
Abstract
Objectives:
The risk for mpox virus (MPXV) transmission in most workplaces has not been thoroughly assessed in the context of the 2022 global mpox outbreak. Our objectives were to describe mpox case patients who worked while infectious and the subsequent workplace contact tracing efforts, risk assessments, and outcomes.
Methods:
The Centers for Disease Control and Prevention requested information from health departments in the United States in September 2022 to identify people with confirmed or probable mpox who worked outside the home while infectious, either before or after diagnosis, from June 1 through August 31, 2022. We collected and summarized data on demographic, clinical, and workplace characteristics of case patients and workplace contact investigations. We stratified data by industry and occupation categories.
Results:
In total, 102 case patients were reported by 6 jurisdictions. The most common industries were accommodation and food services (19.8%) and professional business, management, and technical services (17.0%). Contact investigations identified 178 total contacts; 54 cases (52.9%) had no contacts identified. Of 178 contacts, 54 (30.3%) were recommended to receive postexposure prophylaxis (PEP) and 18 (10.1%) received PEP. None of the contacts developed a rash or were tested for orthopox or mpox, and none were reported to have confirmed or probable mpox.
Conclusion:
Data from 6 jurisdictions suggest that the risk of MPXV transmission from workers to others in workplace settings in many industries is low. These findings might support future updates to exposure risk classifications and work activity recommendations for patients. These findings also demonstrate the importance of collecting and analyzing occupation and industry data in case reports to better understand risks in workplaces.
Mpox (formerly known as monkeypox) is a disease caused by infection with the mpox virus (MPXV). MPXV is part of the Orthopoxvirus genus and Poxviridae family. MPXV typically spreads through close physical contact with lesions, scabs, or bodily fluids of a person with mpox. Patients with mpox are considered infectious from the time symptoms start until the rash has fully healed and a fresh layer of skin has formed. Isolation is recommended for the duration of the illness. 1 People with mpox who are unable to remain fully isolated throughout their illness are recommended to avoid close physical contact, cover their lesions, and wear a well-fitted face mask. 1
The first US case of mpox in the 2022 global mpox outbreak was reported in May 2022. As of July 2023, more than 30 000 confirmed and probable cases of mpox had been reported to the Centers for Disease Control and Prevention (CDC), with most occurring during June, July, and August 2022. 2 Early in the outbreak, CDC became aware of several case patients who worked while infectious prior to diagnosis and provided consultation on contact tracing and risk assessment. The risk for MPXV transmission in workplaces during the 2022 US outbreak has not been systematically assessed, and workplace information was not included in national case-based surveillance. To help understand whether transmission from workers to others occurred, CDC invited health departments from US jurisdictions (state, territorial, and large cities) to report data from patients with confirmed and probable mpox who worked during their infectious period. The objectives of this study were to describe mpox case patients, their workplace characteristics, and the subsequent workplace contact investigations, risk assessments, and outcomes.
Methods
In September 2022, CDC requested via email retrospective information from health departments from US jurisdictions, including states, territories, and large cities, to identify people with confirmed or probable mpox infection who worked outside of the home while infectious at any time either before or after diagnosis, as determined by the responding jurisdiction through interviews with case patients. The infectious period was defined as having prodromal symptoms, including fever, malaise, headache, and sore throat and/or the presence of a rash until after all the scabs had fallen off and a fresh layer of intact skin formed. We used CDC definitions for confirmed and probable cases, 3 which are based on laboratory evidence. We then used unique case identification numbers to link to complete records for each case in the CDC surveillance database. Other inclusion criteria were illness onset date during June 1–August 31, 2022, active contact tracing performed by the health department in the workplace, and conclusion of the monitoring period for contacts. Each health department determined which cases warranted a workplace contact tracing investigation based on the nature of the work and local contact tracing capacity. Health departments assessed the potential case contact events and used CDC definitions of high, intermediate, and low risk of exposure to determine exposure risks and recommendations. 4 Workplace contacts could be coworkers, clients, patients, and anyone else present in the workplace. One state passed the request on to local health departments. Data collection began September 2022 and ended January 2023.
CDC requested information on symptoms, work-related characteristics, and activities and details on workplace contact tracing. Other constitutional symptoms included fatigue, headache, malaise, myalgia, abdominal pain, night sweats, and sore throat. In addition, we defined respiratory symptoms to include cough or nasal congestion; ocular symptoms to include conjunctivitis, pink eye, or eye lesions; rectal symptoms to include pain, bleeding, or tenesmus; and genitourinary symptoms to include dysuria, inguinal pain, genital lesions, or discharge.
We used free-text work-related descriptions provided by the health departments to assign each case a 2-digit industry (type of workplace) and 2-digit occupation (job title) code from the 2012 North American Industry Classification System 5 and 2010 Standard Occupational Classification system 6 with the help of the National Institute for Occupational Safety and Health Industry and Occupation Computerized Coding System. 7 When an industry or occupation had a small number of case patients, we summarized the data and stratified the data by a broadened industry or occupation category. For example, the professional, business, management, and technical services industry category included information, finance, and insurance; professional, scientific, and technical services; and public administration industries. The professional, business, and management occupation category included management; business and financial operations; computer and mathematical; architecture and engineering; life, physical, and social science; community and social services office; and administrative support occupations.
This activity was reviewed by CDC, deemed not research, and conducted consistent with applicable federal law and CDC policy.
Results
Four states, 1 federal district, and 1 county health department provided data (Table 1). During the study period, 3912 cases were reported to the 6 participating jurisdictions. Of these, 102 case patients worked while infectious, and a workplace contact tracing investigation was performed during June 1–August 31, 2022. The District of Columbia, which performed a contact tracing investigation for most of its reported cases during the study period, reported 60 cases (58.8% of all cases). Four case patients worked in a reporting jurisdiction but resided in a different jurisdiction. The 102 case patients included 67 confirmed and 35 probable cases. Month of illness onset included June (n = 27), July (n = 48), and August (n = 27).
Demographic and occupational characteristics of case patients with mpox who worked while infectious (N = 102), 6 US jurisdictions, June 1–August 31, 2022

Unless otherwise indicated.
The District of Columbia performed contact tracing investigations on most of its reported cases during June 1–August 31, 2022, while the other jurisdictions did not.
Three case patients worked in Florida but resided in other states.
One case patient worked in Vermont but resided in another state.
Four case patients worked in 2 jobs in 2 industries while infectious.
Industry categories with 0 cases were mining, quarrying, and oil and gas extraction; wholesale trade; real estate; and management of company and enterprises.
This industry category includes information, finance, and insurance; professional, scientific, and technical services; and public administration.
Four case patients worked in 2 jobs in 2 occupations while infectious. Occupation categories with 0 cases were protective services; farming, fishing, and forestry; and military occupations.
This occupation category includes management; business and financial operations; computer and mathematical; architecture and engineering; life, physical, and social science; community and social services office; and administrative support occupations.
The median age of case patients was 34 (range, 17-62) years; 97 case patients (95.1%) identified as cisgender male (Table 1). Most case patients identified as White (59.8%) or Black or African American (34.3%) race and as non-Hispanic ethnicity (71.6%).
The most common industries of patients were accommodation and food services (19.8% of case patients); professional, business, management, and technical services (17.0%); and health care and social assistance (16.0%). The accommodation and food services industries consisted primarily of restaurants and bars and a few hotels. The most common occupations were professional, business, and management (34.0% of case patients) and food preparation and serving-related occupations (15.1%). Most (51.9%) patients worked while ill for 1 day (range, 1-14 days). The most common symptoms reported while working were rash (79.4% of case patients), other constitutional symptoms (56.9%), and fever and/or chills (30.4%). Of the 81 case patients with rash, the most common rash locations were genitals (39.5%), arms (39.5%), trunk (35.8%), face (35.8%), and legs (33.3%). Thirty-one patients (38.3%) reported covering their lesions while working; 24 (23.5%) reported wearing a face mask while working. However, information about covering of lesions and face mask wearing was missing for most case patients.
For 54 of 102 case patients (52.9%), no contacts were identified (ie, no risk of exposure; Table 2). Contact investigations for 48 case patients identified a total of 178 contacts, including 21 contacts determined to have a high risk of exposure, 45 contacts who had an intermediate risk, and 112 contacts who had a low risk (Table 3). Of 178 total contacts, 54 (30.3%) were recommended to receive postexposure prophylaxis (PEP) with JYNNEOS (Bavarian Nordic) vaccine; 18 of 178 contacts (10.1%) received PEP. Two contacts developed symptoms: 1 contact had an enlarged lymph node and 1 contact had diarrhea; neither developed a rash and neither was tested. No other contacts were tested for orthopox virus or MPXV.
Summary characteristics of workplace contact investigations (N = 102) during the 2022 US mpox virus outbreak, 6 US jurisdictions, June 1–August 31, 2022
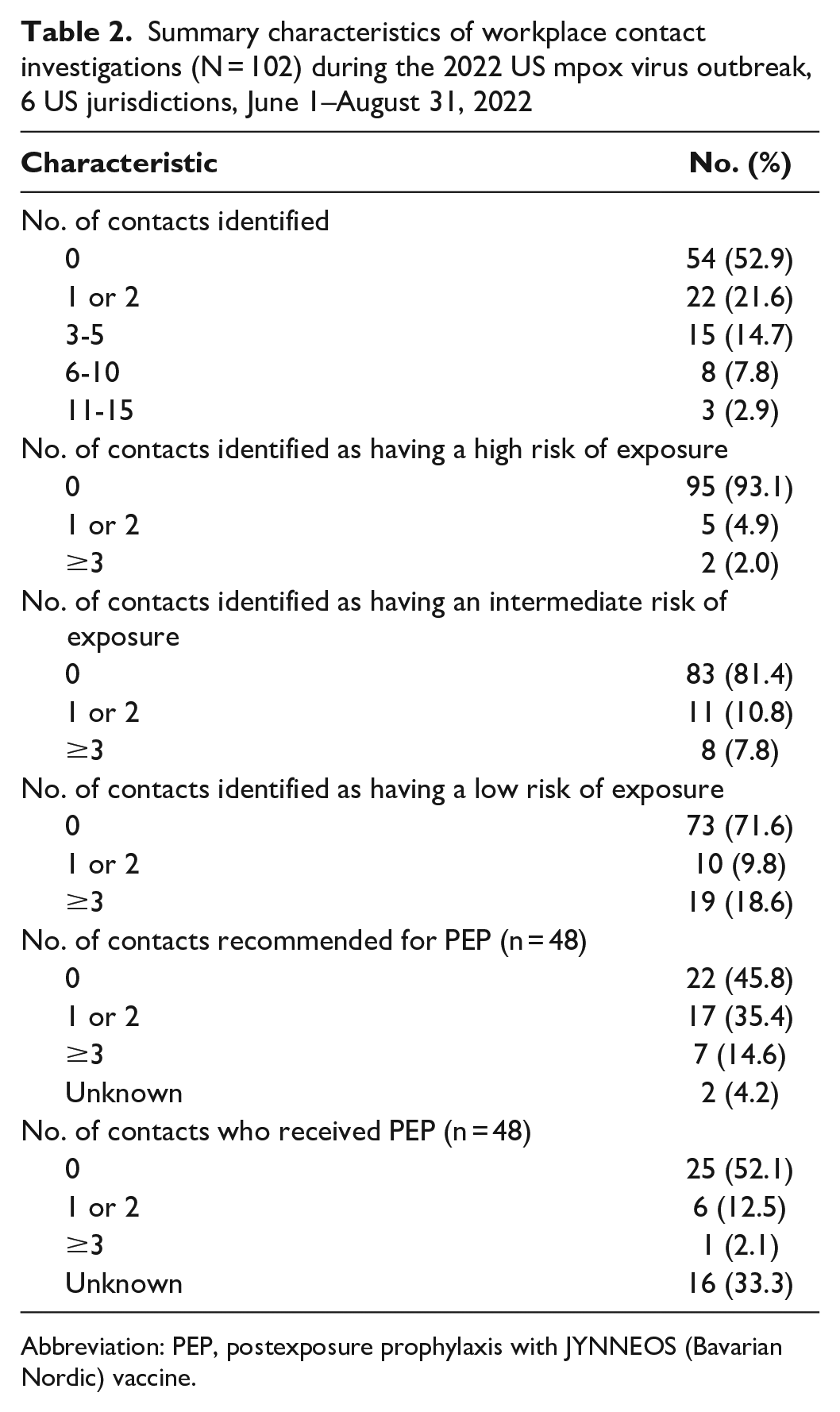
Abbreviation: PEP, postexposure prophylaxis with JYNNEOS (Bavarian Nordic) vaccine.
Summary characteristics of workplace contacts (N = 178) during the 2022 US mpox virus outbreak, 6 US jurisdictions, June 1–August 31, 2022
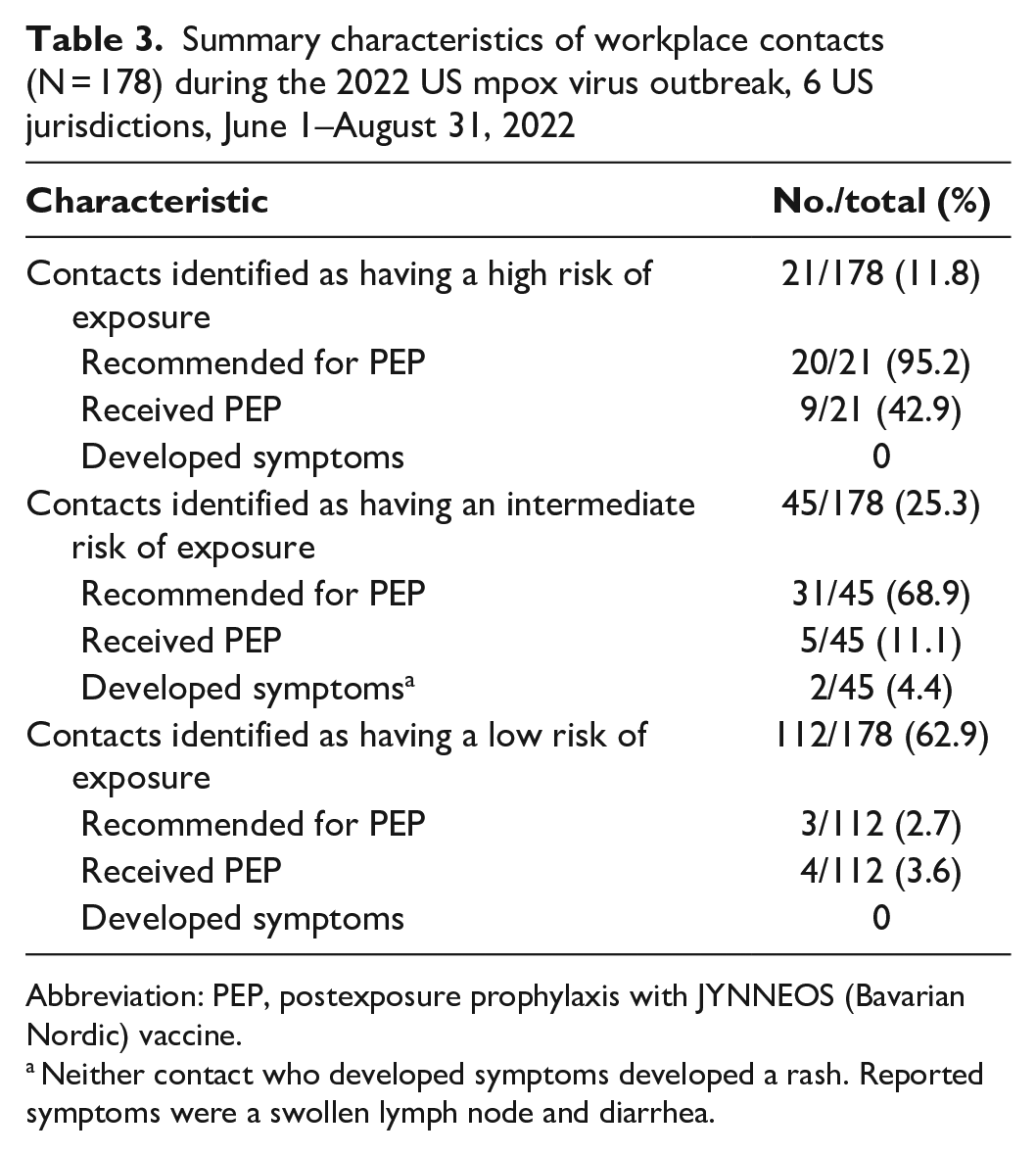
Abbreviation: PEP, postexposure prophylaxis with JYNNEOS (Bavarian Nordic) vaccine.
Neither contact who developed symptoms developed a rash. Reported symptoms were a swollen lymph node and diarrhea.
Of the 26 case patients with ≥3 contacts identified, the most common industries were accommodation and food services (n = 7) and health care and social assistance (n = 6). The most common occupations among this group were professional, business, and management (n = 6) and health care (n = 5) occupations. Of the 54 case patients with no contacts identified, the most common industries were professional business, management, and technical services (n = 15); accommodation and food services (n = 7); and retail trade (n = 7). The most common occupations among this group were professional, business, and management (n = 23) and food preparation and serving-related occupations (n = 7).
Discussion
Workplaces have historically been identified as a source of transmission for multiple infectious diseases. 8 However, in the United States, outbreak data suggest that community transmission of MPXV in 2022 occurred mainly as a result of sexual or close intimate contact.9,10 Our findings among 102 case patients in 6 jurisdictions revealed a low risk of mpox transmission from symptomatic infected workers to others in workplaces in various industries and occupations. Most case patients who worked while ill had no contacts or few contacts in the workplace. Most contacts were considered low-risk exposures, and we found no evidence of secondary transmission.
While there have been rare reports of transmission in health care settings, these transmissions have occurred from patient to health care personnel and mostly via needlestick injuries.11-15 The risk of transmission from infected patients to health care personnel in the United States is low.16,17 There have been no known reports of transmission from health care personnel to patients or coworkers. In our study, 17 patients reported working while ill in the health care industry, and there was no reported secondary transmission. Other contact investigations in community settings such as correctional facilities and airplanes revealed no reports of secondary transmission.18-20 Our study identified 3 case patients who worked in the transportation industry, including the airline and cruise industries, but no case patients who worked in correctional settings. Although work-related information for the first case patient with mpox diagnosed in the United States in the 2022 outbreak was not disclosed, 35 coworkers of this case patient were determined by investigators to have low or uncertain risk of exposure. 17 In an mpox outbreak among 20 patrons in a piercing and tattoo establishment in Spain, the 1 worker at the establishment was not reported to have been infected. 21 One study looking at surface contamination in an office environment occupied by a worker with mpox in the United Kingdom found low-level contamination by polymerase chain reaction in 3 of 34 samples. 22 The professional, business, and management industries and occupations were among the most common in our sample, and this type of work does not typically include skin-to-skin contact.
Limitations
Our findings were subject to some limitations. First, our sample was a passively collected convenience sample, which limited the generalizability of the risk of workplace transmission to all industries nationwide. Second, the health departments used different approaches to case investigations and subsequent workplace contact tracing, which may have led to selection bias. For example, 1 health department conducted a contact investigation for most of their cases but had some missing data; other states conducted contact investigations on fewer of their cases but had more complete data for the information requested. Third, our sample did not include any patients who worked in the sex industry, in which a higher risk of transmission may exist. Fourth, we had limited information on work activities for many case patients and whether they worked before or after diagnosis. Therefore, we could not make any conclusions on factors that were associated with working while infectious. Fifth, data were missing on the use of face masks and covering of lesions. Finally, we were unable to discern whether contacts were coworkers, clients, or others present in the workplace.
Conclusion
These data from 6 US jurisdictions suggest that the risk of MPXV transmission is low from workers to others in workplace settings in many industries. These findings might support future updates to exposure risk classifications and work restriction recommendations for patients. This evaluation also demonstrates the importance of collecting and analyzing occupation and industry data in case reports to better understand risks in workplaces.
Authors’ Note
Footnotes
Acknowledgements
We acknowledge the following people for assistance in data analysis: Jennifer Cornell, Matthew Groenewold, Stacy Marovich, and Jeffrey Purdin, Centers for Disease Control and Prevention. We acknowledge the following people for assistance in coordinating data collection and compilation: Sarah Gillani, Karla Miletti, Allison Morrow, and Selin Prasad, District of Columbia Department of Health; Kevin Cormier, Emma Creegan, Stephanie Doyle, Lara Grenier, Karen Luther, Patricia McAuley, Elizabeth Nahod, and Alyson Thurber, Rhode Island Department of Health; Julie Hand, Jenna Iberg Johnson, Gillian Richardson, and Emma Ortega, Louisiana Department of Health; and Megan Gumke, Florida Department of Health.
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.