
Abstract
Knowledge surrounding perceived network support and alcohol consumption among active duty U.S. military personnel is limited, particularly among sexual minorities.
We sought to determine the correlates of hazardous alcohol consumption and whether perceived network support moderated the relationship between sexual orientation and Alcohol Use Identification Test (AUDIT-C) score.
The sample comprised cisgender men currently serving in the U.S. military (N = 292). Participants were recruited through respondent-driven sampling and completed an online survey. Logistic regression analysis evaluated associations between positive AUDIT-C with sociodemographic characteristics (including sexual orientation), military service, mental health, and perceived social network support. Interaction analysis assessed the moderating effect of perceived network support on sexual orientation and AUDIT-C.
Among study participants, 52.7% (154/292) had positive AUDIT-C, while 65.4% (191/292) self-identified as heterosexual/straight and 34.6% (101/292) identified as gay or bisexual. In adjusted analysis, positive AUDIT-C was associated with increased post-traumatic stress disorder symptomatology (adjusted odds ratio [adjOR] 1.03; 95% CI [1.00, 1.06]; p = .019) and high perceived network support (adjOR 1.85; 95% CI [1.04, 3.29]; p = .036), while mental health service utilization had reduced odds of positive AUDIT-C (adjOR 0.40; 95% CI [0.20, 0.78]; p = .007). In interaction analysis, high perceived network support was associated with increased odds of positive AUDIT-C among sexual minority men (adjOR 3.09; 95% CI [1.21, 7.93]; p = .019) but not heterosexual men (adjOR 1.38; 95% CI [0.68, 2.81]; p = .37).
Hazardous alcohol use was prevalent among all men in our sample. Perceived social network support may influence hazardous alcohol consumption, particularly among sexual minority servicemen. These findings suggest the potential role of tailored social network-based interventions to decrease hazardous alcohol use among military personnel.
Introduction
Excessive alcohol use is a significant public health threat and has been associated with negative health-related outcomes as well as legal and workplace ramifications (Mattiko et al., 2011; Taylor et al., 2007). Alcohol consumption is common among military servicemembers and largely integrated into military culture, for social purposes and to reward hard work (Poehlman et al., 2011; Woodruff, Hurtado, & Simon-Arndt, 2018). Combat exposure and deployments have been associated with increased alcohol consumption and the development of alcohol use disorders among military personnel (Ramchand et al., 2011; Russell et al., 2014). Alcohol may be used as a form of self-medication for underlying mental illness, such as depression or posttraumatic stress disorder (PTSD), or to cope with traumatic or stressful events (Bartone et al., 2017; Schumm & Chard, 2012).
Stressful military workplace dynamics may also contribute to excessive alcohol use (Cochran et al., 2013). A subpopulation particularly vulnerable to such stressors are servicemembers identifying as sexual minorities (SM). Prior military policies, such as Don’t Ask, Don’t Tell, Don’t Pursue (DADT), limited the ability for SM to openly serve, as sexual identity disclosure would result in a dishonorable discharge (U.S. Department of Defense, 2010). This resulted in an environment where SM personnel would serve in secrecy, oftentimes concealing their sexual orientation in both the workplace and social settings (Alford & Lee, 2016). While DADT was repealed in 2011, many SM servicemembers continue to experience discrimination, bias, and accompanying mental health symptomology (Alford & Lee, 2016; Van Gilder, 2017) - causing this subpopulation to be vulnerable to alcohol use disorders and poorer mental health outcomes (Blosnich et al., 2012, 2015; Coronges et al., 2013). Evidence demonstrates that psychological distress due to sexual orientation-based discrimination among civilian SM is associated with an increased risk of alcohol use (Dermody et al., 2014). While data surrounding alcohol use among SM in the military is limited, a recent study has demonstrated that psychological distress related to sexual orientation-based discrimination mediates alcohol use among SM servicemembers (Moody et al., 2020). Among veteran populations, anxiety surrounding concealment of sexual orientation during military service has been associated with elevated rates of PTSD, depression, and alcohol use among SM veterans compared with their heterosexual counterparts (Cochran et al., 2013).
Social networks represent an important form of social support and can be extremely influential in coping with stressful events (Kelley et al., 2017; Sayer et al., 2009), particularly among SM who often rely on social networks comprised of SM to cope with minority stress (Frost et al., 2016; Leahy & Chopik, 2020). Social networks can also reinforce negative behaviors. Studies have identified that group norms and attitudes can significantly influence behavior, particularly regarding alcohol use (Ahern et al., 2008; Knox et al., 2019). Research within civilian social networks in the United States demonstrated that both the proportion of individuals who drink and the number of drinks consumed by network members strongly correlate with one’s own alcohol use (Lau-Barraco et al., 2012; Neighbors et al., 2019). In addition to actual consumption, perceived network drinking behaviors and attitudes are important determinants of alcohol use (Neighbors et al., 2014). This observation may be particularly relevant for military personnel. Overestimation of perceived drinking behaviors and norms has been associated with increased alcohol consumption among veterans (Krieger et al., 2017; Pedersen et al., 2016) and active duty military servicemembers (Ames et al., 2007; Neighbors et al., 2014).
Excessive alcohol consumption within the military is of significant public health importance as it results in negative outcomes that may reduce the overall fitness of the armed forces (Meadows et al., 2018). A recent survey of U.S. military personnel demonstrated that 8.2% of servicemembers reported at least one serious consequence (e.g., arrest for driving under the influence, causing an automobile accident, having a physical altercation, intimate partner violence) and 6.1% reported work-related productivity loss due to alcohol use (Meadows et al., 2018). SM may be more vulnerable to such negative consequences given higher levels of alcohol use reported in this population, with 37.6% SM and transgender active duty service members reporting binge drinking in the past month compared with 29.3% of their non-SM and nontransgender counterparts (Meadows et al., 2018). While civilian social networks have an important impact on alcohol consumption, similar data involving the military is limited. Further, research involving SM military personnel has been hindered due to previous policies (e.g., DADT) that resulted in significant knowledge gaps surrounding health outcomes and experiences of this population (Goldbach & Castro, 2016). As a better understanding of factors associated with hazardous alcohol consumption is critical to the development of efficacious public health programs for harm reduction, this study seeks to evaluate the association of perceived network support, mental health, and sexual orientation with hazardous alcohol use among a cohort of active duty servicemen.
Materials and Methods
Participants and Procedures
Data for the present study come from the Military Acceptance Project, a Department of Defense-funded project designed to understand the acceptance and integration of active duty lesbian, gay, bisexual, and transgender (LGBT) military personnel. Respondent-driven sampling (RDS) was utilized to recruit LGBT and non-LGBT cohorts of active duty servicemembers. Initial seed participants were recruited through referrals from an expert advisory panel and military network contacts from primary investigators and study staff. When seed recruitment slowed, it was augmented by promotion through military-related social media and events, college campus organizations using flyers, and purchased advertising in diverse media outlets, including Facebook and the Military Times. Seeds were provided unique referral codes to share with peers, allow for tracking of recruitment chains, and ensure that no single group or platform yielded more than 20 eligible seeds at a time. All survey respondents were provided up to six unique referral codes to recruit additional participants. Recruitment lasted from August 2017 to March 2018.
Participants were eligible if they were at least 18 years old and active duty servicemembers of the U.S. Army, Navy, Marine Corps, or Air Force. Once screened eligible, participants were directed to a secure online survey using the Qualtrics platform (Qualtrics, Provo, UT, USA). A total of 991 individuals accessed the survey, of whom 709 were eligible and provided consent to participate. Of these, 165 individuals did not pass fraud detection measures or did not complete the survey, 220 individuals were excluded due to identifying as a woman or transgender, and three individuals were excluded due to missing RDS cluster data, resulting in a sample of 321 cisgender men. As the analysis was limited to cisgender men who responded to all variables of interest, 29 individuals were excluded due to missing data, resulting in an analytic sample of 292.
Women from the sample were not included in this analysis given gender differences in alcohol use and consequences (Nolen-Hoeksema, 2004). Studies suggest that the relative contribution of risk factors for alcohol use among men and women in the military may differ, such as gender differences observed with perceptions surrounding trauma, the prevalence of posttraumatic stress symptoms, the prevalence of depression, response to trauma, as well as the impact of combat exposures on PTSD and depressive symptoms (Irish et al., 2011; Skopp et al., 2011; Tanielian & Jaycox, 2008; Tolin & Foa, 2008). Due to concern that these gender-based differences in mental health and risk factors for alcohol use may confound the findings in this analysis, women were excluded from the present study.
Participants were provided a $25 e-gift card for completion of the survey (if off duty) and $10 e-gift card incentives for each referral who completed the survey. The study protocol was reviewed and approved by the Office of the Human Research Protection Program (OHRPP) at the University of California, Los Angeles (#18-000984) and the Human Subjects Protection Program (HSPP) at the University of Southern California (#UP-16-00070).
Measures
Sociodemographic Characteristics
Sex assigned at birth was reported using one item: “What sex were you assigned at birth, (i.e., what sex is on your birth certificate)?” (response options: male or female). Gender identity was assessed using a single question: “What is your gender identity?” (response options: male, female, transgender male/trans man, transgender female/trans woman, genderqueer/gender nonconforming, and gender identity not listed—please specify). As the analysis was limited to cisgender men, individuals who responded “male” to the sex assigned at birth and gender identity questions were included. Sexual orientation was measured using a single item: “What is your sexual identity?” (response options: heterosexual or straight, gay or lesbian, bisexual, and sexual orientation not listed here—please specify). Sexual orientation was recoded as a binary variable to assess those reporting a sexual minority identity (i.e., gay or bisexual) (reference group: heterosexual or straight).
Age was reported as a continuous variable. Racial and ethnic identity was assessed using a single question, with response options including Black or African American, Latino or Hispanic, White or Caucasian, Native American or Alaskan Native, Asian or Pacific Islander, multiracial, and other. Due to the small number of individuals reporting Native American/Alaskan Native, multiracial, or other, these responses were condensed into a single other category (reference group: White or Caucasian). Education was assessed using one item: “What is your highest level of education completed?” (response options: some high school, General Educational Development [GED], high school diploma, some college, associate degree, bachelor’s degree, master’s degree, and doctorate [PhD, MD, JD, etc.]). Due to the small number of individuals reporting doctoral degrees, education was recoded to GED/high school diploma (i.e., GED or high school diploma), some college/associate degree (i.e., some college or associate degree), bachelor’s degree, and graduate school (master’s degree or doctorate) (reference group: high school/GED).
Characteristics of Military Service
Respondents reported their military service branch (U.S. Air Force, U.S. Army, U.S. Marine Corps, or U.S. Navy) (reference group: U.S. Air Force). Current pay grade was assessed (responses ranged from E-1 to O-6) and listed by ascending order of rank based on prior work evaluating substance use among active duty personnel (Bray & Hourani, 2007). Rank/paygrade for service members was grouped based on ascending order of rank and officer status: E1–E3 (junior enlisted), E4–E6 (middle enlisted), E7–E9 (senior enlisted), O1–O3 (junior commissioned officers), and O4–O6 (senior commissioned officers).
Mental Health: Service Utilization and PTSD Symptomatology
To assess receipt of mental health services, respondents were asked whether they had received counseling or mental health services by a military behavioral health provider in the past year (reference group: no). PTSD was measured using the PTSD Checklist for DSM-5 (PCL-5). The PCL-5 consists of a 20 item self-report scale assessing PTSD symptomatology (Weathers et al., 2013), with a PCL-5 score of 33 or higher suggesting that the patient may benefit from PTSD treatment (Blevins et al., 2015; National Center for PTSD, n.d.). PCL-5 scores are reported as a continuous variable with higher PCL-5 scores consistent with higher levels of PTSD symptomatology.
Social Network Characteristics
A social network inventory was obtained, where participants provided information on up to five network members. Participants were asked to preferentially list social network members with military experience, followed by civilians if they did not have five network members who served. Average age of the respondent’s social network members was calculated from the continuously reported age of each member. Network density was calculated from the proportion of actual connections divided by the total possible number of connections between network members (Valente, 2010). Frequency of interaction with network members was assessed with a single item: “Who do you talk to or see at least once per week?”. As the number of nominated social network members varied by respondent, the frequency of interaction with network members was calculated as a proportion. To facilitate interpretation, responses were recoded as a binary variable based on whether the respondent interacted with the majority (i.e., greater than 50%) of network members at least once per week (reference category: less than 50%).
Perceived social network support was assessed with three questions: “Who do you talk to for mentorship or advice, such as about military or career issues?”; “Who can you count on to listen to you when you need to talk?”; and “Who do you go to when you need help or advice?”. Responses to these questions were condensed into one variable by calculating the proportion of network members identified as potential sources of support (proportions were calculated as the number of nominated social network members varied by respondent). To facilitate interpretation of the calculated proportions of network support, proportions were dichotomized into a binary variable based on whether the respondent reported the majority (i.e., greater than 50%) of their network members as a potential source of support (reference group: less than 50%).
Alcohol Use
Alcohol use was evaluated using the Alcohol Use Identification Test (AUDIT-C), a validated screening tool to identify hazardous drinking. The AUDIT-C consists of three questions where responses are measured on a 12-point scale. Scores of 4 or more in men are considered positive and are suggestive of hazardous drinking behaviors (Bush et al., 1998). As the AUDIT-C is used as a clinical screening tool designed to screen for hazardous drinking based on a positive or negative screening result, responses were dichotomized based on positive or negative AUDIT-C.
Data Analysis
We described the association of sexual orientation, military service characteristics, mental health service utilization, and perceived social network support with our outcome of interest—hazardous alcohol use, defined as positive AUDIT-C. Descriptive statistics (frequency, median, interquartile range) were used to describe the sample. Distributional differences between predictor variables with the outcome of interest were evaluated using χ2 analysis and Fisher’s exact tests (where appropriate) for categorical predictors and Kruskal–Wallis tests for nonparametric, continuous variables. Bivariate analyses estimated the association of participant and network characteristics with positive AUDIT-C. Demographic characteristics and predictor variables with an alpha <0.05, or that were important conceptually based on the literature, such as military branch (Schumm & Chard, 2012), rank/paygrade (Woodruff, Hurtado, Simon-Arndt, & Lawrenz, 2018), receipt of mental health services (Edlund et al., 2012), PTSD symptomatology (Debell et al., 2014), network density (Rinker et al., 2016), age of network members (Abikoye & Olley, 2012), social network size (Moody et al., 2020), talking to or seeing network members at least once weekly (Dorsey et al., 1999), were included in multivariable regression models. Logistic regression analysis was used to calculate unadjusted odds ratios (unadj. OR) of selected variables with positive AUDIT-C. Mixed-effects multivariable logistic regression with 10 integration points was used to calculate adjusted ORs, controlling for RDS cluster membership. To evaluate the association of network support with hazardous drinking among SM men, an additional mixed-effects model was created that included an interaction term of network support with sexual orientation. All multivariable regression models adjusted for age, race/ethnicity, education, sexual orientation, military branch, rank/paygrade, receipt of mental health services, PTSD, social network size, average age of network members, network density, interaction with network members at least weekly, and perceived network support. All analyses were conducted using Stata 15.1 (StataCorp, College Town, TX, USA).
Results
Sample Characteristics
Of the 292 men included in the analytic sample, 52.7% (n = 154) had positive AUDIT-C, and 47.3% (n = 138) had negative AUDIT-C scores. Most men self-identified as heterosexual/straight (65.4%; n = 191) with 34.6% (n = 101) identifying as a SM (gay or bisexual). Median age was 26 years (range 19–52). Most men identified their race/ethnicity as White/Caucasian (59.3%; n = 173/292), with 17.1% (n = 50) identifying as African American/Black, 13.0% (n = 38) Hispanic/Latino, 6.2% (n = 18) Asian or Pacific Islander, and 4.5% (n = 13) as multiracial/other. All four military branches were represented, with 35.6% (n = 104) serving in the U.S. Air Force, 36.3% (n = 106) in the Army, 12.7% (n = 37) in the Marine Corps, and 15.4% (n = 45) in the Navy. Most respondents were junior enlisted servicemen (28.4%; n = 83), middle enlisted servicemen (27.7%; n = 81), or junior commissioned officers (31.2%; n = 91). Descriptive statistics of the sample stratified by AUDIT-C score are listed in Table 1.
Descriptive Statistics and Bivariate Analysis of Selected Variables with Positive AUDIT-C Among Active Duty Cisgender Men (N = 292).

Results are presented as either median (interquartile range) or n (%); p-values <0.05 are in bold.
AUDIT-C = Alcohol Use Identification Test; GED = General Educational Development; PTSD = posttraumatic stress disorder.
Bivariate Analysis of Respondent and Network Characteristics
Individuals who identified their race/ethnicity as Asian or Pacific Islander had lower odds of positive AUDIT-C than White/Caucasian servicemen (unadj. OR 0.15; p = .004). Men serving in the U.S. Marine Corps had higher odds of hazardous drinking compared with those in the Air Force (unadj. OR 2.92; p = .011). Receipt of mental health services in the last year reduced the odds of hazardous alcohol use by almost half (unadj. OR 0.53; p = .029) compared with individuals who did not receive mental health care. Additionally, men who reported interacting with most network members at least weekly had higher odds of hazardous drinking (unadj. OR 1.91; p = .008) compared with those who did not. Results from the bivariate analysis are depicted in Table 2.
Mental Health, Military Characteristics, and Social Network Support Associated with Positive AUDIT-C Among Active Duty Cisgender Men (N = 292).
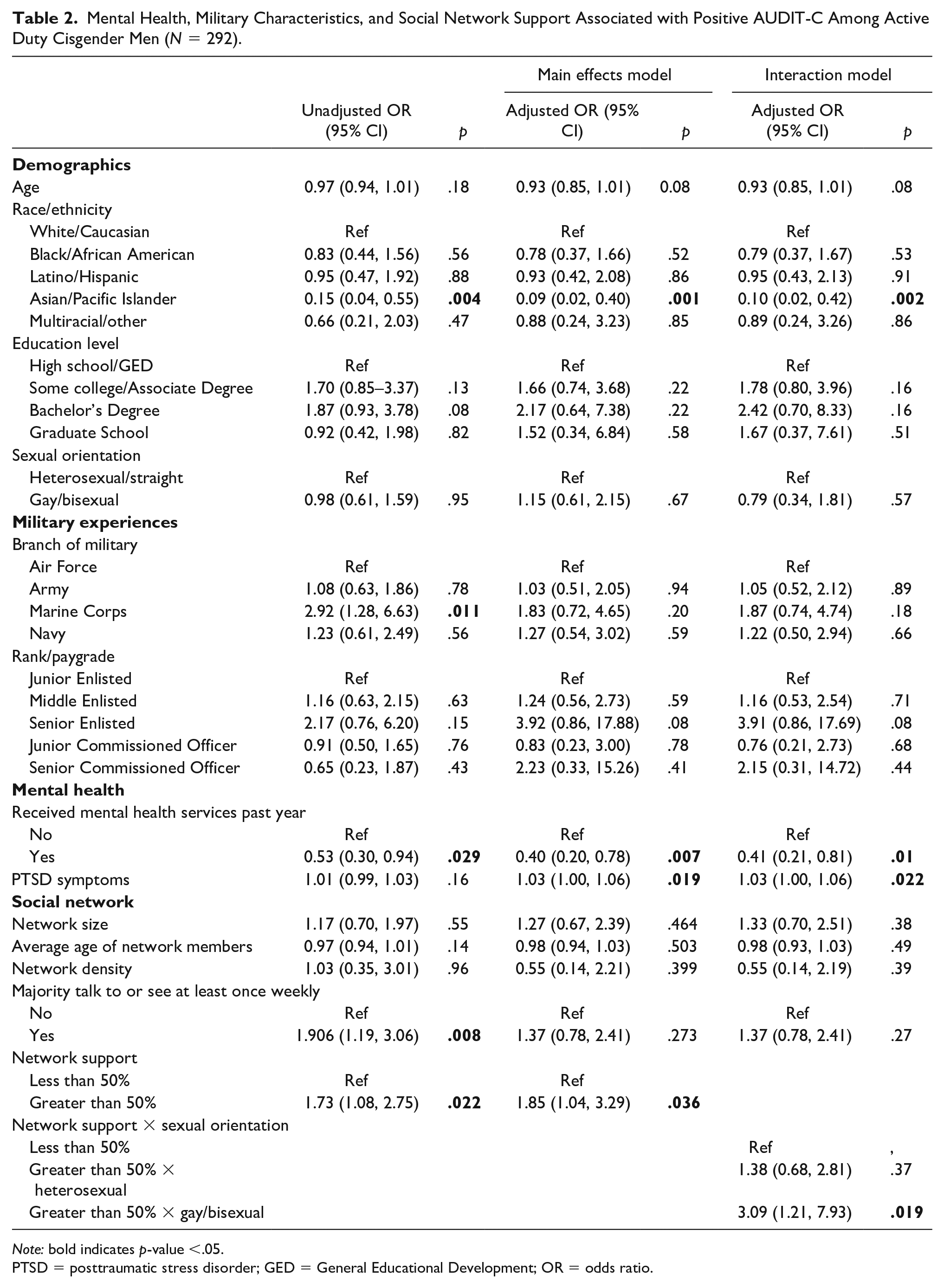
Note: bold indicates p-value <.05.
PTSD = posttraumatic stress disorder; GED = General Educational Development; OR = odds ratio.
Military Experiences and Mental Health
Respondents who received mental health services in the last year had lower odds of hazardous alcohol use than those who did not (adj. OR 0.40; p = .007). Men with worsening PTSD symptomatology had 3% higher odds of hazardous drinking for each unit increase in PCL-5 score in both our main effects (adj. OR 1.03; p = .019) and interaction (adj. OR 1.03; p = .022) models. While respondents who served in the Marine Corps had higher odds of positive hazardous drinking than those in the Air Force in our unadjusted analysis, military branch was not associated with hazardous drinking after adjusting for covariates in our model. Rank/paygrade was not associated with hazardous drinking in any of our models. Age, education, network size, network density, and average age of network members were not associated with hazardous alcohol use in our main effects or interaction models. Results from the main effects and interaction multivariable regression models are in Table 2.
Social Network Support
While significant in bivariate analysis, interacting with a majority of network members at least weekly was not associated with hazardous alcohol use in either multivariable model (adj. OR 1.37, p = .27; adj. OR 1.37, p = .27 for main effects and interaction, respectively) when compared with those with less frequent network interaction. In our main effects model, men who identified most network members as potential sources of support had almost twice higher odds of hazardous drinking compared with those with less supportive networks (adj. OR 1.85; p = .036). When evaluating the interaction of sexual orientation with social network support on hazardous alcohol use, SM men who perceived the majority of their network as supportive had over three times higher odds of hazardous drinking (adj. OR 3.09; p = .019) compared with heterosexual men who identified less than half of their network as supportive. Perceived support from most network members was not associated with hazardous drinking among men who identified as heterosexual/straight (adj. OR 1.38; p = .37) when compared with heterosexual men with less supportive networks.
Discussion
We sought to determine if perceived social network support, sexual orientation, and mental health experiences were associated with hazardous alcohol use in this analysis of U.S. active duty servicemen. Our findings demonstrate a positive relationship between hazardous alcohol use and perceived social network support among all men in our sample. When evaluating for interaction between sexual orientation and network support, our study demonstrates that higher perceived support was associated with hazardous alcohol use among SM men, and yet, no association was observed among heterosexual men with our outcome of interest.
Influence of Military Culture and Social Networks
High rates of hazardous alcohol use were reported in this sample with over half (52.7%) having a positive AUDIT-C. It is well documented that military personnel experience higher rates of alcohol consumption compared with their civilian counterparts, with an estimated 33%–35% of active duty servicemembers having a positive AUDIT score compared with 6% of civilian adults estimated to have an alcohol use disorder (Bray et al., 2013; Mattiko et al., 2011; Meadows et al., 2018; Substance Abuse and Mental Health Administration (SAMHSA), 2017). High rates of alcohol consumption within the military are partially attributed to a culture permissive toward alcohol as well as norms ingrained in military traditions (Jones & Fear, 2011). Alcohol may be used as a method to break down barriers, facilitate bonding, and improve unit cohesion, particularly after a stressful training exercise or deployment (Ames & Cunradi, 2004; Breslau et al., 2016; Fear et al., 2007). Alcohol consumption is additionally used to cope with personal or occupational-related stressors, given accommodating attitudes toward drinking as a form of stress reduction within the armed forces (Bravo et al., 2017; Cerdá et al., 2014; Foran et al., 2011). These cultural norms and attitudes may also influence perceptions regarding alcohol consumption within military social networks.
Our findings demonstrate a positive relationship between perceived network support and hazardous alcohol use. This observation may initially seem counterintuitive as increased levels of social support have been associated with reduced alcohol use, particularly among individuals with PTSD and depressive symptoms (Fuehrlein et al., 2018; Kelley et al., 2017). As respondents preferentially listed social network members with military experience, these findings may reflect the diffusion of military cultural practices into network behaviors. This finding is consistent with research demonstrating that maintaining largely military social networks is associated with increased alcohol consumption among veterans (Hatch et al., 2013). Within these networks, alcohol may be consumed as a social activity: a form of bonding between peers (Ames et al., 2009). Individuals may have key network members from whom they receive support while consuming alcohol (Lau-Barraco et al., 2012; Lau-Barraco & Linden, 2014).
Perceived Network Support Among Sexual Minority Men
SM men with high perceived network support had increased odds of hazardous alcohol use, and yet, no association was observed among heterosexual servicemen in the interaction analysis. This may result from existing military drinking attitudes that are reinforced by network dynamics unique to sexual minorities. Social networks and peer norms have an important influence on the behaviors of SM men, particularly as alcohol consumption in this population frequently occurs in social settings and within groups (Amirkhanian, 2014; Halkitis et al., 2011). Studies have demonstrated that SM men who have network members and/or close peers who drink are more likely to consume alcohol themselves (Baiocco et al., 2010; Hatzenbuehler et al., 2015). These dynamics influence binge drinking as well, with one study demonstrating that a strong predictor of binge drinking among civilian SM men was having a social network member who engaged in binge drinking (Holloway, 2015). In addition to internal dynamics within SM networks shaping individual behavior, external influences on how these networks are formed and maintained likely have an impact, as well.
Historical norms and attitudes toward SM in the military have led to significant marginalization of this group (Alford & Lee, 2016). Exclusionary policies, such as DADT, may have led SM men to have smaller, tighter-knit social networks compared with their heterosexual counterparts (Ramirez & Bloeser, 2018). While DADT was repealed, sexual minorities still face many barriers toward full equity and inclusion within the military and continue to be victims of discrimination and bias (Alford & Lee, 2016; Goldbach & Castro, 2016). Stress from these experiences may result in increased reliance on these tighter-knit networks as a form of social support (Meyer, 2015). If permissive attitudes toward drinking are prevalent within these networks, increased alcohol consumption may result, particularly as the density and intensity of alcohol use among network members has a strong influence on individual drinking behaviors and norms surrounding alcohol consumption (DeMartini et al., 2013).
PTSD and Receipt of Mental Health Services
In adjusted analysis, having PTSD was associated with hazardous drinking which is expected given the high comorbidity of PTSD and alcohol use disorders (Allen et al., 2016; Debell et al., 2014), especially among military members with a history of deployments and combat-related traumas (Dworkin et al., 2018; Ramchand et al., 2011). Among these servicemembers, alcohol consumption is used as a way to regulate emotions (Cooper et al., 1995; Lehavot et al., 2014; Miller et al., 2017), particularly among those who rely upon avoidance coping strategies (Bartone et al., 2017). Consuming alcohol to moderate negative emotions likely explains our finding that receipt of mental health care was negatively associated with hazardous drinking. Additionally, receiving care from a mental health provider may lead to the identification of alcohol use disorders, resulting in linkage to substance use counseling or treatment (Dworkin et al., 2018). Conversely, individuals with high levels of psychotherapy stigma may not seek mental health services resulting in increased drinking behaviors to self-regulate negative emotions (Miller et al., 2017; van den Berk-Clark et al., 2016).
Limitations
As with any study, ours comes with limitations. Data were collected online and via self-report, and therefore, responses may be affected by recall and social desirability bias. However, we utilized attention control measures and assured participants that all responses were confidential throughout the survey to reduce social desirability bias. As complete case analysis was used for our analysis, participants with missing data were excluded, which may have introduced bias. However, we believe that potential bias introduced by using complete case analysis is small (n = 29 participants) and unlikely to significantly influence our results. As respondents were asked to preferentially list network members with military experience, bias could have been introduced as influential members may not have been captured. For example, participants may have had key network members outside of the military who were stronger forms of support than those listed. However, this also represents a potential strength as we evaluated predominantly military social networks of active duty servicemembers, given the paucity of data on this topic. While RDS is a useful sampling tool for difficult to reach populations, our sample may not be generalizable to the entire population of active duty military personnel, particularly as participants were recruited from within respondents’ social networks potentially resulting in selection bias. Finally, given the cross-sectional nature of our data, we are unable to make causal inferences with our analysis.
Conclusions
As military personnel are disproportionately affected by alcohol use disorders, research into factors associated with hazardous alcohol consumption is critical to improve the health and well-being of this population. Our study demonstrates that hazardous drinking is associated with increased perceived network support, particularly among SM men, which have important implications for future program development. Specifically, our findings highlight the potential role of network-based interventions directed at changing attitudes and norms surrounding alcohol use by promoting moderation of drinking behaviors within networks (Fuehrlein et al., 2018; Reid et al., 2015; Valente et al., 2007) and facilitating larger cultural changes regarding alcohol consumption within the military (Ames et al., 2007; Neighbors et al., 2014). Further, network dynamics unique to sexual minorities appear to influence alcohol use within this group. Minority stressors resulting from pursuing a career in a traditionally heteronormative workplace may contribute to these dynamics, suggesting the need for continued changes toward diversity and inclusion within the military (Alford & Lee, 2016). Finally, our study demonstrates that PTSD symptomatology is positively associated with hazardous alcohol use, while receipt of mental health services is protective. This highlights the need for improved screening, identification, and linkage to care of servicemembers with PTSD symptomatology and/or signs concerning alcohol use disorders (Calhoun et al., 2016).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Department of Defense under Grant [W81XWH-151-0700] to CAC, JTG, and IWH. CSB was supported by the National Institute of Mental Health under Grant [T32MH080634].