
Abstract
Objectives:
Integrating vaccination services with other essential health services could increase vaccination rates among socially marginalized populations. We examined the associations between colocation of vaccines at syringe service programs and COVID-19 vaccination status among people who inject drugs and people experiencing houselessness.
Methods:
This study included 1891 participants aged ≥18 years at 9 sites in Oregon from July 2021 through March 2022. Participants self-reported whether they had ever received ≥1 dose of a COVID-19 vaccine. We calculated site-level COVID-19 vaccine availability and overall vaccination rates. We compared site-level vaccination rates and analyzed the association between vaccine availability and vaccination status.
Results:
We found no significant difference in vaccination rates between sites that did and did not offer COVID-19 vaccines (t7 = −0.33; P = .75). We also found no significant association between vaccine availability and vaccination status. However, the odds of having received a COVID-19 vaccine were 2.79 times higher for each additional site visit during which COVID-19 vaccines were available (odds ratio [OR] = 2.79; 95% CI, 2.18-3.58; P < .001). The association between vaccine availability and vaccine status was not moderated by participant age (OR = 1.03; 95% CI, 0.99-1.07; P = .13) or housing instability (OR = 0.59; 95% CI, 0.13-2.60; P = .48).
Conclusions:
Colocating COVID-19 vaccines at syringe service programs was only positively associated with vaccination status if vaccines were offered frequently on-site. Future work should examine whether the frequency of offering vaccination services increases willingness to engage in vaccination and examine trust and convenience as potential mechanisms.
Socially marginalized populations including people who inject drugs (PWID) and people experiencing houselessness (PEH) are at increased risk for several infectious diseases for which vaccines are available, including COVID-19.1-5 PWID and PEH also had a higher risk of COVID-19 morbidity and mortality than the general population during the pandemic.1,6-9 Strategic efforts to provide COVID-19 vaccines to these populations appeared to be successful, but lack of intentional engagement with PWID and PEH may have produced disparities in vaccination rates.10-12 Furthermore, vaccination rates varied in these populations based on individual circumstances and characteristics. Older age is associated with higher vaccination intention compared with younger age among general populations globally. 13 Among PWID and PEH, older age and housing stability are associated with higher vaccination rates compared with younger age and housing instability.10,11,14 It has been theorized that colocating vaccination services at sites that offer health and social services attended by socially marginalized populations may improve vaccination rates.15,16
Syringe service programs (SSPs) provide PWID with safe access to and disposal of syringes and injection equipment, and many SSPs offer other harm-reduction services to reduce the incidence of overdose and the spread of infectious diseases. 17 However, SSPs are unable to offer all of the health services PWID need because of personnel and budgetary constraints,18,19 and only 33% to 40% reported offering COVID-19 vaccination services on-site at the peak of the pandemic in 2021.20,21 Among SSPs that offered COVID-19 vaccines, PWID qualitatively shared that the convenience of colocation of vaccination services at SSPs was a reason for vaccination, 11 although quantitative evidence that supports this assertion is limited. 22
Integrating vaccination services with other essential health services is a top strategic priority in the World Health Organization’s Immunization Agenda 2030. 23 Generally, colocation of services aims to remove structural and physical barriers to care by offering multiple services in places frequented by socially marginalized populations.24,25 We identified several reports of COVID-19 vaccines colocated with other services (eg, SSPs, schools, community service centers for PEH, some hospital services) to reach socially marginalized populations.15,22,26-28 However, only 1 study measured the effect of colocation on vaccination status. While this study detected a 20% increase in vaccine uptake, it was specific to pregnant people in a hospital setting in England. 27 Current evidence on service colocation to improve health outcomes among PWID and PEH is largely based on qualitative and descriptive research studies.22,24,28-30 However, 1 study found that 85% of PWID who received services from SSPs that also hosted COVID-19 vaccination clinics received ≥1 vaccine dose. 22 A need exists for quantitative analyses to better understand the utility of colocation of vaccination services at locations serving PWID and PEH. Understanding the effect of colocation of COVID-19 vaccination services on vaccination status among PWID and PEH may provide insights on the use of this strategy to increase uptake of future vaccines among socially marginalized populations.
The objective of the current study was to evaluate whether colocation of COVID-19 vaccination services at SSPs and community service centers was positively associated with vaccination status among PWID and PEH. We addressed 2 research questions. The first question was, “Is colocation of COVID-19 vaccine availability at SSPs and community service centers associated with self-reported vaccination status among PWID and PEH?” We hypothesized that more participants accessing services at SSPs that offered vaccines would self-report having received a COVID-19 vaccine than those accessing services at sites that never offered vaccines. We also hypothesized that same-day colocation of COVID-19 vaccine availability would be positively associated with self-reported vaccination status; in other words, more participants would self-report being vaccinated on days that COVID-19 vaccines were offered on-site than on days when COVID-19 vaccines were not offered on-site. Lastly, we hypothesized that the number of times participants visited a site when COVID-19 vaccination services were available would be positively associated with self-reported vaccination status. The second question was, “Is the association between colocation of services and vaccination status moderated by age or housing status?” We hypothesized that younger participants and PEH would experience the most benefit from COVID-19 vaccine availability, because these groups were the least likely to seek out COVID-19 vaccines during the pandemic.10-12
Methods
Study Design, Setting, and Participants
This study was part of a larger effort funded by the National Institutes of Health Rapid Acceleration of Diagnostics for Underserved Populations (RADx-UP) initiative. The University of Oregon partnered with HIV Alliance, an Oregon-based nonprofit organization that provides harm-reduction services for PWID, to implement a SARS-CoV-2 testing program at 9 SSPs across Oregon, representing 4 counties (2 rural, 2 small urban). HIV Alliance syringe exchange services occurred weekly at each location. During the pandemic, some of these SSPs were able to host state and local public health medical professionals who offered COVID-19 vaccination services during regular hours of operation in addition to their other harm-reduction services. The frequency with which vaccination services were offered at each SSP varied, and some sites did not offer vaccines at all during the study period.
As part of the SARS-COV-2 testing program, a pop-up testing tent was regularly present at all SSPs. Individuals received a $10 gift card for filling out an intake form (responses recorded by HIV Alliance staff on a Qualtrics form on a computer), engaging in SARS-CoV-2 testing, and consenting to share their information with our research team. Being willing to share information with our research team (ie, testing engagement, intake information, and results after completing routine testing) was the condition for receiving the gift card; for this reason, <5 clients, to our knowledge, opted out of sharing their information with the research team. The intake information shared with the study team included identifiable information (including first and last names and telephone number), demographic characteristics (including gender, race and ethnicity, age, housing stability, employment status, and education), the name of the SSP site that the participant was currently visiting to receive SARS-CoV-2 testing services, and their COVID-19 vaccination status (response options were yes, no, don’t know, or prefer not to answer). HIV Alliance staff administered the intake form after they received training from the study team on human subjects research. The study team retrieved participant responses in collaboration with the University of Oregon SARS-CoV-2 testing laboratory. Because 2 SSPs were colocated at community service centers for PEH, PEH at these centers were also invited to participate in the testing program, and data from these individuals were included in this study.
This study included 1891 participants aged ≥18 years from 9 SSP sites who consented to participate when they used the SARS-CoV-2 testing program from July 2021 through March 2022, resulting in a dataset of 3866 unique combinations of participant, site, and date observations. A total of 991 participants (52.4%) self-identified as SSP participants, while the remainder were on-site receiving services for unhoused community members. The University of Oregon Institutional Review Board reviewed and approved this project.
Measures
COVID-19 vaccine availability
For the site-level analysis, we computed a site-level COVID-19 vaccine availability variable to determine whether or not each site had ever offered COVID-19 vaccines. For the individual-level analyses, we coded on-site COVID-19 vaccine availability as a dichotomous variable, characterizing whether COVID-19 vaccines were available at each participant’s visit to that site. We also calculated the total number of times COVID-19 vaccines were available to participants on-site during their site visits (including their previous and current visits). We derived these site-level data from a summary list maintained by our research team, triangulated by our community partner on a regular basis, and rereviewed the data for accuracy before analyses.
COVID-19 vaccination status
Each time participants were tested for SARS-CoV-2, they reported whether they had ever received ≥1 dose of a COVID-19 vaccine on the intake form by answering the question, “Have you received a COVID-19 vaccine?” (1 = yes, 0 = no).
Demographic covariates and moderators
We included demographic variables as covariates and moderators. Demographic variables included age (continuous variable), housing stability (1 = transitional housing, staying in shelter, or experiencing homelessness; 0 = housed), employment status (1 = unemployed, 0 = employed), and educational background (1 = high school diploma or GED, 0 = no high school diploma or GED). We did not include race or ethnicity as covariates because they were not associated with vaccine uptake in any prior analyses with the current sample.10,11
Analysis
We conducted all analyses in R version 4.2.2 (R Core Team). We conducted 3 analyses: (1) a Welch’s t test comparing site-level COVID-19 vaccination rates (based on vaccination status) among SARS-CoV-2-testing participants at sites that had COVID-19 vaccines available and sites that did not have COVID-19 vaccines available; (2) a mixed-effects logistic regression analysis examining self-reported vaccination status as a function of COVID-19 vaccine same-day availability on-site, adjusting for age, housing stability, employment status, and educational background; and (3) a mixed-effects logistic regression analysis examining self-reported vaccination status as a function of the number of times an individual visited a site when a COVID-19 vaccine was also available (previous to and including the day that participants received SARS-CoV-2 testing services), adjusting for age, housing stability, employment status, and educational background.
To test whether associations between vaccine availability and vaccination status were moderated by age and housing stability, we included these interaction terms in our logistic regression models. We analyzed mixed-effects logistic regression models using the lme4 package version 1.1-29 (R Core Team). 31 We included random effects to account for clustering within participants and sites. Because our primary outcome—vaccination status—requires participants to directly report their vaccination status and is unlikely to be affected by missing data, imputation methods may introduce potential bias or unnecessary assumptions. Thus, we used a complete case approach for all analyses, resulting in a robust analytical dataset of 2871 of the overall 3866 unique combinations of participant, site, and date observations for all regression analyses. 32
Results
Participant age ranged from 18 to 87 years, with a mean (SD) of 46.0 (12.9) years; of the 1891 participants, most reported unstable housing (78.3%; n = 1481) and were unemployed (70.9%; n = 1341) (Table 1). Only 46.7% of participants (n = 883) reported ever receiving a COVID-19 vaccine and 34.6% (n = 655) ever had access to a COVID-19 vaccine during a site visit. The number of visits to our SARS-CoV-2 testing program at SSPs for each participant ranged from 1 to 47, with a mean (SD) of 2.0 (2.9) visits per person. The number of participants within sites ranged from 69 to 588, with a mean (SD) of 222.9 (207.1) participants, and only 90 participants (4.8%) visited >1 site during the study period.
Demographic characteristics and study variables among people who inject drugs and people experiencing houselessness in Oregon, July 2021 through March 2022 (n = 1891) a
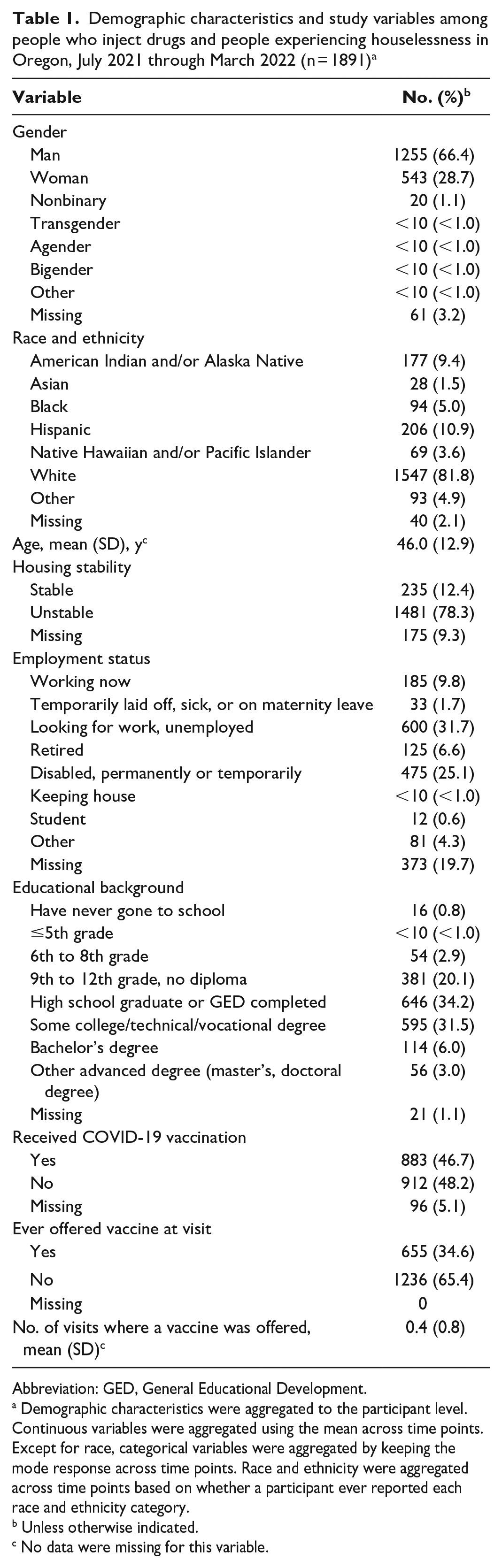
Abbreviation: GED, General Educational Development.
Demographic characteristics were aggregated to the participant level. Continuous variables were aggregated using the mean across time points. Except for race, categorical variables were aggregated by keeping the mode response across time points. Race and ethnicity were aggregated across time points based on whether a participant ever reported each race and ethnicity category.
Unless otherwise indicated.
No data were missing for this variable.
The number of times COVID-19 vaccines were offered to participants during site visits ranged from 0 to 7 (mean = 0.4). Rates of self-reported vaccination status among sites ranged from 24.0% to 65.8% (mean = 46.4%). Four of the 9 study sites offered COVID-19 vaccines at least once, and these included 2 that were colocated at community service centers. The other 5 sites never had COVID-19 vaccines available. Among 90 participants who visited multiple sites, only 54 participants (60.0%) visited both sites that offered COVID-19 vaccines and sites that never offered COVID-19 vaccines. Of the 655 participants who were ever offered a COVID-19 vaccine during visits, the mean (SD) number of times a vaccine was offered to them was 1.4 (0.8).
Colocation of COVID-19 Vaccination Services at SSPs
According to results from the Welch t test, we found no significant difference in self-reported vaccination rates between sites that offered COVID-19 vaccines (mean = 48.4%) and sites that never offered COVID-19 vaccines (mean = 44.8%; t7 = −0.33; P = .75) (Table 2). Overall, we found no significant association between self-reported COVID-19 vaccination status and having COVID-19 vaccines offered on the same day as participants’ site visit (odds ratio [OR] = 1.11; 95% CI, 0.71-1.72; P = .65). The intraclass correlation (ICC) for participants (ICC = 0.84) was substantially larger than for sites (ICC = 0.09). Age was significantly associated with vaccination status, such that each 1-year increase in age was associated with 1.19 times higher odds of receiving a COVID-19 vaccine (OR = 1.19; 95% CI, 1.11-1.27; P < .001), and the odds of having received a COVID-19 vaccine were significantly lower among participants experiencing housing instability than among those with stable housing (OR = 0.04; 95% CI, 0.01-0.13; P < .001).
Logistic regression results for the association between vaccine availability at the current visit and vaccination status, adjusting for demographic characteristics, among people who inject drugs and people experiencing houselessness in Oregon, July 2021 through March 2022 (n = 2871)
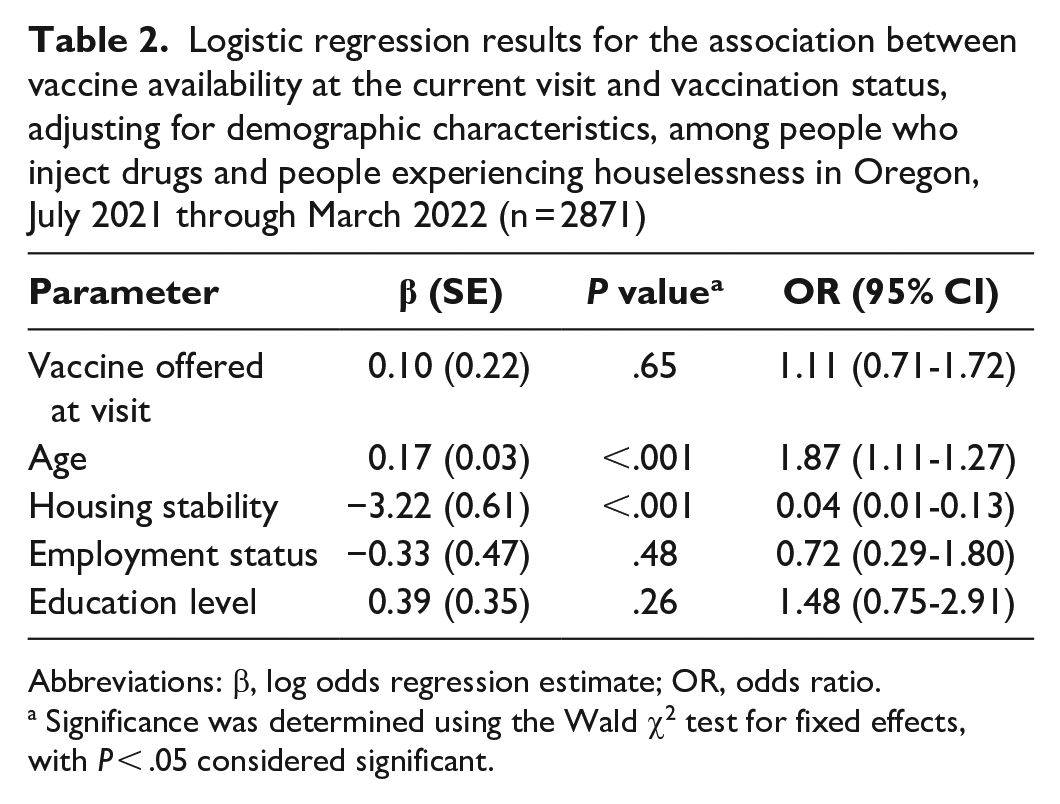
Abbreviations: β, log odds regression estimate; OR, odds ratio.
Significance was determined using the Wald χ2 test for fixed effects, with P < .05 considered significant.
The odds of being vaccinated for COVID-19 were 2.79 (95% CI, 2.18-3.58) times higher for each additional visit in which a vaccine was available to participants (P < .001) (Table 3). Site clustering (ICC = 0.04) accounted for only a small portion of the variance in vaccination status compared with within-individual clustering (ICC = 0.93).
Logistic regression results for the association between the number of visits where the vaccine was offered and vaccination status, adjusting for demographic characteristics, among people who inject drugs and people experiencing houselessness in Oregon, July 2021 through March 2022 (n = 2871)
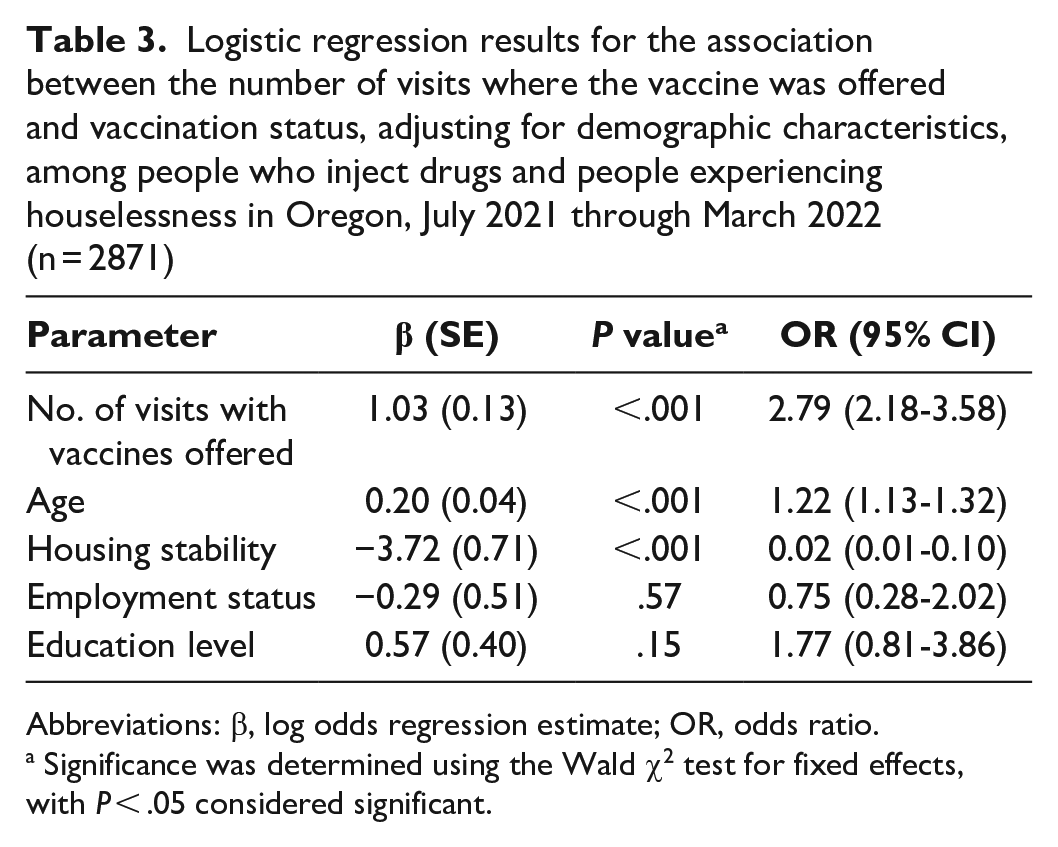
Abbreviations: β, log odds regression estimate; OR, odds ratio.
Significance was determined using the Wald χ2 test for fixed effects, with P < .05 considered significant.
Moderation Analyses
We found no significant interaction between whether a COVID-19 vaccine was offered on the same day as services engagement and age (OR = 1.03; 95% CI, 0.99-1.07; P = .13) or housing stability (OR = 0.59; 95% CI, 0.13-2.60; P = .48; ICCindividual = 0.90; ICCsite = 0.07) (Tables 4 and 5). The interaction between the number of times a COVID-19 vaccine was offered and age was also not significant (OR = 1.03; 95% CI, 0.99-1.07; P = .89) nor was moderation by housing instability (OR = 0.58; 95% CI, 0.13-2.60; P = .21; ICCindividual = 0.94; ICCsite = 0.02).
Moderation results of age and housing stability on the association between vaccine availability at the current visit and vaccination status, adjusting for demographic characteristics, among people who inject drugs and people experiencing houselessness in Oregon, July 2021 through March 2022 (n = 2871)
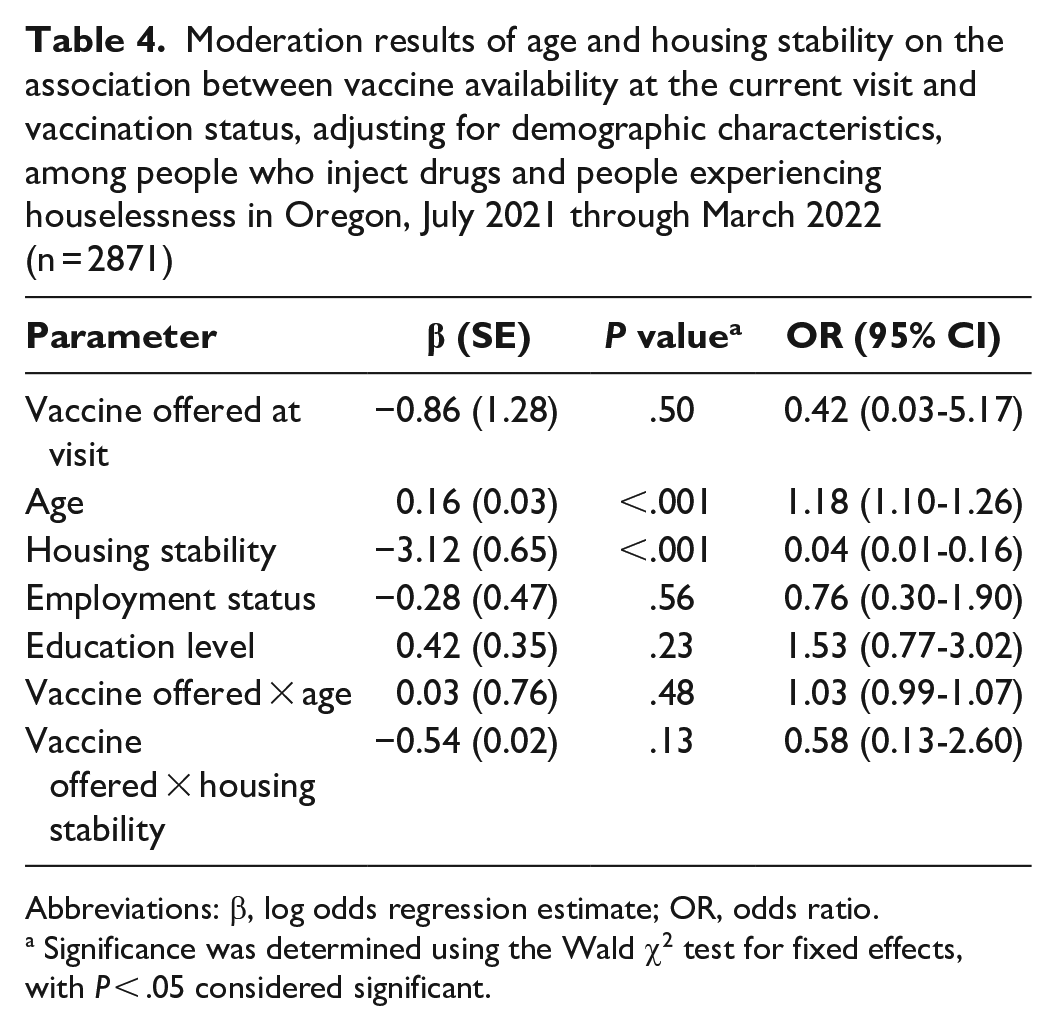
Abbreviations: β, log odds regression estimate; OR, odds ratio.
Significance was determined using the Wald χ2 test for fixed effects, with P < .05 considered significant.
Moderation results of age and housing stability on the association between the number of visits where the vaccine was offered and vaccination status, adjusting for demographic characteristics, among people who inject drugs and people experiencing houselessness in Oregon, July 2021 through March 2022 (n = 2871)
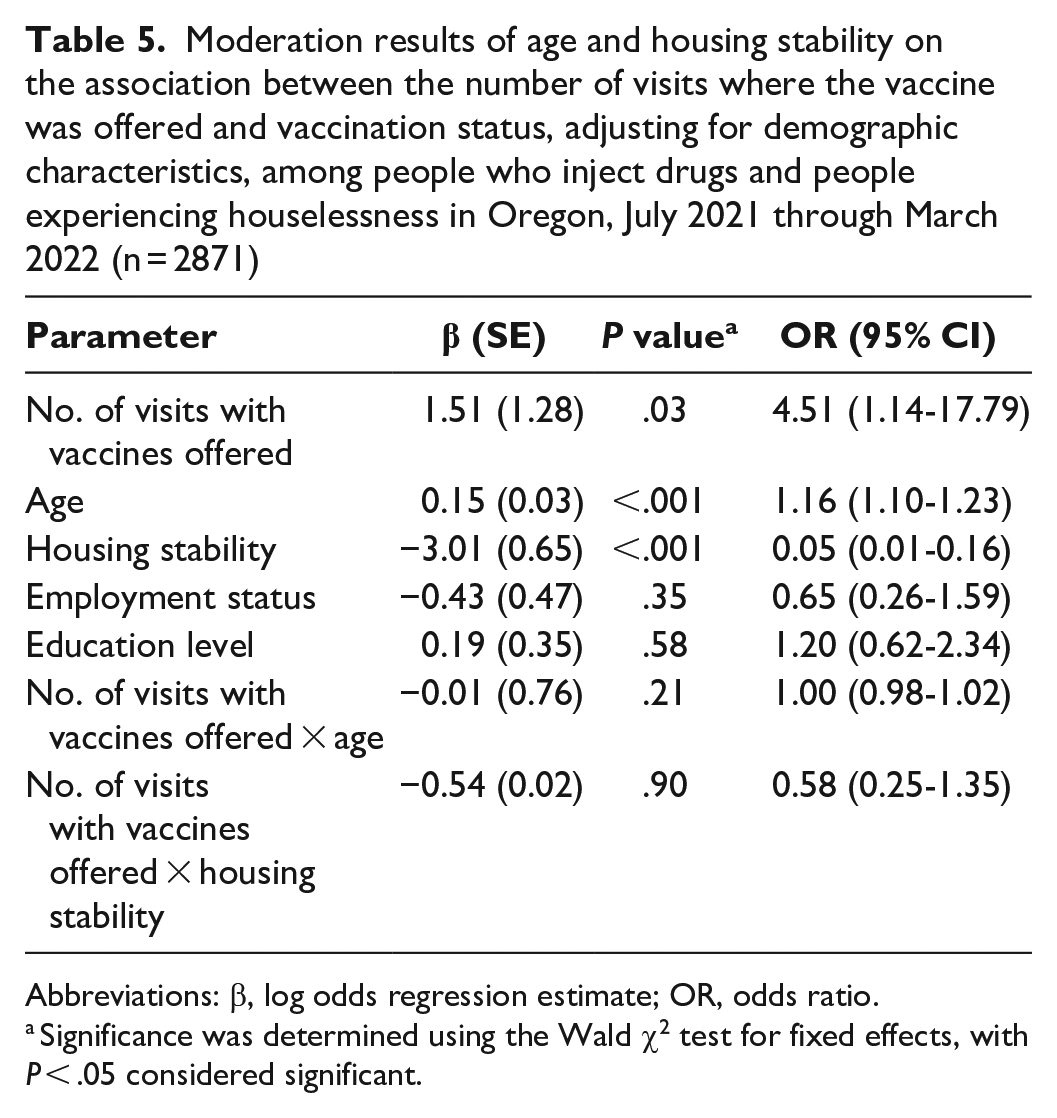
Abbreviations: β, log odds regression estimate; OR, odds ratio.
Significance was determined using the Wald χ2 test for fixed effects, with P < .05 considered significant.
Discussion
In this study, we analyzed whether colocating COVID-19 vaccination services at SSPs and community service centers was associated with vaccination status among PWID and PEH. Our findings partially supported our hypothesis that colocation of services would be associated with COVID-19 vaccination status among PWID and PEH. Specifically, colocating COVID-19 vaccines at SSPs and community service centers on the same day that PWID and PEH engaged with other services was not associated with vaccination status. In contrast, frequency of vaccine availability was associated with an increased likelihood of being vaccinated; that is, participants who had more opportunities to get vaccinated on-site were more likely to report being vaccinated than participants with limited on-site vaccination opportunities. As in previous studies,10-12 and consistent with the prioritization of older adults in vaccine rollout,33,34 housing instability and younger age were associated with being unvaccinated, but housing stability and age did not moderate the associations between colocation of COVID-19 vaccination services and vaccination status. Together, these results suggest that offering vaccines frequently may improve vaccine uptake for PWID and PEH.
Colocation of Vaccination Services
There are several potential explanations for why the frequency of availability was associated with COVID-19 vaccination status among PWID and PEH. Trust in health care providers, attitudinal shifts, and service convenience could explain this association. Distrust in the production and necessity of COVID-19 vaccines was a barrier to vaccine uptake among PWID and PEH.10,11,35-39 Having vaccine providers on-site at trusted sites, specifically SSPs40,41 and community service centers, 42 may have increased client trust in COVID-19 vaccines.43,44 Some PWID and PEH have endorsed beliefs that COVID-19 vaccines are ill-intentioned, harmful strategies by governments and pharmaceutical industries.11,12 Sites that offered frequent vaccination services may have overcome vaccine hesitancy by building trust in vaccine providers over time and affording opportunities to engage in meaningful dialogue about vaccination. About one-third of participants who received the first dose of an mRNA vaccine at a COVID-19 vaccination clinic colocated with an SSP in Maryland got their second dose elsewhere, 22 potentially indicating attitudinal shifts after engaging with the colocated clinics. Future studies could examine vaccine confidence and service provider trust as mechanisms by which colocating vaccination services at trusted community sites increases vaccination uptake. Qualitative research suggests that SSPs operated by community-based organizations are hesitant to partner with local health departments because of concerns about the cultural competence of clinical staff (eg, to not further stigmatize SSP participants), and social stigma is a barrier to advertising vaccination services. 44 Efforts to address these concerns could include destigmatizing campaigns and building community capacity so SSPs can offer vaccination services independently.44,45
Service convenience is another explanation for our findings. Qualitative research has found that convenience facilitated PWID and PEH receiving COVID-19 vaccines.11,35,46 Convenience may not necessarily affect same-day vaccination because participants may still wish to take the time to learn more before making a health decision. Another explanation for our nonsignificant same-day findings is that participants received financial incentives for SARS-CoV-2 testing, 47 so it is possible that participants prioritized testing services over vaccination services because of the financial benefit. Moreover, if participants engaged in vaccination services after testing services, they would not have reported vaccination during their testing visit as it relates to same-day vaccination status.
Moderation Analyses
Similar to prior studies,10-12 younger age and housing instability were associated with a lower likelihood of vaccination compared with older participants and those with stable housing. Considering this finding, we also expected there to be potential for behavior change among these subgroups because of service colocation. However, age and housing stability did not moderate the association between colocation of COVID-19 vaccination services and vaccination status, suggesting this colocation of services strategy was not differentially associated with vaccination status among younger participants and participants experiencing housing instability. Therefore, additional strategies may be needed to further engage young people and PEH in COVID-19 vaccination services. Potential strategies may include providing clearer education, involving trusted peer messengers and financial incentives for PEH,16,46 and using messaging centered on young people, including social media. 38
Limitations
Our study design had several limitations. First, this was a quasi-experimental study, and causal inferences about the effectiveness of service colocation cannot be conclusively made. However, public health entities selected sites to offer COVID-19 vaccines based on their staff availability rather than site characteristics. Second, our results are specific to the context of SSPs in Oregon. That is, regarding sample demographic characteristics, although our sample was >80% White, our sample mirrored the general SSP population that HIV Alliance serves in Oregon. 47 Third, we attempted to track site visits and the vaccination history of each participant, but self-report is vulnerable to bias and may lack precision. We measured only whether each participant self-reported ever receiving a COVID-19 vaccine. Thus, our measure of vaccination status was not exclusive to on-site vaccination; that is, participants could have been vaccinated on- or off-site. Mechanisms such as frequent exposure to vaccination services and trust in service providers could have shifted participants’ attitudes toward COVID-19 vaccines, and our findings may point toward an increase in vaccination at SSPs, community service centers, and elsewhere. Because this study was conducted during a 7-month period, participants may have been more likely to report vaccination toward the end of the study period than at the beginning of the study period due to increased access to COVID-19 vaccines off-site in March 2022 compared with July 2021. Future studies could examine the effect of colocation of vaccination services on vaccine uptake on- and off-site. Fourth, we measured whether vaccination services were available on the same day participants filled out the intake form. This means participants could have been vaccinated after filling out their intake form; as such, their vaccination after engaging in testing would not have been included. Finally, our null finding about the difference in vaccination status between sites that offered a COVID-19 vaccine at any point and sites that did not offer a COVID-19 vaccine at any point may have been a result of our small sample size of sites (n = 9). Analyzing this association again with a larger sample size might yield different results.
Conclusions
This study provides evidence that frequent colocation of vaccination services at SSPs and community service centers may increase vaccination among PWID and PEH, 2 populations that are undervaccinated compared with the general US population.12,36,48,49 Fewer than half of SSPs in the United States offered COVID-19 vaccinations on-site during the peak of the pandemic,20,21 as many faced barriers such as lack of appropriate facilities, funding, and trained staff.21,44 Offering vaccines frequently at trusted community sites is important for improving vaccination rates among PWID and PEH.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this article was supported by the National Institute on Drug Abuse of the National Institutes of Health under award no. R01DA037628, U01DA055982, U01DA057849. The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.