
Abstract
Objective:
Linkage to HIV medical care is important in the continuum of HIV care and health outcomes for people with HIV. The objective of this analysis was to identify how the community-based organization (CBO) program contributes to linkage to HIV medical care among people with newly diagnosed HIV in the Centers for Disease Control and Prevention’s (CDC’s) HIV testing program.
Methods:
We analyzed HIV linkage-to-care data submitted to CDC from 2019 through 2021. Linkage was defined as confirmation that an individual attended their first HIV medical care appointment within 30 days of their HIV test date. We included in the analysis data submitted from the health department (HD) program that included 61 state and local HDs in the United States, Puerto Rico, and the US Virgin Islands and the CBO program that included 150 CBOs.
Results:
The CBO program linked a higher proportion of people to HIV medical care within 30 days of diagnosis (86.7%) than the HD program (73.7%). By population group, the proportion linked in the CBO program was higher than the proportion linked in the HD program among men who have sex with men (prevalence ratio [PR] = 1.13; P < .001), men who have sex with men/people who inject drugs (PR = 1.29; P < .001), transgender people (PR = 1.28; P < .001), and those reporting no sexual contact or injection drug use (PR = 1.34; P < .001). In the Cox proportional hazards model, time to linkage in the CBO program was significantly shorter than in the HD program (hazard ratio = 0.63; P < .001).
Conclusion:
This analysis shows that the CBO program fills a vital need in linking newly diagnosed HIV-positive people to HIV medical care, which is important in the HIV care continuum and for viral suppression.
The Ending the HIV Epidemic in the United States (EHE) initiative, led by the US Department of Health and Human Services, has a goal to reduce HIV infections in the United States by 90% by 2030. 1 Diagnosing people with HIV (PWH) as early as possible and treating them rapidly and effectively to reach viral suppression are 2 core pillars of the Centers for Disease Control and Prevention’s (CDC’s) approach to implementing the EHE initiative. A critical component of CDC’s HIV prevention program is linkage to HIV medical care. Timely engagement in medical care is crucial for achieving viral suppression for PWH. 2 Early initiation of antiretroviral therapy (ART) substantially improves survival compared with deferred therapy. 2 The US national goal is to link 95% of people with newly diagnosed HIV to care within 30 days. 3 However, in 2020, only 76% of newly identified PWH tested through CDC’s HIV prevention program were linked to care within 30 days. 4
CDC promotes linkage and other HIV outcomes through its HIV prevention program by providing funding for HIV prevention and care services at 61 health departments (HDs, hereinafter referred to as the HD program) and 150 community-based organizations (CBOs, hereinafter referred to as the CBO program) in the United States and dependent areas. CDC’s funding for the HD program provides each HD jurisdiction the opportunity to carry out comprehensive HIV prevention programs broadly that prevent new HIV infections and achieve viral suppression among those living with HIV in their communities. 5 The CBO program provides HIV prevention and care services to populations with the greatest need.6,7
CDC has collaborated with CBOs since the 1980s, and CBOs are in a unique position to support and enhance the reach of the HD program’s HIV prevention efforts.6-8 The CBO program sites are co-located in selected HD jurisdictions and have found success by employing diverse staff who represent the prioritized populations (ie, those with certain risk factors, such as men who have sex with men [MSM] and injection drug use) and/or speak the language of the population. 9 Staff at these CBOs may have more interaction and trust with their prioritized populations than in other HIV prevention settings because of daily community outreach, established organizational presence, and trust from the communities they serve. 10 CDC’s funding of the CBO program provides support for CBOs to conduct individualized HIV prevention interventions for their prioritized populations and maximize the nimbleness of their approaches. Without the CBO program, jurisdictions may miss opportunities to identify people with newly diagnosed HIV and provide linkage-to-care services.
Although the rationale for CDC’s support for CBOs is well-established, little work has been published that examines how the program contributes to the overall goals for HIV prevention and linkage to care. One exception is a recently published study that found that the CBO program enhanced CDC-funded testing, identifying people with newly diagnosed HIV infection at a rate that was nearly 3 times that of the HD program. 11 Our analysis expands on that finding by assessing linkage to HIV medical care by program. Specifically, we assessed linkage to HIV medical care among people newly diagnosed with HIV in the CBO and HD programs, including overall linkage within 30 days from diagnosis annually and from 2019 through 2021, time from diagnosis to linkage, and linkage within 30 days from diagnosis by sociodemographic attributes in non–health care settings (where detailed sociodemographic information is available). Analyzing program-specific contributions to CDC’s HIV prevention and care goals serves to inform future policies and programs.
Methods
Data Source
We used National HIV Prevention Program Monitoring and Evaluation (NHM&E) HIV testing data submitted for tests conducted from January 31, 2019, through December 31, 2021, by 61 CDC-funded state and local HDs in the United States, Puerto Rico, and the US Virgin Islands and from 150 CBOs. Most HDs conduct HIV testing throughout their jurisdiction, providing routine opt-out testing (where patients are informed that an HIV test will be conducted unless they explicitly decline to be tested), mostly by medical professionals in health care settings. The CDC Division of HIV Prevention’s Office of Science determined that review by an institutional review board was not needed for the collection of NHM&E HIV testing data because the study was deemed non-research, it was a public health program activity, and it did not involve human subjects. The Office of Management and Budget (OMB) approved the NHM&E data collection (OMB 0920-0696).
Variables and Measures
Gender categories used in the analysis were male, female, transgender male to female (transgender women), transgender female to male (transgender men), and transgender unspecified. These categories are used on standardized CDC HIV testing forms and data collection requirements. Age was categorized into 6 groups: <13, 13-19, 20-29, 30-39, 40-49, and ≥50 years. US Census regions were Midwest, Northeast, South, West, and US dependent areas. 12 Race and ethnicity categories were Hispanic/Latino (of any race), Black/African American, White, Asian, American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, or >1 race.
Our data analysts constructed population groups based on self-reported gender identity and HIV risk behaviors. We followed the methodology of the Annual HIV Testing Report for CDC-Funded HIV Testing in the United States, Puerto Rico, and US Virgin Islands and presented the following mutually exclusive population groups: MSM, MSM and people who inject drugs (PWID) (MSM/PWID), transgender people, transgender people who inject drugs (transgender/PWID), PWID, heterosexual men, heterosexual women, other risk, and those who reported no sexual contact or injection drug use at the time of the HIV test. 7
Our data analysts categorized HIV test data by funding program and, for HDs, the test setting. Categories included the CBO program, the HD program in health care settings, and the HD program in non–health care settings (non–health care settings accounted for 23.1% of HD program tests). More specifically, the HD program site types included health care settings that provided both medical diagnostic and treatment services (eg, outpatient clinics) and non–health care settings that did not provide both medical diagnostic and treatment services (eg, community testing sites such as bars). The CBO program reaches out to prioritized populations that are at risk for HIV in their community; for example, young MSM of color and young transgender people of color who have sex with men. The CBO programs recruit people by hosting activities, creating safe spaces, and meeting people in the community to serve these populations. Both the HD and CBO programs are required to link PWH to medical care within 30 days, and both programs offer behavioral interventions, linkage-to-care services, and medication adherence services.
Newly diagnosed HIV-positive people were those who received a positive HIV test result and self-reported no prior positive HIV test result. We defined linkage to HIV medical care within 30 days of diagnosis as confirmation, either through self-report or through the HIV surveillance system, that the person attended their first HIV medical care appointment within 30 days of their HIV test date.
Data Analyses
We used descriptive statistics to present CBO and HD program HIV tests conducted during 2019-2021. We assessed differences in the proportion of newly diagnosed people linked to care within 30 days through the CBO and HD programs for each sociodemographic group using robust Poisson models accounting for potential lack of independence of tests within jurisdictions. Models produced prevalence ratio (PR) estimates comparing linkage in the CBO program with linkage in the HD program. We adjusted P values and 95% CIs by using Bonferroni correction to account for multiple testing; P < .05 was considered significant. To assess differences in the timing of linkage to care after diagnosis, we generated a Kaplan–Meier plot and used an unadjusted Cox proportional hazard model to generate a hazard ratio (HR) and P value.
Results
Of the 1 426 860 HIV tests conducted during 2019-2021, 23 140 (1.6%) people were newly diagnosed with HIV. The CBO program accounted for 3027 (13.1%) and the HD program accounted for 20 113 (86.9%) people with newly diagnosed HIV (Table 1). The number of newly diagnosed HIV-positive people at the CBO program decreased 40.9% from 1370 in 2019 to 809 in 2021. We found a 12.9% decrease in newly diagnosed HIV-positive people for the HD program, from 7749 in 2019 to 6753 in 2021. Of those newly diagnosed with HIV in either program, 14 323 of 18 969 (75.5%) were linked to HIV medical care within 30 days.
Linkage to HIV medical care within 30 days among newly diagnosed HIV-positive people at 150 CDC-funded CBOs and 61 CDC-funded health departments, United States, 2019-2021 a
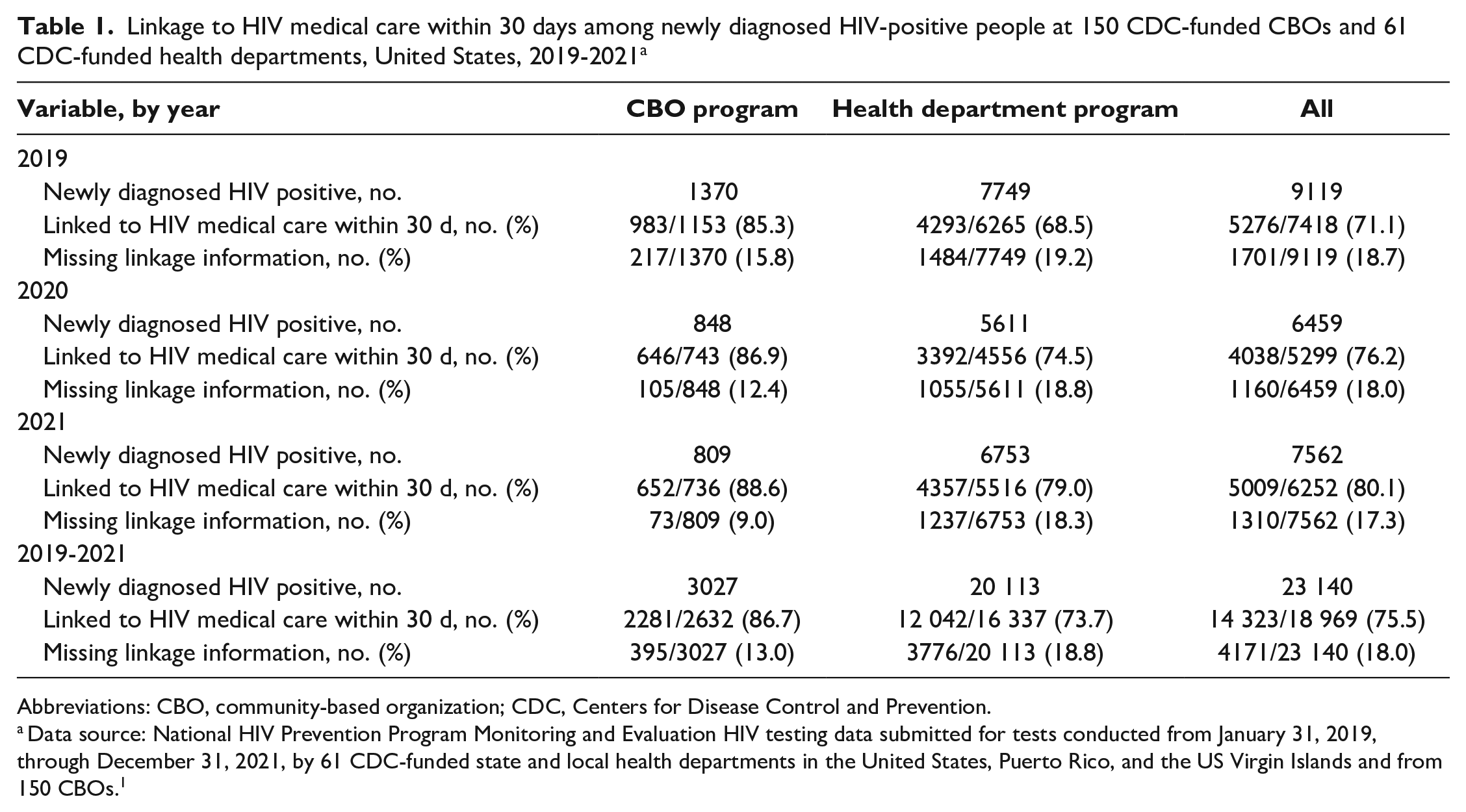
Abbreviations: CBO, community-based organization; CDC, Centers for Disease Control and Prevention.
Data source: National HIV Prevention Program Monitoring and Evaluation HIV testing data submitted for tests conducted from January 31, 2019, through December 31, 2021, by 61 CDC-funded state and local health departments in the United States, Puerto Rico, and the US Virgin Islands and from 150 CBOs. 1
The median number of days until a person newly diagnosed with HIV was linked to HIV medical care was 7 days during the study period (Table 2). For both CBO and HD programs, the median number of days until the person was linked to HIV medical care decreased from 5 to 3 days for the CBO program and from 10 to 7 days for the HD program from 2019 to 2021. The Kaplan–Meier plot also shows that the shorter time to linkage to HIV medical care at the CBO program persisted over time (Figure). Linkage to HIV medical care among those receiving a new HIV-positive test result on the same day of the test occurred for 23.9% in the CBO program and 16.2% in the HD program. Time to linkage to HIV medical care at the CBO program was significantly shorter than at the HD program in the Cox proportional hazards model (HR = 0.63; P < .001).
Median number of days until people newly diagnosed with HIV were linked to HIV medical care at 150 CDC-funded CBOs and 61 CDC-funded health departments, 2019-2021 a
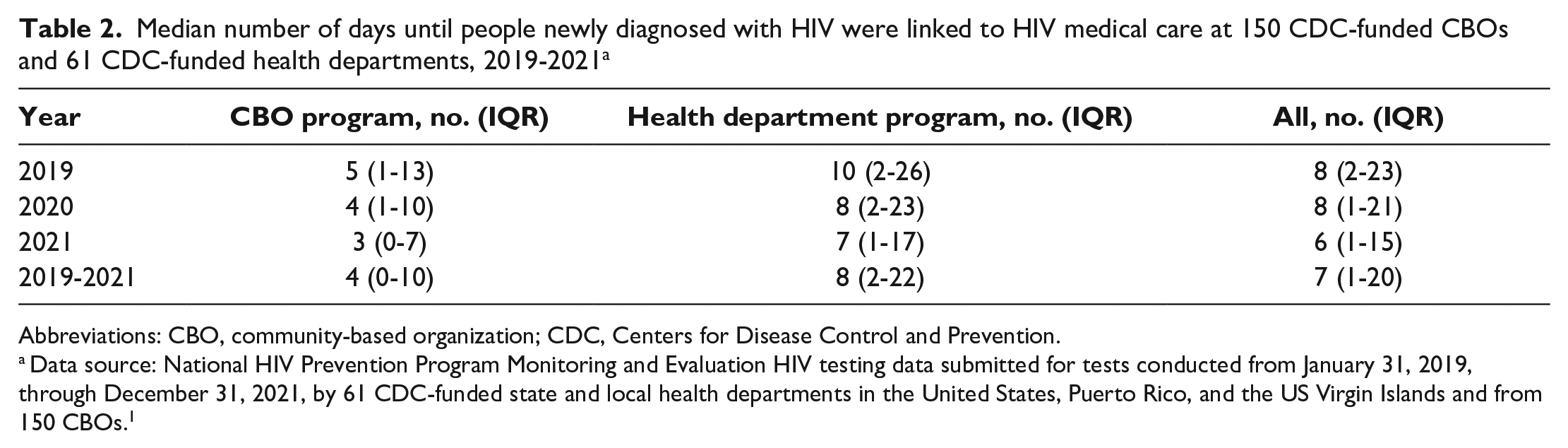
Abbreviations: CBO, community-based organization; CDC, Centers for Disease Control and Prevention.
Data source: National HIV Prevention Program Monitoring and Evaluation HIV testing data submitted for tests conducted from January 31, 2019, through December 31, 2021, by 61 CDC-funded state and local health departments in the United States, Puerto Rico, and the US Virgin Islands and from 150 CBOs. 1
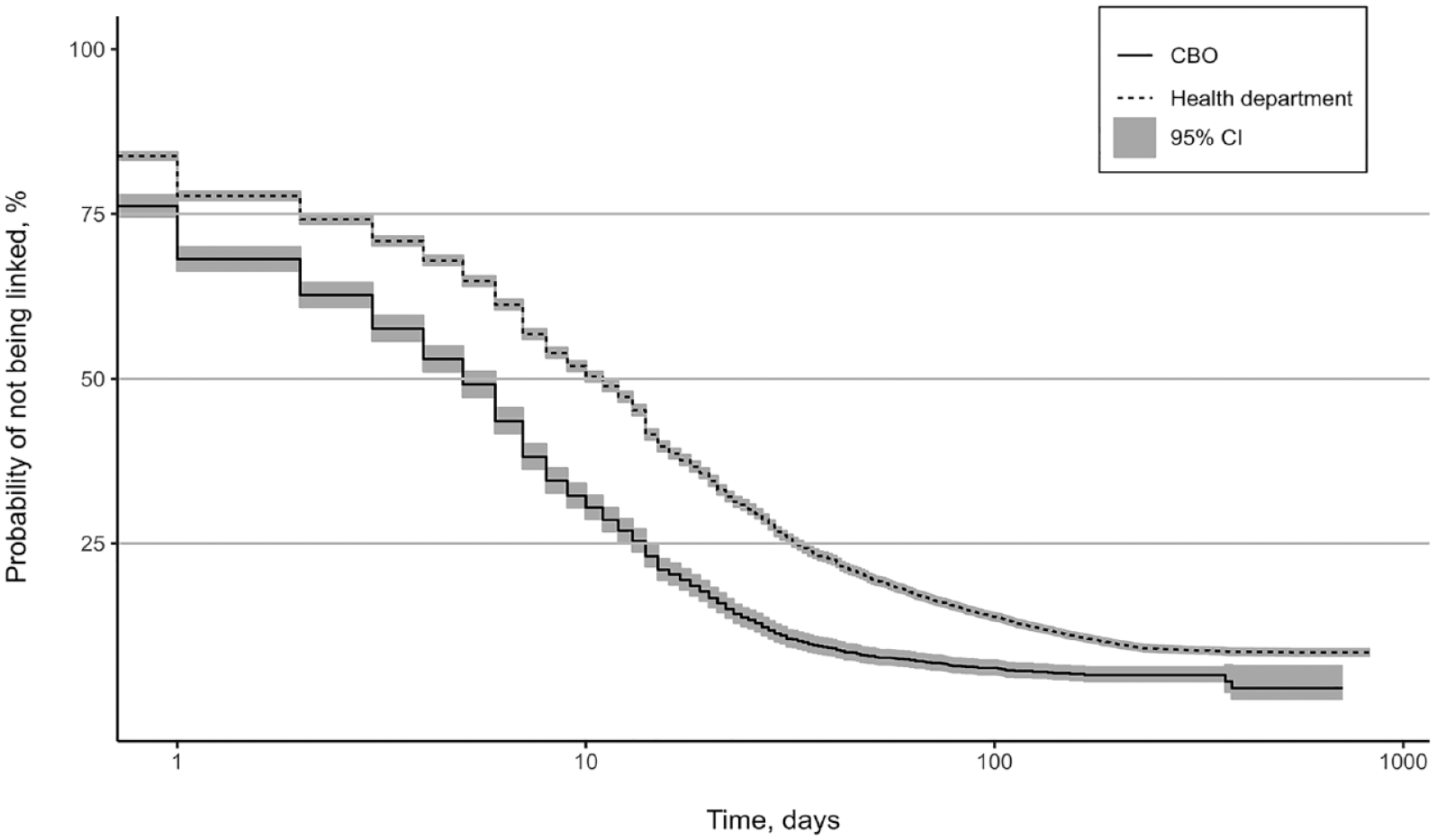
Time to linkage to HIV medical care at 150 CDC-funded CBOs and 61 CDC-funded health departments, 2019-2021. Abbreviations: CBO, community-based organization; CDC, Centers for Disease Control and Prevention.
Linkage to HIV medical care varied among sociodemographic groups when we examined the CBO program and HD non–health care settings (Table 3). The CBO program linked a significantly higher percentage of newly diagnosed people in non–health care settings to HIV medical care within 30 days (86.7%) compared with the HD program (73.6%) (P < .001). When stratifying by sociodemographic characteristics, we found several differences between the CBO and HD programs. By gender, linkage to HIV medical care was significantly higher in the CBO program than in the HD program among males (87.2% vs 74.3%; PR = 1.17; P < .001), females (81.0% vs 70.1%; PR = 1.15; P = .01), and transgender women (87.8% vs 65.7%; PR = 1.34; P < .001). By age group, linkage to HIV medical care was significantly higher in the CBO program than in the HD program for people aged 13-19 years (92.3% vs 75.8%; PR = 1.22; P = .004), 20-29 years (88.4% vs 73.9%; PR = 1.20; P < .001), 30-39 years (87.7% vs 74.5%; PR = 1.18; P < .001), and 40-49 years (85.4% vs 73.4%; PR = 1.16; P < .001). By region, linkage to HIV medical care was significantly higher in the CBO program than in the HD program only in the South (88.3% vs 71.5%; PR = 1.23; P < .001). Linkage to HIV medical care was also significantly higher in the CBO program than in the HD program among newly diagnosed HIV-positive people who reported race and ethnicity as White (87.0% vs 72.9%; PR = 1.19; P < .001), Black/African American (85.3% vs 71.4%; PR = 1.19; P < .001), or Hispanic/Latino (90.0% vs 78.6%; PR = 1.14; P < .001). By population group, linkage to HIV medical care was significantly higher in the CBO program than in the HD program among MSM (88.1% vs 77.7%; PR = 1.13; P < .001), MSM/PWID (89.9% vs 69.5%; PR = 1.29; P < .001), transgender people (88.8% vs 69.2%; PR = 1.28; P = .001), and those reporting no sexual contact or injection drug use (92.1% vs 68.9%; PR = 1.34; P < .001).
Linkage to HIV medical care within 30 days among newly diagnosed HIV-positive people at 150 CDC-funded CBOs and 61 CDC-funded health departments (non–health care settings only), by sociodemographic groups, 2019-2021 a
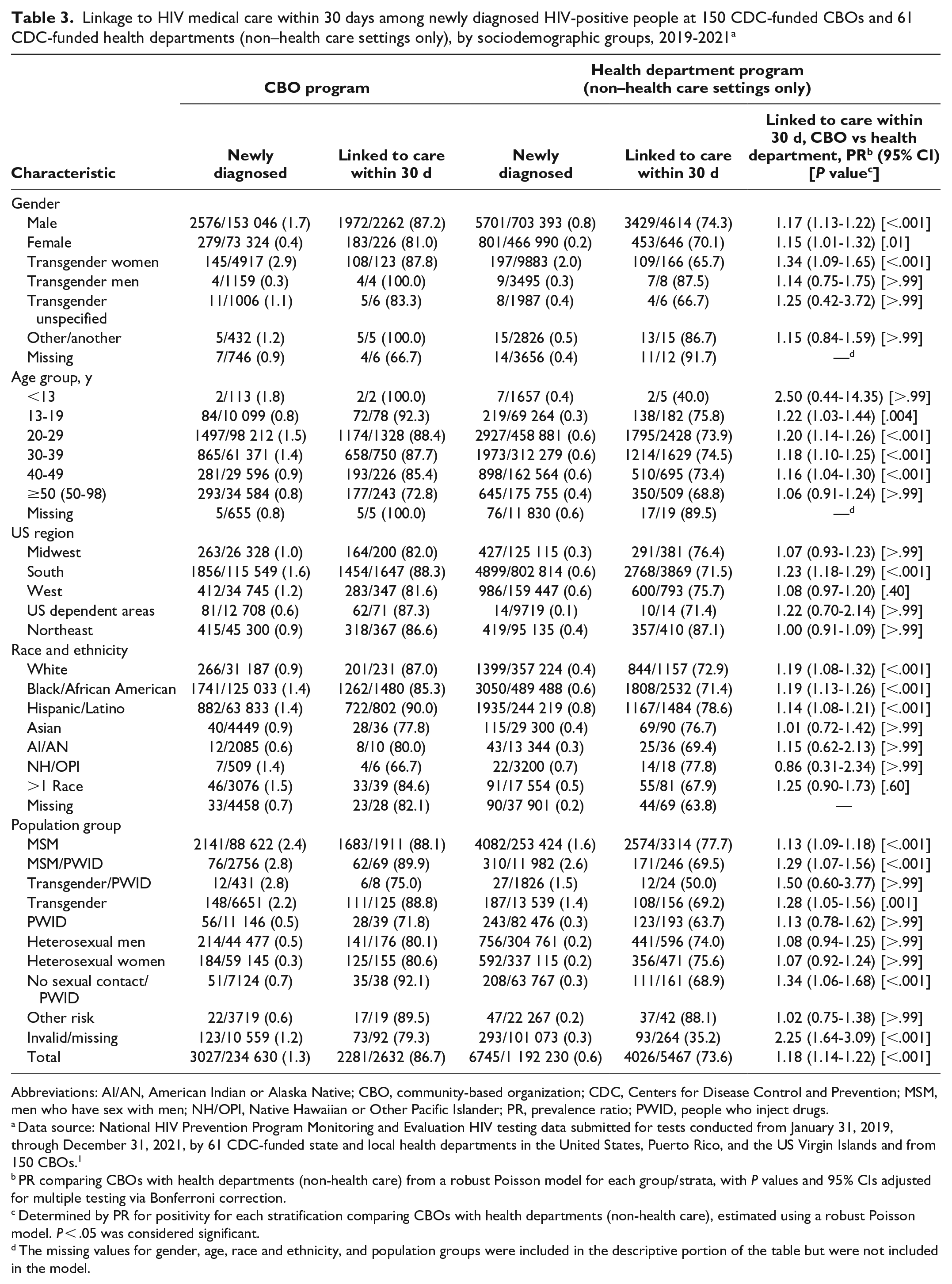
Abbreviations: AI/AN, American Indian or Alaska Native; CBO, community-based organization; CDC, Centers for Disease Control and Prevention; MSM, men who have sex with men; NH/OPI, Native Hawaiian or Other Pacific Islander; PR, prevalence ratio; PWID, people who inject drugs.
Data source: National HIV Prevention Program Monitoring and Evaluation HIV testing data submitted for tests conducted from January 31, 2019, through December 31, 2021, by 61 CDC-funded state and local health departments in the United States, Puerto Rico, and the US Virgin Islands and from 150 CBOs. 1
PR comparing CBOs with health departments (non-health care) from a robust Poisson model for each group/strata, with P values and 95% CIs adjusted for multiple testing via Bonferroni correction.
Determined by PR for positivity for each stratification comparing CBOs with health departments (non-health care), estimated using a robust Poisson model. P < .05 was considered significant.
The missing values for gender, age, race and ethnicity, and population groups were included in the descriptive portion of the table but were not included in the model.
Discussion
Our analysis shows that CBO programs linked a higher proportion of people to HIV medical care within 30 days than the HD program across nearly all sociodemographic groups. Findings published in 2022 showed that the CBO program provided a small percentage (3%) of the CDC HIV prevention program HIV tests but identified a larger percentage (8%) of people with newly diagnosed HIV when compared with all HD program tests. 11 This finding highlights the overall value of the CBO program for identifying those who may have not been reached otherwise.
To effectively reach the EHE goal of reducing HIV infections by 90%, the CBO and HD programs must complement each other’s strategies. The CBO programs coordinate with the HD program through memoranda of understanding and are closely connected with HD staff and to the services provided by the HD, including disease intervention specialists. Jurisdictions’ collective HIV prevention approach often includes the HD program offering services to all members of the community, while the CBO program provides focused HIV prevention to groups of people whose social determinants of health (eg, stigma, poverty, lack of access to care) may increase their chances of getting HIV.
The CBO and HD programs in non–health care settings provided HIV tests and linked people to HIV medical care in similar areas with similar population groups; however, the CBO program linked a higher proportion of people to care and linked them faster. One reason for this finding could be enhanced interventions for linkage to HIV medical care in the CBO program. One enhanced linkage strategy at the CBO program level is linkage-to-care coordinators, who facilitate same-day linkage to HIV medical care with a physician, sometimes referred to as a “warm handoff.” Another strategy includes having a physician either on-site or off-site to expedite linkage even further. The CBO program also offers evidence-based interventions such as ART and Access to Services (ARTAS) and HIV Navigation Services—STEPS to Care, to link PWH to HIV medical care.13,14 And, lastly, CBO program staff often represent the communities they serve and have access, familiarity, and comfort with the people they serve.
Literature that explores the relationship between social determinants of health and linkage to HIV medical care is limited. However, a recent CDC analysis found that rates of linkage to HIV medical care were significantly lower among people living in counties with higher poverty levels than among people living where <13% of the population live below the federal poverty level, among people in counties with lower rates of health insurance coverage than where <12% of the population lacked health insurance, and among people in counties with lower education levels than where <13% of the population had less than a high school diploma. 15 The CBO program is working to bridge some of these gaps for PWH. CBOs continue to operate in the space between health and social care, relying on their expertise and person-centered approach to overcome barriers to linkage and care for HIV. In addition to ARTAS and STEPS to Care, evidence-based interventions such as Stay Connected for Your Health and PROMISE for HIP allow CBO staff to address individuals’ barriers to HIV medical care and access to ART.16,17 These interventions, among others, improve aspects of their clients’ social determinants of health, which otherwise may keep them from receiving the care they need.18,19
Limitations
Our findings were subject to at least 2 limitations. First, the lack of contextual data on factors such as health insurance, economic barriers, and stigma limited our ability to address why linkage-to-care rates were lower among some sociodemographic and population groups. Second, some cell sizes in this analysis were small, which reduced the power of the overall analysis.
Conclusion
Our analysis indicates that the CBO program is effective in linking newly diagnosed HIV-positive people to HIV medical care, which is important in the HIV care continuum and for viral suppression (which can reduce HIV transmission). Paired with other recent results, these data show that the CBO program fills a critical need by testing and rapidly linking to care newly diagnosed HIV-positive people who are at high risk for acquiring HIV, such as people living in the South, transgender women, and people in racial and ethnic minority groups. 11
Our analysis shows that CDC’s HIV prevention program for CBOs is well-positioned and needed to help end the HIV epidemic. An important lesson learned is that personalized services should be considered for all CDC-funded HIV prevention programs. The CBO program creates affirming spaces for people and staff who represent the population, creating a successful model for enhanced linkage to care and improved outcomes for PWH. To improve rates of viral suppression and outcomes for PWH more broadly, it is important for CDC to continue supporting the CBO program in its efforts to provide HIV testing, rapid linkage to HIV medical care, and support to programs that address the social determinants of health, including housing, racism, and homophobia.
Footnotes
Acknowledgements
The authors acknowledge and thank Gary Uhl, PhD, Translation and Evaluation Branch, Division of HIV Prevention, National Center for HIV, Viral Hepatitis, STD, and TB Prevention, Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.