
Abstract
Objectives
To reduce the number of new HIV infections and improve HIV health care outcomes, the social conditions in which people live and work should be assessed. The objective of this study was to describe linkage to HIV medical care by selected demographic characteristics and social determinants of health (SDH) among US adults with HIV at the county level.
Methods
We used National HIV Surveillance System data from 42 US jurisdictions and data from the American Community Survey to describe differences in linkage to HIV medical care among adults aged ≥18 with HIV infection diagnosed in 2017. We categorized SDH variables into higher or lower levels of poverty (where <13% or ≥13% of the population lived below the federal poverty level), education (where <13% or ≥13% of the population had <high school diploma), and health insurance coverage (where <12% or ≥12% of the population lacked health insurance). We calculated prevalence ratios (PRs) and 95% CIs.
Results
Of 33 204 adults with HIV infection diagnosed in 2017, 78.4% were linked to HIV medical care ≤1 month after diagnosis. Overall, rates of linkage to care were significantly lower among men and women living in counties with higher versus lower poverty (PR = 0.96; 95% CI, 0.94-0.97), with lower versus higher health insurance coverage (PR = 0.93; 95% CI, 0.92-0.94), and with lower versus higher education levels (PR = 0.97; 95% CI, 0.96-0.98).
Conclusions
Increasing health insurance coverage and addressing economic and educational disparities would likely lead to better HIV care outcomes in these areas.
Keywords
More than 1.1 million people in the United States were living with HIV in 2016. 1 In 2017, almost 40 000 adults and adolescents received an HIV diagnosis. 2 Despite previous declines, the annual number of new HIV infections was stable from 2013 to 2016. 2 -4 To reduce HIV transmission in the United States, several federal initiatives were implemented, including Ending the HIV Epidemic: A Plan for America. 5 Components of these initiatives focus on efforts to increase linkage to HIV medical care and understand the social determinants of health (SDH) that affect HIV-related care outcomes. 2,6,7
After diagnosis, linkage to care is a crucial stage in the HIV care continuum. Although immediate referral to HIV care is recommended, linkage is often delayed for many people. A Centers for Disease Control and Prevention (CDC) report found lower linkage rates among Black/African American people (hereinafter referred to as Black people), adolescents and young adults aged 13-24, and males with infection attributed to male-to-male sexual conduct and injection drug use (MMSC/IDU). 8 Most research has focused on demographic characteristics such as race/ethnicity and age to describe differences in linkage to care and other HIV health outcomes; however, SDH can provide insight on other pertinent characteristics, which may help increase understanding about the effects of the shortage or absence of health and treatment resources on the HIV care continuum.
SDH are overlapping social structures and economic systems (eg, social and physical environments, health services, structural and societal factors) that contribute to health inequities. 9 Although several studies identified socioeconomic barriers among people with HIV including, but not limited to, poverty, 10 -14 lack of health insurance coverage, 15 -17 and low education level, 18 -20 few have explored associations between linkage to care and SDH in various geographic areas (urban, metropolitan, rural) of the United States. The objective of our study was to describe linkage to care among adults with diagnosed HIV by demographic and SDH characteristics at the county level.
Methods
HIV Surveillance Data
We analyzed data from CDC’s National HIV Surveillance System (NHSS) 21 for adults aged ≥18 with HIV diagnosed in 2017 to determine linkage to care within 1 month of diagnosis. 21 We measured linkage to care by documentation of ≥1 CD4+ T-lymphocyte test (CD4 test) (measured as a count in cells/μL or as a CD4 percentage of total lymphocytes) or ≥1 viral load test (measured as copies/mL) performed ≤1 month after diagnosis, the standard used by CDC. 3 Our analysis included data from 42 jurisdictions (41 states and the District of Columbia) with complete reporting of CD4 and viral load test results to CDC as of December 2018. Data from these jurisdictions represent 87.9% of all adults who received a diagnosis of HIV in the United States in 2017. We analyzed linkage to care for selected characteristics (sex at birth, age, race/ethnicity, and transmission category) and by population of residence (metropolitan [≥500 000 population], urban [50 000-499 999 population], or rural [<50 000 population]). We adjusted data in transmission category to account for people with missing data on risk factors. 22 We did not seek institutional review board approval for this study because our research was a public health activity and did not involve human subjects.
Census Data
We obtained county-level data for 3 SDH variables (federal poverty level [FPL], education level, and health insurance coverage) from the US Census Bureau’s American Community Survey (ACS) 5-year estimates. 23 We calculated the proportion of residents who were living below the FPL at any time during the 12 months before the survey response, the proportion of residents with less than a high school diploma, and the proportion of residents without health insurance or a health coverage plan.
Analysis
We linked NHSS data for adults aged ≥18 with HIV diagnosed in 2017 with ACS data by county of residence at diagnosis. We categorized SDH variables into 2 levels of poverty, education, and health insurance coverage using the median values of poverty, education, and health insurance coverage from all counties in the 42 areas as cut points. We based the cut points on the medians of the empirically derived quartiles for poverty level, education level, and health insurance coverage (13%, 12%, and 12%, respectively). We excluded cases or counties when no county information was available for the case, no SDH information was available for the county, or we could not match the county indicated in the surveillance data with a county indicated in the ACS.
We calculated prevalence ratios (PRs) and 95% CIs by using the SAS GENMOD procedure (SAS Institute, Inc) to assess significant differences in linkage to care between adults with HIV diagnosed in 2017 residing in counties at or above the SDH variable cut point and adults with HIV diagnosed in 2017 in counties below the SDH variable cut point. We assessed significance using 95% CIs, where we considered values significant if the 95% CIs did not include 1. Linkage to care within 1 month of diagnosis was the outcome category, and the low-level SDH groups (<13% living below FPL, <12% without health insurance, and <13% with <high school diploma) were the referent groups.
Results
Linkage to Care
Among adults in the 42 areas, 33 381 received an HIV diagnosis during 2017 and 33 204 (99%) met study inclusion criteria. Of the 33 204 adults included in analysis, 26 033 (78.4%) were linked to care ≤1 month after diagnosis (Table 1). Among men, by age group, the prevalence of linkage to care was lowest among men aged 18-24 (74.6%). By race/ethnicity, the prevalence of linkage was lowest among Black people (74.6%), and by transmission category, linkage was lowest among men with infection attributed to MMSC/IDU (75.5%). By county of residence, linkage was lowest among men in urban areas (77.1%).
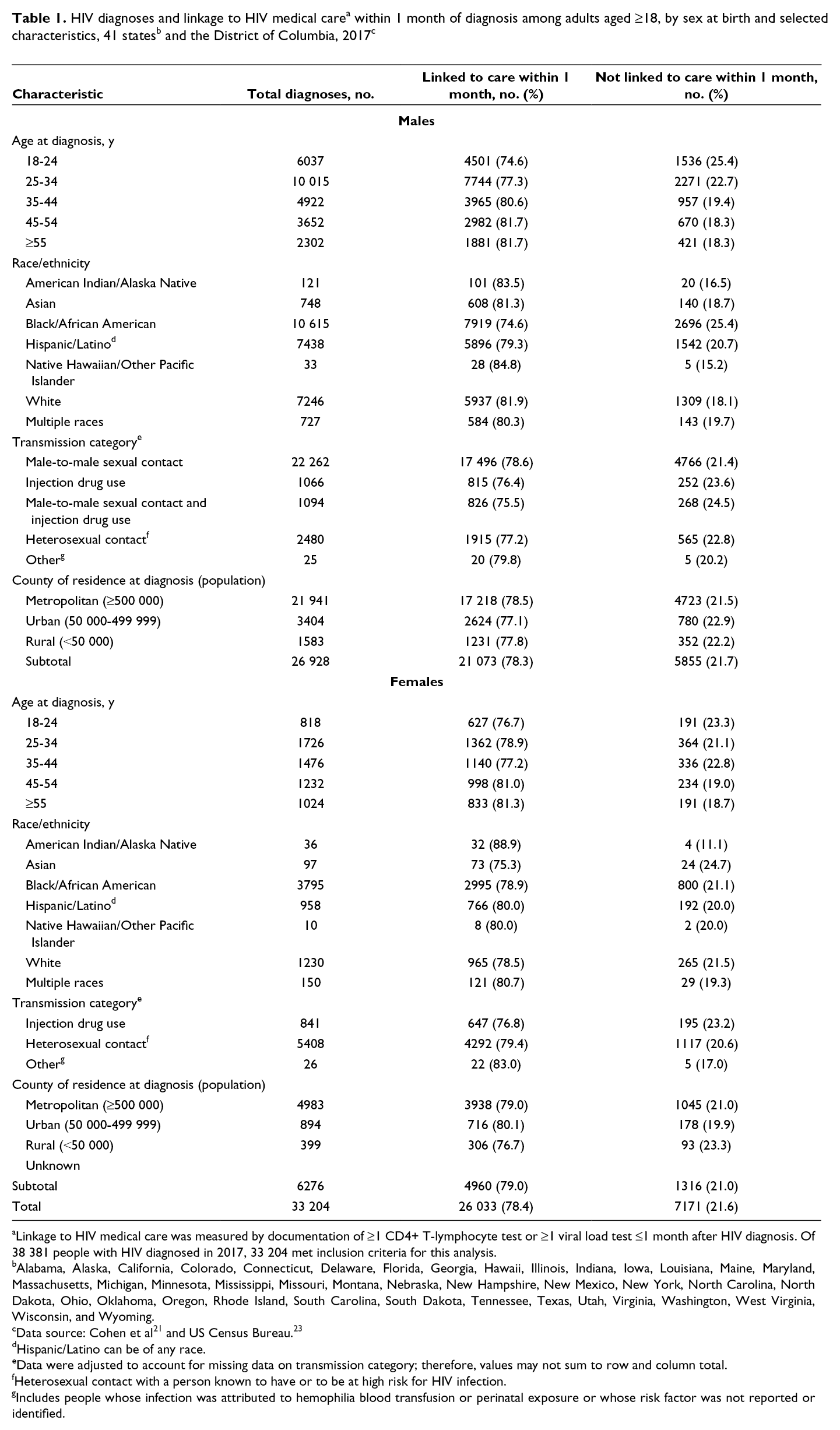
aLinkage to HIV medical care was measured by documentation of ≥1 CD4+ T-lymphocyte test or ≥1 viral load test ≤1 month after HIV diagnosis. Of 38 381 people with HIV diagnosed in 2017, 33 204 met inclusion criteria for this analysis.
bAlabama, Alaska, California, Colorado, Connecticut, Delaware, Florida, Georgia, Hawaii, Illinois, Indiana, Iowa, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Oregon, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, Washington, West Virginia, Wisconsin, and Wyoming.
dHispanic/Latino can be of any race.
eData were adjusted to account for missing data on transmission category; therefore, values may not sum to row and column total.
fHeterosexual contact with a person known to have or to be at high risk for HIV infection.
gIncludes people whose infection was attributed to hemophilia blood transfusion or perinatal exposure or whose risk factor was not reported or identified.
Among women, by age group, the prevalence of linkage to care was lowest among women aged 18-24 (76.7%). By race/ethnicity, linkage was lowest among Asian people (75.3%), and by transmission category, linkage was lowest among women who injected drugs (76.8%). By county of residence, linkage was lowest among men in rural areas (76.7%).
Linkage to Care and FPL
Overall, among adults with HIV diagnosed in 2017, 21 000 (63.2%) resided in counties where ≥13% of the residents lived below the FPL (Table 2). The prevalence of linkage to care was lower among adults in counties with higher poverty than among adults in counties with lower poverty (77.1% vs 80.7%; PR = 0.96; 95% CI, 0.94-0.97).
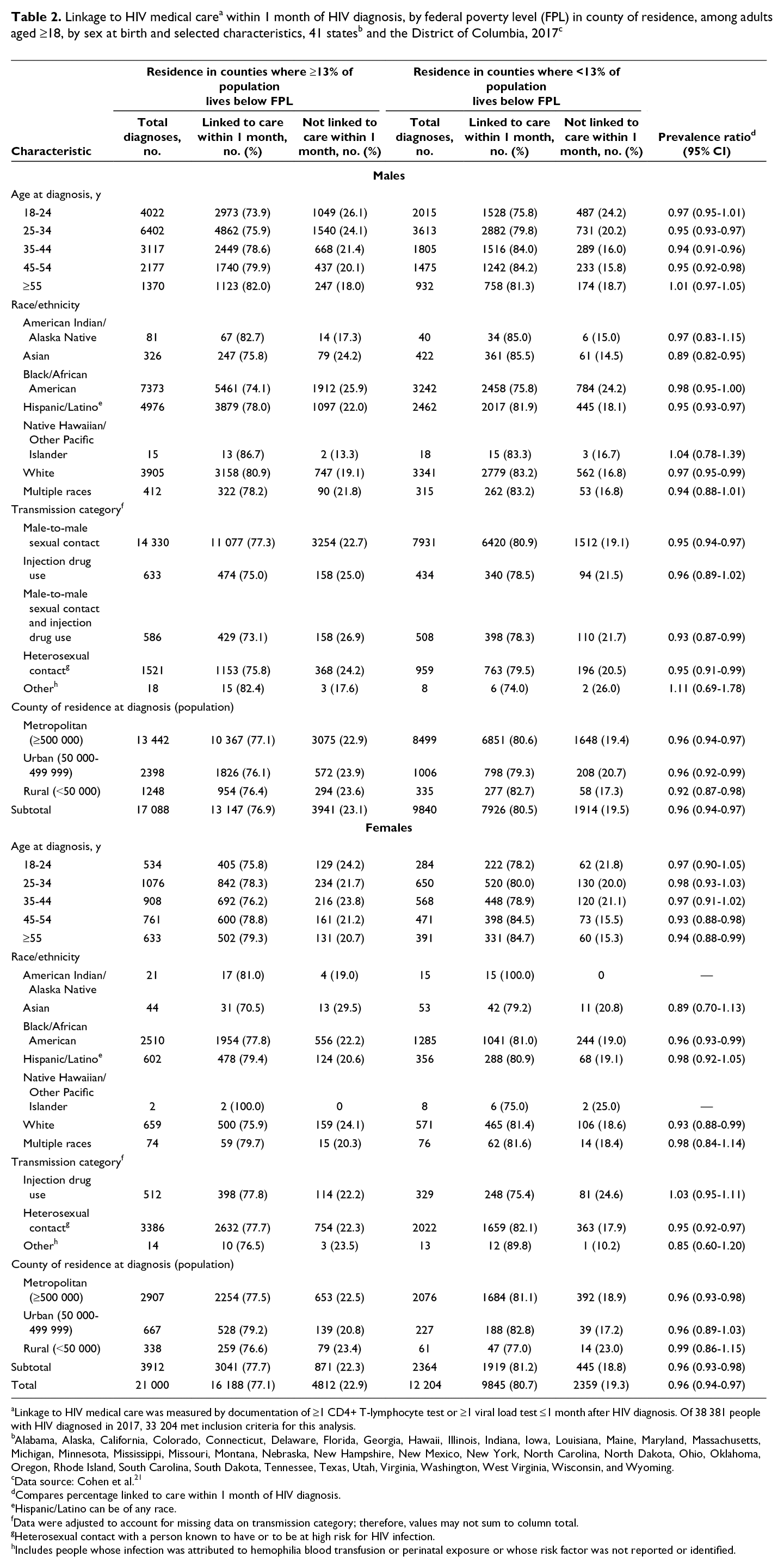
aLinkage to HIV medical care was measured by documentation of ≥1 CD4+ T-lymphocyte test or ≥1 viral load test ≤1 month after HIV diagnosis. Of 38 381 people with HIV diagnosed in 2017, 33 204 met inclusion criteria for this analysis.
bAlabama, Alaska, California, Colorado, Connecticut, Delaware, Florida, Georgia, Hawaii, Illinois, Indiana, Iowa, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Oregon, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, Washington, West Virginia, Wisconsin, and Wyoming.
cData sources: Cohen et al. 21
dCompares percentage linked to care within 1 month of HIV diagnosis.
eHispanic/Latino can be of any race.
fData were adjusted to account for missing data on transmission category; therefore, values may not sum to column total.
gHeterosexual contact with a person known to have or to be at high risk for HIV infection.
hIncludes people whose infection was attributed to hemophilia blood transfusion or perinatal exposure or whose risk factor was not reported or identified.
Among males, linkage to care was lower in counties with higher poverty than in counties with lower poverty (PR = 0.96; 95% CI, 0.94-0.97) by age, for males aged 35-44 (PR = 0.94; 95% CI, 0.91-0.96), 25-34 (PR = 0.95; 95% CI, 0.93-0.97), and 45-54 (PR = 0.95; 95% CI, 0.92-0.98); by race/ethnicity, for Asian (PR = 0.89; 95% CI, 0.82-0.95), Hispanic/Latino (PR = 0.95; 95% CI, 0.93-0.97), and White (PR = 0.97; 95% CI, 0.95-0.99) males; by transmission category, for males with infection attributed to MMSC/IDU (PR = 0.93; 95% CI, 0.87-0.99), males with MMSC (PR = 0.95; 95% CI, 0.94-0.97), and males with heterosexual contact (PR = 0.95; 95% CI, 0.91-0.99); and by population of residence, in rural (PR = 0.92; 95% CI, 0.87-0.98), metropolitan (PR = 0.96; 95% CI, 0.94-0.97), and urban (PR = 0.96; 95% CI, 0.92-0.99) areas.
Among females, linkage to care was lower in counties with higher poverty than in counties with lower poverty (PR = 0.96; 95% CI, 0.93-0.98) by age, for females aged 45-54 (PR = 0.93; 95% CI, 0.88-0.98) and ≥55 (PR = 0.94; 95% CI, 0.88-0.99); by race/ethnicity, for White (PR = 0.93; 95% CI, 0.88-0.99) and Black (PR = 0.96; 95% CI, 0.93-0.99) females; by transmission category, for infection attributed to heterosexual contact (PR = 0.95; 95% CI, 0.92-0.97); and by population of residence, in metropolitan areas (PR = 0.96; 95% CI, 0.93-0.98).
Linkage to Care and Health Insurance Coverage
Overall, among adults with HIV diagnosed in 2017, 22 169 (66.8%) adults resided in counties with lower insurance coverage, where ≥12% of residents did not have health insurance (Table 3). Linkage to care was lower among adults in counties with lower health insurance coverage than among adults in counties with higher health insurance coverage (PR = 0.93; 95% CI, 0.92-0.94).
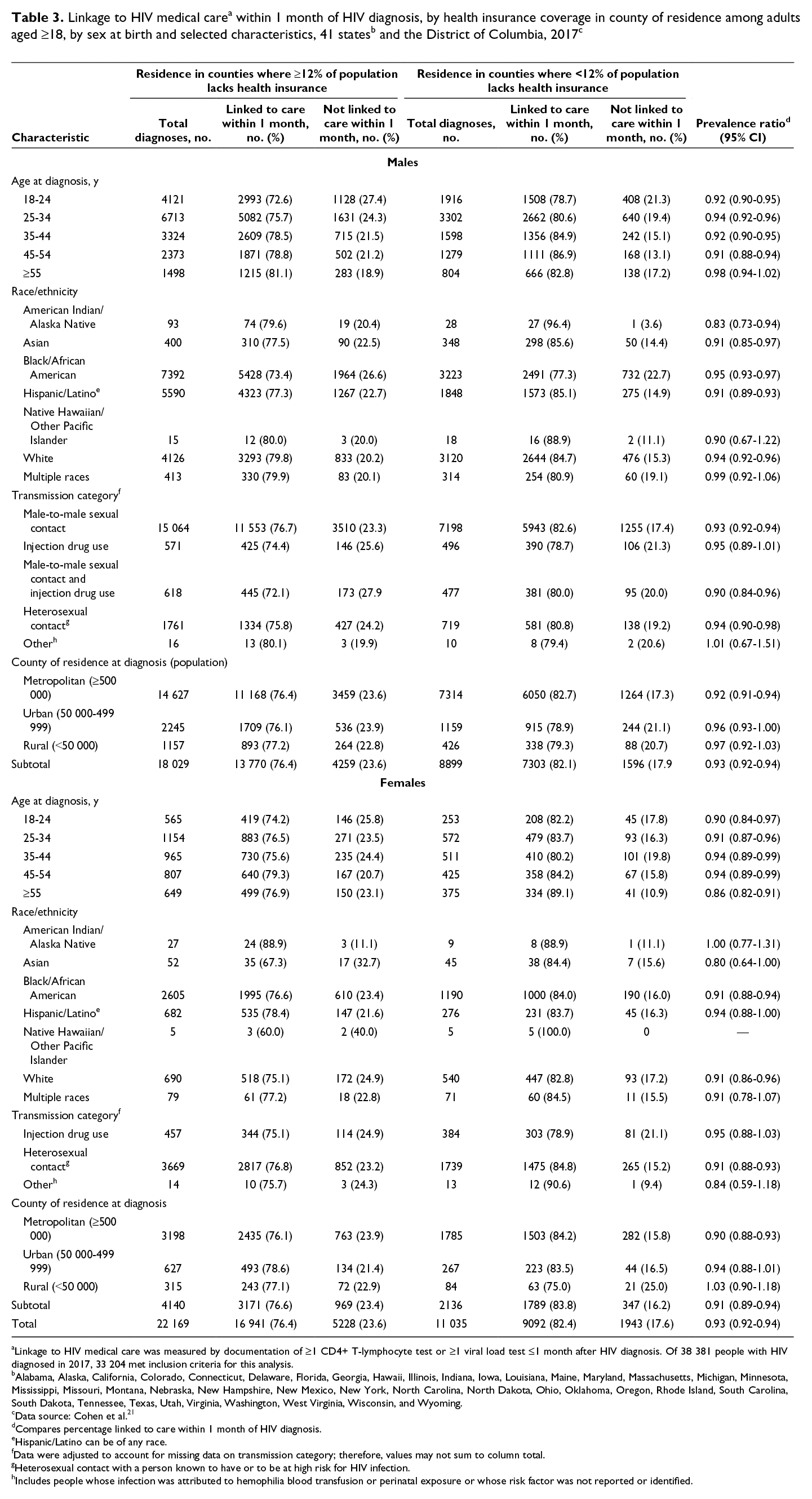
aLinkage to HIV medical care was measured by documentation of ≥1 CD4+ T-lymphocyte test or ≥1 viral load test ≤1 month after HIV diagnosis. Of 38 381 people with HIV diagnosed in 2017, 33 204 met inclusion criteria for this analysis.
bAlabama, Alaska, California, Colorado, Connecticut, Delaware, Florida, Georgia, Hawaii, Illinois, Indiana, Iowa, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Oregon, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, Washington, West Virginia, Wisconsin, and Wyoming.
cData source: Cohen et al. 21
dCompares percentage linked to care within 1 month of HIV diagnosis.
eHispanic/Latino can be of any race.
fData were adjusted to account for missing data on transmission category; therefore, values may not sum to column total.
gHeterosexual contact with a person known to have or to be at high risk for HIV infection.
hIncludes people whose infection was attributed to hemophilia blood transfusion or perinatal exposure or whose risk factor was not reported or identified.
Among males, linkage to care was lower in counties with lower health insurance coverage than in counties with higher health insurance coverage (PR = 0.93; 95% CI, 0.92-0.94) by age, for males aged 18-24 (PR = 0.92; 95% CI, 0.90-0.95), 25-34 (PR = 0.94; 95% CI, 0.92-0.96), 35-44 (PR = 0.92; 95% CI, 0.90-0.95), and 45-54 (PR = 0.91; 95% CI, 0.88-0.94); by race/ethnicity, for American Indian/Alaska Native (PR = 0.83; 95% CI, 0.73-0.94), Asian (PR = 0.91; 95% CI, 0.85-0.97), Hispanic/Latino (PR = 0.91; 95% CI, 0.89-0.93), White (PR = 0.94; 95% CI, 0.92-0.96), and Black (PR = 0.95; 95% CI, 0.93-0.97) males; by transmission category, for males with infection attributed to MMSC/IDU (PR = 0.90; 95% CI, 0.84-0.96), males with MMSC (PR = 0.93; 95% CI, 0.92-0.94), and males with heterosexual contact (PR = 0.94; 95% CI, 0.90-0.98); and by population of residence, in metropolitan areas (PR = 0.92; 95% CI, 0.91-0.94).
Among females, linkage to care was lower in counties with lower health insurance coverage than in counties with higher health insurance coverage (PR = 0.91; 95% CI, 0.89-0.94) by age, for females aged 18-24 (PR = 0.90; 95% CI, 0.84-0.97), 25-34 (PR = 0.91; 95% CI, 0.87-0.96), 35-44 (PR = 0.94; 95% CI, 0.89-0.99), 45-54 (PR = 0.94; 95% CI, 0.89-0.99), and ≥55 (PR = 0.86; 95% CI, 0.82-0.91); by race/ethnicity, for Black (PR = 0.91; 95% CI, 0.88-0.94) and White (PR = 0.91; 95% CI, 0.86-0.96) females; by transmission category, for infection attributed to heterosexual contact (PR = 0.91; 95% CI, 0.88-0.93); and by population of residence, in metropolitan areas (PR = 0.90; 95% CI, 0.88-0.93).
Linkage to Care and Education Level
Overall, among adults with HIV diagnosed in 2017, 16 372 (49.3%) adults resided in counties with lower education levels, where ≥13% of residents had less than a high school diploma (Table 4). Linkage to care was lower among adults in counties with lower education levels than among adults in counties with higher education levels (PR = 0.97; 95% CI, 0.96-0.98).
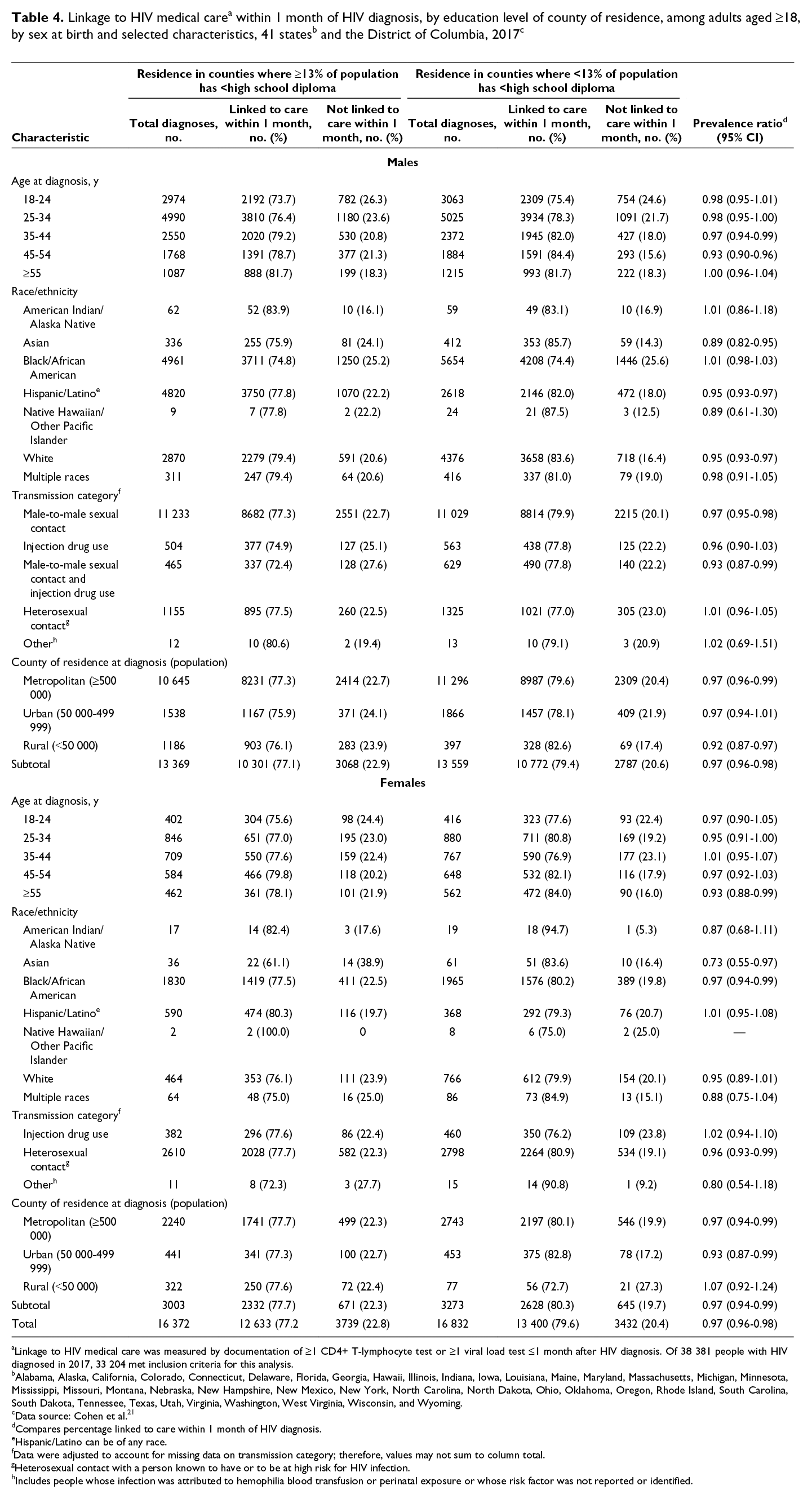
aLinkage to HIV medical care was measured by documentation of ≥1 CD4+ T-lymphocyte test or ≥1 viral load test ≤1 month after HIV diagnosis. Of 38 381 people with HIV diagnosed in 2017, 33 204 met inclusion criteria for this analysis.
bAlabama, Alaska, California, Colorado, Connecticut, Delaware, Florida, Georgia, Hawaii, Illinois, Indiana, Iowa, Louisiana, Maine, Maryland, Massachusetts, Michigan, Minnesota, Mississippi, Missouri, Montana, Nebraska, New Hampshire, New Mexico, New York, North Carolina, North Dakota, Ohio, Oklahoma, Oregon, Rhode Island, South Carolina, South Dakota, Tennessee, Texas, Utah, Virginia, Washington, West Virginia, Wisconsin, and Wyoming.
cData source: Cohen et al. 21
dCompares percentage linked to care within 1 month of HIV diagnosis.
eHispanic/Latino can be of any race.
fData were adjusted to account for missing data on transmission category; therefore, values may not sum to column total.
gHeterosexual contact with a person known to have or to be at high risk for HIV infection.
hIncludes people whose infection was attributed to hemophilia blood transfusion or perinatal exposure or whose risk factor was not reported or identified.
Among males, linkage to care was lower in counties with lower education levels than in counties with higher education levels (PR = 0.97; 95% CI, 0.96-0.98) by age, for males aged 35-44 (PR = 0.97; 95% CI, 0.94-0.99) and 45-54 (PR = 0.93; 95% CI, 0.90-0.96); by race/ethnicity, for Asian (PR = 0.89; 95% CI, 0.82-0.95), Hispanic/Latino (PR = 0.95; 95% CI, 0.93-0.97), and White (PR = 0.95; 95% CI, 0.93-0.97) males; by transmission category, for males with infection attributed to MMSC/IDU (PR = 0.93; 95% CI, 0.87-0.99) and MMSC (PR = 0.97; 95% CI, 0.95-0.98); and by population of residence, in rural (PR = 0.92; 95% CI, 0.87-0.97) and metropolitan (PR = 0.97; 95% CI, 0.96-0.99) areas.
Among females, linkage to care was lower in counties with lower education levels than in counties with higher education levels (PR = 0.97; 95% CI, 0.94-0.99) by age, for females aged ≥55 (PR = 0.93; 95% CI, 0.88-0.99); by race/ethnicity, for Asian (PR = 0.73; 95% CI, 0.55-0.97) and Black (PR = 0.97; 95% CI, 0.94-0.99) females; by transmission category, for infection attributed to heterosexual contact (PR = 0.96; 95% CI, 0.93-0.99); and by population of residence, in urban (PR = 0.93; 95% CI, 0.87-0.99) and metropolitan (PR = 0.97; 95% CI, 0.94-0.99) areas.
Discussion
For adults with diagnosed HIV in 2017 in the United States, our analysis found lower rates of linkage to care in the overall population and among males with infection attributed to MMSC/IDU, for adults residing in areas characterized by the 3 SDH extremes of higher poverty, lower health insurance coverage, and lower education levels. Linkage was lowest among males aged 45-54 in counties with lower health insurance coverage and lower education levels, among Asian and Hispanic/Latino males in counties with higher poverty and lower education levels, among males residing in rural areas with higher poverty and lower education levels, and among White and Black females in counties with higher poverty and lower health insurance coverage.
Few studies have examined SDH and linkage to care in the United States, and direct comparisons of findings are limited because of differences in the outcomes measured and populations observed. However, in general, we found that most studies support our overall findings of lower linkage to care among people residing in high-poverty areas and areas with low health insurance coverage. 24 -27 These findings may be attributed to factors such as lack of social support services, socioeconomic instability, and limited public transportation and highlight that structural and societal factors such as social and physical environments, and availability, cost of, and access to health services, may create barriers to HIV care. 24 -27 Identifying the limitations to accessing care and the SDH factors that may contribute to these limitations is critical and will provide insight on additional factors associated with lower rates of linkage to care in the United States.
For results across race/ethnicity, we found that Asian and Hispanic/Latino males residing in counties with higher poverty and lower education levels had lower rates of linkage to care. Several studies on HIV health outcomes among Asian people in the United States have suggested that cultural, behavioral, and belief factors must be addressed to increase linkage-to-care rates among Asian people in general. 28,29 A study of Latino men in large US cities found factors such as limited education, inadequate health insurance, language barriers, and migration contribute to poor health outcomes in the Hispanic/Latino population, which can directly and indirectly affect opportunities to be linked to HIV care. 30,31 Considering the heterogeneous nature of Asian and Latino populations, it may be beneficial to disaggregate these populations for better insight in future analyses.
In our study, linkage-to-care rates were low among White and Black females in counties with higher poverty and lower health insurance coverage. Although national surveillance data on health outcomes and SDH found lower linkage-to-care rates among White women in counties with lower poverty, additional studies are needed to provide better insight into the effect of SDH on care outcomes in this population. 14 Although recent studies have not analyzed SDH and linkage to care among Black women, some studies do support our findings of lower linkage-to-care rates among Black women in high-poverty areas. 13,32,33 A study of Florida residents found that non-initiation of care increased as poverty level increased and as the density of non-Hispanic Black people increased. 34 Limited access to quality health care, housing, transportation, and HIV education, in addition to stigma, discrimination, and fear, may directly affect linkage-to-care rates among Black women. 32,33
By population of residence, linkage to care was lowest among males residing in rural areas with higher poverty and lower education levels than among males in counties with lower poverty and higher education levels. People living in rural areas of the United States may be at a disadvantage for accessing and receiving HIV care, and HIV-related stigma is greater in rural areas than in large urban communities. 35,36 Although a study of care outcomes by geographic population found greater linkage-to-care rates among people in rural areas than in urban and metropolitan areas in the United States, 37 additional barriers such as living in an area of high poverty or low education generally affect other HIV-related outcomes, such as retention in care and adherence to treatment to attain viral suppression. 18
Linkage-to-care rates were lower among young adults aged 18-24 than among adults in other age groups. Surveillance studies have found that 44% of undiagnosed HIV infections and 21% of new HIV diagnoses in the United States are among adolescents and young adults, 1,2 and this group is less likely than other age groups to be retained in care and to be virally suppressed. 3,38 Adolescents and young adults often face challenges to testing, entry, and maintenance of HIV care, which include limited transportation, underemployment, stigma and fear, and low levels of family support, which affect their decision making on care options. 27,39 Understanding these barriers and other SDH factors is critical and will provide insight for work to improve linkage to care among young adults. 40 In addition, increasing the availability of adolescent-friendly, culturally competent, confidential, and convenient health services may facilitate access to HIV care for this population. 41
Limitations
Our analysis had several potential limitations. First, data were available from 42 jurisdictions with complete reporting of HIV-related laboratory data to CDC. These 42 areas represent 87.9% of all HIV diagnoses that occurred in the United States in 2017 and, as such, may not be representative of all people with diagnosed HIV infection in the United States. Third, because all people with HIV have not been tested and/or reported, the number and percentage of people linked to care may not be representative of all adults with diagnosed HIV infection in the 42 areas in 2017. Fourth, use of county-level aggregated data for this ecological analysis may not accurately reflect or represent the SDH environment at the individual level. Finally, although some SDH indicators may be correlated (eg, lack of education has been associated with both poverty and low income in the United States), 42,43 we did not analyze correlations between SDH indicators in our study.
Conclusions
Although health outcomes of people with HIV infection have improved in the past decade, some populations are disproportionately affected. 8 Prevention interventions need to be supplemented to address underlying factors such as poverty, lack of health insurance, and lack of education. A key strategy of the Ending the HIV Epidemic initiative is to reduce HIV transmission through interventions that improve rates of viral suppression. 4,5,7 Linkage to care is the gateway to receiving prompt and proper HIV treatment for the attainment and maintenance of viral suppression. Increasing low- to no-cost health insurance options among low-income populations would likely lead to better HIV care outcomes for these populations. In addition, increased use of peer navigators and allied health workers and the development of targeted campaigns may improve linkage-to-care rates among groups that are at high risk of having poor HIV health outcomes. Future studies are needed to analyze the relative effects of both county-level and individual poverty, education, and health insurance measures to inform whether variance in linkage is attributed to individual or aggregate county SDH, or both.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.