
Abstract
Objectives:
The launch of state certification for community health workers (CHWs) in Massachusetts in 2018 aimed to promote and champion this critical workforce. However, concerns exist about unintentional adverse effects of certification. Given this, we conducted 2 cross-sectional surveys to evaluate this certification policy.
Methods:
We conducted surveys of CHW employers and CHWs in 3 sample frames: community health centers and federally qualified health centers, acute-care hospitals, and community-based organizations. We administered the surveys in 2016 (before certification launch) and 2021 (after certification launch) to answer the following questions: Was certification associated with positive outcomes among CHWs after its launch? Did harmful shifts occur among the CHW workforce and employers after certification launch? Was certification associated with disparities among CHWs after its launch?
Results:
Certification was associated with higher pay among certified (vs noncertified) CHWs, better perceptions of CHWs among certified (vs noncertified) CHWs, and better integration of certified (vs noncertified) CHWs into care teams. We found no adverse shifts in CHW workforce by sociodemographic variables or in CHW employer characteristics (most notably CHW employer hiring requirements) after certification launch. After certification launch, certified and uncertified CHWs had similar demographic and educational characteristics. However, certified CHWs more often worked in large, clinical organizations while uncertified CHWs most often worked in medium-sized community-based organizations.
Conclusions:
Our evaluation of Massachusetts CHW certification suggests that CHW certification was not associated with workforce disparities and was associated with positive outcomes. Our study fills a notable gap in the research literature and can guide CHW research agendas, certification efforts in Massachusetts and other states, and program efforts to champion this critical, grassroots workforce.
Community health workers (CHWs) leverage their unique understanding of the experience, language, and culture of the communities they serve to carry out several public health functions, such as health education, outreach, advocacy, and linkage to community resources.1-3 Known by various job titles and working in diverse settings, CHWs provide a multitude of services and are increasingly recognized as a key component of clinical and community-based public health efforts.1-3
With the growing recognition of CHWs among research, health care, and legislative audiences, voluntary certification has been raised by many advocates as a means of promoting and sustaining the workforce.4-13 Anticipated benefits of CHW certification include clarifying CHWs’ scope and role, increasing employer engagement and recognition of CHWs, better integrating CHWs into clinical care teams, promoting career advancement, and increasing salaries.4-6,14 However, concerns exist about unintentional adverse effects of certification, such as employers requiring certification for hire, inequitable access to certification, decreased workforce diversity, and certification threatening CHW identity.4-6,15,16 Furthermore, requiring certification may marginalize uncertified CHWs and create barriers to practice.4,14,16
In Massachusetts, legislation in 2010 initiated the creation of a voluntary certification process for CHWs through the establishment of the Massachusetts Board of Certification of CHWs, which at a minimum must have 4 CHWs serving of its 11 members.17-19 During the next decade, the Massachusetts Board of Certification of CHWs (with input from the Massachusetts Department of Public Health [MDPH] Office of CHWs and members of the CHW workforce) designed 2 avenues of voluntary certification: (1) the work experience pathway, which launched in October 2018, will likely sunset in July 2025 and requires that the CHW has accrued 4000 hours of work experience as a CHW and (2) the combined training and work experience pathway, which launched in July 2021 and requires 2000 hours of CHW work experience and the successful completion of a Massachusetts Board of CHWs–approved training program. 20
Massachusetts CHW certification aimed to impart numerous benefits, including increased pay, improved perceptions and recognition, more advancement opportunities, and increased care team integration.4-6,14 However, given that the full ramifications of certification were unknown and to mitigate disparities developing in the CHW workforce due to certification, before certification launch, the MDPH Office of CHWs designed with partners a programmatic approach to champion the entire Massachusetts CHW workforce (Supplement 1). This approach includes offering technical assistance and developing core competency training (which is recommended for all CHWs).
Research is limited on the positive and potential adverse effects of state CHW certification. To evaluate Massachusetts CHW certification, we implemented the Massachusetts CHW Workforce Surveys. 21 These surveys answer 3 research questions. First, because the goal of CHW certification in Massachusetts is to benefit the workforce, we assessed whether certification was associated with positive outcomes for CHWs after certification launch in 2018. We contrasted, by certification status, metrics intended to be associated with certification: increased pay, perceptions and recognition, and advancement opportunities. Due to the appeal of CHW certification in credential-oriented health care settings, we assessed the integration of CHWs into clinical care teams among CHWs in clinical organizations.4,5,22-24 Second, mitigating the development of workforce disparities due to certification was a major programmatic focus. To evaluate this aspect of certification, we assessed whether CHW employers were requiring certification for potential hires and whether declines occurred in the sociodemographic diversity of the CHW workforce after certification launch. Third, we assessed whether being certified differed by race, ethnicity, language, or other sociodemographic characteristics after certification launch; such differences may indicate developing workforce disparities.
Methods
Sample Frame, Survey Administration, and Weighting
The methods used in the development, administration, and statistical analysis of the Massachusetts CHW Workforce Surveys are described elsewhere. 21 We conducted outreach to identify CHWs and CHW employers in Massachusetts in 3 sample frames based on previous findings indicating where CHWs are likely to be employed: community-based organizations (CBOs), all community health centers and federally qualified health centers in Massachusetts (hereinafter, health centers), and all acute-care hospitals in Massachusetts. 25 We identified 871 CHWs and 298 CHW employers in Wave 1 (2016) and 948 CHWs and 283 CHW employers in Wave 2 (2021). Given the diversity of official titles of CHWs across organizations, we defined CHWs in the samples not solely by title but also by answers to questions asking about their functions. This project was deemed nonhuman subjects research by the University of Massachusetts Chan Medical School Institutional Review Board.
We administered Wave 1 of the surveys from June 14 to August 1, 2016, and Wave 2 from April 13 to July 1, 2021. The CHW employer response rate was 66.5% in Wave 1 and 62.1% in Wave 2. The CHW response rate was 63.2% in Wave 1 and 52.6% in Wave 2. We weighted the data using inverse probability scores to account for differential response patterns by neighborhood stress score, organization size, and organization type, the methods of which are described previously. 21 At the time of this writing (August 2023), 1171 certifications had been issued by the Massachusetts Board of CHW Certification, of which 83.9% were current or pending. 26
Content of Wave 1 and Wave 2 Surveys
Survey tools were described previously. 21 We administered 2 surveys in each wave: one to CHWs and one to CHW employers. We aligned selected questions where CHW and CHW employer contrasts were of interest. Both surveys assessed numerous topics. Selected metrics reported here from the CHW survey include CHW employment (eg, job title, pay, full- or part-time employment), CHW sociodemographic information (eg, race and ethnicity, gender/sex, educational attainment), training and certification (eg, 80-hour core competency training, certification status), clinical care team integration in clinical organizations (eg, use and access to electronic health records, interactions with the clinical care team), and CHW’s perceived value assessed on a Likert-type scale. For example, 1 statement was “Organization values the work that CHWs do.” We calculated the percentage of CHWs who completely agreed with each statement. Metrics from the CHW employer survey reported here include the respondent’s job title, the number of CHWs supervised, and CHW hiring requirements (eg, minimum educational requirements, qualifications).
Statistical Analysis
We calculated means and medians for continuous measures. For Wave 2, we stratified data by certification status (certified CHWs vs noncertified CHWs) and, in selected cases, by employer organization type (clinical organizations [acute-care hospitals and health centers] vs nonclinical organizations [CBOs]). We elected to stratify by organization type when we believed employer characteristics might confound certification-related findings. In the analysis of salaries, to account for potential confounding, we restricted the analysis to full-time CHWs and CHWs working in clinical organizations because certified CHWs (vs uncertified CHWs) more often work full-time and certified CHWs (vs uncertified CHWs) are overrepresented in clinical organizations. However, due to small cell size, we were unable to stratify by both full-time status and organization type simultaneously.
For statistical comparisons between waves and strata, we used Quantum version 5.8 (Informer Technologies, Inc) to conduct 2 independent-sample t tests. Given the small percentage of CHWs and CHW employers responding to both survey waves (8.0% CHWs, 9.8% CHW employers), we deemed sample independence to be an acceptable assumption. We set significance at a 2-sided α of .05. Tests incorporated survey weights, used effective base, and assumed equal variances.
Results
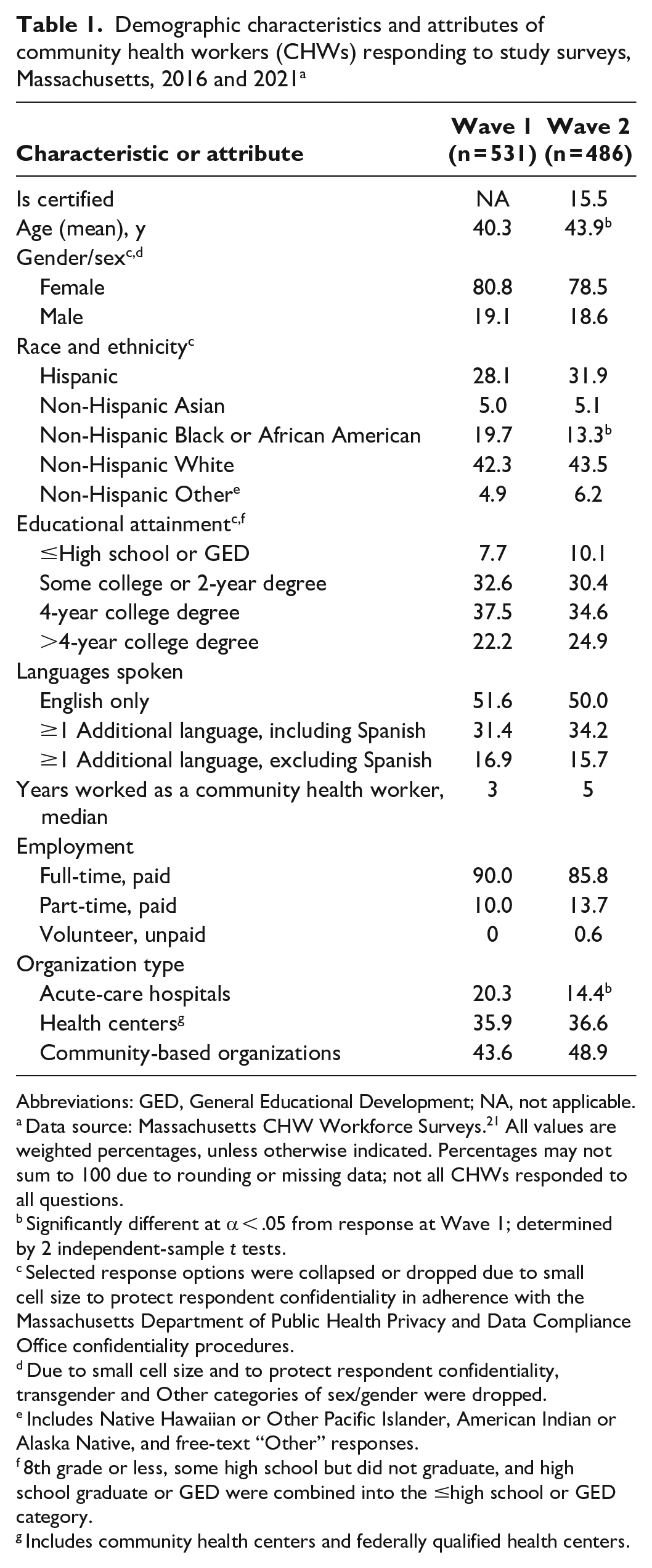
In Wave 2, 15.5% of responding CHWs indicated that they were certified by the Massachusetts CHW Board of Certification (Table 1).
Demographic characteristics and attributes of community health workers (CHWs) responding to study surveys, Massachusetts, 2016 and 2021 a
Abbreviations: GED, General Educational Development; NA, not applicable.
Data source: Massachusetts CHW Workforce Surveys. 21 All values are weighted percentages, unless otherwise indicated. Percentages may not sum to 100 due to rounding or missing data; not all CHWs responded to all questions.
Significantly different at α < .05 from response at Wave 1; determined by 2 independent-sample t tests.
Selected response options were collapsed or dropped due to small cell size to protect respondent confidentiality in adherence with the Massachusetts Department of Public Health Privacy and Data Compliance Office confidentiality procedures.
Due to small cell size and to protect respondent confidentiality, transgender and Other categories of sex/gender were dropped.
Includes Native Hawaiian or Other Pacific Islander, American Indian or Alaska Native, and free-text “Other” responses.
8th grade or less, some high school but did not graduate, and high school graduate or GED were combined into the ≤high school or GED category.
Includes community health centers and federally qualified health centers.
Was Certification Associated With Positive Outcomes for CHWs After Its Launch?
Certification was associated with numerous positive outcomes. Among all responding CHWs in Wave 2, the mean salary of certified CHWs was significantly higher than that of noncertified CHWs ($44 670 vs $40 810; P = .01). Full-time certified CHWs earned a mean salary of $44 670 and full-time noncertified CHWs earned a mean salary of $42 310; in clinical settings, certified CHWs earned a mean salary of $45 530 and noncertified CHWs earned a mean salary of $42 440 (significance tests not conducted because of small sample sizes).
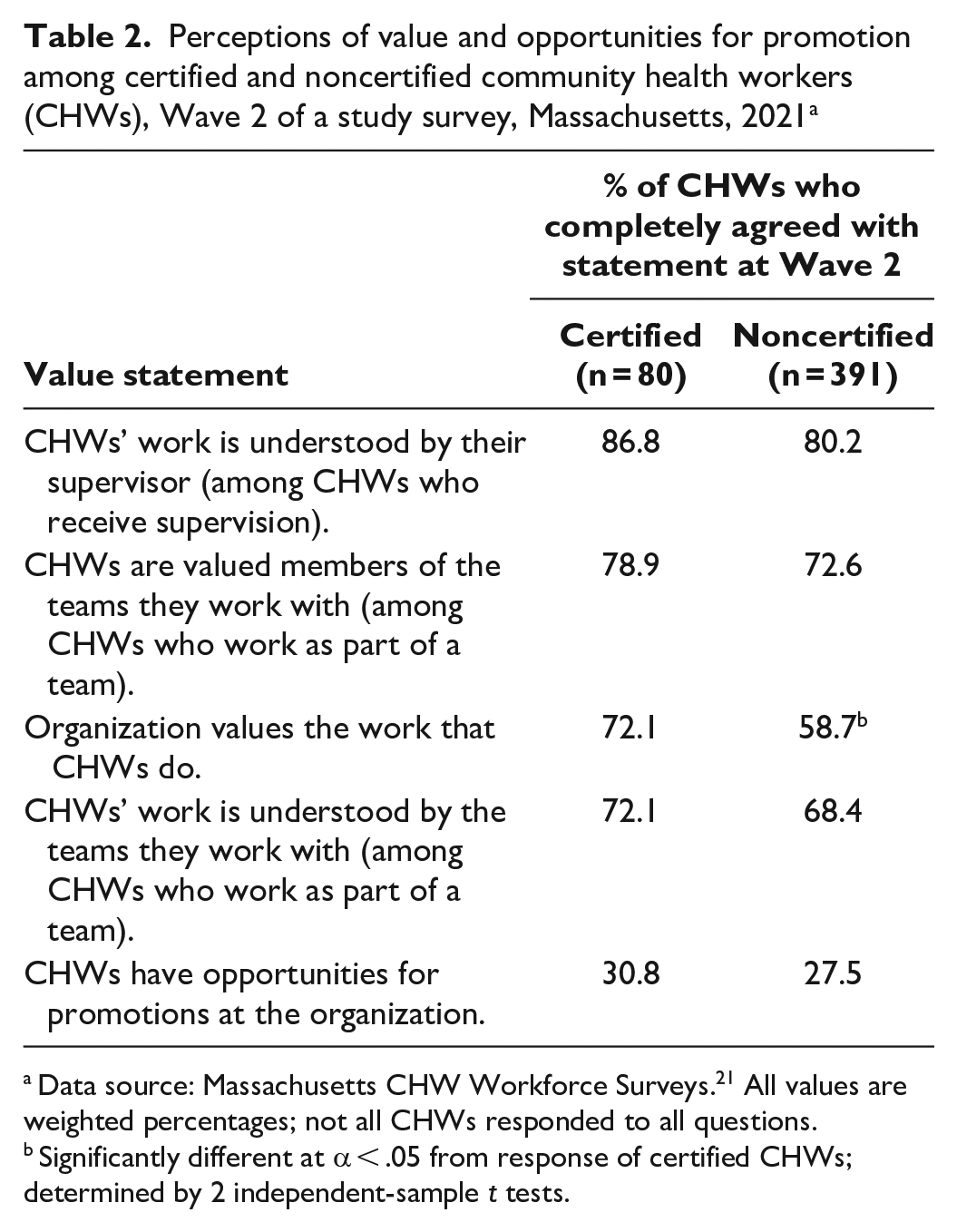
In nearly all statements of perceived value and opportunities for promotion, certified CHWs more frequently than noncertified CHWs agreed completely with each statement (Table 2). Notably, 72.1% of certified CHWs agreed completely that their organization values their work, whereas only 58.7% of noncertified CHWs agreed completely (P = .04). However, certified and noncertified CHWs reported similar opportunities for promotion (30.8% and 27.5%, respectively; P = .57).
Perceptions of value and opportunities for promotion among certified and noncertified community health workers (CHWs), Wave 2 of a study survey, Massachusetts, 2021 a
Data source: Massachusetts CHW Workforce Surveys. 21 All values are weighted percentages; not all CHWs responded to all questions.
Significantly different at α < .05 from response of certified CHWs; determined by 2 independent-sample t tests.
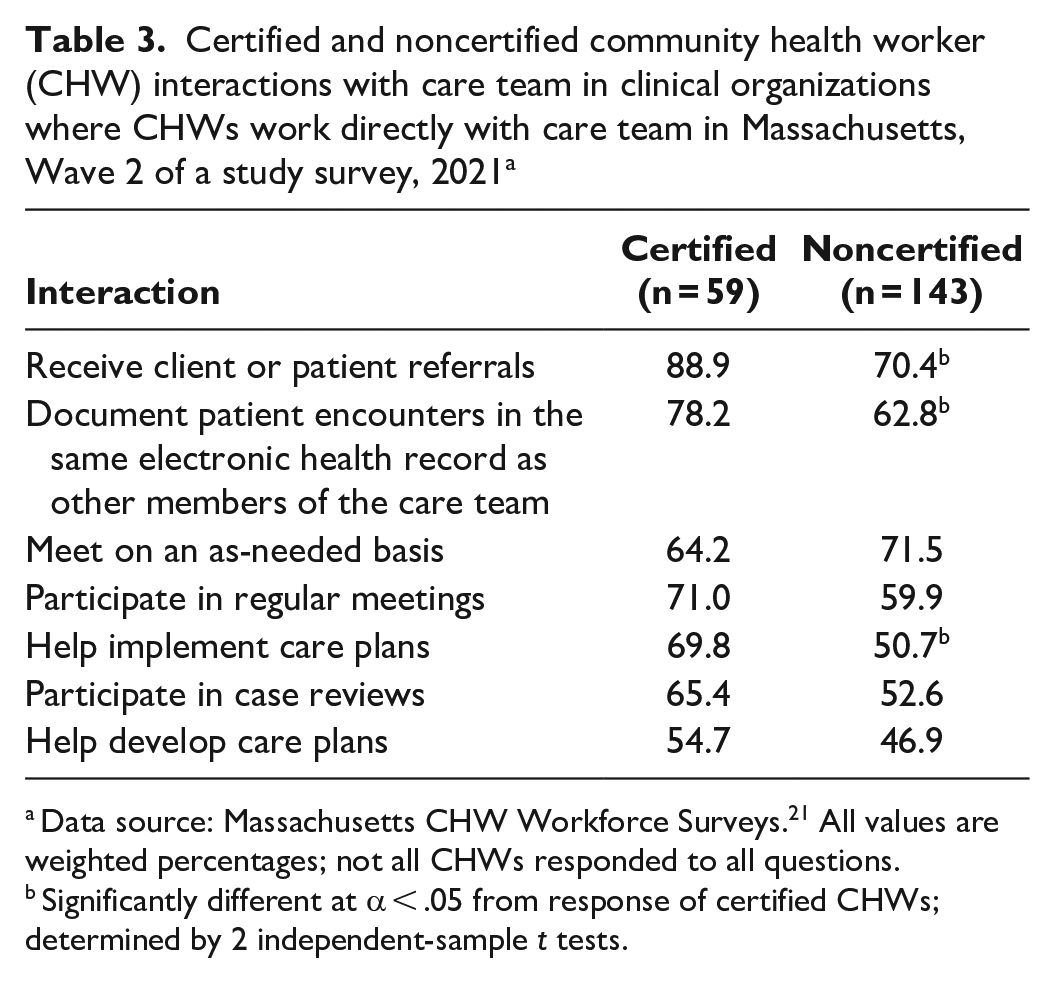
Certified CHWs reported significantly more often than noncertified CHWs that they receive patient referrals (88.9% vs 70.4%; P = .009), document their work in the same electronic health record as other members of the clinical care team (78.2% vs 62.8%; P = .048), and help implement care plans (69.8% vs 50.7%; P = .02) (Table 3). Certified CHWs more often than noncertified CHWs reported participating in 3 of the remaining 4 activities, although these differences were not significant.
Certified and noncertified community health worker (CHW) interactions with care team in clinical organizations where CHWs work directly with care team in Massachusetts, Wave 2 of a study survey, 2021 a
Data source: Massachusetts CHW Workforce Surveys. 21 All values are weighted percentages; not all CHWs responded to all questions.
Significantly different at α < .05 from response of certified CHWs; determined by 2 independent-sample t tests.
Did Harmful Shifts Occur Among the CHW Workforce and CHW Employers Before and After Certification Launch?
Our analysis detected few significant sociodemographic shifts in the workforce after certification launch (Table 1). The types of organizations in which responding CHWs worked were similar before and after certification launch, with the most common setting being CBOs (43.6% in Wave 1, 48.9% in Wave 2; P = .08) and health centers (35.9% in Wave 1, 36.6% in Wave 2; P = .83). We found a significant decline in CHWs employed by hospitals from Wave 1 to Wave 2 (20.3% in Wave 1, 14.4% in Wave 2; P = .02). In both waves, most respondents were female (80.8% in Wave 1, 78.5% in Wave 2; P = .40) and many held a 4-year college degree (37.5% in Wave 1, 34.6% in Wave 2; P = .37). Fewer than half of the respondents were non-Hispanic White (42.3% in Wave 1, 43.5% in Wave 2; P = .72), followed by Hispanic (28.1% in Wave 1, 31.9% in Wave 2; P = .22), non-Hispanic Black or African American (19.7% in Wave 1, 13.3% in Wave 2; P = .01), non-Hispanic Asian (5.0% in Wave 1, 5.1% in Wave 2; P = .95), and non-Hispanic Other (4.9% in Wave 1, 6.2% in Wave 2; P = .40). Nearly half of the CHWs spoke more than 1 language, including Spanish (31.4% in Wave 1, 34.2% in Wave 2; P = .37).
Most CHW employers responding to both waves of the survey (187 in Wave 1, 172 in Wave 2) self-identified as a program manager or director (52.0% in Wave 1, 53.5% in Wave 2; P = .78). The median number of CHWs that CHW employers managed was similar in both waves (4 in Wave 1, 5 in Wave 2; P = .85), although CHW employers reported having fewer paid full-time CHWs in Wave 2 than in Wave 1 (82.4% vs 76.0%; P = .001) (Supplement 2).
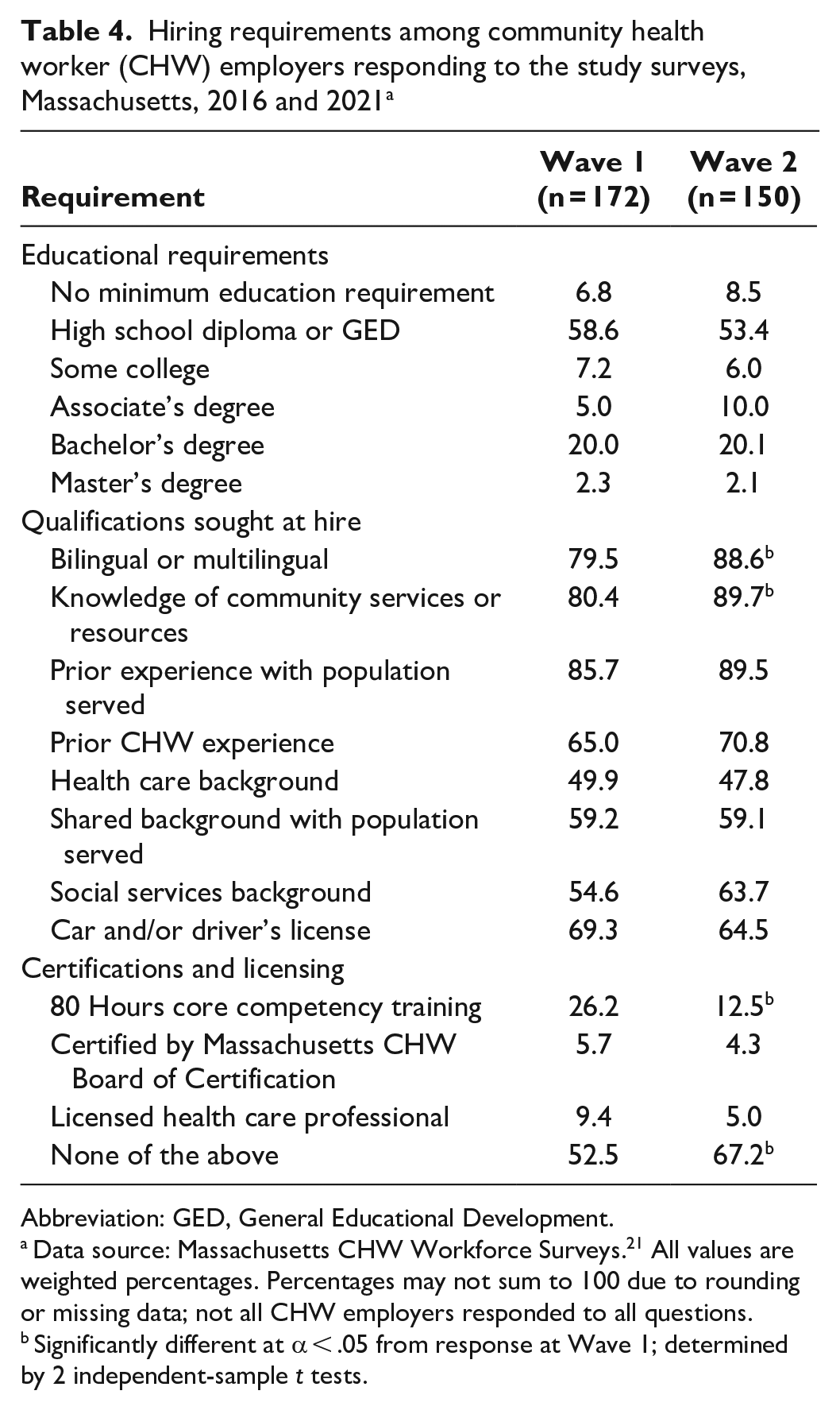
Few CHW employers in Massachusetts required certification for hire or were implementing training or education requirements (Table 4). The percentage of employers requiring that CHWs be certified by the Massachusetts CHW Board of Certification in Wave 2 was low, at 4.3%. In contrast, 10.0% of CHWs reported that their employer required certification. In Wave 1, 52.5% of CHW employers reported not requiring core competency training, health care professional licensing, or certification by the Massachusetts CHW Board of Certification as a condition for hiring, which increased to 67.2% in Wave 2 (P = .01). The most common education level sought by CHW employers in both waves was a high school diploma or General Educational Development (58.6% in Wave 1, 53.4% in Wave 2; P = .36).
Hiring requirements among community health worker (CHW) employers responding to the study surveys, Massachusetts, 2016 and 2021 a
Abbreviation: GED, General Educational Development.
Data source: Massachusetts CHW Workforce Surveys. 21 All values are weighted percentages. Percentages may not sum to 100 due to rounding or missing data; not all CHW employers responded to all questions.
Significantly different at α < .05 from response at Wave 1; determined by 2 independent-sample t tests.
Was Certification Associated With Disparities Among CHWs After Its Launch?
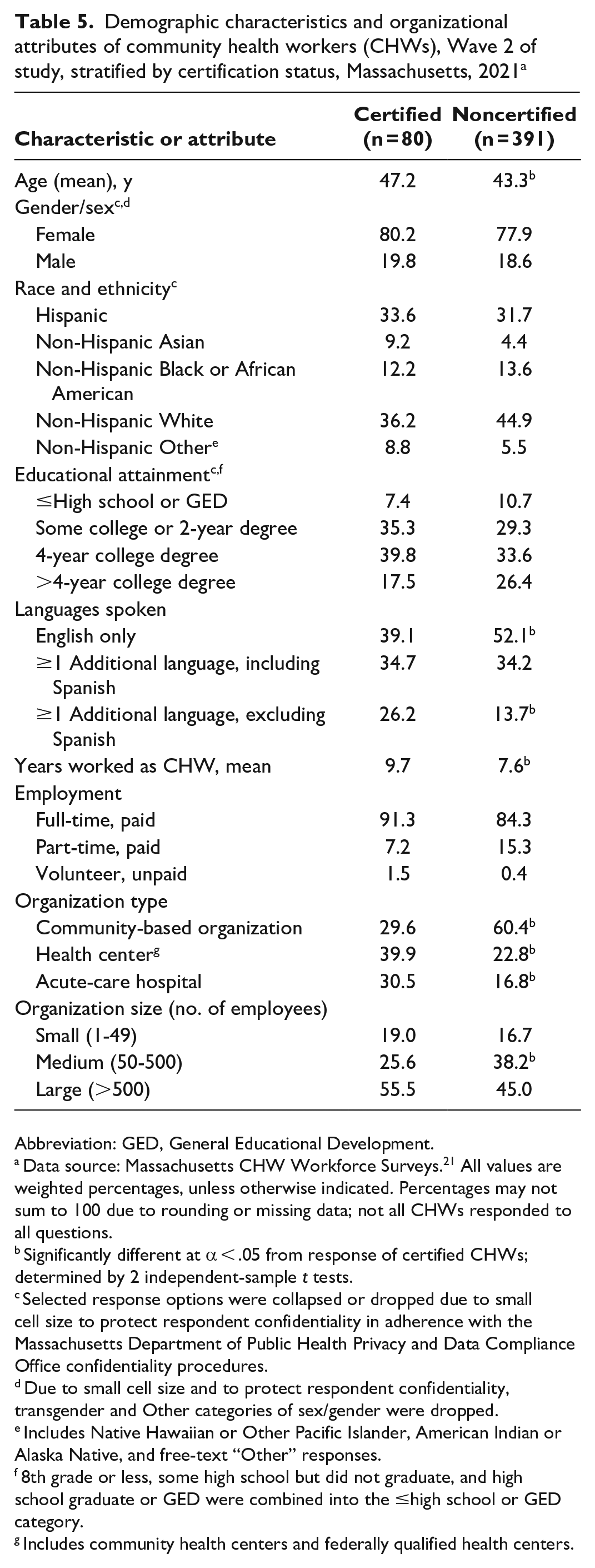
Wave 2 results showed that certification launch was not significantly associated with sociodemographic disparities among CHWs (Table 5). In Wave 2, compared with noncertified CHWs, certified CHWs were significantly older (47.2 vs 43.3 y; P = .02) and worked longer as a CHW (9.7 vs 7.6 y; P = .047). We found no significant disparities in education level between certified and noncertified CHWs, with 39.8% of certified CHWs and 33.6% of noncertified CHWs holding a 4-year college degree (P = .32). We noted some patterns by race, ethnicity, and gender/sex, but these were not significant.
Demographic characteristics and organizational attributes of community health workers (CHWs), Wave 2 of study, stratified by certification status, Massachusetts, 2021 a
Abbreviation: GED, General Educational Development.
Data source: Massachusetts CHW Workforce Surveys. 21 All values are weighted percentages, unless otherwise indicated. Percentages may not sum to 100 due to rounding or missing data; not all CHWs responded to all questions.
Significantly different at α < .05 from response of certified CHWs; determined by 2 independent-sample t tests.
Selected response options were collapsed or dropped due to small cell size to protect respondent confidentiality in adherence with the Massachusetts Department of Public Health Privacy and Data Compliance Office confidentiality procedures.
Due to small cell size and to protect respondent confidentiality, transgender and Other categories of sex/gender were dropped.
Includes Native Hawaiian or Other Pacific Islander, American Indian or Alaska Native, and free-text “Other” responses.
8th grade or less, some high school but did not graduate, and high school graduate or GED were combined into the ≤high school or GED category.
Includes community health centers and federally qualified health centers.
Analysis of employment stratified by certification status in Wave 2 showed several important patterns. The percentage of CHWs certified by the Massachusetts CHW Board of Certification in clinical organizations was nearly 3 times that of CHWs in nonclinical organizations (23.8% vs 8.1%; P = .001). The most common employer among noncertified CHWs was CBOs (60.4%), followed by health centers (22.8%) and hospitals (16.8%). Conversely, certified CHWs most often worked in health centers (39.9%) and acute-care hospitals (30.5%), while only 29.6% worked in CBOs. Finally, certified CHWs were more often employed full-time (91.3%) than were noncertified CHWs (84.3%), although this difference was not significant (P = .13).
Discussion
Nationally, CHW certification has been proposed as a method of increasing CHWs’ perceived value and compensation, as well as better integrating CHWs into care teams.4-6 In Massachusetts, CHW certification regulations were crafted with extensive community input.14,19 Because our study is one of the few of its kind nationally to evaluate both positive and potential adverse trends associated with state CHW certification, it provides crucial insight to state policy makers and CHW advocates seeking to pass similar equity-centered regulations in their own state. 21
Because one of the largest concerns many CHW advocates had about launching certification was creating workforce disparities, it is reassuring to see few significant changes in Wave 1 versus Wave 2 and by certification status.4,16 Centering equity, as was done in Massachusetts when designing CHW certification, is important for other states considering certification regulations. However, the overall decrease in Black and African American CHWs from Wave 1 to Wave 2, even though not differing by certification status, bears tracking in future workforce assessments. We expected older and more experienced CHWs to be certified more often than younger and less experienced CHWs, given that certification by the work experience pathway launched before the combined training and work experience pathway (October 2018 vs July 2021).
It is reassuring that few Massachusetts CHW employers reported requiring certification for hire and that employers continued to emphasize the unique skillsets and attributes of CHWs. Employers requiring certification for hire, which in turn may create barriers to practice for qualified CHWs, is a notable concern with certification and is a reason that Massachusetts CHW certification is voluntary.4,14,20 In contrast, a study of Texas employers found that most employers required certification for hire. 27 Employer hiring criteria may reflect the long-standing availability of CHW state certification in Texas (since 2002) and that the initial certification law in Texas required certification for those receiving compensation as CHWs (although there are no regulations for enforcement). 28 In addition, the MDPH Office of CHWs engages extensively with employers regarding hiring of CHWs, which may explain the increase in employers not requiring any licensing or educational requirements.
In our study, CHW certification was associated with positive outcomes among CHWs. However, CHW certification in Massachusetts is intended to eventually result in benefits for all CHWs (Supplement 1). 29 Nevertheless, full-time certified CHWs reported $2360 higher mean earnings than full-time uncertified CHWs; in clinical organizations, certified CHWs reported $3090 higher mean earnings than uncertified CHWs. These findings agree with those in a recent national study, which found higher pay for CHWs in states with CHW certification than in states without certification. 30 Although CHWs undertake their work to serve their communities, a living wage is important for workforce sustainability and is an anticipated effect of certification. 4
Among CHWs, we found that certification was associated with positive perceptions. Increased recognition of CHWs is a key outcome of certification, which may lead to numerous benefits, such as increased use of sustainable funding and greater workforce retention.4,16 However, our study found that opportunities for promotion were low across both certified and uncertified CHWs. Although career advancement is an active topic in the CHW community, guidance on this topic is limited,31-33 leaving CHW employers ill equipped to promote CHWs. Recent studies of CHW career advancement provide important information on this understudied topic.32,33 Additional research is needed.
In clinical organizations, certified CHWs reported more extensive engagement with the care team than noncertified CHWs. Certification may be a way of increasing the integration of CHWs into health care teams.4,5,24 Given that health care is a highly professionalized field, a channel through which certification is hypothesized to facilitate care team integration is shifting health care providers’ perceptions of CHWs and increasing understanding of CHW roles.4,16,34 A qualitative study found that care teams with high levels of CHW integration tended to have positive perceptions of CHWs and better alignment in understanding the role of CHWs. 34 Despite mixed findings in a multistate study assessing whether state CHW certification programs were associated with improved perception of CHWs among registered nurses, the study did not indicate whether the nurses surveyed actually worked directly with certified CHWs. 23
Finally, our findings suggest notable differences in employment patterns by certification status. Certified CHWs tended to work in clinical organizations (vs nonclinical organizations) and more often worked full-time (vs part-time), whereas noncertified CHWs tended to work in nonclinical organizations (vs clinical organizations) and were more often working part-time (vs full-time). Our finding that certified CHWs more often worked in clinical than in nonclinical settings was not surprising, because certification of CHWs has received particular attention in health care settings.22,24 Certification has been raised as a method to legitimize the role of CHWs in health care, ensure consistency in the quality of their work, and change perceptions of CHWs among health care providers.4,5 Furthermore, a recent study suggested that employment of CHWs is growing in health care settings and that clinical employers may be interested in the training and certification status of applicants. 22 Nevertheless, CHW certification in Massachusetts is intended to benefit both clinical and nonclinical CHWs. 14 Further engagement with CBO employers and CHWs is necessary to understand and potentially address these patterns. Finally, these employment patterns should continue to be monitored and are essential to consider when assessing positive outcomes purportedly associated with certification (eg, pay); failure to do so may result in biased conclusions.
Limitations
Our study had several limitations. First, weaknesses of our survey methodology included limited generalizability beyond the selected sample frames and challenges in survey administration due to COVID-19. 21 Second, unique aspects of CHW certification in Massachusetts must be kept in mind. Development of CHW certification, core competencies, and other programming required years of consensus building and centered the CHW voice in decision-making. However, this approach does not always occur in other states, 16 and it should be a central consideration in evaluating other states’ certification processes. Third, certification policies vary widely by state, which is a noted limitation of studies assessing certification-related outcomes across states.23,30 Fourth, as outlined in the theory of change model, the MDPH Office of CHWs and their partners undertake numerous activities to champion the CHW workforce; these efforts may have affected our findings (Supplement 1). Fifth, the COVID-19 pandemic, which occurred between survey waves, may have affected survey results, such as through differential response due to increased telework. 21 Sixth, continuous engagement with the CHW workforce, their employers, and other key informants, particularly the use of qualitative methods, is equally as important as an evaluation component as the CHW Workforce Survey. Seventh, our cross-sectional study of Massachusetts CHW certification was pragmatic, intersecting with state policy changes and a web of external factors. Given this, we must be cautious not to overstate findings.
Conclusions
Our evaluation of Massachusetts CHW certification suggests that CHW certification was not associated with workforce disparities and was associated with positive outcomes. Our study fills a notable gap in the research literature and can guide CHW research agendas, certification efforts in Massachusetts and other states, and program efforts to champion this critical, grassroots workforce.
Supplemental Material
sj-docx-1-phr-10.1177_00333549241253419 – Supplemental material for The Launch of Massachusetts Community Health Worker Certification: Findings From the Massachusetts Community Health Worker Workforce Surveys
Supplemental material, sj-docx-1-phr-10.1177_00333549241253419 for The Launch of Massachusetts Community Health Worker Certification: Findings From the Massachusetts Community Health Worker Workforce Surveys by Victoria M. Nielsen, W.W. Sanouri Ursprung, Glory Song, Gail Hirsch, Theresa Mason, Claire Santarelli, Erica Guimaraes, Erica Marshall, Caitlin G. Allen, Pei-Pei Lei, Diane Brown and Bittie Behl-Chadha in Public Health Reports
Footnotes
Authors’ Note
Survey data, including contact information, individual responses, and aggregate data, are considered confidential by the Massachusetts Department of Public Health (MDPH). Questions regarding these data should be directed to the MDPH Office of CHWs (
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Centers for Disease Control and Prevention under the State Public Health Actions to Prevent and Control Diabetes, Heart Disease, Obesity and Associated Risk Factors and Promote School Health (DP13-1305) and Improving the Health of Americans through Prevention and Management of Diabetes and Heart Disease and Stroke (CDC-RFA-DP18-1815).
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.