
Abstract
In March 2020, a Tribal telehealth program—the Indian Country Extension for Community Health Outcomes (ECHO)—added emergency COVID-19 to its programming to support the pandemic response. A long-standing relationship with a network of Indian Health Service, Tribal, and urban Indian clinicians supported a rapid launch of the COVID-19 telehealth program. This nationwide service offered primary care clinicians and staff serving American Indian/Alaska Native people access to virtual learning opportunities, expert clinical recommendations, technical assistance, and capacity building. From March 12, 2020, through April 30, 2021, the program provided 85 clinical sessions in 12 months, with an average participation of 120 attendees per clinic (N = 11 710). Attendees could complete a voluntary evaluation form for each session via an online link. A total of 2595 forms were completed. Attendees came from 33 states and 206 unique locations, primarily from the Pacific Northwest (n = 931, 35.9%). Most pharmacists (78.1%), providers (ie, medical doctor, doctor of osteopathy, advanced practice nurse, physician assistant, or clinical nurse midwife; 70.8%), and nurses (59.6%) gave the sessions the highest rating of “very satisfied.” The highest proportion of attendees indicating that they planned a change in practice were pharmacists (68.0%), nurses, (64.1%), and providers (61.3%). Most attendees (93.1%) said that the COVID-19 sessions gave them a sense of social support. Lessons learned were that (1) a telehealth platform can be quickly retasked for emergency response with no further delays, (2) a telehealth network can be scaled up quickly with participation from preexisting relationships, and (3) the platform is flexible and adaptable to the needs of participants. An existing telehealth program can be a key part of timely, relevant, large-scale emergency readiness and response efforts.
The COVID-19 pandemic reached emergency status in early 2020. During the next year, the official guidance on COVID-19 disease, including transmission and treatment, underwent large and frequent changes as new studies added new information.1,2 Health care systems underwent rapid changes in policy and practice on telemedicine and telehealth. COVID-19–related medical care and the continuity of provision of primary and specialty care were adapted for delivery via virtual platforms.3-6 Telehealth was also adapted to be a core part of emergency medical response to reach health professionals with relevant and accurate COVID-19–related updates, as general policies and clinical guidance had to be locally interpreted for implementation.7,8 For example, long-standing infrastructure limitations imposed constraints on internet and telephone service among certain populations, such as rural health care workers and patients. 9 Specifically, American Indian/Alaska Native (AI/AN) populations, which have a high proportion of rural members, had an elevated rate of hospitalizations and deaths from COVID-19, adding urgency to the emergency response for Tribal Nations and the Indian Health System.10,11
Nationally, the Indian Health System comprises federal, Tribal, and urban health facilities that collectively serve an estimated 2.6 million AI/AN people, 12 mostly in rural health facilities located far from specialists. This health system has been well documented to be severely underresourced in monetary and human resources.13,14
Purpose
In early 2020, as the severity of the COVID-19 pandemic became clear, the Northwest Portland Area Indian Health Board (NPAIHB) redeployed resources to rapidly provide a national platform for emergency response supporting Tribal Nations. The purpose of this case study was to (1) detail the adaptation of an established telehealth network to rapidly respond to a public health emergency at scale without additional resources and (2) document lessons learned. While the use of telehealth to provide medical services to conform with social distancing policies is well documented, to our knowledge, this case study is the first to document a telehealth program centered on COVID-19 content for Tribal Nations.
Methods
The Northwest Tribal Epidemiology Center, housed at NPAIHB, hosts telehealth services as part of its Indian Country Extension for Community Health Outcomes (ECHO) program. 15 Indian Country refers to any of the many self-governing AI/AN communities throughout the United States. As a legal category, Indian Country includes Indian reservation lands, Indian communities within the borders of the United States, and Indian allotments/titles (which have not been extinguished). This nationwide telehealth service offers primary care clinicians and staff serving AI/AN people access to virtual learning opportunities, expert clinical recommendations, technical assistance, and capacity building. The program offers regular virtual sessions: interactive online learning environments where clinicians, Tribal leadership, public health professionals, and other staff members who serve AI/AN patients can connect with peers, engage in didactic presentations, collaborate on complex case consultations, and receive mentorship from clinical experts and peers from across Indian Country to deliver high-quality health care in their communities. The model demonstrated equal efficacy to in-person specialist care for hepatitis C virus (HCV) treatment, 16 and facilities participating in the Tribal HCV ECHO had a significantly higher rate of ordering HCV medications than facilities that did not participate. 17
Since 2017, Indian Country ECHO programs have been expanded to meet clinical demand in scope and frequency. These ECHO programs serve clinicians and staff working in the Indian Health System and include topics such as HCV, substance use disorder, and other health topics. The programs offer virtual ECHO sessions, which are regularly scheduled videoconferencing sessions that include a small team of specialists and administrative/technical support staff (the “hub”) and learners (10-20 health facilities, or “spokes,” within the Indian Health System), who engage in didactic presentations and case-based learning.
To respond to COVID-19 and with the goal of reaching a large audience working mainly in remote regions across the entire Indian Health System, the ECHO program mounted a new series on COVID-19. For faculty, the ECHO program collaborated with infectious disease specialists from its long-standing HCV and HIV telehealth programs. These faculty were also at the forefront of the COVID-19 response in the Indian Health System and allotted time to lead COVID-19 ECHO sessions. To promote attendance from the Indian Health System, invitations to join the new COVID-19 sessions were sent to the entire database of Indian Country ECHO attendees. In addition, participation was strongly encouraged by NPAIHB leadership in meetings, emails, and other communications.
The telehealth team adapted a new format for the COVID-19 ECHO clinic. The new format emphasized presentations from multiple experts rather than the usual short didactic presentation. Participants could not submit case presentations for consultation, but time was allotted for questions from attendees, going beyond the allotted time or following up by email if necessary. COVID-19 ECHO sessions were offered twice per week and are ongoing. There was no set syllabus; faculty chose COVID-19 topics for each ECHO clinic based on urgency, usefulness, and needs identified by participants. To accommodate as many time zones as possible, the sessions were given at midday Mountain Standard Time and recorded for participants to view on demand.
To streamline attendance, preregistration was not required. The COVID-19 ECHO teams solicited evaluations during each session. A weblink to a standardized evaluation form was posted at the end of each clinic. Evaluation forms requested information on the professional licensure and location (facility name, city, state) of participants, as well as the participant’s satisfaction with the clinic and its relevance. Satisfaction questions were measured on a 4-point Likert scale (1 = very unsatisfied, 4 = very satisfied) or a scale of 1 (not at all likely) to 10 (extremely likely). The survey also asked participants if they were likely to change their practice as a result of the session, with a scale of 1 (very unlikely) to 4 (very likely). The change-of-practice question allowed space to add optional free-text entries. Participation was voluntary. We collected and analyzed all data using Microsoft Excel. The NPAIHB Institutional Review Board reviewed and cleared the results for publication.
Outcomes
The first COVID-19 ECHO session launched on March 12, 2020, within a week of initial planning. The hub conducted 85 sessions from March 12, 2020, through April 30, 2021, with a mean of 120 attendees per session (N = 11 710). The content of the COVID-19 ECHO sessions varied widely and included testing, nonpharmaceutical interventions, infection control and transmission, and treatment.
In addition to facilitating virtual attendance, the ECHO program hosts a resource page where COVID-19 presentation slides and recordings are available for viewing or download; this resource page logged 25 670 visits during the study period.
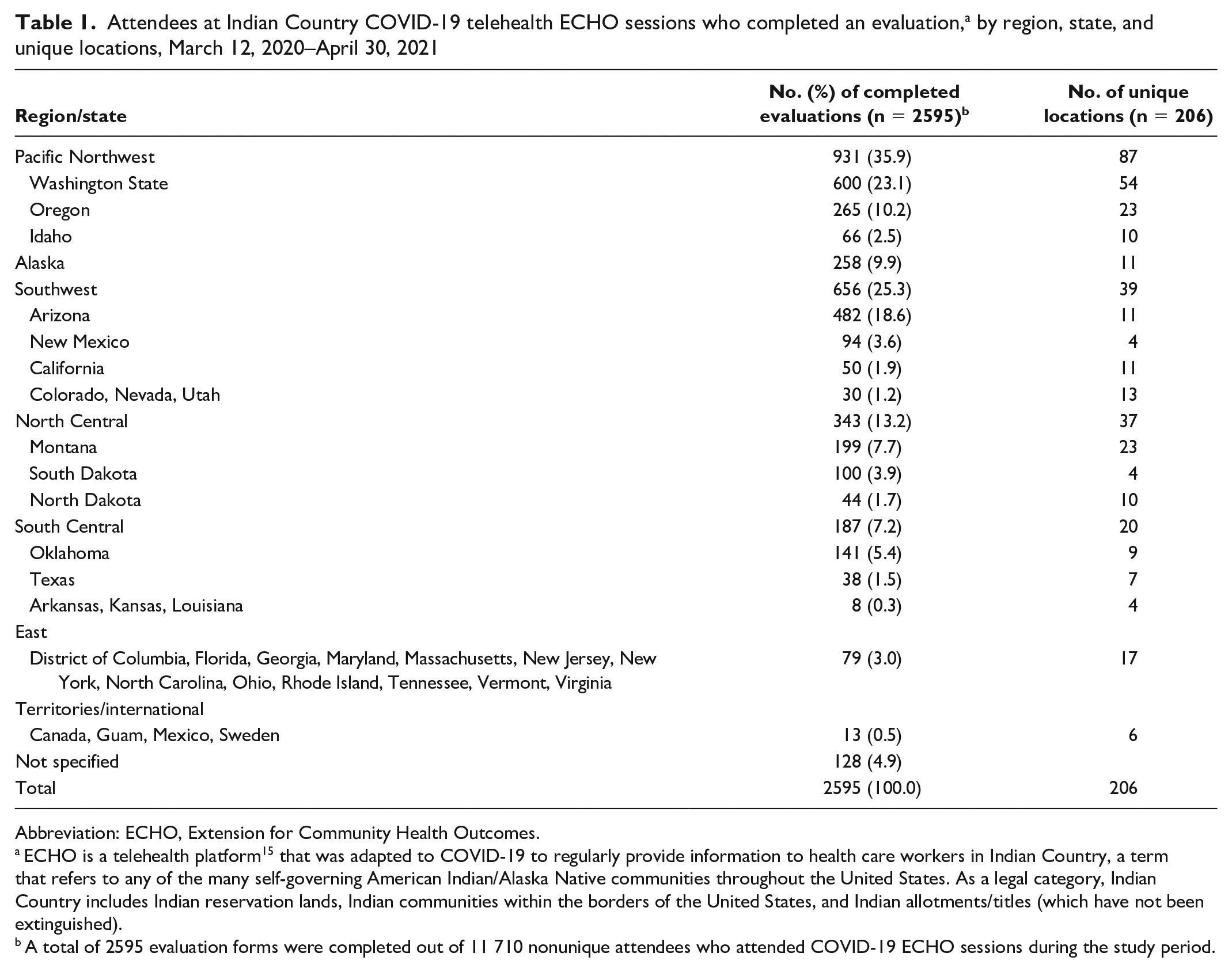
Participants completed 2595 evaluations. COVID-19 ECHO participants were from 206 unique locations in 33 states (Table 1). By state, the highest proportion of evaluations were returned from Washington State (n = 600, 23.1%), Arizona (n = 482, 18.6%), Oregon (n = 265, 10.2%), Alaska (n = 258, 9.9%), and Montana (n = 199, 7.7%).
Attendees at Indian Country COVID-19 telehealth ECHO sessions who completed an evaluation, a by region, state, and unique locations, March 12, 2020–April 30, 2021
Abbreviation: ECHO, Extension for Community Health Outcomes.
ECHO is a telehealth platform 15 that was adapted to COVID-19 to regularly provide information to health care workers in Indian Country, a term that refers to any of the many self-governing American Indian/Alaska Native communities throughout the United States. As a legal category, Indian Country includes Indian reservation lands, Indian communities within the borders of the United States, and Indian allotments/titles (which have not been extinguished).
A total of 2595 evaluation forms were completed out of 11 710 nonunique attendees who attended COVID-19 ECHO sessions during the study period.
COVID-19 ECHO sessions reached a range of health care professionals. Evaluations were completed by providers (n = 1262, 48.6%), nurses (n = 642, 24.7%), and pharmacists (n = 316, 12.2%). The category of providers comprised medical doctor/doctor of osteopathy (56.7%), advanced practice nurse (27.2%), physician assistant (15.8%), clinical nurse midwife (0.2%), behavioral health professional (1.4%), nursing aide/medical assistant and peer educator (0.8%), and other health professional (11.9%). Attendees classified as other health professional (n = 311) included dental (n = 129, 41.4%), substance use counselor (n = 26, 8.4%), health information technologist/analyst (n = 16, 5.1%), and other (eg, Tribal health board chair, optometrist, emergency response coordinator; n = 140, 45.0%).
Completed evaluations indicated that most attendees were very satisfied (66.2%) or satisfied (31.6%) and few attendees were unsatisfied or very unsatisfied (1.8%). By licensure, most pharmacists (78.1%), providers (70.8%), and nurses (59.6%) indicated that they were very satisfied with the sessions. Analysis did not show any patterns of satisfaction by topic, session, or presenter. Most attendees (93.1%) responded that the COVID-19 clinics gave them a sense of social support.
By licensure, attendees from all clinical categories rated the COVID-19 clinics a 9 or 10 on a scale of 1 to 10 (Table 2). In all clinical categories, most attendees stated that they were very likely or likely to make a change in clinical practice: pharmacists (68.0%), providers (64.1%), and nurses (61.5%).
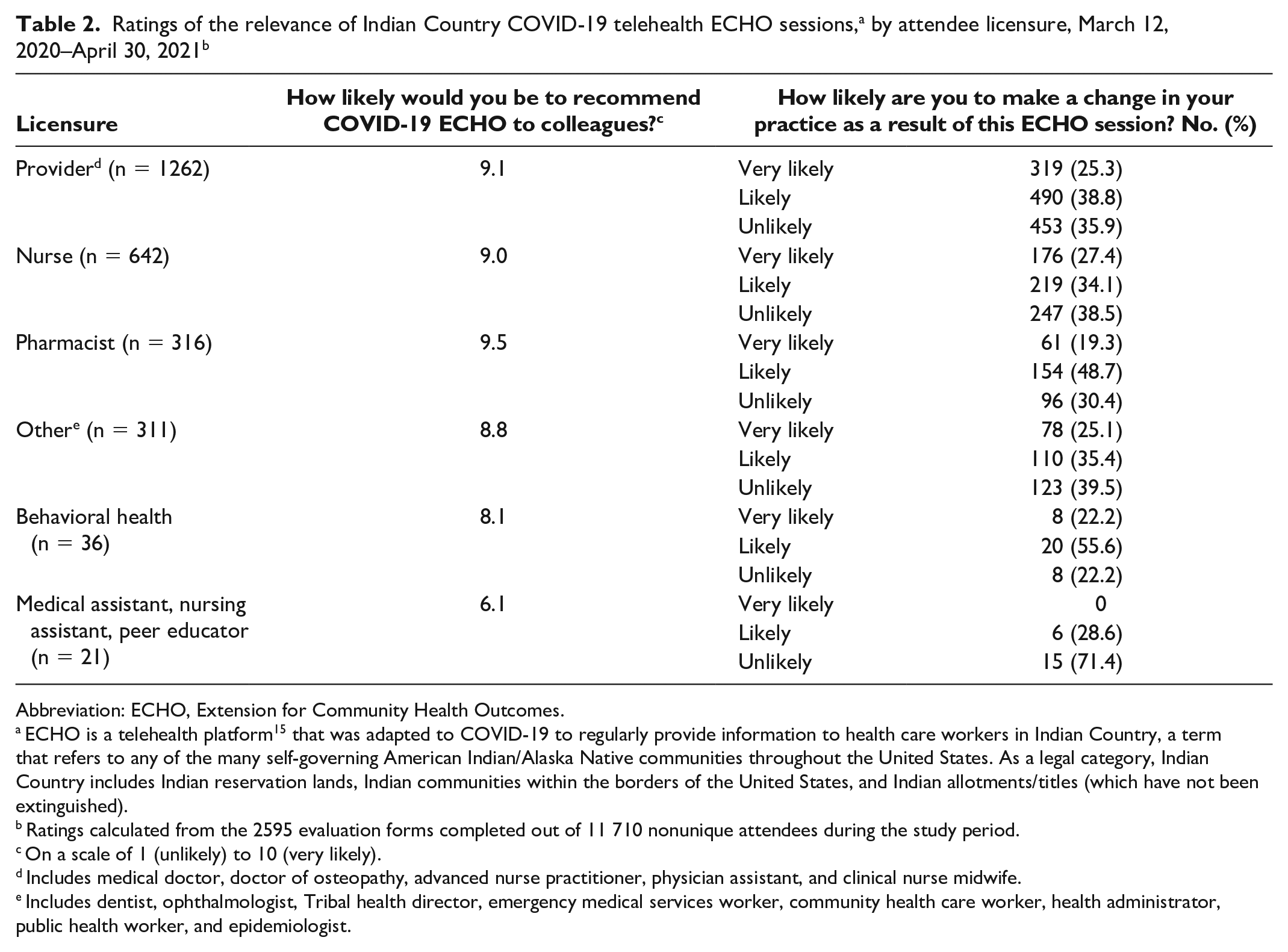
Abbreviation: ECHO, Extension for Community Health Outcomes.
ECHO is a telehealth platform 15 that was adapted to COVID-19 to regularly provide information to health care workers in Indian Country, a term that refers to any of the many self-governing American Indian/Alaska Native communities throughout the United States. As a legal category, Indian Country includes Indian reservation lands, Indian communities within the borders of the United States, and Indian allotments/titles (which have not been extinguished).
Ratings calculated from the 2595 evaluation forms completed out of 11 710 nonunique attendees during the study period.
On a scale of 1 (unlikely) to 10 (very likely).
Includes medical doctor, doctor of osteopathy, advanced nurse practitioner, physician assistant, and clinical nurse midwife.
Includes dentist, ophthalmologist, Tribal health director, emergency medical services worker, community health care worker, health administrator, public health worker, and epidemiologist.
A total of 509 (40.1%) evaluations described in a free-text format the changes that health care providers planned to make; of these, 66.9% (n = 337) specified topics that could be categorized. Of these topics, the most frequently cited changes in practice were SARS-CoV-2 testing (24.3%), use of COVID-19 recommendations (19.1%), SARS-CoV-2 vaccination (14.1%), infection control and nonpharmaceutical interventions (10.9%), COVID-19 treatment (9.1%), patient education (7.6%), plans and policies (5.9%), telemedicine use (4.9%), and contact tracing (2.1%). Conversely, 467 (37.0%) evaluations stated why health care providers were unlikely to make a change in practice. The most frequently cited reasons were that the change had already been implemented (47.1%) and the change was not possible in their clinical role (37.3%).
Lessons Learned
The ECHO program responded with timely and relevant COVID-19 support at scale for health care professionals in the Indian Health System. When compared with the ECHO program before the COVID-19 pandemic, the ECHO program during the pandemic had more attendees, a larger geographic scope, and higher rates of use of ancillary online resources. The number of COVID-19 ECHO sessions (n = 85) was nearly double the number of the most frequent pre–COVID-19 ECHO sessions (HCV, n = 45), and the mean number of attendees at COVID-19 ECHO sessions was >8 times higher than for HCV ECHO sessions. The number of visits to online resources during the study period was approximately 2.7 times higher than pre–COVID-19.
These results suggest that existing telehealth networks can be a key part of health systems’ emergency readiness and response. The ECHO telehealth network was able to rapidly meet the dynamic challenges presented by the COVID-19 pandemic with no additional resources. Trusted relationships with clinicians created during years of telehealth services and clear messaging from regional Tribal leadership resulted in high levels of participation from the outset. The telehealth hub team was highly adaptable; all members were cross-trained in supportive administrative roles and had experience working virtually or off-site before COVID-19.
The telehealth attendees were mainly providers but included other clinicians and nonclinical staff. Evaluations suggest that clinical attendees who were not providing direct care and nonclinical attendees may have found slightly less value in the content than other attendees. A high proportion of clinicians found the telehealth sessions useful and planned to make a change to clinical practice. While most clinicians were very satisfied with the COVID-19 ECHO clinics, differences by licensure may indicate the potential for improvement—for example, providing more targeted content for specific roles, such as a clinician in primary care or a hospital or health care workers in charge of infection control policies.
One key characteristic of the COVID-19 pandemic was the vast amount of clinical data being generated worldwide as providers attempted to understand their experiences and report via peer-reviewed literature what seemed to work and what did not work. Keeping up with this ever-changing knowledge base was a challenge for ECHO faculty and attendees. In addition, frequently updated interim recommendations from the Centers for Disease Control and Prevention, the World Health Organization, and other organizations made it difficult to consider many clinical findings and recommendations as being worthy of immediate implementation. This context may help explain why gaining knowledge and appreciating the support of others facing the same clinical dilemmas were described more often than implementing clinical changes. Another possible explanation for not implementing clinical changes was that only hospitals initially had the capacity for monoclonal antibody treatment for COVID-19, but a high proportion of facilities in the Indian Health System are primary care clinics.
The evaluation data had several limitations. First, the data represent only attendees who completed an evaluation, which may skew satisfaction results higher. Second, more evaluations were completed early in the year, which may indicate evaluation fatigue among respondents and may have affected which topics were deemed most clinically useful. Third, we were unable to determine why some attendees participated in only a few sessions. Specific outreach to attendees who participated in only a few sessions or a needs assessment might benefit future ECHO clinic planning. Finally, attendees were anonymous and could complete an evaluation at each clinic. As such, respondents who regularly completed evaluations may have been overrepresented. Geographic bias also exists in the profile of our attendees. The telehealth hub has the most contacts in the Pacific Northwest, which had the highest representation. Other regions may be underrepresented because outreach efforts were not disseminated effectively to potential participants, scheduling restraints, or use of other webinars or sources of COVID-19 information.
The learning phase of COVID-19 response is not yet over, and COVID-19 ECHO may be called on to adapt again. The COVID-19 ECHO will continue to seek the optimal collaborative learning environment as new variants appear, new therapeutics become available, and new data on vaccines and immunity emerge.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Mera has been principal investigator in COVID-19 clinical trials sponsored by Gilead and Merck at Cherokee Nation Health Services.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support came from the US Department of Health and Human Services Minority HIV/AIDS Fund through the Indian Health Service and the Robert Wood Johnson Foundation.