
Abstract
Objectives:
The Think. Test. Treat TB health communications campaign aims to increase the awareness of latent tuberculosis infection (LTBI) primarily among people born in the Philippines and Vietnam and other non–US-born groups (consumers) and the health care providers (providers) who serve them. We conducted a process evaluation to assess reach and audience engagement and an outcome evaluation to assess awareness, knowledge, perceptions, and behavioral intentions among audiences of the campaign.
Methods:
To evaluate the process, the Centers for Disease Control and Prevention measured exposure to (eg, with impressions [total advertisements]) and engagement with (eg, online clicks) the campaign during its rollout (March–September 2022). After the rollout, to evaluate outcomes, we administered online surveys to consumers and providers who were exposed and not exposed to the campaign.
Results:
The Think. Test. Treat TB campaign resulted in >33 million impressions, >2000 materials downloaded from the internet, and >33 000 materials shipped. Of 173 consumers who completed the evaluation survey, 123 (71.1%) were exposed to the campaign, with 108 (87.8%) reporting intention to ask their provider about tuberculosis (TB) during their next visit. Of 44 providers who completed the evaluation survey, 24 (54.5%) did not feel that they were the intended audience of the campaign, yet all felt the campaign materials were relevant to their patients, and 42 (95.5%) felt the materials were relevant to providers who serve patients at risk for TB.
Conclusion:
The Think. Test. Treat TB campaign was successful in raising awareness of LTBI among the intended audiences. Continuing engagement with key audiences about LTBI to encourage testing and treatment is integral to eliminate TB in the United States.
Tuberculosis (TB) is a bacterial infection caused by Mycobacterium tuberculosis. If a person is infected with TB bacteria and their immune system cannot stop the bacteria from multiplying in the body, TB disease develops, may spread to others, and can be fatal if not treated properly. Latent TB infection (LTBI) is a condition that occurs when the immune system stops the bacteria from multiplying and a small number of TB bacteria remain in the body that are alive but inactive. People with LTBI do not have symptoms, do not feel sick, and cannot spread TB to others. Up to an estimated 13 million people are living with LTBI in the United States. 1 About 5% to 10% of people with LTBI will develop TB disease if untreated. More than 85% of TB cases in the United States have been attributed to LTBI progression to TB disease. 2
Efforts to eliminate TB in the United States include LTBI testing and treatment. The Centers for Disease Control and Prevention (CDC) recommends primary care providers and clinicians test for TB infection as a routine and integral part of health care for patients with increased risk for TB and prescribe and manage LTBI treatment if needed. 3 People born outside the United States accounted for 73.8% of the 8331 reported TB cases in the United States in 2022. 4 Within this group, more than half of reported cases were among people from Mexico, the Philippines, India, Vietnam, and China, and 44.0% of reported cases were people who identified as non-Hispanic Asian. 4
Description of the Program Being Evaluated
In 2020, CDC’s Division of Tuberculosis Elimination launched the first national LTBI health communications campaign, Think. Test. Treat TB. 5 The campaign aims to increase awareness of LTBI primarily among people born in the Philippines and Vietnam and other non–US-born groups (hereinafter, consumers) and among the health care providers (hereinafter, providers) who serve them. The campaign’s principal concept is that it is critical for patients and providers to “think” about TB risk factors and talk about TB, “test” for LTBI, and “treat” LTBI to prevent the development of TB disease. The campaign was disseminated in Seattle, Washington, and Los Angeles, California, and materials were made available online for use nationally. Campaign activities launched around World TB Day in March 2020 and were amplified around Asian American and Pacific Islander Heritage Month in May 2020. Public health departments received materials ahead of the launch and were encouraged to promote the campaign. Consumer campaign materials were available in English, Vietnamese, Chinese, Ilocano, Marshallese, Tagalog, and Spanish; provider materials were in English. Materials included digital and print formats. To align with consumers’ media consumption habits, CDC reached out to in-language Asian American media outlets for placements at no cost, leveraged CDC-owned channels (ie, CDC internet pages and social media platforms), and paid to place signage in grocery stores, pharmacies, and shopping centers and on electronic truck signs circulating in the community. For campaign materials for providers, CDC leveraged its media channels on TB (ie, websites and social media accounts) and paid to advertise campaign materials among trade and medical partners (eg, American Academy of Family Physicians, MedScape).
Purpose of the Evaluation
CDC conducted formative, 6 process, and outcome evaluations to gain a holistic view of the Think. Test. Treat TB communications campaign. The objective of the process evaluation was to assess reach and audience engagement during the campaign rollout. The objective of the outcome evaluation was to assess awareness, knowledge, perceptions, and behavioral intentions among campaign audiences. Lessons learned from the process and outcome evaluations can guide adjustments to campaign content and strategy.
Methods
Process Evaluation Methods
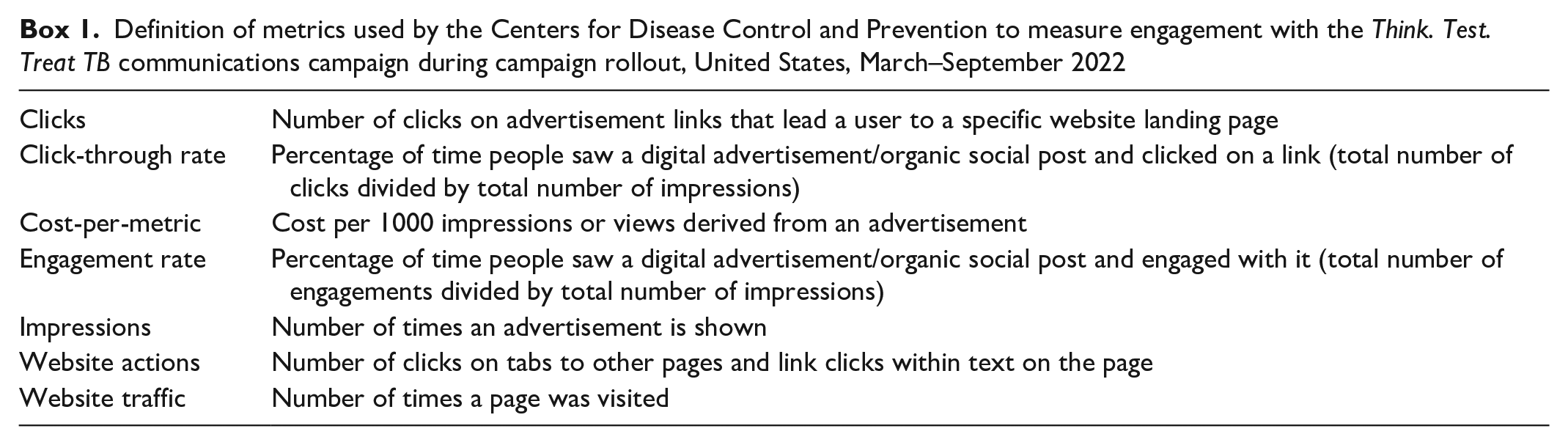
During rollout of the Think.Test. Treat TB health communications campaign (March through September 2022), CDC measured exposure to and engagement with the campaign. CDC measured exposure by impressions, television spots, email opens, cost-per-metric (CPM), and distribution of the campaign (ie, posts, email sends, number of placements). CDC measured engagement by clicks, click-through rates (CTRs), engagement rates, website traffic/actions, social media actions, and CDC warehouse orders (Box 1). Metrics included those for paid media, where CDC purchased distribution, and earned media, where CDC conducted outreach to media outlets to promote the campaign at no cost.
Definition of metrics used by the Centers for Disease Control and Prevention to measure engagement with the Think. Test. Treat TB communications campaign during campaign rollout, United States, March–September 2022
Outcome Evaluation Methods
We conducted online surveys with consumers and providers in Seattle, Washington, from July 28 through August 22, 2022. We administered surveys via the Snap Surveys software platform (Snap Surveys Ltd). Consumers could take the survey in English or Vietnamese; providers could take the survey in English only. We based survey questions on McGuire’s Communication–Persuasion Matrix to assess campaign exposure, information recall, message comprehension, perceived risk, agreement with messages, decisions and rationale related to messages, actions taken in response to messages, and advising others to take action. 7
We created separate surveys for consumers and providers. For both surveys, we started the survey with questions to screen for exposure to the campaign. For respondents who reported exposure to the campaign, we provided questions about where they saw the materials and actions taken in response to the materials. For respondents who reported no exposure to the campaign, we provided campaign materials midway through the survey and provided follow-up questions about the materials. Respondents answered a mix of closed- and open-ended questions.
Respondents
Eligibility for consumer surveys included respondents (1) born in the Philippines or Vietnam, (2) aged 20 to 65 years, and (3) living in zip codes where the campaign was disseminated. Eligibility for provider surveys included providers who (1) self-reported that ≥20% of their patient population comprised non–US-born Asian people, (2) self-identified as a primary care provider (defined as an internal, general, or family medicine physician; nurse; nurse practitioner; or physician associate/physician assistant), and (3) practiced in the zip codes where the campaign was disseminated. Because of resource constraints, our target sample size was 150 to 200 consumers and 25 to 50 providers. To ensure people exposed to the campaign were well represented, we aimed to sample 3 consumers or providers who were exposed to the campaign per 1 consumer or a provider who was not exposed to the campaign. We additionally aimed to sample equal proportions of consumers by sex and country of birth.
Recruitment and data collection
We recruited respondents through an online survey panel and community outreach. For community outreach, we distributed flyers in establishments, based on zip codes where the campaign was distributed, that serve the intended audience. The flyers had an invitation to join the panel to participate in the survey. On the flyers, we included an email address and telephone number that respondents could use to express interest and a QR code that respondents could scan with a smartphone. Each survey required approximately 15 minutes to complete. Respondents could decline to respond to any question. We considered surveys as complete, with results included in the analyses, if ≥90% of closed-ended items had a response.
Statistical analysis
We analyzed responses to open-ended questions by using thematic coding. We analyzed closed-ended responses descriptively to identify patterns. We calculated means and proportions to examine sample characteristics and used tests of association (Fisher exact tests for categorical variables, t tests for continuous variables, Mann–Whitney U tests for ordinal variables) to examine relationships between campaign exposure and responses to survey questions, with P < .05 considered significant. We used SPSS version 29.0.1.0 (IBM Corp) for analyses.
Ethical Considerations
CDC determined that the evaluation was not research and its conduct was consistent with applicable federal law and CDC policy (eg, 45 CFR part 46; 21 CFR part 56; 42 USC §241[d]; 5 USC §552a; 44 USC §3501 et seq). We obtained informed consent from respondents electronically and provided copies of informed consent forms to respondents. We compensated respondents with a $25 payment for consumers and a $75 payment for providers. We provided compensation even if respondents ended the survey before completion.
Results
Process Evaluation Results
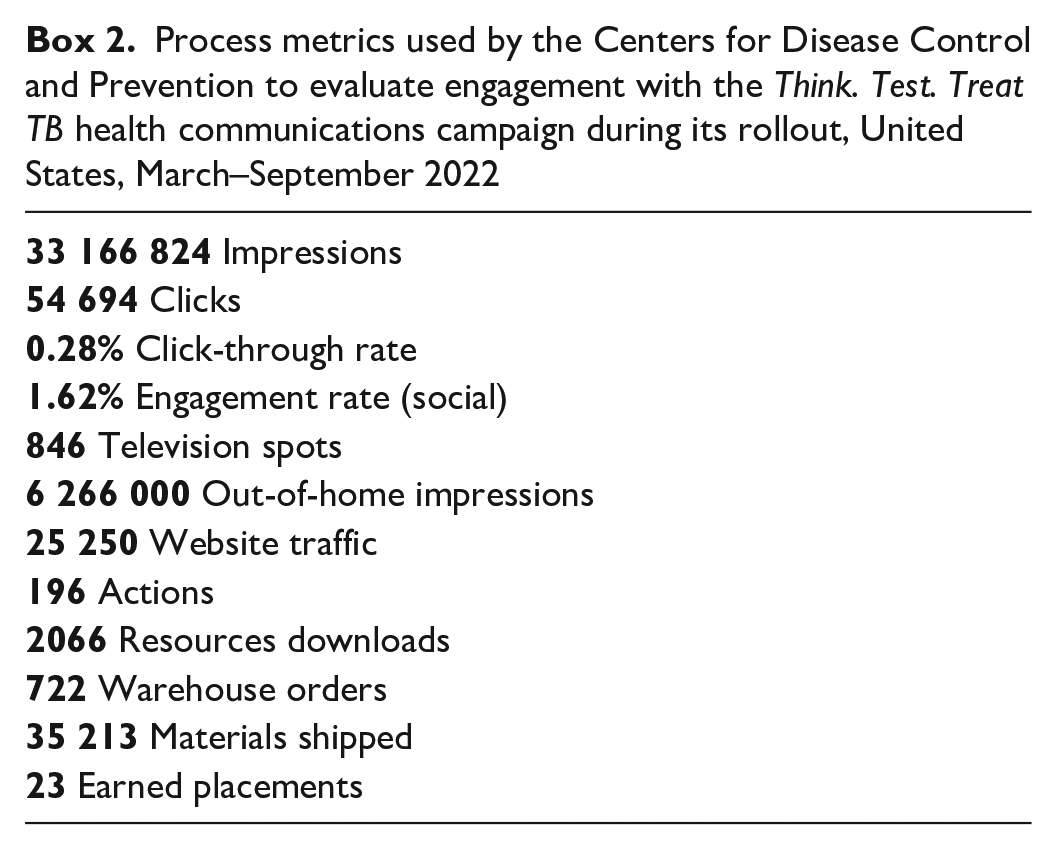
In process metrics used by CDC to evaluate the Think. Test. Treat TB campaign (Box 2), the consumer-paid media portion of the campaign delivered 24.8 million impressions and 33 281 clicks. Digital display banners and video, available on sites such as yahoo.com and msn.com, delivered the most impressions (12 million), the most clicks (18 000), and the lowest CPM ($5.78) compared with out-of-home, social, YouTube, television, and print media. Digital banners delivered more impressions (9 million) than video did (3 million), and video garnered slightly more clicks than digital banners did (10 000 vs 9000). YouTube generated fewer impressions and clicks than digital video did (~2 million impressions and 578 clicks). Social media (Facebook and Instagram) had the second-lowest CPM ($6.51) and the strongest CTR (0.37%). The consumer-earned media portion of the campaign resulted in 23 print, newspaper, website, television, and YouTube placements with about 4 million total impressions.
Process metrics used by the Centers for Disease Control and Prevention to evaluate engagement with the Think. Test. Treat TB health communications campaign during its rollout, United States, March–September 2022
The provider-paid media portion of the campaign resulted in about 1.4 million impressions and 1770 clicks with a 0.13% CTR. Compared with email and newsletters, digital displays available via online medical references and scientific journals were the most effective in driving impression reach and click engagements, with placements in American Family Physician and Medscape contributing most to these metrics. The provider-earned media portion of the campaign included coverage in numerous news and other publications (eg, CBS, Fox News outlets). More than 2 million unique visitors per month visited earned media publications for providers.
From March 15 through July 31, 2022, the Think. Test. Treat TB CDC website garnered 55 151 page views, with >20 000 of these views on the Vietnamese page. The top 3 English materials ordered from the CDC warehouse were the provider conversation guide (107 orders, 5039 materials distributed), patient conversation guide (83 orders, 5152 materials distributed), and Learn the Facts factsheet (81 orders, 5525 materials distributed).
Outcome Evaluation Results
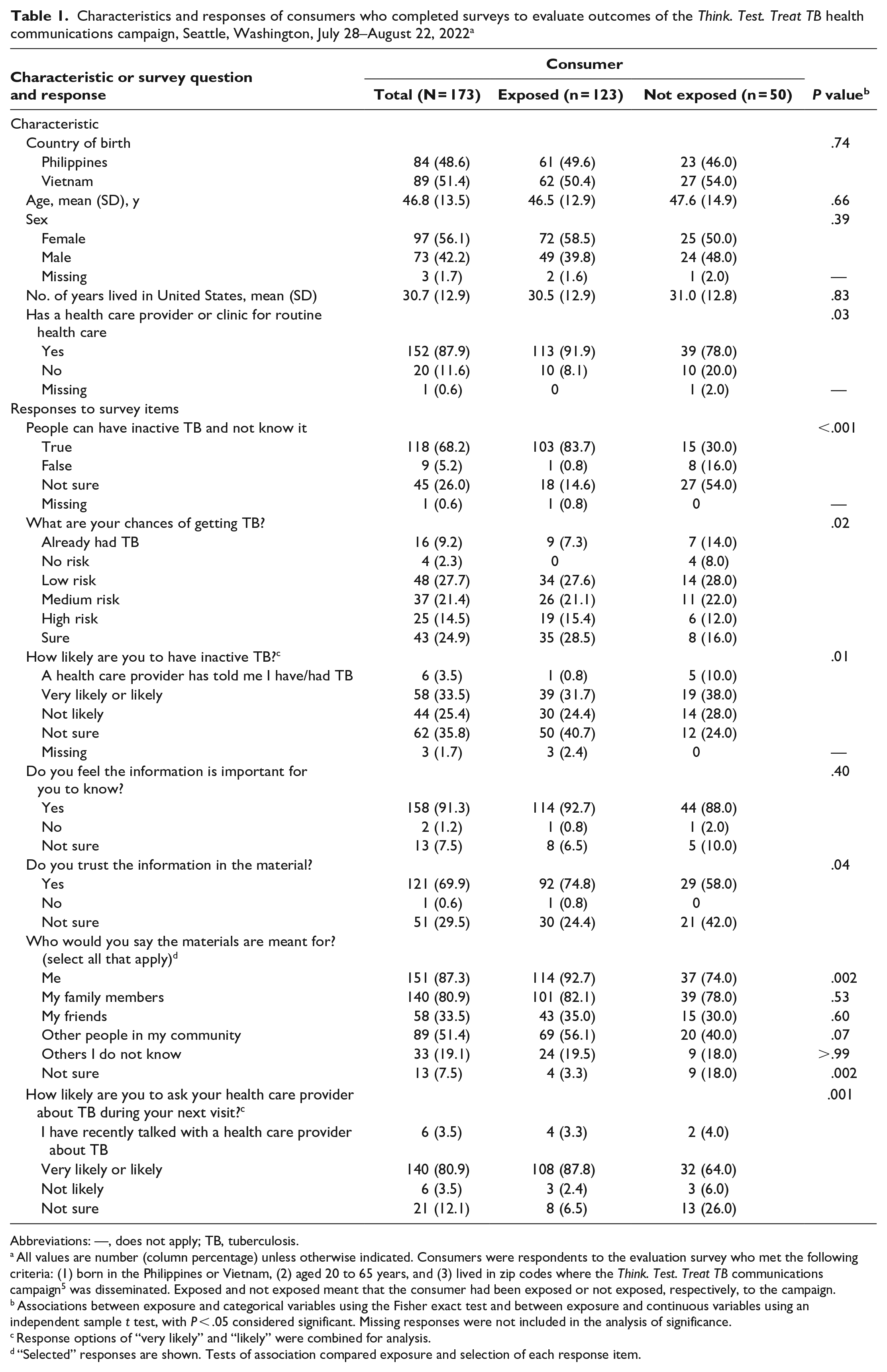
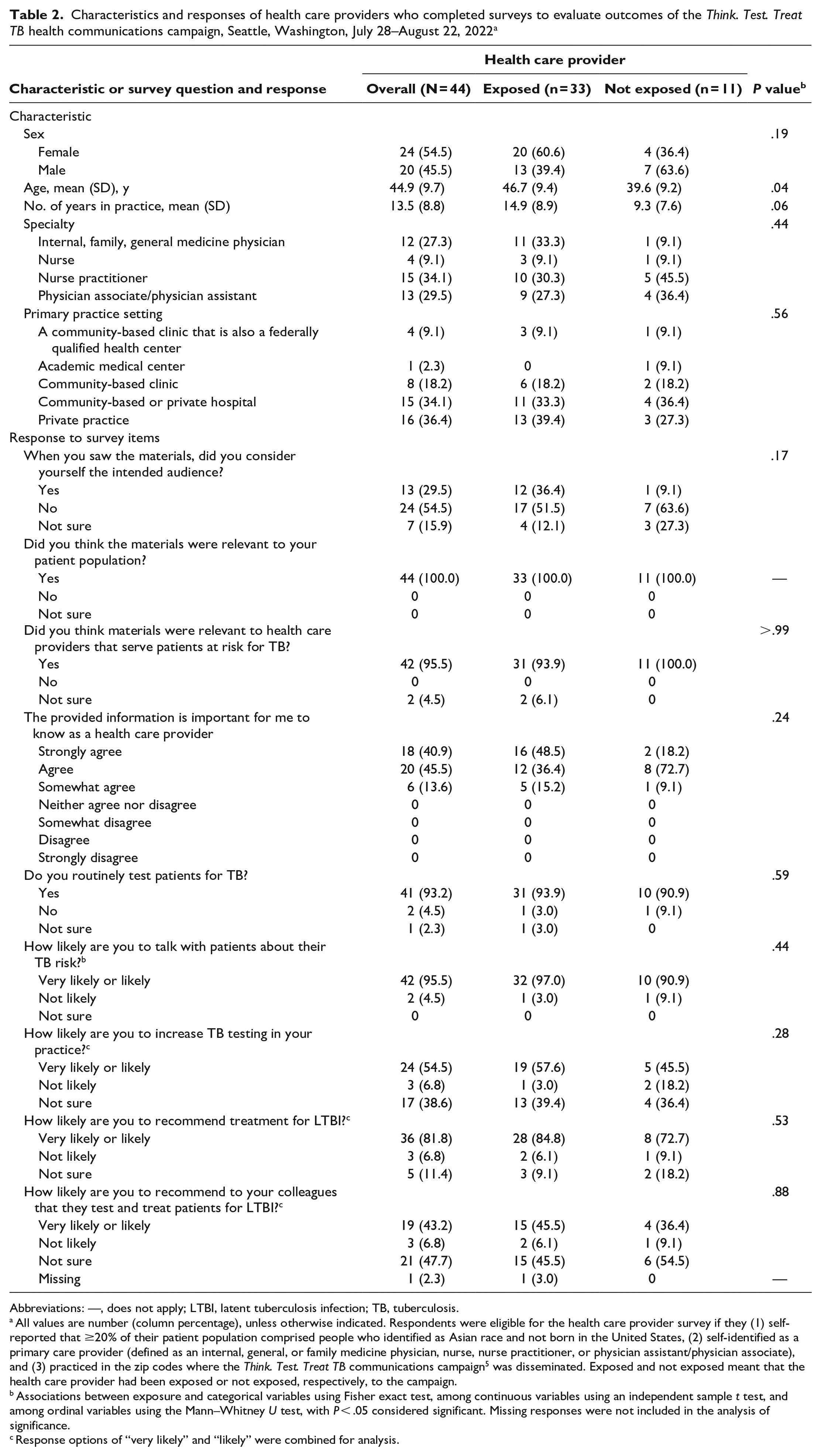
Of 173 consumers who completed the survey, 123 were exposed and 50 were not exposed to the campaign (Table 1). Of 44 providers who completed the survey, 33 were exposed and 11 were not exposed to the campaign (Table 2). Consumers had a response rate of 19.3% (405 started the survey of 2100 invitations), and providers had a response rate of 15.9% (60 started the survey of 377 invitations) (Figure). Four consumer surveys were completed in Vietnamese (1 exposed, 3 not exposed). Consumers exposed to the campaign (113 of 123; 91.9%) were significantly more likely than consumers not exposed to the campaign (39 of 50; 78.0%) to report having a provider or clinic for routine health care (P = .03). Providers exposed to the campaign were on average about 7 years older than providers not exposed to the campaign (P = .04). Other demographic characteristics were not significantly different between exposure groups.
Characteristics and responses of consumers who completed surveys to evaluate outcomes of the Think. Test. Treat TB health communications campaign, Seattle, Washington, July 28–August 22, 2022 a
Abbreviations: —, does not apply; TB, tuberculosis.
All values are number (column percentage) unless otherwise indicated. Consumers were respondents to the evaluation survey who met the following criteria: (1) born in the Philippines or Vietnam, (2) aged 20 to 65 years, and (3) lived in zip codes where the Think. Test. Treat TB communications campaign 5 was disseminated. Exposed and not exposed meant that the consumer had been exposed or not exposed, respectively, to the campaign.
Associations between exposure and categorical variables using the Fisher exact test and between exposure and continuous variables using an independent sample t test, with P < .05 considered significant. Missing responses were not included in the analysis of significance.
Response options of “very likely” and “likely” were combined for analysis.
“Selected” responses are shown. Tests of association compared exposure and selection of each response item.
Characteristics and responses of health care providers who completed surveys to evaluate outcomes of the Think. Test. Treat TB health communications campaign, Seattle, Washington, July 28–August 22, 2022 a
Abbreviations: —, does not apply; LTBI, latent tuberculosis infection; TB, tuberculosis.
All values are number (column percentage), unless otherwise indicated. Respondents were eligible for the health care provider survey if they (1) self-reported that ≥20% of their patient population comprised people who identified as Asian race and not born in the United States, (2) self-identified as a primary care provider (defined as an internal, general, or family medicine physician, nurse, nurse practitioner, or physician assistant/physician associate), and (3) practiced in the zip codes where the Think. Test. Treat TB communications campaign 5 was disseminated. Exposed and not exposed meant that the health care provider had been exposed or not exposed, respectively, to the campaign.
Associations between exposure and categorical variables using Fisher exact test, among continuous variables using an independent sample t test, and among ordinal variables using the Mann–Whitney U test, with P < .05 considered significant. Missing responses were not included in the analysis of significance.
Response options of “very likely” and “likely” were combined for analysis.
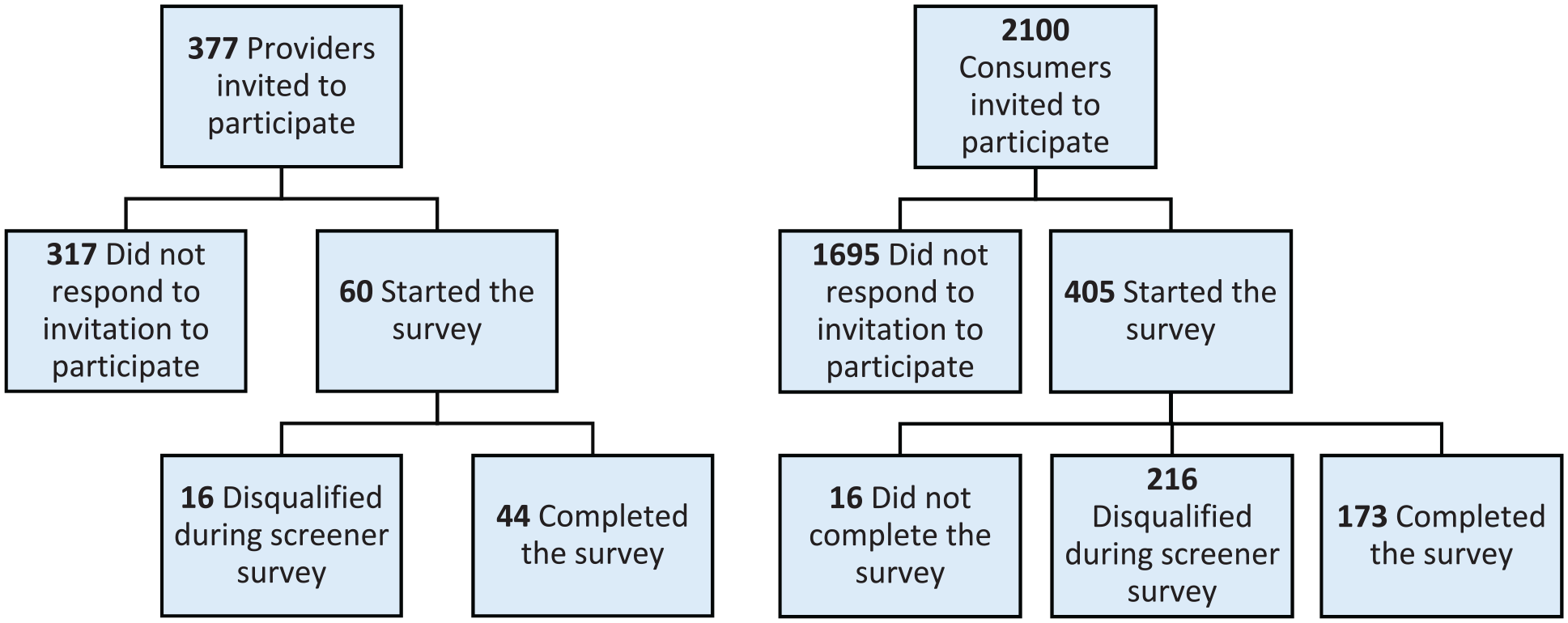
Flow diagrams of response rates of consumers and health care providers (providers) to surveys conducted to evaluate outcomes of the Think. Test. Treat TB health communications campaign, Seattle, Washington, July 28–August 22, 2022.
Consumer responses
Among 123 consumers exposed to the campaign, 76 (61.8%) reported seeing the materials in their physician’s office, 72 (58.5%) on social media, 38 (30.9%) in a newspaper or magazine, 28 (22.8%) in the supermarket on a television screen, 18 (14.6%) on television, 17 (13.8%) at a store on a ceiling banner, 11 (8.9%) on YouTube, 3 (2.4%) on websites, and 1 (0.8%) on a truck sign in the community (responses not mutually exclusive). Consumers reported taking the following actions most often after exposure to the campaign: reading through the messages (48 of 123; 39.0%), looking up more information on TB (42 of 123; 34.1%), and scrolling through the content (40 of 123; 32.5%) (responses not mutually exclusive).
Consumer knowledge was assessed with the item “people can have inactive TB and not know it.” A higher percentage of people exposed to the campaign correctly answered “true” (103 of 123; 83.7%) compared with those not exposed (15 of 50; 30.0%) (Table 1). When asked about their chances of getting TB, of all 173 consumers, 4 (2.3%) reported no risk, 48 (27.7%) reported low risk, 37 (21.4%) reported medium risk, and 25 (14.5%) reported high risk, whereas 43 consumers (24.9%) were not sure. Of 173 consumers, 58 (33.5%) felt very likely or likely to have inactive TB, 44 (25.4%) felt not likely, and 62 (35.8%) were not sure. Almost all consumers (158 of 173; 91.3%) felt the information in the campaign was important for them to know, and 121 consumers (69.9%) reported trusting the information. Overall, most consumers (151 of 173; 87.3%) felt the materials were meant for themselves; those exposed to the campaign (114 of 123; 92.7%) were significantly more likely than those not exposed to the campaign (37 of 50; 74.0%) to feel that the materials were meant for themselves (P = .002), whereas consumers not exposed to the campaign (9 of 50; 18.0%) were significantly more likely than those exposed to the campaign (4 of 123; 3.3%) to report not being sure whom the materials were meant for (P = .002). Of 173 consumers, 140 (80.9%) reported being likely or very likely to ask their provider about TB during their next visit; those exposed to the campaign (108 of 123; 87.8%) significantly more often reported being very likely or likely to ask their provider about TB than those not exposed (32 of 50; 64.0%) (P = .001).
To improve the campaign, consumers suggested adding more information about TB and providing a method to learn more or ask questions. For example, 1 consumer suggested, “Tell me why I should do what it says; they tell you to do something and don’t say why I need to.”
Provider responses
Of 33 providers exposed to the campaign, 18 (54.5%) reported seeing the materials in a communication from the public health department; 16 (48.5%) in their workplace; 15 (45.5%) on the CDC website; 13 (39.4%) on social media; 5 (15.2%) on Medscape, UpToDate, or other online references for clinical information; 3 (9.1%) on online networking services for medical professionals; 2 (6.1%) in journals or medical publications; 2 (6.1%) in professional association newsletters or emails; 2 (6.1%) on professional organization webpages; and none in materials at professional meetings (responses not mutually exclusive). After seeing the campaign, providers most frequently reported looking up additional information about TB (19 of 33; 57.6%), scrolling through the content (14 of 33; 42.4%), reviewing the patient conversation guide (10 of 33; 30.3%), and reading through the messages (10 of 33; 30.3%) (responses not mutually exclusive). More than half of exposed providers felt the materials helped expand their knowledge of incidence of progression from LTBI to active TB disease (22 of 33; 66.7%) and testing options for TB (17 of 33; 51.5%) (responses not mutually exclusive).
Of all 44 providers, 24 (54.5%) did not feel that they were the intended audience of the campaign, yet all felt the campaign materials were relevant to their patients, all agreed on some level that the information was important for them to know, and 42 (95.5%) felt the materials were relevant to providers who serve patients at risk for TB (Table 2). Of 44 providers, 41 (93.2%) reported already routinely testing patients for TB. We examined the perceived relevance of campaign materials among the 2 providers who reported not already testing, and neither felt they were the intended audience. Most providers reported being very likely or likely to talk with patients about their TB risk (42 of 44; 95.5%), increase TB testing in their practice (24 of 44; 54.5%), and recommend treatment for LTBI (36 of 44; 81.8%). Providers reported that the primary reason they were not sure about or not likely to increase testing was that they were already testing patients. Of the 2 providers who reported not already testing for TB, 1 provider felt likely to increase testing and the other was not sure. Fewer than half of providers (19 of 44; 43.2%) reported being very likely or likely to recommend that their colleagues test and treat patients for LTBI, and 21 (47.7%) were unsure. Provider suggestions for improving the campaign focused on the appearance of the materials (ie, images, colors).
Lessons Learned
The integrated Think. Test. Treat TB health communications campaign was distributed and amplified across paid, earned, and owned channels to consumers and providers. The messages, images, and channel mix, which were guided by best practices, local TB programs and partners, and formative evaluation, were successful in raising awareness of LTBI among the intended audiences. Timing the launch of the campaign with World TB Day successfully garnered attention from intended audiences and partners. The campaign had earned media and CDC-owned social content specific to Asian American and Pacific Islander Heritage Month and provided general content across other channels. Future campaign efforts can explore developing creative content specific to cultural observances.
In the context of McGuire’s Communication–Persuasion Matrix, both consumers and providers reported paying attention to the campaign, understanding and retaining content, and indicating agreement with messages, as illustrated by self-reports of seeking more information after exposure to the campaign. Because consumers who reported being exposed to the campaign (vs those not exposed to the campaign) felt campaign materials were meant for themselves and noted behavioral intentions aligned with the campaign’s goals, dissemination channels may have improved the perceived relevance and effectiveness of messages. Among providers who responded to the survey, both exposed and not exposed providers reported already routinely testing patients for TB and behavioral intentions aligned with the campaign’s goals, which may have influenced why provider respondents did not perceive the campaign as relevant to themselves, even though they felt the campaign was relevant to their patients. However, just 19 of 44 providers reported intentions to recommend LTBI testing and treatment to colleagues, and the 2 providers who reported not already testing patients for TB did not feel they were the intended audience of the campaign, which signaled to us an audience that warrants further investigation. Participant suggestions will guide future communications products.
Limitations
Our outcome evaluation had some limitations. First, surveys relied on self-reported information, which can be subject to social desirability and recall biases. Second, our evaluation was a small, localized evaluation conducted with the intended audiences for a tailored health communications campaign; thus, results are not generalizable to or representative of US provider and consumer audiences. Generalizability was further decreased by respondents needing to own an electronic device with internet access and self-selecting participation based on community outreach. Third, surveys were conducted shortly after campaign rollout, which limited the possibility to assess long-term effects and behavior change. Fourth, other TB-related interventions may have had confounding effects, particularly among providers working in a city with a proactive public health department TB program. Process evaluation metrics were also challenging to compare across platforms.
Conclusion
Evaluation of the first large-scale LTBI health communications campaign in the United States demonstrated the importance of communicating with key audiences about LTBI. Continuing engagement with providers and consumers about LTBI to encourage testing and treatment is integral to eliminate TB in the United States. The campaign is just one part of a multifaceted approach taken by CDC to advance this goal, and other CDC TB prevention efforts include the TB Elimination Alliance, 8 TB Centers of Excellence, 9 TB personal stories, 10 and the development and dissemination of other multilingual educational products. 11
Footnotes
Acknowledgements
The authors thank the California Department of Public Health, Washington State Department of Health, Los Angeles County Department of Public Health, Orange County Health Care Agency, and Public Health–Seattle & King County for their partnership in strategy, dissemination, and outreach efforts of the campaign and their work to advance TB prevention and control. The authors acknowledge the work of Weber Shandwick for contributions to the process evaluation and CATMEDIA and Tallgrass Market Research for their contributions to the outcome evaluation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Centers for Disease Control and Prevention through contracts HHSD2002015M88164B and HHSD2002015M88156B provided funding for the evaluations.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. The use of product or company names in this article is for identification purposes only and does not imply any endorsement by the authors.