
Abstract
Objectives:
Although studies have addressed food insecurity among veterans, few have focused on active-duty soldiers or on variables associated with the military occupational context. We examined the link between marginal food insecurity (defined as anxiety over food sufficiency or shortage of food in the house) among US soldiers and demographic, behavioral health, and unit-related factors.
Methods:
We analyzed survey data from 6343 active-duty soldiers using χ2 tests, generalized linear mixed-effect models, and adjusted odds ratios (AORs) to identify significant differences between soldiers categorized as marginally food insecure versus those who were not.
Results:
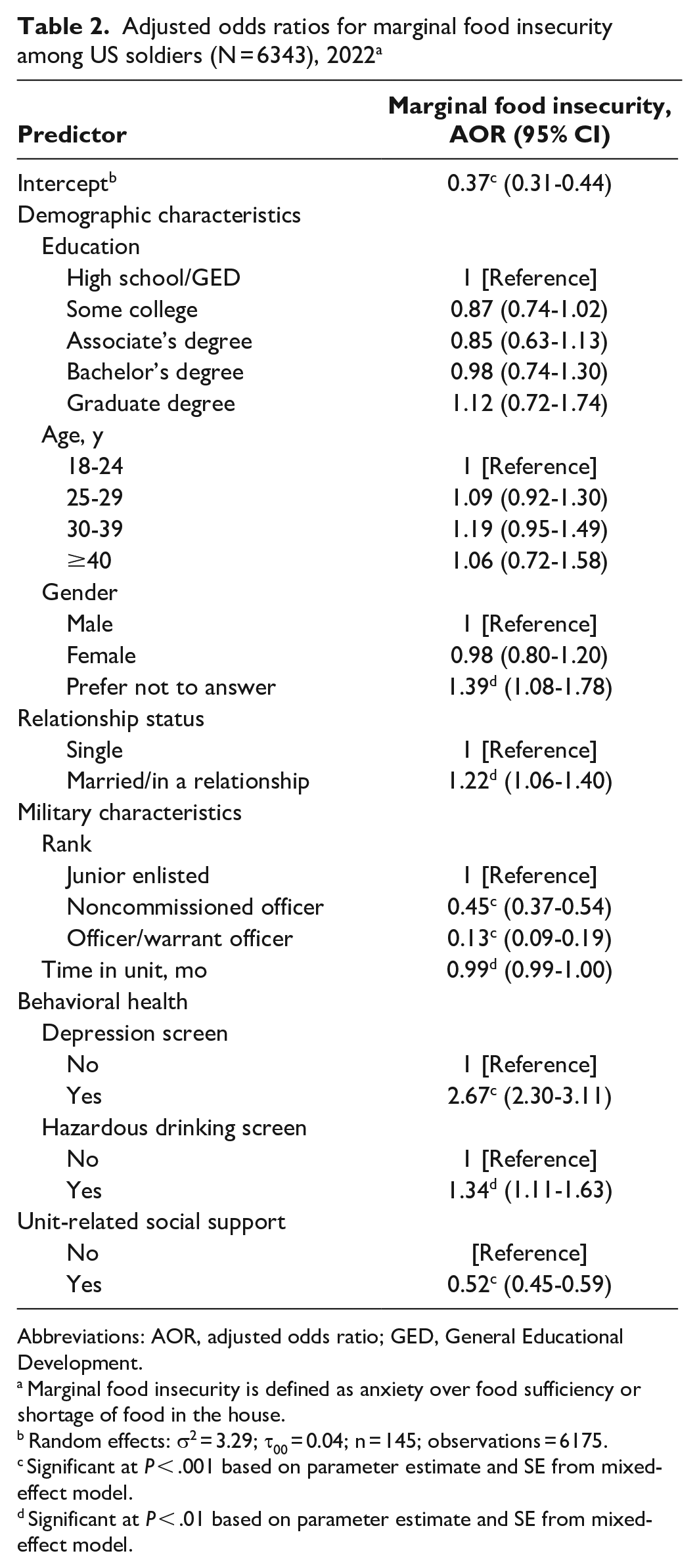
In a fully adjusted model taking unit into account, marginal food insecurity was associated with preferring not to report gender (vs reporting being male) (AOR = 1.39; 95% CI, 1.08-1.78), being married/in a relationship (vs being single) (AOR = 1.22; 95% CI, 1.06-1.40), junior enlisted rank (vs noncommissioned officer: AOR = 0.45; 95% CI, 0.37-0.54; and vs officer: AOR = 0.13; 95% CI, 0.09-0.19), less time in unit (vs more time) (AOR = 0.99; 95% CI, 0.99-1.00), screening positive for depression (vs not) (AOR = 2.67; 95% CI, 2.30-3.11), screening positive for hazardous drinking (vs not) (AOR = 1.34; 95% CI, 1.11-1.63), and lack of reported unit-related social support (vs support) (AOR = 0.52; 95% CI, 0.45-0.59).
Conclusions:
In this sample, more than 1 in 5 US soldiers reported marginal food insecurity. In addition to supporting households with financial and food assistance and targeting junior enlisted personnel, policy makers and leaders should prioritize soldiers who are married or in a relationship, who are new to their unit, and who screen positive for depression and hazardous drinking, and they should encourage units to take care of unit members who need support. Policy makers and leaders can use these study results to direct prevention and early intervention initiatives.
Food security is necessary for ensuring that individuals are healthy and fit, 1 yet approximately 12.8% of US households report food insecurity, 1 suggesting that it is a national concern. It is also a concern in the military community. In military veteran households, estimates of food insecurity range from 11.1% 2 to 24.0%, 3 and in the few studies of currently serving military personnel, approximately 1 in 4 (25.3%, 4 24.0%, 5 and 25.8% 6 ) may be at risk of food insecurity. Indeed, comparisons with civilian samples find that food insecurity is more than twice as common in the military than in the demographically equivalent civilian population. 4
The US Department of Agriculture defines food security as “access by all people at all times to enough food for an active, healthy life” and high food security as “no reported indications of food-access problems or limitations.” 7 In contrast, marginal food insecurity is defined as “anxiety over food sufficiency or shortage of food in the house. Little or no indication of changes in diets or food intake”; low food security is defined as “reports of reduced quality, variety, or desirability of diet. Little or no indication of reduced food intake”; and very low food security is defined as “reports of multiple indications of disrupted eating patterns and reduced food intake.” 7 The US Department of Agriculture categorizes marginal food insecurity as being food secure; however, research has documented the importance of using a broader lens when considering food insecurity, 8 including marginal, low, and very low food security. In addition, using this broader approach has become a standard of measurement for studies in the military context.9-11
From the military’s perspective, food insecurity is a readiness issue. Food insecurity is linked to lower levels of cognitive functioning 12 and higher levels of mental health difficulties than food security,13,14 and marginal food insecurity is associated with a greater likelihood of leaving military service 9 and intimate partner violence victimization than high food security is. 10 Thus, addressing marginal food insecurity can affect individuals, families, and the larger military organization.
That marginal food insecurity among military personnel is an issue is relatively surprising given that the military invests in supporting its personnel through stable income, housing, and health care, as well as programs designed to improve budgeting skills, mental health, and education. By identifying characteristics of active-duty military personnel who are at risk for marginal food insecurity, the military may be able to further refine outreach efforts. Previous efforts have identified demographic correlates of food insecurity among service members, but studies have not focused on variables that reflect military life, such as time in unit and unit-related social support, while adjusting for systematic differences across units.
The present study builds on previous research by considering risk factors for food insecurity that have been examined in civilian, veteran, and active-duty military samples, but the study pivots by focusing on occupational context. Compared with higher educational attainment, lower educational attainment has generally been a risk factor in some but not all studies of civilian 15 and veteran2,16 samples. 17 The association between lower educational attainment and marginal food insecurity has also been found in samples of active-duty personnel, 18 although, as in the case of civilian studies, results have been inconsistent. 11 In terms of age, studies have found that younger age (vs older age) is a risk factor for food insecurity in civilian 15 and veteran samples.16,19,20 In active-duty samples in which the age span is restricted, studies suggest that there is no significant effect by age.17,18
Sex has also been identified as a risk factor for food insecurity. Whereas studies of civilian 21 and veteran 22 samples have typically found females to be at greater risk for food insecurity than males are, at least 1 study found that male veterans may be at greater risk than female veterans are. 23 Among active-duty personnel, sex may not be a risk factor, 11 perhaps because individuals of the same rank receive equal pay regardless of their sex. Being married is regarded as a protective factor in studies with civilian 24 and veteran22,23 samples; however, in a study of active-duty personnel, being married was associated with a greater risk of food insecurity than being single was. 11 Instability in spousal employment—because of frequent relocations, lack of available jobs, and a dearth of affordable childcare11,25,26—may contribute to marital status as a risk factor for marginal food insecurity in active-duty personnel.
Studies of military personnel have found that junior rank is a risk factor for marginal food insecurity.14,27 Consistent with this finding, studies suggest that military pay does not meet costs of living 25 and that service members may be excluded from receiving Supplemental Nutrition Assistance Program (SNAP) benefits because of how eligibility is determined for military personnel.26,28 Just as studies of civilians 29 and veterans 22 show an inverse relationship between income and risk of food insecurity, rank may function in a similar role because it determines a service member’s basic pay.
Another military-specific risk factor for marginal food insecurity may be the requirement for military personnel to relocate approximately every 2.5 years. 30 Such transitions have been identified as a risk factor for the health of military personnel. 31 Relocating might also present risk because of financial costs associated with reestablishing a household. Thus, examining how long a service member has been in their unit (as a proxy for relocation recency) may offer insight into this potential risk factor.
Behavioral health difficulties have been identified as risk factors for food insecurity in civilian14,32 and veteran samples. 16 In active-duty samples, screening positive for depression, anxiety, suicidal ideation, 9 and posttraumatic stress 8 are risk factors for marginal food insecurity. Similarly, hazardous alcohol use is a risk factor for food insecurity in research with civilians 33 and veterans, 34 although less direct information is available about hazardous drinking and marginal food insecurity in active-duty samples.
Lack of social support has also been identified as a risk factor in civilian17,35,36 and veteran 22 samples. While at least 1 study found that overall social support is not associated with marginal food insecurity among active-duty military personnel, 11 being able to rely on unit members has been associated with positive adjustment in other military studies.37,38 Thus, lack of unit-related social support may also be a risk factor for marginal food insecurity in an occupational context such as the military.
The objective of the present study was to assess the relationship between marginal food insecurity and demographic characteristics, military characteristics, behavioral health, and unit-related social support in a sample of active-duty soldiers. Identifying variables that confer or mitigate risk for marginal food insecurity can be used to target screening and early intervention efforts across the military.
Methods
Study participants were active-duty US soldiers at a large Army post in the Midwest. Participants completed an anonymous electronic survey administered across the installation as part of a larger wellness assessment conducted in March 2022. 39 Distribution of the survey link was provided via QR code. The study was approved by the Human Subjects Protection Branch of the Walter Reed Army Institute of Research.
Measures
Marginal food insecurity
We measured marginal food insecurity with the 2-item Hunger Vital Sign, 40 which has been used in previous studies with the military.9,11 The items were “We worried whether our food would run out before we got money to buy more” and “The food we bought just didn’t last, and we didn’t have money to get more.” Participants rated both items on a 4-point scale: 1 = don’t know, 2 = never true, 3 = sometimes true, and 4 = often true. We classified those indicating “sometimes true” or “often true” on either or both items as screening positive for at least being marginally food insecure. Previous research found that these items were the 2 most endorsed on the 18-item Household Food Security Survey Module. 40 According to a validation study by Hager et al, 40 the 2-item screener and its scoring algorithm yield good sensitivity and specificity.
Correlates of Marginal Food Insecurity
Personal demographic characteristics included education, which was assessed with a single variable, “What is your highest level of civilian education?” (high school diploma/GED [General Educational Development], some college, associate’s degree, bachelor’s degree, graduate degree); age (18-24, 25-29, 30-39, ≥40 y); gender, which was assessed with a single item asking, “What is your gender?” (male, female, prefer not to answer); and relationship status, which was determined by asking a yes/no question, “Are you in a relationship/marriage? (eg, spouse, partner, fiancé, girlfriend/boyfriend)?”
For military characteristics, we categorized rank as junior enlisted (E1-E4), noncommissioned officer, or officer/warrant officer. We assessed time in unit by the question, “How many months have you been with your current unit?” with responses ranging from 0 to 99.
We measured screening positive for depression using the 9-item Patient Health Questionnaire. 41 Participants rated items (eg, “Little interest or pleasure in doing things”) on a 4-point Likert scale (1 = not at all to 4 = nearly every day) that was then summed (ranging from 9 to 36). We based screening positive on respondents marking depressed mood or anhedonia occurring “more than half the days” and 5 or more of the 9 items occurring at least “more than half the days.” 41 Hazardous drinking was measured by using the 3-item Alcohol Use Disorders Identification Test-Consumption. 42 Items (eg, “How often do you have a drink containing alcohol?”) were rated on a 5-point scale assessing frequency (0 = never to 4 = ≥4 times per week), volume (0 = no, 1, or 2 drinks; 4 = ≥10 drinks), and consuming ≥6 drinks on a single occasion (0 = never to 4 = daily/almost daily). Responses were summed (ranging from 0 to 12). Screening positive was calculated by using a cutoff score of ≥6 for males and ≥5 for females. 43
For unit-related social support, we developed a single item for this study in consultation with senior US Army leaders: “My unit takes care of soldiers who are facing personal challenges (eg, divorce, nagging injury, substance abuse).” Participants rated this item on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). We categorized scores of agree and strongly agree as indicating unit-related social support.
Analysis Plan
We computed frequencies for each variable and analyzed them in terms of marginal food insecurity status using Pearson χ2 test statistics and a t test for time in unit. We calculated adjusted odds ratios (AORs) for predicting marginal food insecurity for demographic characteristics, military characteristics, screening positive for behavioral health problems, and unit-related social support. We used generalized linear mixed-effect models with a binary link function and random intercept for unit membership to adjust individual-level estimates for potential unit-level effects. We conducted analyses using the lme4 package 44 in R version 4.2.2 (R Foundation for Statistical Computing).
Results
In all, 7831 (75.8%) participants provided their informed consent, and 1039 (13.3%) participants had missing data on both food insecurity variables. In total, 6792 participants provided data on food insecurity item(s), but because of missing data on other variables, the final dataset for analysis was 6343.
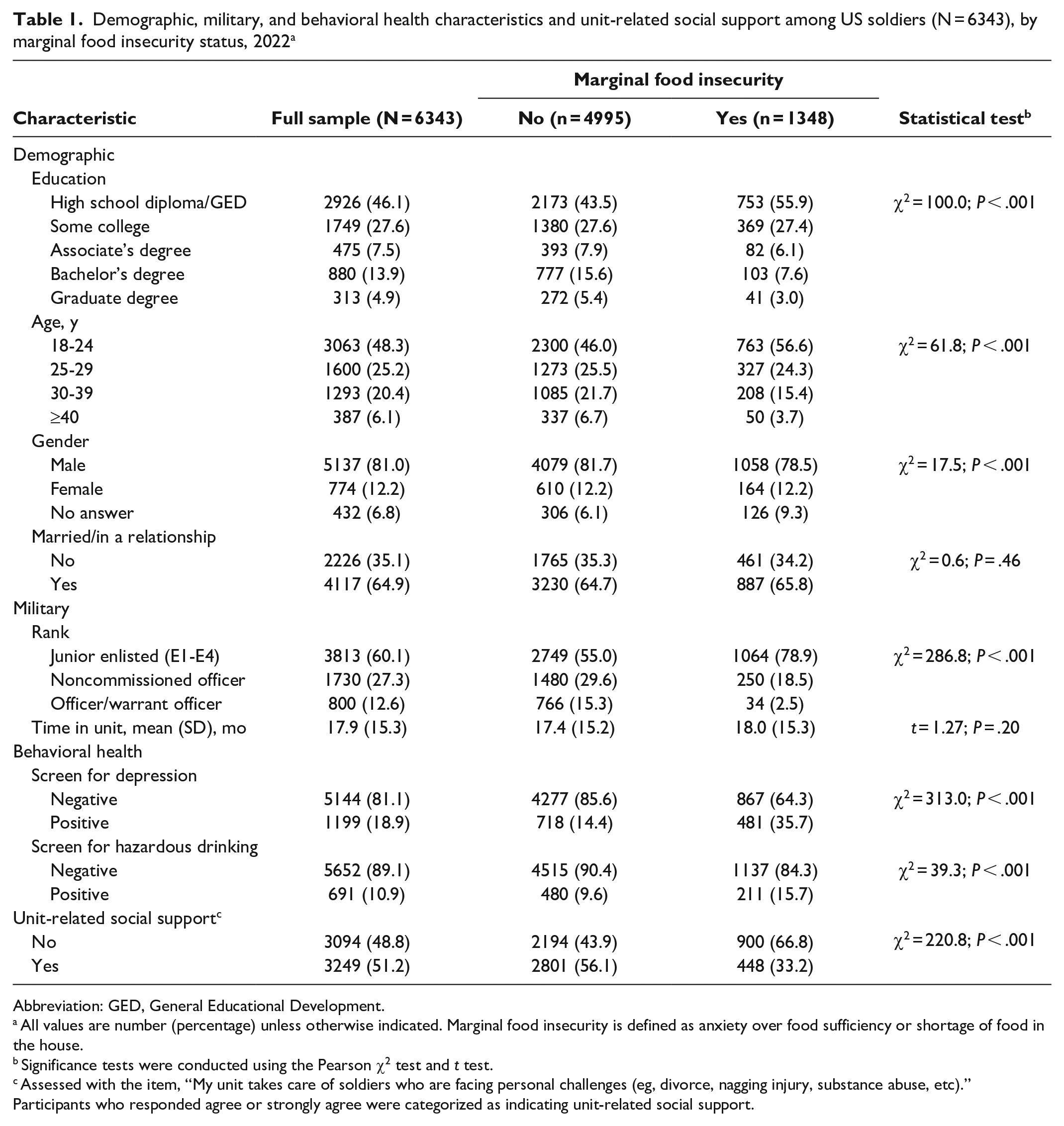
In this final dataset, 2926 (46.1%) had a high school diploma or GED, 3063 (48.3%) were aged 18 to 24 years, 5137 (81.0%) were male, and 4117 (64.9%) were married or in a relationship; 3813 (60.1%) were junior enlisted (E1-E4) and in their current unit for nearly 1.5 years (mean [SD] = 17.9 [15.3] months) (Table 1). A total of 1199 (18.9%) participants screened positive for depression, and 691 (10.9%) screened positive for hazardous drinking. More than half (n = 3249; 59.8%) agreed with the item assessing unit-related social support (Table 1).
Demographic, military, and behavioral health characteristics and unit-related social support among US soldiers (N = 6343), by marginal food insecurity status, 2022 a
Abbreviation: GED, General Educational Development.
All values are number (percentage) unless otherwise indicated. Marginal food insecurity is defined as anxiety over food sufficiency or shortage of food in the house.
Significance tests were conducted using the Pearson χ2 test and t test.
Assessed with the item, “My unit takes care of soldiers who are facing personal challenges (eg, divorce, nagging injury, substance abuse, etc).” Participants who responded agree or strongly agree were categorized as indicating unit-related social support.
Overall, 1348 (21.3%) respondents screened positive for marginal food insecurity. We found significant unadjusted differences in marginal food insecurity status by education (χ2 = 100.0; P < .001), age (χ2 = 61.8; P < .001), gender (χ2 = 17.5; P < .001), rank (χ2 = 286.8; P < .001), depression (χ2 = 313.0; P < .001), hazardous drinking (χ2 = 39.3; P < .001), and unit-related social support (χ2 = 220.8; P < .001; Table 1). The nature of the differences for each predictor is examined in the fully adjusted model.
In the fully adjusted model, gender, relationship status, rank, time in the unit, screening for depression and hazardous drinking, and unit-related social support were each independently associated with screening positive for marginal food insecurity (Table 2). Soldiers who preferred not to report their gender (vs reported being male), were married or in a relationship (vs being single), were junior in rank (vs a noncommissioned officer or officer rank), were in their unit for fewer months (vs more months), screened positive for depression and hazardous drinking (vs screened negative for these risk factors), and did not report unit-related social support (vs reported unit-related social support) were more likely to screen positive for marginal food insecurity.
Adjusted odds ratios for marginal food insecurity among US soldiers (N = 6343), 2022 a
Abbreviations: AOR, adjusted odds ratio; GED, General Educational Development.
Marginal food insecurity is defined as anxiety over food sufficiency or shortage of food in the house.
Random effects: σ2 = 3.29; τ00 = 0.04; n = 145; observations = 6175.
Significant at P < .001 based on parameter estimate and SE from mixed-effect model.
Significant at P < .01 based on parameter estimate and SE from mixed-effect model.
Discussion
In this large survey of US soldiers, more than 1 in 5 screened positive for marginal food insecurity. In fully adjusted models taking any systematic unit differences into account, marginal food insecurity was associated with preferring not to report gender, junior rank, shorter time in the unit, screening positive for depression, screening positive for hazardous drinking, and lack of unit-related social support. These findings highlight risk factors that are independently associated with marginal food insecurity.
Several findings were consistent with previous research in civilian and veteran samples, demonstrating a link between marginal food insecurity and behavioral health difficulties.12,16,32 Furthermore, our findings confirm results from studies of active-duty samples indicating a link between food insecurity and junior rank.11,27
Although age was significant in the unadjusted models, consistent with studies of civilians 15 and veterans,16,19,20 age was not associated with marginal food insecurity in the fully adjusted model. This nonsignificant relationship replicated results from previous studies with active-duty samples.11,18 Education was also significant in the unadjusted model, mirroring results from civilian studies, 15 but not associated with marginal food insecurity in the fully adjusted model; in the unadjusted model, some college (vs high school/GED) was associated with less food insecurity, but higher education levels were not.
One difference between civilian and military samples is that military samples typically include rank as a key characteristic, and rank is correlated with both education and age. Thus, to explore this relationship further, we conducted a post hoc analysis excluding rank. In these analyses, all levels of educational attainment (vs high school/GED) and the age categories of 30- to 39-year-olds and ≥40-year-olds (vs 18- to 24-year-olds) were significantly associated with less marginal food insecurity. Studies with military personnel may need to examine these relationships separately to avoid masking the role of demographic predictors. For researchers consolidating findings that include military samples, it might be important to consider that rank may suppress effects evident in nonmilitary samples.
Results also extend our understanding of other risk factors for marginal food insecurity. We found no significant difference in marginal food insecurity between male and female respondents; however, respondents who indicated “prefer not to answer” to the question on gender were at increased risk for marginal food insecurity compared with male respondents. In this survey, it is unclear what the 6.8% who endorsed “prefer not to answer” indicated: gender identity, interest in privacy, or something else. Nevertheless, the results suggest that for active-duty soldiers, male and female gender are not useful risk factors for marginal food insecurity screening.
Moreover, while previous research with civilians 24 and veterans22,23 found that marriage protects against marginal food insecurity, the current study confirmed results from previous studies of active-duty personnel, 11 identifying that being married (or in a relationship) was associated with increased risk of marginal food insecurity. Frequent relocations and spousal unemployment may contribute to this greater risk of marginal food insecurity.
Our study also extends previous findings about social support. Studies of civilians and veterans have found that social support is associated with less risk of food insecurity,17,22,35,36 and yet at least 1 study with active-duty personnel did not replicate this association. 11 In the present study, our measure of social support referenced the context of the military unit rather than social support in general. Perhaps soldiers in units where support is provided are better able to access resources, effectively countering the risk of marginal food insecurity. Future studies may want to consider different forms of unit-related social support and their relationship to marginal food insecurity.
Being in a unit for less time was also identified as a risk factor for marginal food insecurity. To our knowledge, this is the first study on marginal food insecurity to identify time in unit as a variable of interest. Even though the effect was modest, to the extent that time in unit is a proxy for military relocation, this finding points to moving as a potential risk factor for marginal food insecurity. Because the military routinely moves soldiers and their families, the military may want to leverage relocation as an opportunity to screen for marginal food insecurity and offer opportunities to supplement food during this period of transition.
Besides identifying families at risk for food insecurity, such screening can also proactively link them with food programs such as SNAP and the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC). While these are federally funded programs, they are administered by the state, and soldiers must reenroll almost every time they relocate. Moreover, soldiers may not be aware of or are misinformed about program eligibility requirements (Binny Chokshi, MD, MEd, Uniformed Services University of the Health Sciences, email communication, April 10, 2024). Outreach can also include facilitating access to the local food pantry 6 and providing information at food venues about items at the commissary covered by SNAP and WIC. Such communication strategies could be useful given that items qualifying for coverage vary by state.
Given that military leaders are key in establishing the culture within their units, 45 they should be educated on the prevalence of marginal food insecurity and prepared to proactively link service members with resources. Moreover, by encouraging unit social support, leaders may contribute to an environment better able to address the risk of marginal food insecurity.
Limitations
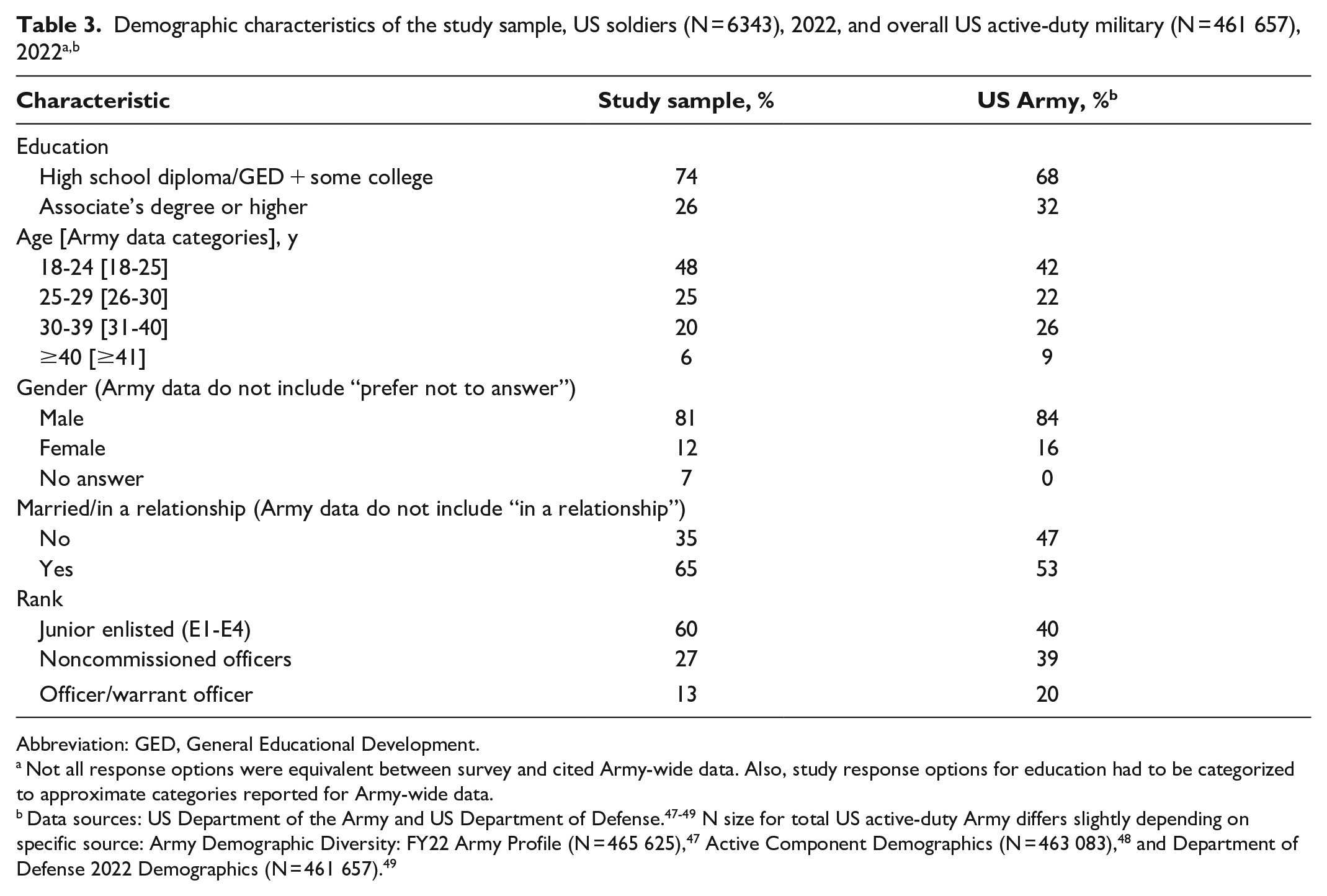
This study had several limitations. First, the survey was cross-sectional, precluding conclusions about causality. Second, relationship status did not distinguish between being married and being in a relationship, which could mask the effect on marginal food insecurity status of basic allowance for housing and other financial supports for married personnel. Third, we assessed gender (not sex), thus restricting the ability to detect differences by sex in the sample. Fourth, we did not assess items about physical health status, 20 children, 29 where the soldier lived (eg, on post),18,46 or the soldier’s race and ethnicity,11,29 each of which have been found to be risk factors for food insecurity in previous studies. Fifth, the variable assessing time in unit did not address whether a soldier had relocated geographically, thereby potentially underestimating the effect of relocation cost on soldiers. Some soldiers may be new to a unit in the same geographic location as their previous unit, whereas other soldiers may be new to a unit after having geographically relocated and incurring associated financial costs. Finally, the sample was not necessarily representative of the Army as a whole because it was taken from primarily operational units in a division located at a single Army installation; the study sample appeared to be younger and more junior ranking than the Army as a whole (Table 3).47-49
Abbreviation: GED, General Educational Development.
Not all response options were equivalent between survey and cited Army-wide data. Also, study response options for education had to be categorized to approximate categories reported for Army-wide data.
Data sources: US Department of the Army and US Department of Defense.47-49 N size for total US active-duty Army differs slightly depending on specific source: Army Demographic Diversity: FY22 Army Profile (N = 465 625), 47 Active Component Demographics (N = 463 083), 48 and Department of Defense 2022 Demographics (N = 461 657). 49
Conclusion
Future research would benefit from examining how to optimize screening for food insecurity and outreach during military relocation and as part of behavioral health evaluations. Future research would also benefit from understanding additional drivers of marginal food insecurity. For example, rank was a significant predictor of food insecurity, and income was likely part of the reason. Assessing the soldiers’ larger financial context may provide additional context, including the toll of financial pressures on household budgets, whether soldiers are prepared to manage their finances, decision-making about spending priorities, and adequacy of reasonably priced, healthy food options.
Food security is critical for everyone. For the military community, it is important to support soldier well-being and their ability to meet the unique demands of their occupation. Thus, it is important to identify who is at risk of marginal food insecurity, what unit-related variables are associated with this risk, and what might be helpful in mitigating this risk in this high-stakes environment.
Footnotes
Acknowledgements
The authors acknowledge the support of Yvonne Allard, MPH, Johns Hopkins University; Matthew Beymer, PhD, Defense Centers for Public Health; and Douglas Sharp, MS, Fires Battle Lab, in coordinating this study. This article was reviewed by the Walter Reed Army Institute of Research, which did not object to its presentation and/or publication. The opinions or assertions contained herein are the private views of the authors and are not to be construed as official or as reflecting the true views of the US Department of the Army, the US Department of Defense, the US Department of Education, or the Oak Ridge Institute for Science and Education.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the US Department of Defense (DOD) Research Participation Program administered by the Oak Ridge Institute for Science and Education through an interagency agreement between the US Department of Energy and the DOD. Funding was also provided by the Military Operational Medicine Research Program (Project #MO220112).