation likely exists among hospitals in capturing the high-acuity ICD-10-CM codes used to calculate TBI hospitalization rates, making accurate comparisons among regions challenging.51,52
Conclusion
As the first epidemiologic study to our knowledge to comprehensively assess TBI-associated morbidity and mortality in Alaska, our findings highlight the considerable public health burden of TBIs and notable disparities in TBI rates in the state. They also highlight the need for focused prevention efforts and future studies to better understand the effectiveness of these prevention efforts once implemented.
Footnotes
Acknowledgements
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.