
Abstract
To reduce opioid-related morbidity and mortality, local coalitions on substance use prevention in Kern County, California, have sought to increase equitable engagement and reengagement with harm reduction supplies, including naloxone. Through a community–academic partnership and funding from the local managed health care plan in Kern County, we ordered, stocked, and monitored a temperature-controlled outdoor harm reduction vending machine (HRVM) in Bakersfield, California. We outlined the necessary steps for successful procurement and implementation of community-based HRVMs. To increase acceptability, we engaged in open dialogue with our partners, interested parties, and people with lived experience of substance use to inform the contents of the harm reduction supply kits. In addition, we consulted the literature, physicians, and epidemiologists to inform best practices for the quantity of supplies per kit and the frequency limits for dispensation. To ensure long-term sustainability, we secured grant funding from the California Harm Reduction Supply Clearinghouse to maintain a backstock of harm reduction supplies for the kits, successfully applied for the Naloxone Distribution Project through the California Department of Health Care Services for a continuous supply of free naloxone, and developed student internship and research assistant positions through our academic partner to support participant recruitment and data collection and management efforts. Our efforts culminated in the launch of the county’s first HRVM and orders for 2 additional HRVMs. Through our experiences, we gained insight on how to improve the feasibility, acceptability, and sustainability of community-based HRVMs, which can enhance health equity.
Keywords
Since 1999, drug overdoses have killed almost 1 million people in the United States, 1 and annual rates of fatal drug overdoses have been increasing. 2 Fentanyl and synthetic opioids account for approximately 75% of drug overdose deaths. 1 Although overdose fatalities have reached historic highs for all racial and ethnic groups in the United States, Black people in the United States have had the steepest increase in rate of drug overdose deaths of any other racial or ethnic group since 2015, 3 and drug mortality rates have tripled among the Latine population since 2011. 4 Similarly, people experiencing homelessness are at elevated risk for drug fatalities. 5 Furthermore, the increases in illicit heroin and synthetic opiate use and injection drug use have been accompanied by public health issues, such as increases in the prevalence of hepatitis C virus (HCV) and HIV infection, which also disproportionately affect Black and Latine populations and people experiencing homelessness. 6
Purpose
In response to national and local trends in drug overdose and HCV and HIV infection rates, cities across the United States have started implementing harm reduction vending machines (HRVMs). 7 However, to our knowledge, no studies to date have addressed community-based HRVM reach and effectiveness in harm reduction supply access or addressed whether HRVMs decrease health disparities among racial and ethnic minority groups and people experiencing homelessness. Low-barrier HRVMs can increase access to harm reduction services, which could improve opioid overdose prevention practices and reduce the rates of opioid-related morbidity and mortality. 8 To examine the feasibility of applying this intervention in predominantly Latine and Black communities with high levels of income inequality, we developed a community–academic partnership and installed, stocked, and monitored a free HRVM outside a federally qualified health center in a mixed-use residential community.
Methods
Setting
More than 1 in 10 nationwide fatal drug overdoses occurred in California in 2021. 9 Although Black people comprise 5% of the California population, 10 rates of fatal opioid overdoses per 100 000 population were second highest among Black people, after American Indian or Alaska Native people. 11 Of the 2.4 million people in the United States with HCV infection, 321 900 reside in California, with disproportionate rates of new and chronic HCV infections reported among racial and ethnic minority groups. 12 Similarly, the prevalence rate of HIV infection in California is higher than the national prevalence rate. 12 According to a recent meta-analysis, people who inject drugs who experience homelessness or housing instability have a greater risk for HIV infection than people who have housing. 13 Both Black and Latine Californians are disproportionately affected by HIV compared with other racial and ethnic groups; in 2020, Black men were 4.3 times more likely and Black women were 5.4 times more likely to be diagnosed with HIV compared with their White counterparts, and Latine people comprised 50% of all new HIV diagnoses. 14
Intervention
Numerous studies have documented the role of syringe service programs (SSPs) in reducing the transmission of bloodborne pathogens and increasing naloxone engagement. 15 According to a recent study that used a decision analytic model, opioid overdose interventions such as naloxone, a life-saving medication approved by the US Food and Drug Administration to treat opioid overdoses, were estimated to reduce opioid-related fatalities by 37% in populations with opioid use disorder and no medication to treat opioid use disorder. 16 However, disparities in the use of SSPs among racial and ethnic minority groups have been reported. One study reported that Black people in the United States were less likely to access SSPs and that Latine people in the United States who had to travel longer distances between SSP sites and locations of drug purchase were significantly less likely to use SSPs than their White counterparts. 17
With the international success of HRVMs to increase access to naloxone and harm reduction supplies, 18 Clark County, Nevada, launched the first HRVM project (Trac-B Exchange) in the United States in 2017. 7 An initial report on Trac-B Exchange showed an association between naloxone dispensation at HRVMs and decreased opioid-related fatalities. However, the study did not examine the role of participants’ race and ethnicity in rates of opioid-related overdoses. 7
In a 2023 study from Ohio that evaluated the effects of an HRVM on accessibility to harm reduction supplies, the HRVM substantially increased the availability and distribution of harm reduction supplies, exceeding distribution rates from SSPs. 19 Moreover, the study showed an association between implementation of the HRVM and a decrease in fatal opioid overdoses and a downward trend in HIV incidence. However, more than 90% of the participants identified as White. On the basis of these successes, the local collaborative participating in the Rural Communities Opioid Response Program (RCORP) under the US Health Resources and Services Administration (HRSA) recommended securing and piloting an HRVM in metropolitan Bakersfield, the county seat of Kern County, to evaluate the acceptability and accessibility of HRVMs among Black and Latine residents.
Implementation
Project HOPE (Health and Overdose Prevention and Education) was a collaborative effort among California State University, Bakersfield (CSUB), Department of Social Work; Clinica Sierra Vista, a federally qualified health center; and Anthem Blue Cross Blue Shield (BCBS), the local managed health care plan in Bakersfield. Clinica Sierra Vista was awarded an HRSA RCORP Planning Grant in 2020 and collaborated with faculty from the CSUB Department of Social Work to conduct a gap analysis and develop a strategic plan to address opioid use disorder in rural communities. The CSUB Human Subjects Institutional Review Board approved this study (approval no. 24-125) on February 28, 2024.
Outcomes
Through participation in HRSA RCORP trainings, the Project HOPE team learned about and connected with an HRVM program in Plumas County, California, which was also sponsored by Anthem BCBS. Plumas County Public Health facilitated the introduction to Anthem BCBS, which later agreed to provide a donation toward the HRVM.
The Project HOPE team installed, stocked, and monitored 1 community-based outdoor HRVM in Bakersfield, which was accessible 24 hours per day, 7 days per week free of cost to registered users in the community (Figure 1). The HRVM was located outside a federally qualified health center embedded in a public housing apartment community operated by the Housing Authority of the County of Kern in a low-income, mixed-use neighborhood. Registered users entered their unique participant identification number to dispense kits containing naloxone, safer injection, wound care, sharps disposal, safer sex, hygiene, or menstrual hygiene supplies.

Outdoor harm reduction vending machine (HRVM) and security cage, Bakersfield, California, June 2023. The HRVM was installed by Project HOPE (Health and Overdose Prevention and Education), a collaborative effort among California State University, Bakersfield, Department of Social Work; Clinica Sierra Vista, a federally qualified health center; and Anthem Blue Cross Blue Shield, the local managed health care plan in Bakersfield.
The overall startup cost for the temperature-controlled outdoor HRVM was more than $20 000. Although the startup cost was steep, the annual costs were relatively sustainable and affordable at $2000 per year; however, this amount excluded unforeseen maintenance costs after the end of the 3-year warranty period. With the support of Anthem BCBS, Clinica Sierra Vista obtained a donation of approximately $11 000 to purchase the HRVM, which was stocked with harm reduction supply kits packaged in opaque bags ($100/1000 bags) to minimize barriers and stigma. To mitigate risks of damage and vandalism, Clinica Sierra Vista applied for a grant from the California Harm Reduction Supply Clearinghouse to cover the cost of a custom-built cage ($4800) for the HRVM. Clinica Sierra Vista also successfully applied for the Naloxone Distribution Project through the California Department of Health Care Services to provide naloxone at no cost. In addition, Clinica Sierra Vista funded the cost of facility improvements to establish an outdoor electrical and data source for the machine ($2500), the software subscription ($600/year), the printing of promotional materials ($500), and psychoeducational inserts for each kit ($530). The HRVM required wireless internet, an ethernet connection, or cellular service ($600/year) for use of the inventory-tracking technology software. Using funds allocated to Clinica Sierra Vista from the California Department of Public Health, the Project HOPE team ordered harm reduction supplies from the California Harm Reduction Supply Clearinghouse to assemble and maintain backstock of the harm reduction supply kits.
Because the HRVM was installed on property owned by the Housing Authority of the County of Kern, the Project HOPE team fostered a collaborative relationship to determine the contents of the harm reduction kits. Based on concerns from the community apartment tenants, safer injection kits did not contain syringes, and safer smoking kits were not included. Psychoeducational inserts in the safer injection kits directed participants to community-based resources, such as the local SSP and infectious disease clinic, to access sterile syringes. Despite concern about syringe litter, the Housing Authority of the County of Kern declined to install a sharps disposal kiosk. Therefore, the team included a personal, portable sharps disposal kit in the HRVM. The team also assured the Housing Authority of the County of Kern that the HRVM would benefit the community apartment tenants because these tenants would also be eligible to register and use the HRVM to access health and harm reduction supplies.
The Project HOPE team solicited feedback from physicians from Clinica Sierra Vista and peer support workers, as well as researchers and epidemiologists with experience in SSPs and harm reduction efforts, to determine the standard quantities of harm reduction supplies (Table). The team determined the following weekly use limits for each type of kit: once daily for the safer sex, safer injection, wound care, naloxone, and menstrual hygiene kits and once weekly for the hygiene and sharps disposal kits (Table). Furthermore, the team conducted a review of the evidence-based literature on harm reduction best practices and consulted with Clinica Sierra Vista physicians and case workers to develop the psychoeducational materials and relevant community-based referrals for each harm reduction kit (Figure 2).
Harm reduction supply kit inventories and costs for an outdoor harm reduction vending machine (HRVM), Bakersfield, California, June 2023 a
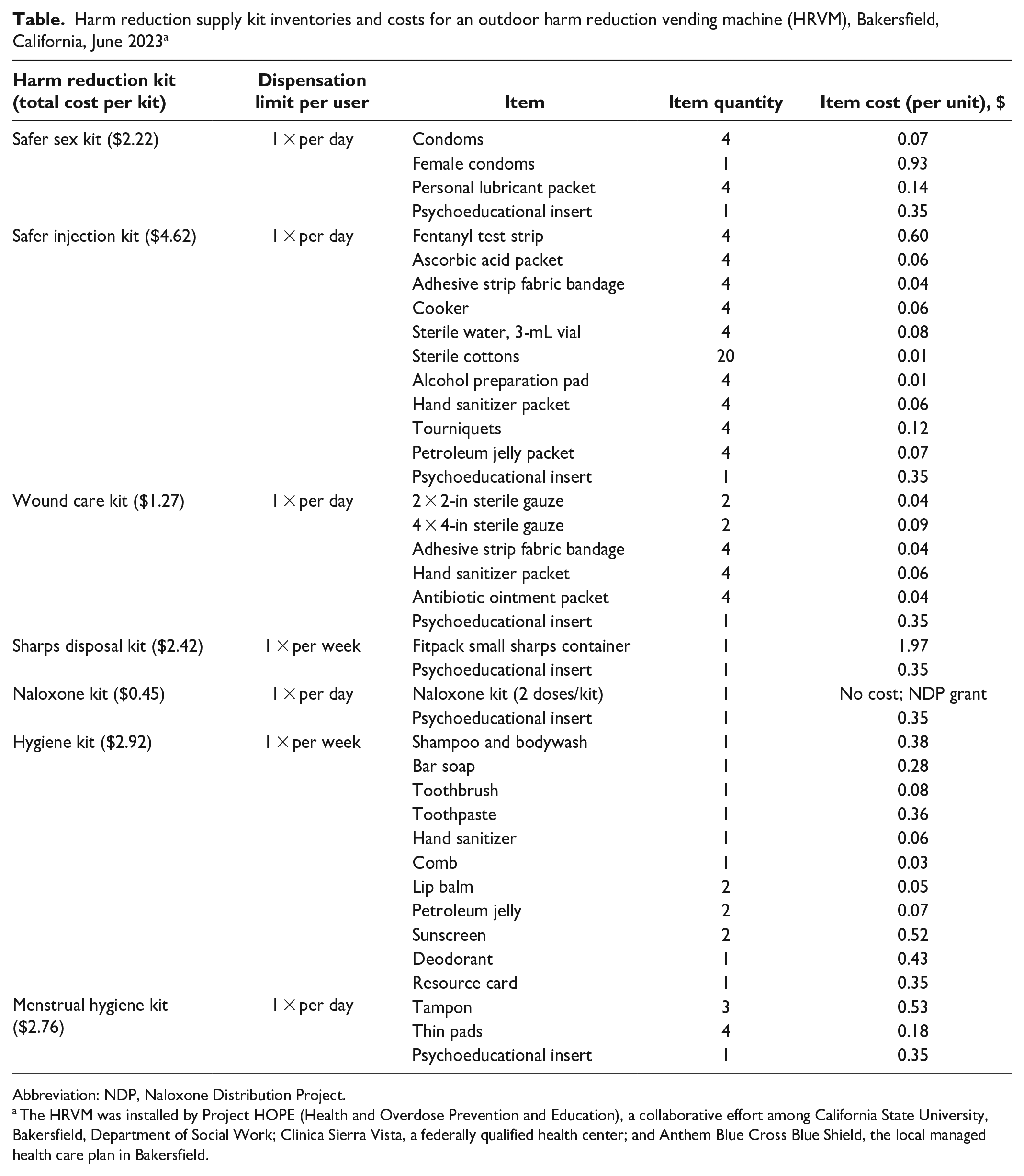
Abbreviation: NDP, Naloxone Distribution Project.
The HRVM was installed by Project HOPE (Health and Overdose Prevention and Education), a collaborative effort among California State University, Bakersfield, Department of Social Work; Clinica Sierra Vista, a federally qualified health center; and Anthem Blue Cross Blue Shield, the local managed health care plan in Bakersfield.
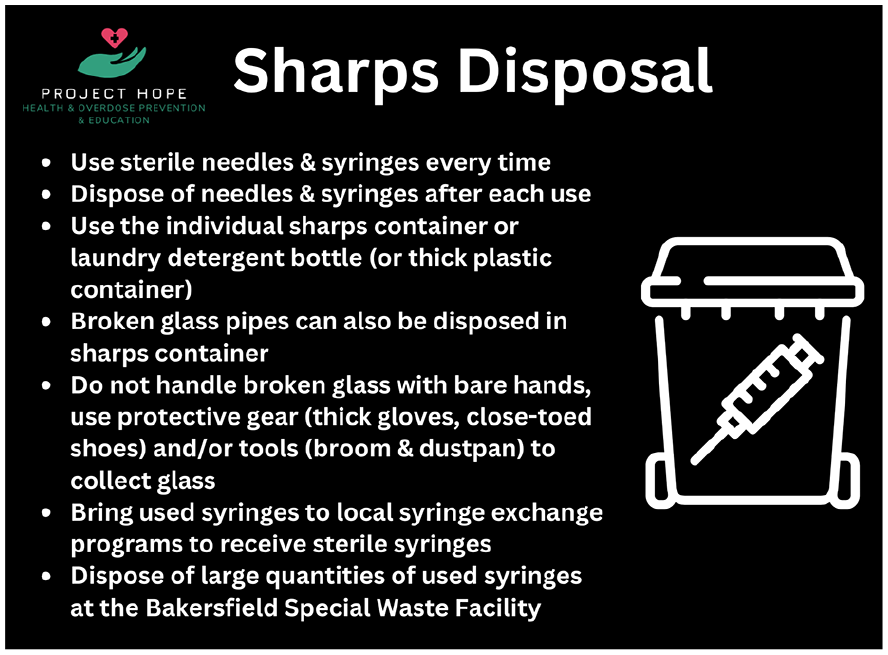
Sample psychoeducational card inserted in the sharps disposal kit of an outdoor harm reduction vending machine (HRVM), Bakersfield, California, June 2023. The HRVM was installed by Project HOPE (Health and Overdose Prevention and Education), a collaborative effort among California State University, Bakersfield, Department of Social Work; Clinica Sierra Vista, a federally qualified health center; and Anthem Blue Cross Blue Shield, the local managed health care plan in Bakersfield.
To finalize the preproduction process and begin fabrication of the HRVM, the Project HOPE team mailed samples of each type of harm reduction kit to the vending machine manufacturer (Intelligent Dispensing Solutions). The manufacturer weighed the kits and developed a planogram for the harm reduction kits based on the team’s input about desired product quantities. The team also submitted high-resolution image files to customize the branding for the HRVM, which included recognition of contributions from Project HOPE partners. After submission of sample kits and images, production time averaged about 4 to 6 months.
To prepare for the recruitment and registration of participants, the Project HOPE team developed a brief survey instrument through Qualtrics. In the pilot test, participants completed the survey in approximately 5 minutes. Although the registration survey did not request any identifying information, participants were required to create a unique 8-digit identification number. Participants also had the option of reporting information on sociodemographic characteristics, overdose history, and service needs on the registration survey.
Team members from the CSUB Department of Social Work provided ongoing support by recruiting and registering participants through the Qualtrics registration survey, entering the unique identification numbers of participants in the HRVM’s software, monitoring supply levels, assembling harm reduction kits, restocking the HRVM, and developing reports based on quantities dispensed and use rates of the harm reduction kits. Team members from Clinica Sierra Vista hosted the HRVM and the harm reduction supply room and managed the budget and orders from the California Harm Reduction Supply Clearinghouse. Through a community–academic partnership, Project HOPE developed a sustainable approach to maintaining and expanding community-based HRVMs in Kern County.
Project HOPE developed a comprehensive approach to enhancing community awareness and engagement with the HRVM. First, Project HOPE staff launched a media campaign with the local cable news channel and support from the Clinica Sierra Vista Communications and Community Outreach Department to publicize the HRVM on television and online. Second, staff partnered with the local substance use prevention coalition to conduct a social media campaign on Facebook, X, and Instagram to further publicize the HRVM. Third, faculty and student interns from the CSUB Department of Social Work set up and staffed tables in front of the clinic and apartment community where the HRVM was located to recruit and register participants 5 days per week between 8
Lessons Learned
To support continued project expansion, sustainability, and success of HRVM projects across the United States, we highlight the following lessons learned. First, we recommend approaching community-based organizations as collaborative partners and presenting HRVMs, their location, and the selection of harm reduction supply kits as responsive and reflective of the organization’s and local community’s values. By providing information about items stocked in other HRVMs and evidence-based information on the value of harm reduction supplies, we fostered open discussion, addressed any misconceptions or biases, and advocated for low-barrier access to harm reduction services. Although we were not able to stock our first machine with sterile syringes, safer smoking kits, pregnancy tests, or HIV test kits, we secured these kits for upcoming HRVM partnerships with the county behavioral health agency and the Urban Indian Health program. However, by accepting the current sociopolitical climate and concerns of our community partners, we successfully introduced HRVMs to Kern County, increased naloxone and harm reduction supply engagement and reengagement, and enhanced visibility and acceptability of this intervention throughout the community. As communities become more comfortable with harm reduction best practices, communities can advocate for the inclusion of safer smoking kits and sterile syringe kits in HRVMs to provide access to safer and preferred routes of administration and to decrease the spread of bloodborne pathogens and skin-related injury and infection.
Second, as the community demand for HRVMs increases, we need to increase funding streams and capacity to stock and monitor additional HRVMs. Given our initial success with Anthem BCBS, we recommend contacting the county’s local managed health care plans, pursuing intermural grants through higher education institutions, and identifying and submitting extramural grant applications to HRSA, the Substance Abuse and Mental Health Services Administration, and the National Institute on Drug Abuse. To ensure continued access to an adequate supply of harm reduction materials, we also advise contacting the county and state and public health agencies for support. Finally, through a community–academic partnership model, institutions of higher education are well-suited to provide the expertise and labor for participant recruitment and data collection and management.
Conclusion and Future Plans
After a period of intensive outreach, recruitment, and engagement, the Project HOPE team will shift its focus to data collection and analysis to examine rates of harm reduction supply use and dispensing and rates of overdose episodes. Over time, the team will accrue longitudinal data, which can be used to guide best practices for product limits, access models, and types of harm reduction supplies. The pilot data from the first HRVM will inform products for 2 future community-based HRVMs, which will be outside a behavioral health clinic and inside an Urban Indian Health program clinic. Initial data will also shape future recruitment and engagement strategies to ensure equitable scale-up of community-based HRVMs. With continued success of the HRVM located in a metropolitan area, the team intends to expand the intervention to rural communities to further increase equity and access and to decrease disproportionate overdose fatalities among Black and Latine communities.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Drug Abuse (grant no. 3R01DA055673-03S1).