
Abstract
Objectives:
To assess the prevalence of sleep disturbance among patients evaluated at a clinic for patients afflicted with Post-acute sequelae of COVID-19 (PASC).
Methods:
Sleep disturbance was assessed with the Patient-Reported Outcomes Measurement Information System-Sleep Disturbance (PROMIS-SD) framework among adult patients of the PASC clinic.
Results:
Among 312 patients, the mean age was 46.2 years, and 70.2% were women. About 41.0% of patients had no sleep disturbance; sleep disturbance was mild to moderate in 51.3% and severe in 7.7%. PROMIS-SD score was negatively correlated with the time from the initial positive COVID-19 test to the initial consultation in the PASC clinic (Pearson r = −.094; r2 = .0088).
Conclusions:
The PROMIS-Sleep Disturbance framework can serve as a tool to assess the burden of sleep disturbances in PASC patients.
Introduction
Since the emergence of the COVID-19 pandemic, an increasing number of persons have experienced post-acute sequelae of COVID-19 (PASC). PASC is defined by the Centers for Disease Control and Prevention as symptoms lasting more than 4 weeks after infection with the SARS-CoV-2 virus. 1 The World Health Organization defines post-COVID-19 condition (PCC; also termed long COVID) as persistent or new symptoms approximately 3 months after acute infection by the SARS-CoV-2 virus and lasting at least 2 months. 2 One report estimated that the incidence of 1 or more long-lasting symptoms of COVID-19 ranges from 13% to 80%. 3 Reported symptoms have included fatigue, dyspnea, headache, anosmia, poor sleep, and disturbed circadian rhythms, all of which compromise well-being. 3
During the pandemic, the International COVID-19 Sleep Study (ICOSS) began a collaboration across Europe, Asia, and North and South America to investigate the effects of the pandemic and social isolation on sleep, circadian rhythms, and the mental health of the population. 4 The ICOSS found an increase in sleep problems resulting in deterioration of mental health and well-being, particularly in evening-types, despite increased flexibility in sleep-wake behavior. 2 Studies to determine the effect of COVID-19 on sleep and symptom persistence could lead to treatments to mitigate the negative effects on mental health and physical well-being. 2
Patients with PASC present a challenge in identifying disturbances across different organ systems. Patient-reported outcome assessments serve as tools to help clinicians assess a patient’s symptoms and severity of disturbances. The Patient-Reported Outcomes Measurement Information System (PROMIS) is an initiative by the National Institutes of Health focusing on measuring patients’ physical, mental, and social well-being. 5 PROMIS Sleep Disturbance (SD) item banks were also developed and validated to assess the sleep-wake function of patients. A recent meta-analysis estimated the pooled prevalence of sleep disturbances in PASC patients at 46%. The analysis centered on studies that assessed burden by using standardized sleep disturbance questionnaires, including the Pittsburgh Sleep Quality Index (PSQI), A single-item sleep quality scale (SQS), insomnia severity index (ISI), the Athens insomnia scale (AIS), and the Epworth sleepiness scale (ESS). 6 However, there is limited data in assessing the burden of sleep disturbances using the PROMIS-SD framework.
In this study, we aimed to assess the presence of sleep disturbance and the severity of sleep dysfunction among patients with PASC by using the PROMIS-SD questionnaire.
Methods
This study was reviewed by the Institutional Review Board and deemed exempt (#21-008343). A retrospective review of the electronic health record was completed for adult patients (age >18 years) who were enrolled in the PASC clinic from May 1, 2021, through September 30, 2022. Each patient received various patient-reported outcome measures, including the PROMIS-SD form (PROMIS Bank v1.0—Sleep Disturbance [computerized adaptive test]). The PROMIS-SD questionnaire is administered on a computer using an algorithm to select questions based on previous patient responses. 7 The PROMIS-SD questionnaires are scored to follow a normal distribution, with a mean (SD) T-score of 50 (10) points. PROMIS-SD scores higher than 50 indicate a higher level of sleep disturbance. 8 Prior analyses have established thresholds of PROMIS-SD T-scores of 55, 60, and 70 as cutoffs for mild, moderate, and severe sleep disturbance, respectively. 9
Each chart review encounter included identification of age, gender, and body mass index (BMI). A search was conducted in the chart to evaluate for any prior diagnosis of obstructive sleep apnea. The initial visit with the PASC clinic included information on the initial date of diagnosis and whether the patient was hospitalized for treatment of COVID-19, including any intensive care unit treatment. The time elapsed between the initial diagnosis and the patient’s first visit to the PASC clinic was also determined. Each patient’s health record was also reviewed for ongoing symptoms and medical history. Specifically, a history of fatigue and snoring was done. Furthermore, the patient’s history was also evaluated for any presence of any prior mental health diagnosis. Specifically, the chart was reviewed for the presence of any previous diagnosis of anxiety and/or depression. Each patient had completed PRO forms before the initial visit to the PASC clinic. The PROMIS-SD results were obtained through chart review, including the standardized score, which the Electronic Medical Record (EMR) automatically provided. Pearson product-moment correlation was determined to evaluate the relationship between PROMIS-SD score and time from COVID-19 positivity to PASC clinic visit. Lastly, each patient’s chart was reviewed for whether they underwent any objective testing for a sleep disorder with polysomnography.
Results
A total of 312 patient health records were identified and reviewed. For our cohort, 2 (1%) patients identified as “American Indian/Alaskan Native,” 3 (1%) as “Asian,” 16 (5%) as “Black,” 265 (85%) as “Non-Hispanic Caucasian,” 17 (5%) as “Hispanic,”1 (0.3%) as Pacific Islander, and 8 (3%) as “Not Disclosed/Other.”
The mean (SD) age was 46.2 (8.4) years, and 219 patients (70.2%) were women. The mean (SD) BMI was 30.0 (8.0). The weight distribution of the patients was 2.9% underweight (n = 9), 24.4% healthy weight (n = 76), 27.6% overweight (n = 86), 23.7% obese class 1 (n = 74), 10.3% obese class 2 (n = 32), and 10.6% obese class 3 (n = 33), with missing data for 2 patients (0.6%). Overall, 24.7% of patients (n = 77) had hypertension, and 22.2% (n = 69) had a prior diagnosis of obstructive sleep apnea. Many patients had a history of mental health problems documented at any point in their health record, with 76.9% (n = 240) diagnosed with anxiety and 64.4% (n = 201) diagnosed with depression. A total of 73 patients (23.4%) required COVID-related hospitalization, and of those, 16 (21.9%) required intensive care unit-level care.
The mean (SD) PROMIS-SD score overall was 57.3 (8.4), with scores indicating normal results for 41.0% (n = 128), mild sleep disturbance for 24.4% (n = 76), moderate sleep disturbance for 26.9% (n = 84), and severe sleep disturbance for 7.7% (n = 24). The average PROMIS-SD was 52.5 for “American Indian/Alaskan Native,” 51.0 for “Asian,” 58.6 for “Black,” 57.1 for “Non-Hispanic Caucasian,” 60.2 for “Hispanic,” 56 for the sole patient who identified as “Pacific Islander,” and 59.8 for the “Not Disclosed/Other” group.
The average date of COVID-19 positivity was March 19, 2021, and the average PASC clinic visit was on February 12, 2022—a mean (SD) time from COVID-19 positivity to visit of 329 (194) days. Of the 312 patients, 108 (34.6%) had an oximetry study at a mean (SD) of 64 (67) days after PASC clinic visit; the mean oxygen desaturation index was 5.7 (9.5), with a mean duration of 7.4 (21.8) minutes at an oxygen saturation of 88% or less. Of the 312 patients, 35 (11.2%) underwent polysomnography, a mean (SD) of 169 (123) days after the PASC clinic visit; the mean apnea-hypopnea index was 11.4 (15.5), and the mean duration at an oxygen saturation of 88% or less was 5.4 (11.3) minutes. The Pearson correlation coefficient for the relationship between PROMIS-SD score and the time from initial COVID-19 positivity to PASC clinic visit was r = −.094 (r2 = .0088; Figure 1).
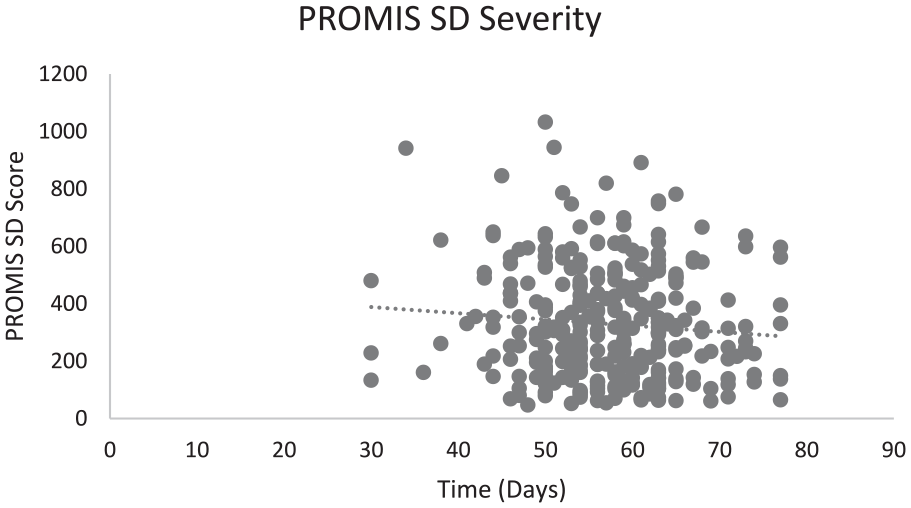
PROMIS scores and the number of days from COVID-19 positivity to PASC clinic visit.
Discussion
In this work, we assessed the sleep quality of 312 patients of the PASC clinic by using the PROMIS-SD. Our results showed a sleep disturbance prevalence of 59% in our patient population, as outlined by the PROMIS scoring criteria. Specifically, 24.4% had mild sleep disturbance, 26.9% had moderate sleep disturbance, and 7.7% had severe sleep disturbance. In comparison, a recent meta-analysis estimates a pooled prevalence of sleep disturbances at 46% (95th percentile confidence interval of 38%-54%). 6 Differences in study sample sizes, the definition of sequelae, reported symptoms and duration of symptoms contribute to the wide range in reported prevalence. Our findings using the PROMIS-SD framework have not significantly deviated from the range found in the meta-analysis noted above. 6 Our results provide preliminary support that the PROMIS framework, specifically the sleep disturbance domain, can be used to assess the presence of sleep disturbance. Furthermore, PROMIS-SD is correlated to other sleep questionnaires, such as the Pittsburgh Sleep Quality Index (PSQI) and Insomnia Severity Index. 5
Persons with PCC symptoms (duration >3 months), which are like those of myalgia, encephalomyelitis, or chronic fatigue, 10 often have sleep disorders. 11 Studies are ongoing to determine the clinical features of PCC. Risk factors for PASC include advanced age; race and ethnicity other than non-Hispanic White; severe acute infection; more than 5 symptoms in the first week of acute infection; obesity, dyspnea, or chest pain as a presenting symptom on acute onset; comorbid conditions including asthma; and physical deconditioning from acute illness.3,12,13 Our cohort’s self-reported ethnicity was predominantly non-Hispanic Caucasian (85%) versus 5% for Black and 5% for Hispanic. Our cohort was not as heterogeneous as the general American population, estimated to be 57.8% non-Hispanic Caucasian, 18.7% Hispanic, and 12.1% Black per 2020 census data (https://www.census.gov/library/stories/2021/08/2020-united-states-population-more-racially-ethnically-diverse-than-2010.html). However, both minority groups in our cohort showed relatively higher scores for sleep disturbance: 58.6 for Black patients and 60.2 for Hispanic patients, in comparison to 57.1 for non-Hispanic Caucasian patients. An analysis of a large set of patients using EMR data noted that PASC patients do exhibit differences in symptom onset and burden when examined through the lens of ethnicity. 14 However, specific data on ethnicity and sleep disturbance burden in PASC patients is lacking. The study only noted Black patients were reported to have a lower reported rate of sleep disorders as compared to Whites. 14 Before the pandemic, an emerging consensus was that socioeconomically disadvantaged groups, especially racial/ethnic minorities, have had difficulty achieving sleep and this should be considered when evaluating health outcomes. 15 Our results point to a potential increase in sleep disturbance severity for racial/ethnic minorities in the PASC patient population. However, our support for this conclusion is tempered by our relatively small sample size, and a less diverse sample as compared to the general American population. We hope future research examines sleep disturbance in a larger cohort of patients and examines patients for social determinants of health and sleep disturbances.
It is essential to study the role of sleep and circadian rhythms in relation to the risk of coronavirus infection, disease severity, and disease persistence because these profoundly affect immune and neural physiologic functions and mental well-being.4,16 Conversely, the neurologic effects of COVID-19 may increase sleep and mental health problems, including nightmares, insomnia, and depression. 17 Patient-reported outcome measures, like the PROMIS framework, can be easily deployed to assess the burden of symptoms across different domains.
Another analysis identified 3 studies that assessed sleep disturbance using a PSQI cutoff of 16 to 21; for these studies, the pooled prevalence of sleep disturbance was 19%. 18 Of note, a global PSQI score greater than 5 is typically used to identify poor sleep quality, and therefore, use of this lower cutoff would most likely lead to a higher prevalence. 18 The same meta-analysis also noted 6 studies that used other validated screening tools for sleep disturbance and reported a pooled prevalence of 29%; 4 studies reported a pooled prevalence of 42% with the use of invalidated screening tools. 18
The ICOSS has established 5 main hypotheses for sleep concerns associated with COVID-19: (1) COVID-19 involves the nervous system and is associated with excessive daytime sleepiness similar to postviral fatigue syndrome 19 ; (2) biological and psychological differences may be predisposing factors for PCC symptoms 3 ; (3) COVID-19 results in frequent dreaming and nightmares associated with severity and duration of the infection, pandemic restrictions, and socioeconomic changes4,20; (4) trauma and severe stress result in higher rates of nightmares and suicidal thoughts 2 ; and (5) COVID-19 results in increased risk of sleep disorders including rapid eye movement sleep behavior disorder, circadian dysfunction, insomnia, and sleepiness. 4 Our study also showed a weak negative correlation between the severity of the sleep disturbance and time elapsed since the initial positive COVID test (Figure 1). Evidence has emerged for brain-related abnormalities in patients with COVID-19, especially in the limbic and olfactory structures. 21 In prior cases, brainstem and limbic system impairments have been indicated in rapid-eye-movement sleep behavior disorder.22,23 Thus, the correlation in our study raises the question of whether the persistence of PASC symptoms, like sleep disturbance, is related to underlying structural changes in the brain.
There are clear limitations in our study, including a lack of controls and a small sample size. Furthermore, our study design of a cross-sectional study leads to a selection bias, and additionally, our study solely focused on the sleep disturbance part of the PROMIS domains. We hope future studies examine the burden of sleep disturbances with a control group (patients with a history of COVID-19 without PASC). Despite these limitations, our findings in our study do lay a pathway for additional studies to evaluate other PROMIS domains in the PASC patient population.
Footnotes
Acknowledgements
We thank the Division of Allergy, Pulmonary and Sleep Medicine and the PASC clinic for working together to study the effects of PCC on sleep. The Scientific Publications staff provided editorial consultation, proofreading, and administrative and clerical support.
Author Contributions
Mantavya Punj: Writing—original draft, reviewing and editing, Visualization, Validation, Methodology, Conceptualization, Formal analysis. Michael Schwartz: Data curation, Formal analysis, Methodology, Validation. Anjali Morris: Methodology, Validation, Formal analysis, Writing—review and editing. Joseph Cheung: Conceptualization, Visualization, Methodology, Writing—review and editing. Bala Munipalli: Writing—original draft, review and editing, Project administration, Resources, Supervision, Visualization, Conceptualization, Data curation, Formal analysis. All authors reviewed and agreed with the final draft.
Data Statement
All relevant data supporting the findings of this study are reported within the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.