
Abstract
Objectives:
More than 3300 rural Alaska Native homes lack piped water, impeding hand hygiene. During the COVID-19 pandemic, the Alaska Native Tribal Health Consortium and the Centers for Disease Control and Prevention partnered with 10 Tribal communities and regional Tribal health organizations to install a low-cost, intermediate-technology water and sanitation system, the Miniature Portable Alternative Sanitation System (Mini-PASS). We assessed the impact of the Mini-PASS handwashing station on handwashing, other water-related uses, and problems encountered over time.
Methods:
In this pre–postintervention study, we conducted semi-structured interviews by telephone seasonally with representatives of 71 households with the Mini-PASS from February 2021 through November 2022 to assess the impact of the units on water use and health.
Results:
Before Mini-PASS installation, all participating households primarily used washbasins for handwashing. Postintervention, more than 70% of households reported using the Mini-PASS as their primary handwashing method in all 3 follow-up intervals (3, 6-9, and 12 months postintervention). The proportion of households using the handwashing station for other household tasks increased during 12 months, from 51.4% (19 of 37) at 3 months postintervention to 77.8% (21 of 27) at 12 months postintervention. Although approximately 20% to 40% of households reported problems with their handwashing station during the 12 months postintervention, a large proportion of interviewees (47% to 60%) said they were able to conduct repairs themselves.
Conclusions:
Households in rural Alaska quickly adopted the Mini-PASS for hand hygiene and other needs and were largely able to troubleshoot problems themselves. Further research evaluating the impact of improved handwashing behaviors facilitated by the Mini-PASS should be conducted.
Handwashing is a well-known strategy to prevent infections. However, according to the World Health Organization, more than 2.3 billion people worldwide lack access to handwashing facilities with water, including 1.4 million people in the United States.1,2 Racial and ethnic minority–headed households, particularly American Indian/Alaska Native (AI/AN) households, are more likely than households of other racial and ethnic groups to lack these handwashing facilities and have the associated health risks, including SARS-CoV-2 infection.3-8
At the start of the COVID-19 pandemic, in March 2020, 3300 of 20 250 (16.3%) AI/AN households in rural Alaska lacked in-home plumbing, hindering hand hygiene.9,10 Residents of unpiped homes typically haul water from the community-treated watering point and store water in partially filled 32-gallon plastic buckets in the home. Self-hauling water means a limited and uncertain in-home water supply because of transportation needs, weather, climate-related changes to sources, storage capacity, and having physically capable family members or the financial means to hire someone to haul water.10-13 To wash hands, residents typically scoop water from the bucket into a bowl, or washbasin, before placing their hands in the water to wash.10-14 Often, residents reuse water to conserve the supply,10,11,15 a practice that increases exposure to pathogens.16,17
Studies have found associations between a lack of in-home plumbing and respiratory, skin, middle ear, and gastrointestinal infections in rural AI/AN communities.18-23 Hennessy et al 18 found that rates of water-washed disease (ie, diseases that hygienic practices such as handwashing contribute to preventing), specifically respiratory and skin infections, in communities with inadequate water and sanitation services were up to 5 times higher, particularly among young children (aged 3-6 y) and older adults (aged ≥65 y), than in rural communities with piped water service. Hicks et al 19 found an increased prevalence of middle-ear disease in rural unpiped AI/AN homes. Another study in Arizona found that the incidence of COVID-19 was 4 times higher in unpiped reservation homes than in homes with water and sewer service. 7
The COVID-19 pandemic renewed the urgency to increase health equity in unpiped AI/AN homes. In response, the Centers for Disease Control and Prevention (CDC) and the CDC Foundation partnered with the Alaska Native Tribal Health Consortium (ANTHC) to develop the Miniature Portable Alternative Sanitation System (Mini-PASS) handwashing station. We assessed the impact of the Mini-PASS on hand hygiene methods, whether households used the station for other uses, problems encountered during the 12 months after installation, and whether households were able to resolve those problems.
Methods
Mini-PASS Intervention
The Mini-PASS is a targeted intervention to improve health and quality of life by facilitating in-home handwashing and sanitation practices (Figure). It is a simplified version of the Portable Alternative Sanitation System (PASS), 24 an intermediate technology that makes moderate use of resources, materials, and technology compared with piped systems. The Mini-PASS includes a stand-alone handwashing station, a 20-gallon tank for protected water storage, and a vented bucket latrine known as a “vented honey bucket.” The handwashing station consists of a dual-sediment water filter (25 micron and 1 micron) with a gravity-fed faucet and sink that sit below the tank. The water drains into a 5-gallon wastewater bucket fitted with an overflow sensor and alarm, all contained in a cabinet.
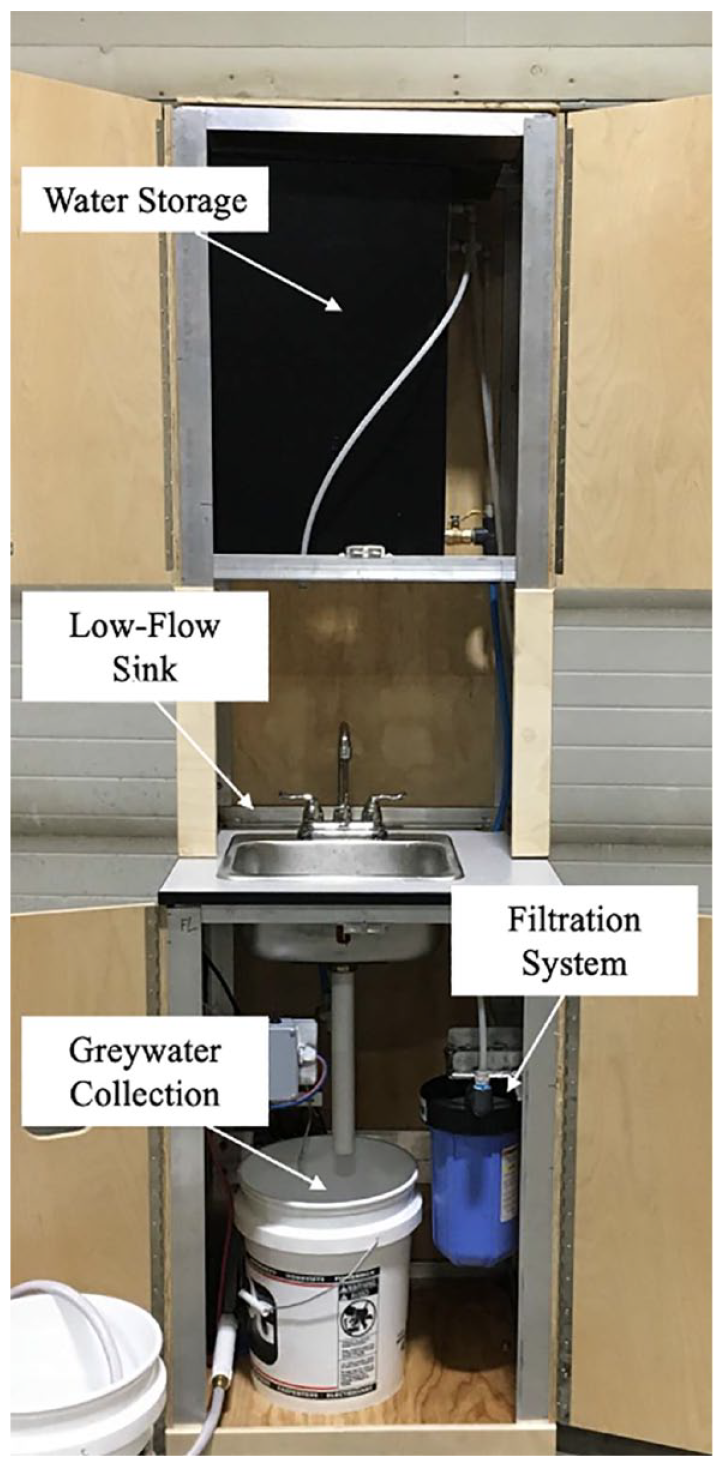
The Miniature Portable Alternative Sanitation System (Mini-PASS) handwashing station installed. The Mini-PASS is an intermediate-technology water and sanitation system that was installed in American Indian/Alaska Native households that lacked piped infrastructure as an affordable solution for handwashing during the COVID-19 pandemic, Alaska, 2021.
Community Engagement and Partnerships
ANTHC engineers designed these systems in partnership with AI/AN leaders in unpiped communities statewide to fill a gap for water and sanitation services that has persisted for decades. Community and household engagement in piloting and modifying the PASS began in 2016. Initial evaluation data indicated that it was economically feasible and reliable in challenging environmental conditions. 25 Households have used the PASS in every season (temperatures reaching as low as −40 °F), showing that it can be used in extreme environments (unpublished field notes, ANTHC, January 15, 2019).
ANTHC developed the Mini-PASS as a quick and affordable solution to the urgent needs posed by the COVID-19 pandemic. The Mini-PASS costs an average of $10 500 per household for materials and installation (paid for by the CDC Foundation and individual Tribal health organizations) and an additional $5 per month for operation and maintenance. Comparatively, piped systems may cost ≥$400 000 per home for materials and installation and an additional ≥$100 per month for operation and maintenance.
As part of the intervention, the Mini-PASS team provided homeowner training on how Mini-PASS works and how to make repairs and information on handwashing etiquette. Because of pandemic-related restrictions, in-person education was limited. Therefore, a sticker was placed on the handwashing station cabinet that outlined basic handwashing procedures. Other materials, such as a quick-start manual and troubleshooting manuals, were left with homeowners to answer commonly asked questions.
ANTHC partnered with CDC, the CDC Foundation, the Rasmussen Foundation, Christian Health Ministries Alaska, Silverline LLC, regional Tribal health organizations, and individual Tribes to install Mini-PASS units into 98 unpiped rural AI/AN households from February through December 2021. ANTHC coordinated installations in 10 communities in Interior, Northwestern, and Western Alaska by working with each region’s Tribal health organizations to select recipient communities. Each community’s Tribal council determined the priority of households that would receive the units, and most prioritized households with elders and/or young children. Households could decline Mini-PASS units or choose only 1 component for installation. By October 2022, the team had installed a total of 186 Mini-PASS units in 13 rural Alaskan communities.
This project was reviewed and approved by the Indian Health Service Alaska Area Institutional Review Board (FWA IRB00000636; protocol no. 2018-03-009-21). The protocol was also approved by the ANTHC Health Research Review Committee and the regional Tribal health organizations, Tanana Chiefs Conference, and Norton Sound Health Corporation. All 98 of the first Mini-PASS households were asked to participate in the evaluation study. The consent procedure included time to discuss the decision with their family, and potential participants were told that their decision would have no impact on services provided by ANTHC or the Mini-PASS project.
Recruitment and Data Collection
The team conducted semi-structured interviews by telephone before installation (preintervention) and at 3 follow-up intervals (postintervention). We based this longitudinal approach on the assumption that water use changes seasonally11-13 and to explore whether household handwashing station use changed over time. If unable to contact recipients before installation, researchers called within a month of installation to conduct a preintervention interview using the same questions as a preinstallation interview. Three-month postintervention interviews occurred between August and November 2021, around the time that community raw water sources began to freeze and water was collected from the washateria, a facility that offers services such as laundry, showers, flush toilets, and treated drinking water. Follow-up interviews occurred 6 to 9 months postintervention, coinciding with 2 of the coldest months (February and early April 2022). Final interviews occurred 12 months postintervention, from June through August 2022. Open-ended questions collected data on demographic characteristics, where people collected their water, volume of water collected, what they were using the water for, if there were any issues with the Mini-PASS system, if they were able to resolve those issues, their type of in-home sanitation, and what they were using for handwashing. A list of questions asked during the preintervention and postintervention interviews can be found in the Supplemental Material.
Study Population
Most residents in Mini-PASS recipient communities are Indigenous people from Alaska including Iñupiaq, Yup’ik, Athabascan, and Gwichin.3,26 All but 1 community is located off the road system and primarily reached by airplane. The median population size for these communities is 117, between 4 and 615 year-round residents.26,27 Community life centers around cultural and church celebrations, the school calendar, and subsistence activities. The median poverty rate for the communities in this study is 41% (range, 24%-100%), almost 4 times the average poverty rate for the United States (11%). 28 Most jobs available in these communities are in Tribal offices, schools, or construction, and many are seasonal.26,27
We interviewed 84 self-designated representatives of 71 households (13 households had >1 representative who was interviewed) from April 2021 through July 2022, representing 72.4% of the original 98 households that received Mini-PASS units during that period. Most interviewees (50 of 84; 59.5%) identified as female. The median (range) age of interviewees was 45 (19-80) years. We interviewed 41 respondents preintervention, 37 respondents 3 months postintervention, 40 respondents 6 to 9 months postintervention, and 27 respondents 12 months postintervention. Of these, 13 respondents were interviewed at all 3 postintervention interviews. Study staff attempted to contact all 98 households who received the Mini-PASS; however, some households did not have working telephones, were otherwise unreachable, or did not wish to participate.
Analysis
We coded responses to questions such as where people collected their water, volume of water collected, and how in-home sanitation and bathing were conducted into appropriate categories and then imported data into RStudio version 2023.06.1+524 (Posit Software) for analysis. We deductively created the category codes that were applied to the responses. We used summary statistics, such as number of participants, mean, maximum, minimum, and median, when appropriate, as a quantitative analysis approach to the data presented in the results.
Results
Impact of the Mini-PASS on Handwashing Method by Follow-up Time Frame
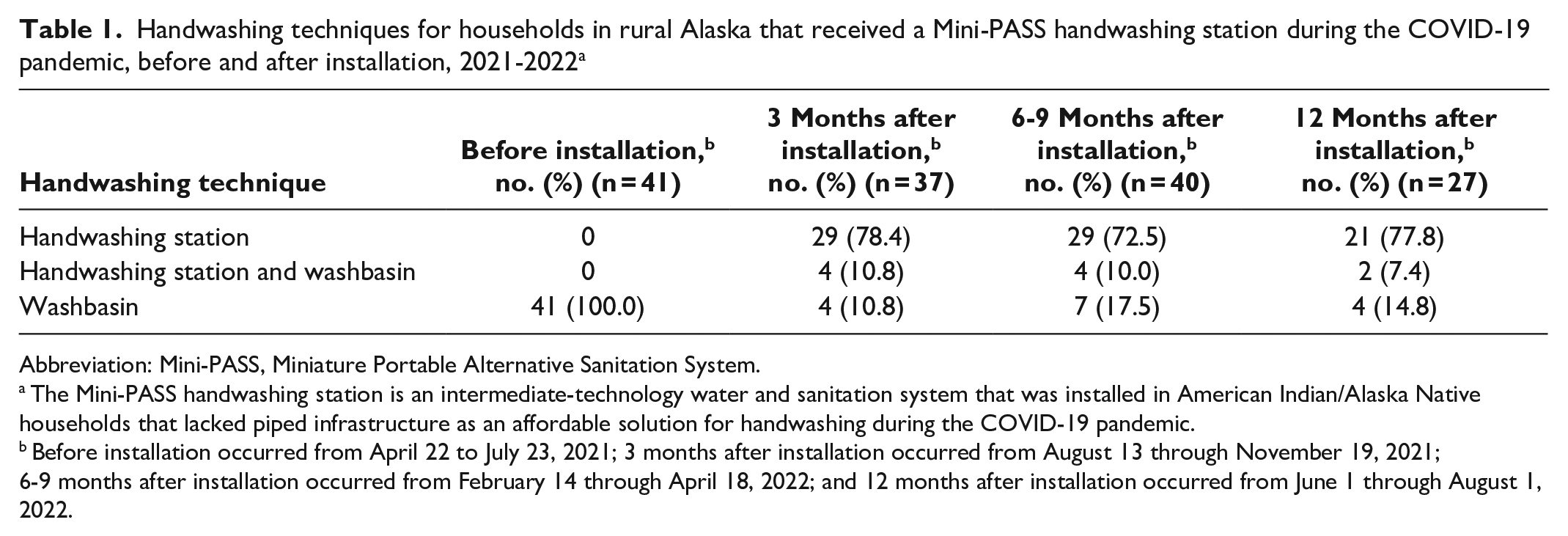
Preintervention, all participating households primarily used washbasins for handwashing (Table 1). During all 3 postintervention interviews, >70% of households reported using the Mini-PASS as their primary handwashing method.
Handwashing techniques for households in rural Alaska that received a Mini-PASS handwashing station during the COVID-19 pandemic, before and after installation, 2021-2022 a
Abbreviation: Mini-PASS, Miniature Portable Alternative Sanitation System.
The Mini-PASS handwashing station is an intermediate-technology water and sanitation system that was installed in American Indian/Alaska Native households that lacked piped infrastructure as an affordable solution for handwashing during the COVID-19 pandemic.
Before installation occurred from April 22 to July 23, 2021; 3 months after installation occurred from August 13 through November 19, 2021; 6-9 months after installation occurred from February 14 through April 18, 2022; and 12 months after installation occurred from June 1 through August 1, 2022.
Three months postintervention, 29 of 37 respondents (78.4%) reported using the handwashing station’s flow-through water as their only handwashing technique. Six to 9 months postintervention, 29 of 40 respondents (72.5%) reported using the handwashing station’s flow-through water as their only handwashing method. Twelve months postintervention, 21 of 27 respondents (77.8%) reported using the handwashing station’s flow-through water as their only handwashing method.
Of the 13 respondents interviewed in all 3 postintervention intervals, 4 had a different response about which handwashing method was used at each time point. Two of 13 respondents said they washed their hands with a washbasin at 3 months postintervention and only used the handwashing station 6 to 9 months postintervention and 12 months postintervention. One respondent indicated washing hands only with the handwashing station 3 months postintervention, using a washbasin as well at 6 to 9 months postintervention, and using the handwashing station at 12 months postintervention. One respondent only washed hands with the handwashing station at 3 months and 6 to 9 months postintervention but only used a washbasin at 12 months postintervention. Neither respondent who started using a washbasin at 6 to 9 months or 12 months postintervention reported having any issues with the handwashing station and chose not to use it because of “personal preference.”
Although every household we interviewed received a handwashing station, some respondents reported not using it at all: 4 of 37 respondents (10.8%) at 3 months postintervention, 7 of 40 respondents (17.5%) at 6 to 9 months postintervention, and 4 of 27 respondents (14.8%) at 12 months postintervention. When asked why they did not use the handwashing station, several respondents reported having a problem with the handwashing station, and several said it was because of “personal preference” or “habit.” For example, 1 respondent reported not using the handwashing station for fear of “wasting water” and wanting to use “heated water” in a washbasin.
Uses of Mini-PASS Handwashing Station Other Than for Washing Hands
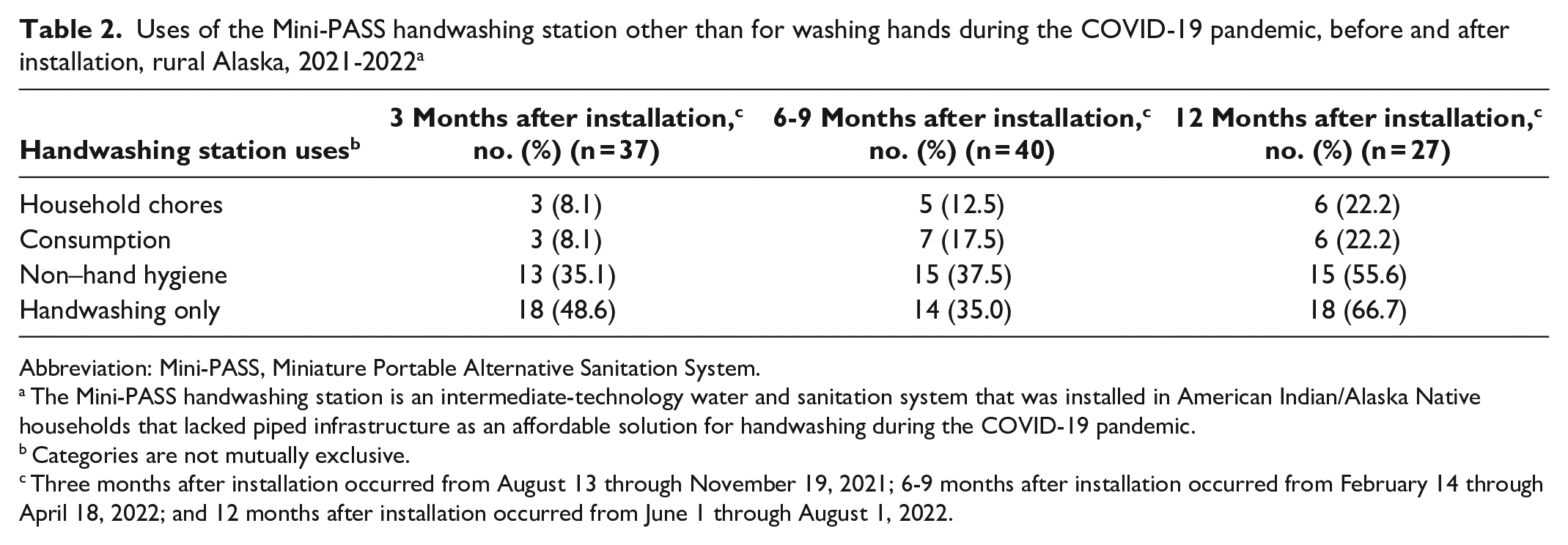
Eighteen of 37 respondents (48.6%) at 3 months postintervention, 13 of 40 respondents (32.5%) at 6 to 9 months postintervention, and 7 of 27 respondents (25.9%) at 12 months postintervention said that they used the handwashing station only to wash their hands (Table 2). Nineteen of 37 respondents (51.4%) at 3 months postintervention, 27 of 40 respondents (67.5%) at 6 to 9 months postintervention, and 20 of 27 respondents (74.1%) at 12 months postintervention reported using the handwashing station for at least 1 other task in addition to handwashing, including household chores (eg, washing dishes, scrubbing the floors), consumption (eg, cooking, drinking water), and general hygiene (eg, brushing teeth, washing up).
Uses of the Mini-PASS handwashing station other than for washing hands during the COVID-19 pandemic, before and after installation, rural Alaska, 2021-2022 a
Abbreviation: Mini-PASS, Miniature Portable Alternative Sanitation System.
The Mini-PASS handwashing station is an intermediate-technology water and sanitation system that was installed in American Indian/Alaska Native households that lacked piped infrastructure as an affordable solution for handwashing during the COVID-19 pandemic.
Categories are not mutually exclusive.
Three months after installation occurred from August 13 through November 19, 2021; 6-9 months after installation occurred from February 14 through April 18, 2022; and 12 months after installation occurred from June 1 through August 1, 2022.
Problems Reported With the Mini-PASS Handwashing Station
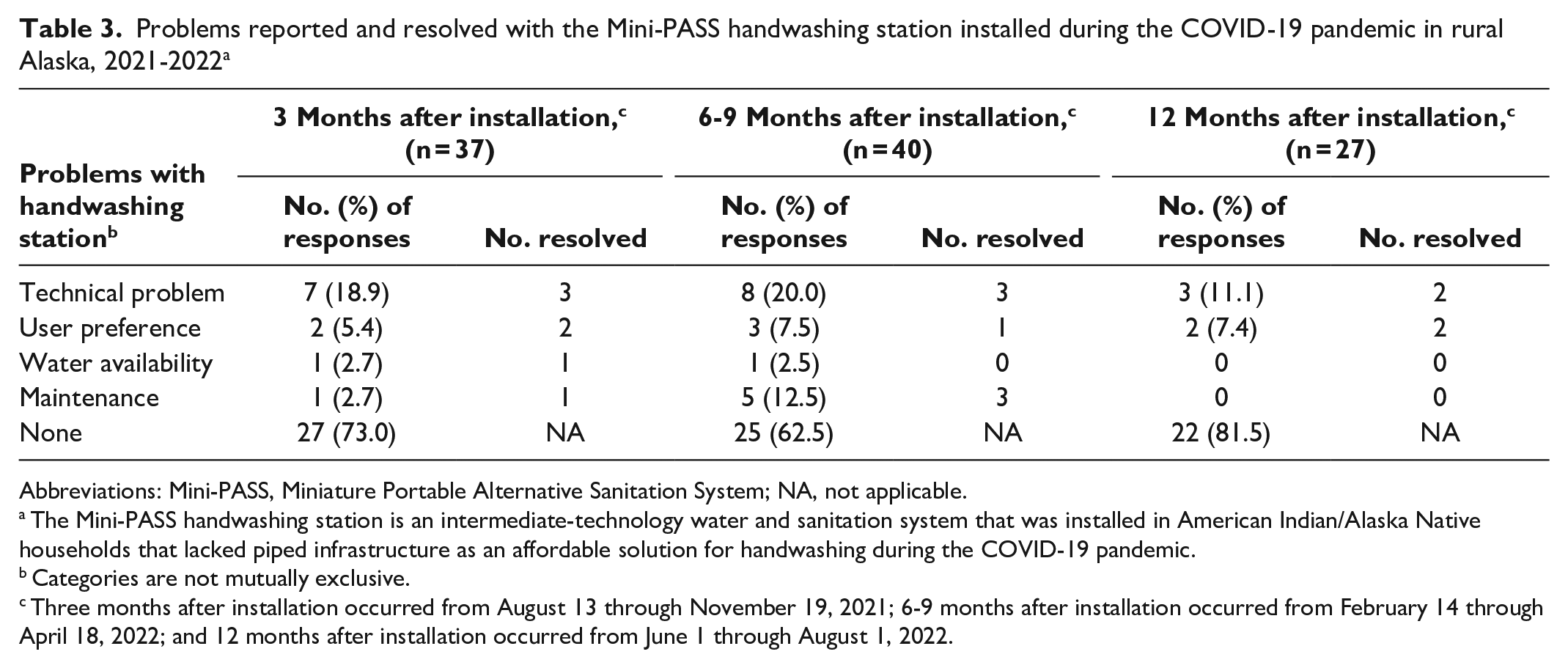
Most respondents reported having no issues with their handwashing station. However, 10 of 37 respondents (27.0%) at 3 months postintervention, 15 of 40 respondents (37.5%) at 6 to 9 months postintervention, and 5 of 27 respondents (18.5%) at 12 months postintervention reported having at least 1 problem with their handwashing station (Table 3). Issues included mechanical problems (eg, issues with the alarm or pump), unmet needs or preferences (eg, wanting a bigger sink or storage cabinet, the flow of the water being too slow), water availability, and maintenance problems (eg, the sink drain clogging, mold, the faucet dripping). Of the problems reported, the only issue that was tied to changes in the season was the pump breaking. During the winter months (6 to 9 months postintervention), 4 respondents reported pumps “cracking” due to water freezing inside the pump. Six of 10 respondents at 3 months postintervention and 7 of 15 respondents at 6 to 9 months postintervention who reported having issues with their handwashing station resolved their problems themselves. For example, 1 respondent reported trouble with the sink draining but resolved it by cleaning out the soap buildup in the drain. Three of 4 respondents at 12 months postintervention who used the handwashing station reported having a problem with their handwashing station that they resolved on their own.
Problems reported and resolved with the Mini-PASS handwashing station installed during the COVID-19 pandemic in rural Alaska, 2021-2022 a
Abbreviations: Mini-PASS, Miniature Portable Alternative Sanitation System; NA, not applicable.
The Mini-PASS handwashing station is an intermediate-technology water and sanitation system that was installed in American Indian/Alaska Native households that lacked piped infrastructure as an affordable solution for handwashing during the COVID-19 pandemic.
Categories are not mutually exclusive.
Three months after installation occurred from August 13 through November 19, 2021; 6-9 months after installation occurred from February 14 through April 18, 2022; and 12 months after installation occurred from June 1 through August 1, 2022.
Discussion
Access to a handwashing station with a functional water tap is one of the main determinants of effective hand hygiene.29-31 Scholars working in low- and middle-income communities found that in infrastructure-restricted communities, in-home handwashing stations improved hand hygiene.32,33 Our results indicated that the Mini-PASS shifted household handwashing from the washbasin to flowing water. Before receiving a Mini-PASS unit, all participating households indicated using a washbasin for hand hygiene. In all of the postintervention periods, more than 70% of interviewees reported that their household primarily used the handwashing station’s flow-through water to wash their hands.
While the health benefits of handwashing are commonly accepted,33-36 handwashing interventions are often hampered by inadequate access to handwashing supplies (eg, clean water, soap, towels) and facilities. Previous studies have shown that having a place for handwashing that has a functional tap is the “strongest structural determinant of effective overall handwashing technique.” 37 Guides such as “Community Handwashing Guide: Utilizing Available Resources to Initiate a Handwashing Intervention” state that access to physical handwashing resources in communities regardless of socioeconomic status is vital. 38 The availability and functionality of a handwashing station is crucial for safe and effective handwashing. Maintaining safe and reliable handwashing stations is difficult in settings that lack infrastructure, capacity, and access to clean water. Systems such as the Mini-PASS are a low-cost, effective alternative to piped systems. Other handwashing stations such as the Autarky, an on-site system that treats and recycles water for handwashing and toilet flushing, also show that niche interventions can be successful in informal settlements (ie, housing that does not comply with the local requirements for traditional housing) when they are culturally and environmentally appropriate. 39 Similar to the Autarky, the Mini-PASS was produced with community members, leading to high acceptability among homeowners.
Our results also showed an increasing number of households used water from the handwashing station for tasks other than washing hands (51.4%, 67.5%, and 74.1% at 3 months, 6 to 9 months, and 12 months postintervention, respectively). This finding indicates that more people are incorporating the handwashing station into other aspects of their daily routine, likely due to the convenience of in-home access to running water. Others have found that the ability to easily access water inside the home can facilitate increased water use,25,32,33,40,41 and incorporating the protected water storage and tap into areas beyond handwashing may increase in-home water use, health, and quality of life.
In their discussion of the principles of water, sanitation, and hygiene interventions, Sutherland et al 39 emphasized the importance of working with communities to ensure the intervention is environmentally appropriate. Other studies have demonstrated the importance of an environmentally appropriate handwashing station to facilitate use. For example, Bai et al 42 found that changing the handwashing environment, such as lighting and surface composition, can alter handwashing behavior. The PASS and eventually the Mini-PASS included a handwashing station that had a cabinet, faucet, and sink that was environmentally appropriate and encouraged its use.
Our data indicate high levels of use and few problems. Most homeowners we interviewed had no issues with the handwashing station, and respondents who reported problems had issues that were resolved quickly. This finding underlines the need to provide maintenance support for engineered interventions after an intervention has been installed. Equity in public health interventions means that populations that are the most vulnerable to water-washed diseases can get support to benefit from those interventions.
Applications in Other Communities
Although the Mini-PASS was designed for homes in rural Alaska, it could be implemented in communities around the world that lack reliable piped water. In rural Alaska, while access to safe and reliable water is not always available, electricity is subsidized. The PASS and the Mini-PASS were built with these conditions in mind. For example, the handwashing station does not rely on constant electricity to use because it is gravity fed and can rely on a battery for pumping water to the holding tank during power outages. This feature could make the Mini-PASS useful in urban areas that experience rolling blackouts. For example, since 2007, the power grid in South Africa has been mismanaged, which has led to the inability of the country to deliver as much power as demanded. This mismanagement has led to rolling blackouts, in which electricity delivery is stopped for a time in various regions of the country. 43 Along with power supply issues, South Africa is also experiencing a water crisis and asking its citizens to conserve water use. 44 The Mini-PASS would be an appropriate solution to ensure that clean water is flowing in homes that have limited water and electricity. The Mini-PASS could also be useful in war-torn countries such as Ukraine, where active missile attacks have damaged substantial sections of the country’s power grid. 45 Besides being functional with limited electricity, the mini-PASS also offers a sense of normalcy as the cabinet is bolted to the ground and is comparable to handwashing facilities that rely on a piped water system.
Limitations
Our study had 2 limitations. First, our findings were limited by the fact that only 13 of the 71 participating households were interviewed in all 3 postintervention periods. As such, we were unable to conduct statistical analyses of trends over time. Second, because of pandemic-related travel restrictions, all follow-up data were collected remotely, and the scope of this assessment was limited to self-reported handwashing methods (ie, washbasin, handwashing station, or other).
Conclusions
For future applications of the Mini-PASS in low-resource communities, active communication with the community about what the system is, how it works, and how it is installed will be needed. It will also be necessary to have in-person interactions with homeowners that include more training about how to use and repair the system. Households that incorporate the Mini-PASS should be required to have at least 1 representative participate in trainings provided by ANTHC at no cost. Communities would benefit from an infrastructure that could provide replacement parts with their systems locally.
Proper handwashing is essential for closing gaps in health disparities. Providing running water for washing hands via an in-home facility such as the Mini-PASS can improve hand hygiene for households without piped water. Future research should be conducted to evaluate the health impact of improved handwashing behaviors provided via the Mini-PASS.
Supplemental Material
sj-xlsx-1-phr-10.1177_00333549241255260 – Supplemental material for Impact of In-Home Handwashing Stations on Hand Hygiene During the COVID-19 Pandemic in Unpiped Rural Alaska Native Homes
Supplemental material, sj-xlsx-1-phr-10.1177_00333549241255260 for Impact of In-Home Handwashing Stations on Hand Hygiene During the COVID-19 Pandemic in Unpiped Rural Alaska Native Homes by Olivia A. Harmon, Tricia S. Howe, Jacqualine D. Schaeffer, Ramot Adeboyejo and Laura P. Eichelberger in Public Health Reports
Footnotes
Acknowledgements
The authors respectfully acknowledge that we work on the Indigenous lands of Alaska Native peoples and thank the Tanana Chiefs Conference and Norton Sound Health Corporation for their collaboration. We thank the CDC Foundation and the Robert Wood Johnson Foundation for funding this work. We thank Climate Solutions and Silverline LLC for their work on this project. In addition to the authors Harmon, Howe, and Schaeffer, interview data and notes were collected by Julia Phelan, Zoe Merritt, Stefani Martinez, and Kari Pedersen. We thank Troy Ritter, PhD, and John Warren, PE, who greatly improved this work by reviewing the article and offering their expertise. We also thank the homeowners and communities that participated in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the CDC Foundation (grant no. 1085.38) and the Robert Wood Johnson Foundation (grant no. 76579).
Underlying Research Material
The underlying research materials for this article can be accessed by contacting Dr. Laura P. Eichelberger at
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.