
Abstract
Objective:
Employment is a well-documented social determinant of physical and mental health and can be used to determine who is disproportionately affected by public health emergencies. We examined trends in unemployment overall and by gender, by race or ethnic group, and by their interaction for 2 public health emergencies (the COVID-19 pandemic and the 2020 California wildfires).
Methods:
We obtained summary data files on the number of initial unemployment insurance (IUI) claims made in all 58 California counties from January 2018 through December 2021. We fit fixed-effects Poisson regression models to county data on weekly IUI claims cross-classified by gender and race or ethnic group. We used models to evaluate the overall effect of COVID-19, whether this effect changed over time increasing under compounding emergencies, and whether the overall and compounding effects of COVID-19 differed by gender and race or ethnic group.
Results:
During the COVID-19 pandemic, weekly IUI claims rates increased to as much as 10 times their prepandemic level. The increase in IUI claims for COVID-19 weeks, compared with weeks from the same month in the 2 years prior, was greater for women than for men of all race or ethnic groups, except for Black women. The higher rates of IUI claims for most women during COVID-19 entailed a reversal of prepandemic gender differences in claims that persisted through 2021.
Conclusion:
Public health officials should consider using IUI claims for surveillance of social determinants of health, particularly in the context of emergencies, which we show can have a persisting effect on the social patterning of social determinants. Future research is needed to forecast these affects and inform public health and policy mitigation and prevention strategies.
Monitoring upstream social determinants of health is a priority of the Public Health 3.0 call to action for public health leaders to “work across sectors to address social, environmental, or economic determinants of health.” 1 However, surveillance of these social determinants remains underdeveloped among public health surveillance systems. Employment is a critical social determinant of health,2-4 changing more rapidly than education status, age, or physical health. Employment can provide income, health insurance coverage, and social connections; in contrast, the lack of employment can result in substantial physical and mental distress. 5 Although the World Health Organization’s Commission on Social Determinants has emphasized the importance of tracking social determinants, the Commission has not provided viable options for specific unemployment indicators to monitor. 6 Relevant and sensitive unemployment indicators are needed to understand the mechanisms that contribute to or prevent health inequities among populations that are vulnerable to social determinants of health.
Although routine monitoring is critical, monitoring the social determinants of public health emergencies (PHEs)—which, much like social determinants, can have substantial and lasting effects on people’s physical and mental health—is especially important. 7 To our knowledge, few, if any, data sources are available to jurisdictions across the United States to track social determinants at the substate level in near-real time. 8 The effects of PHEs are unequally distributed across a population through various social and economic mechanisms, and, although PHEs often are found to further exacerbate existing health disparities, PHEs also can offer an opportunity to address the inequalities in wealth and power that result in health equities.9-11 In the context of PHEs, tracking changes in employment status by sociodemographic groups may provide critical information on who is disproportionately affected by the PHE and how those effects change over time.12,13 In addition, information on employment status could begin to inform theoretical models and research to better elucidate the mediating mechanisms among unemployment, health, and health inequities.
Since the 2008 recession, unemployment has historically been higher for men than for women and for Black women and men than for people in other racial and ethnic minority groups. 14 Using initial unemployment insurance (IUI) claims for California residents from the California Economic Development Department (EDD), we examined the effects of 2 cooccurring PHEs: the COVID-19 pandemic and the 2020 California wildfires. We considered whether and how these PHEs affected IUI claims for men and women of various race or ethnic groups. To our knowledge, our study is the first to examine such trends.
Methods
After establishing a data-use agreement with the California EDD, we obtained weekly counts of IUI claims for the 58 counties of California stratified by the claimants’ self-reported gender and race or ethnic group. To minimize the number counts that are too small to be disclosed, the EDD reports gender as male, female, or unknown and race or ethnic group as Native American or Alaskan Native (hereinafter referred to as American Indian or Alaska Native [AI/AN]), Asian, Black, Hispanic (hereinafter referred to as Latinx), White, or unknown. The EDD also provides slightly less granular public-use data through a dashboard in which counts of weekly, county-level IUI claims are reported by gender, by race or ethnic group, and by other categories (ie, industry, age group, or education). 15 We calculated IUI rates by using annual, county-level population counts stratified by gender, by race or ethnic group, and by the cross-classification of gender and race or ethnic group. The county-level population counts data are projected and publicly disseminated by the California Department of Finance, Demographic Research Unit. 16 The weekly IUI rates that we calculated cover the 4-year period from January 2018 through December 2021, during which 2 PHEs occurred: (1) the COVID-19 pandemic, for which claims were expected to be increased immediately after the California governor’s business closure mandate on March 19, 2020, and (2) the 2020 California wildfires, for which claims were expected to change over time and space for the 12 California counties that the US Federal Emergency Management Agency declared to be affected by wildfire disasters from August 22 through September 6, 2020.17-19 RAND’s Human Subjects Protection Committee (2019-0920-AM03) determined this study to be exempt from formal ethical review because we used publicly available data without personal identifiers.
We used difference-in-difference regression analysis to evaluate whether COVID-19 affected the weekly counts of IUI claims and whether IUI claims changed over time and across counties in a way that was consistent with the disaster declarations and disaster mandates. To overcome the limitations of the Stata version 17 poisson command for fitting complex data structures, we used a generalized linear model (with Poisson family specification) to estimate the differences in IUI rates while also weighting for the size of the respective strata (ie, county-specific gender by race or ethnic group population counts) and adjusting the SEs for clustering within these strata over time. Our most basic model evaluated the differences in IUI rates for the COVID-19 period (March 19, 2020–December 11, 2021) compared with the pre–COVID-19 period (January 2018–March 18, 2020), adjusting for differences by geography (county), demographic characteristics (gender, race or ethnic group, and their interaction), and seasonality (month and year).
We then evaluated whether the effect of COVID-19 on IUI claims changed over time, with an assessment of differences in the COVID-19 effect for the following 2 periods respective to all other COVID-19 weeks: (1) for the period of the California business closure mandate (March 28 through April 18, 2020) in all counties and (2) for the period of the California wildfires (August 22 through November 28, 2020) in the counties affected by the wildfires (Butte, Lake, Lassen, Mendocino, Monterey, Napa, San Mateo, Santa Clara, Santa Cruz, Shasta, Siskiyou, Solano, Sonoma, Stanislaus, Trinity, Tulare, and Yolo) (model 1, Table 1). We next evaluated whether the effect of COVID-19 on IUI claims differed across sociodemographic groups defined by gender (model 2, Table 1), by race or ethnic group (model 3, Table 1), and by the interaction of gender and race or ethnic group (model 4, Table 1). We tested but found no significant sociodemographic differences in the change in the effect of COVID-19 during either the business closure period (model 5, Table 1) or the California wildfires (model 6, Table 1). We tested goodness of fit (Wald statistics, Akaike information criterion, and Bayesian information criterion) to evaluate the improvements in model fit for sequential models that tested the change in the effect of COVID-19 over time, the demographic differences in the effect of COVID-19 overall, and the demographic differences in the change in the effect of COVID-19 over time. We predicted the expected changes in rates of weekly IUI claims during the PHEs by gender and race or ethnic group using the best-fitting model (model 4, Table 1).
Models assessing changes in rates of weekly initial unemployment insurance (IUI) claims during various phases of the COVID-19 public health emergency and after the 2020 California wildfires, California counties, 2018-2021 a
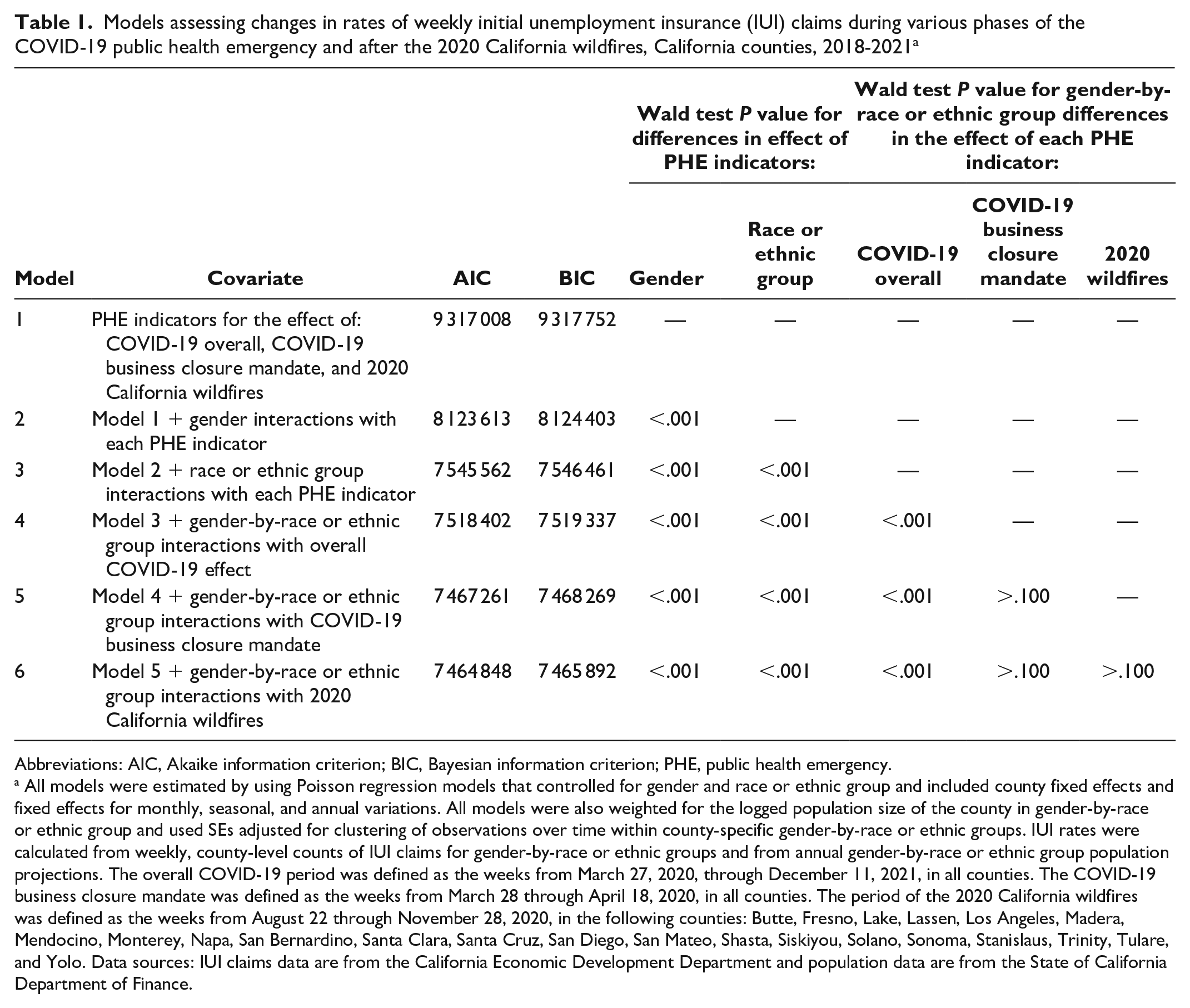
Abbreviations: AIC, Akaike information criterion; BIC, Bayesian information criterion; PHE, public health emergency.
All models were estimated by using Poisson regression models that controlled for gender and race or ethnic group and included county fixed effects and fixed effects for monthly, seasonal, and annual variations. All models were also weighted for the logged population size of the county in gender-by-race or ethnic group and used SEs adjusted for clustering of observations over time within county-specific gender-by-race or ethnic groups. IUI rates were calculated from weekly, county-level counts of IUI claims for gender-by-race or ethnic groups and from annual gender-by-race or ethnic group population projections. The overall COVID-19 period was defined as the weeks from March 27, 2020, through December 11, 2021, in all counties. The COVID-19 business closure mandate was defined as the weeks from March 28 through April 18, 2020, in all counties. The period of the 2020 California wildfires was defined as the weeks from August 22 through November 28, 2020, in the following counties: Butte, Fresno, Lake, Lassen, Los Angeles, Madera, Mendocino, Monterey, Napa, San Bernardino, Santa Clara, Santa Cruz, San Diego, San Mateo, Shasta, Siskiyou, Solano, Sonoma, Stanislaus, Trinity, Tulare, and Yolo. Data sources: IUI claims data are from the California Economic Development Department and population data are from the State of California Department of Finance.
Results
The weekly rates of IUI claims peaked for men and women in the week after the March 19, 2020, mandate that closed all nonessential businesses due to COVID-19, reaching more than 2000 claims per 100 000 people for both men and women (Figure 1). In the 2 years before the pandemic, weekly IUI rates were about 20-fold smaller at about 100 claims per 100 000 people, and rates were consistently higher among men than among women. In the week after the business closure mandate, IUI rates per 100 000 people for women peaked at nearly 2700 claims and exceeded rates for men by more than 350 claims. IUI rates for women remained higher than rates for men for most of 2020 and 2021. A second peak in IUI rates occurred in August and September 2020 concurrent with the California wildfire disaster declarations (at 1200-1400 claims per 100 000 people). After the wildfires, IUI rates declined gradually; by late 2021, they had dropped to a level close to that before the pandemic (about 100 claims per 100 000 people) (Figure 1).
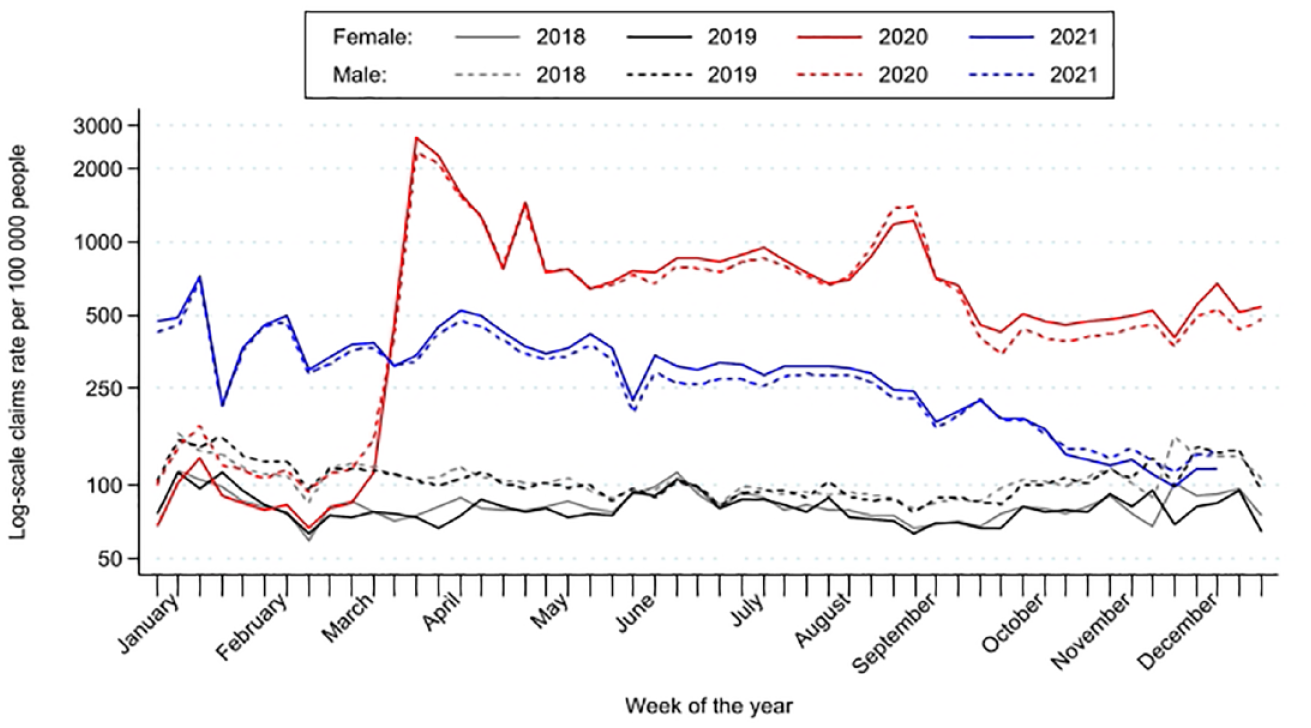
Weekly rates of initial unemployment insurance (IUI) claims by gender, California counties, 2018-2021. Data sources: IUI claims data are from the California Economic Development Department and population data are from the State of California Department of Finance.
When examining the PHE-associated increases in weekly IUI rates, we found variations over time and at the intersection of gender and race or ethnic group. Beginning with the March 2020 peak in IUI rates, IUI rates for women were greater than for men across all race or ethnic groups (Figure 2). In contrast, from January 2020 through the first 2 weeks of March 2020, only small differences between men and women in IUI claim rates were shown (ranging from 4 fewer claims for Black women vs Black men per 100 000 people to an average of 87 fewer claims for AI/AN women vs AI/AN men per 100 000 people). Consistent with the peak in IUI rates in the week after the business closure mandate, IUI rates peaked and remained higher among women than among men in all but 1 race or ethnic group. For Black men and women, IUI rates reversed to higher rates among women compared with men during the third week of March 2020 but then rapidly declined to lower than or about equal rates for women compared with men by the second week of April 2020.
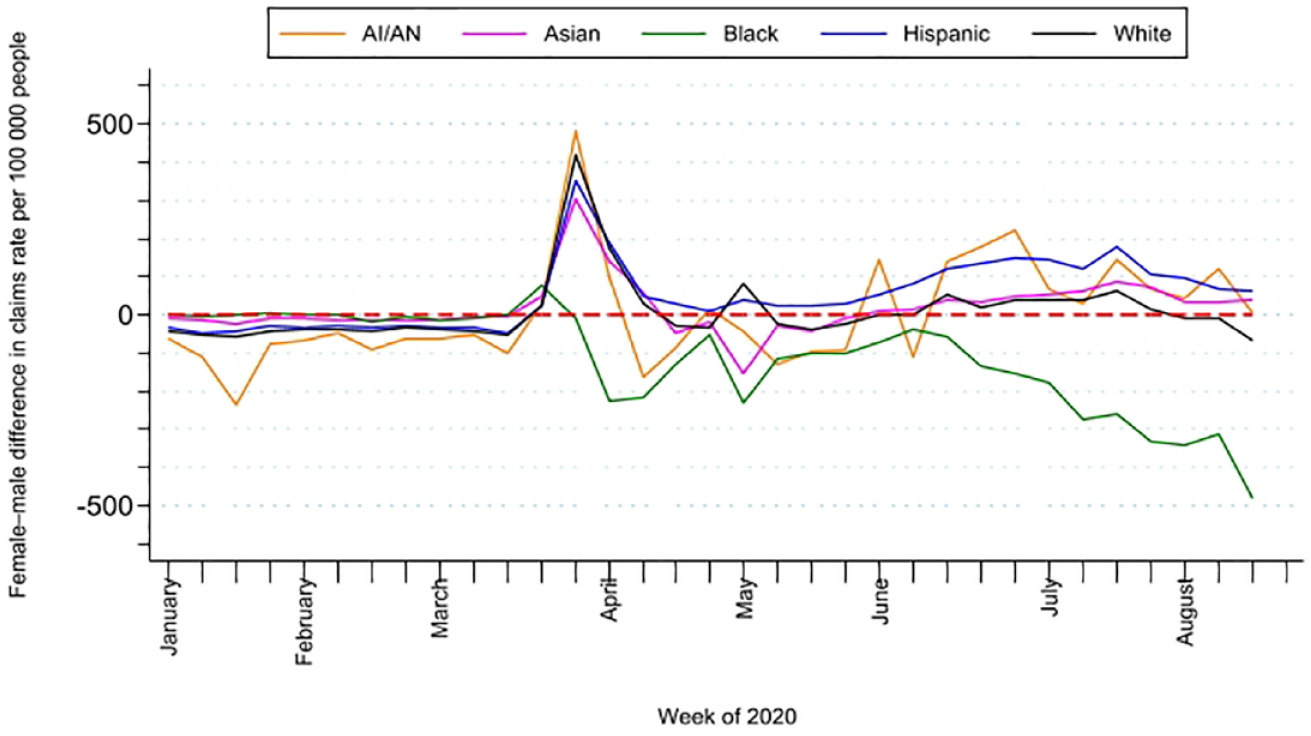
Gender differences in weekly rates of initial unemployment insurance (IUI) claims, by race or ethnic group, California counties, 2020. Gender difference is calculated from (female) – (male) IUI claims rates. Data sources: IUI claims data are from the California Economic Development Department and population data are from the State of California Department of Finance. Values of 0 (dashed line) indicate that weekly IUI rates were the same for women and men. Values >0 indicate that weekly IUI rates were greater for women than for men. Values <0 indicate that weekly IUI rates were greater for men than for women. Abbreviation: AI/AN, American Indian and Alaska Native.
Our statistical regression model strengthened the descriptive evidence (Figure 1, Figure 2). We determined that the set of PHE effects (COVID-19 overall, change in the COVID-19 effect during the business closure mandate, and change in the COVID-19 effect during the 2020 California wildfires) varied significantly by gender (P < .001) (model 2, Table 1) and by race or ethnic group (P < .001) (model 3, Table 1). Furthermore, gender differences in the overall COVID-19 effect also varied significantly by race or ethnic group, providing evidence for intersectionality in the COVID-19 effect (P < .001) (model 4, Table 1).
Overall Effect of COVID-19 on IUI Rates
The change in weekly IUI rates (predicted from model 4, Table 1) for COVID-19 months compared with prepandemic months from the previous 2 years increased significantly, with varied changes across race or ethnic groups. The smallest COVID-19 increases in rates (per 100 000 people) were for Latinx and White men and women (Table 2), ranging from 596 (95% CI, 553-638) more IUI claims during COVID-19 months than during prepandemic months for Latinx men to 714 (95% CI, 654-775) more claims during COVID-19 months than during prepandemic months for White women. The next largest COVID-19 increases were for Asian men (805 more claims; 95% CI, 749-862) and Asian women (915 more claims; 95% CI, 845-984); however, the 95% CIs were partially overlapping for Asian and White men (Table 2). The largest COVID-19 increases were for AI/AN and Black men and women (Table 2), ranging from 1292 (95% CI, 1091-1493) more claims for AI/AN men to 1375 (95% CI, 1300-1450) more claims for Black men.
Magnitude of predicted change in rates of weekly initial unemployment insurance (IUI) claims during COVID-19, during the COVID-19 business closure mandates, and during the 2020 California wildfires, by gender and race or ethnic group, for California counties, 2018-2021 a
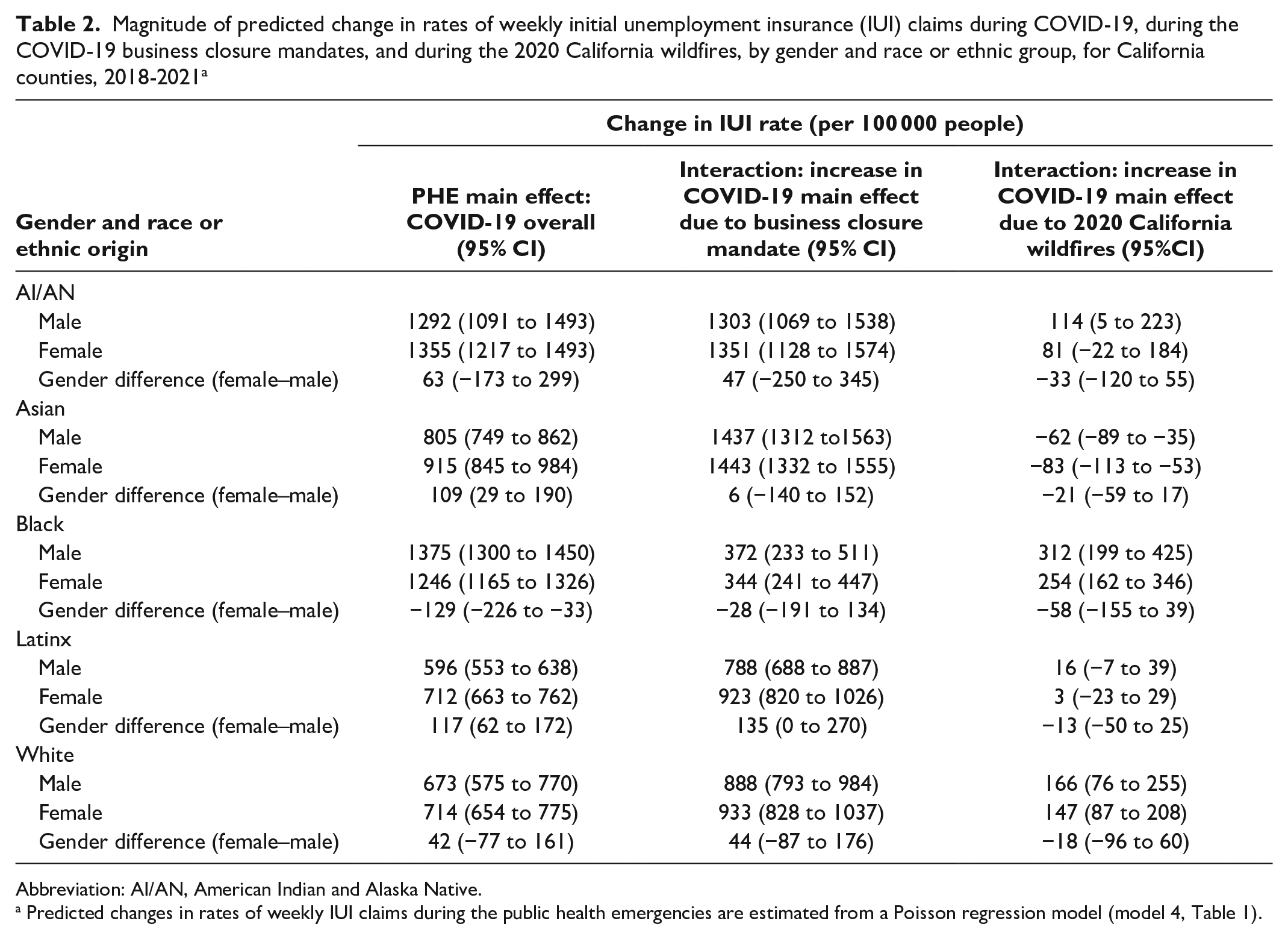
Abbreviation: AI/AN, American Indian and Alaska Native.
Predicted changes in rates of weekly IUI claims during the public health emergencies are estimated from a Poisson regression model (model 4, Table 1).
The change in weekly IUI rates for COVID-19 months also showed significant gender differences that varied by race or ethnic group, with the largest gender differences for Asian and Latinx men and women (Table 2). For the COVID-19 months, Asian women had 109 (95% CI, 29-190) more claims than Asian men did, and Latinx women had 117 (95% CI, 62-172) more claims than Latinx men did. However, no significant gender differences were shown for AI/AN or White men and women. The direction of the gender difference was reversed for Black men and women (Table 2), with a smaller COVID-19 increase for women than for men by 129 (95% CI, 33-226) fewer claims.
Peak in the Effect of COVID-19 Due to the Business Closure Mandate
The increase in the effect of COVID-19 during the business closure mandate period (compared with the same months in the following COVID-19 year) varied by race or ethnic group and gender (Table 2). For AI/AN and Asian men and women, the increase was the largest, ranging from 1303 (95% CI, 1069-1538) more claims during the closures than after the closures for AI/AN men to 1437 (95% CI, 1332-1555) more claims during the closures than after the closures for Asian men. For Latinx and White men and women, the increase was significantly smaller, ranging from an increase of 788 (95% CI, 688-887) more claims during the closures than after the closures for Latinx men to an increase of 933 (95% CI, 820-1026) more claims during the closures than after the closures for White women. For Black men and women, the increase was the smallest (for women, 344 [95% CI, 241-447] more claims; for men, 372 [95% CI, 233-511] more claims). Gender differences in the increased COVID-19 effect during the business closure was significant only for Latinx women compared with Latinx men, with 135 (95% CI, 0-270) more claims for women than for men.
Increase in the Effect of COVID-19 Due to the 2020 California Wildfires
The increase in the COVID-19 effect due to the 2020 California wildfires (compared with the same months in the following COVID-19 year) varied by race or ethnic group and gender (Table 2): compared with after the wildfires, 114 (95% CI, 5-223) more claims were made during the wildfires for AI/AN, 147 (95% CI, 87-208) more claims were made during the wildfires for White women, 166 (95% CI, 76-255) more claims were made during the wildfires for White men, 254 (95% CI, 162-346) more claims were made during the wildfires for Black women, and 312 (95% CI, 199-425) more claims were made during the wildfires for Black men. We found no significant differences between men and women in the compounding effects of the 2020 California wildfires for any race or ethnic group.
Discussion
We observed that IUI claims were a timely and granular way to track the effects of PHEs at the intersection of individuals’ race or ethnic group and their gender. Specifically, we found that the COVID-19 pandemic and the subsequent 2020 California wildfires were associated with greater increases in rates of weekly IUI claims among men and women from racial or ethnic minority groups (vs non-Hispanic White men and women) and among women (vs men). The changes in employment trends that we observed with these 2 PHEs suggest that examinations of short- and long-term effects of PHEs on the social determinants of health may be valuable. Future studies should continue to track these types of shifts over time to document whether the rapidly changing societal conditions stemming from PHEs and other major events cause lasting disruptions to social determinants of health, such as employment, and whether these disruptions reduce or exacerbate inequities in social determinants, particularly as the economy rebounds and as people reenter the workforce. 20
Our analyses identified gender differences in the increases of weekly IUI claims due to COVID-19 that varied markedly by race or ethnic group and that were compounded by the business closure mandate and the 2020 California wildfires, again in different ways for men and women from various race or ethnic groups. This finding suggests that these types of PHEs affect employment status, a key social determinant of health, through various mechanisms. For example, we speculate that the increase in IUI claims due to COVID-19 were likely associated with mitigation measures implemented to ensure physical distancing (business closures and stay-at-home orders), whereas the wildfires damaged important industries in California (wineries and agriculture).
Limitations
Our study had several limitations. First, changes in IUI claim rates are a proxy indicator of unemployment rates and may be imperfect. Data representativeness and validity of IUI claims may be limited because (1) not all workers are eligible for unemployment insurance benefits and (2) not all eligible workers apply for unemployment insurance benefits. Second, changes in the sociodemographic distribution of unemployment insurance claims data following a PHE are likely a combination of differential effects of the disaster on certain sociodemographic groups and changes in claiming behavior. For example, IUI claims could have increased because people may have received more support during the pandemic than they had before the pandemic to complete the unemployment insurance application (eg, at shelters). COVID-19 may have increased the general knowledge among people about the availability of unemployment insurance assistance and the application process, such that unemployment insurance claims data may be more representative of unemployed adults now than before COVID-19. In addition, before COVID-19, unemployment insurance claimants were more likely to be White, male, and union members compared with all unemployed individuals. 21 However, our findings show that, since COVID-19, more women have started to apply for IUI benefits. Finally, although this study cannot establish a causal relationship between these PHEs and shifts in IUI claims, we were able to leverage quasi-experimental difference-in-difference methods to improve our inferences.
Conclusion
This analysis underscores the importance of using timely, geographically granular data sources that allow for stratification at the intersection of gender and race or ethnic group to monitor the effects of PHEs over time on key social determinants of health, such as employment. The need for actionable data to document progress toward health equity, including those related to economic opportunity and other social determinants of health, was outlined in the original vision of Public Health 3.0 1 and a subsequent call to action. 22 Because unemployment has roots in historical (and current) systemic racism and has well-known links to downstream effects on physical and behavioral health,23,24 public health officials should consider using unemployment insurance claims for surveillance of social determinants. Future work could aim to elucidate the mechanisms through which unemployment affects physical and behavioral health and forecast the potential health effects associated with PHEs so that appropriate public health and policy mitigation strategies could be implemented to prevent downstream effects. 25
Social determinants of health are often deeply entrenched and challenging to modify, yet addressing them is fundamental to promoting health equity. Our study showed that major events such as PHEs can disrupt historical patterns in employment status. Timely monitoring of upstream social determinants of health is a first step toward operationalizing Public Health 3.0 and toward beginning to understand and address the complex drivers of long-standing health inequities in the United States.
Footnotes
Acknowledgements
The authors thank RAND colleagues Kathryn Edwards, PhD and Rajeev Ramchand, PhD, for providing subject matter expertise in the conceptualization of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The reported research was funded by the Centers for Disease Control and Prevention (CDC), an agency of the US Department of Health and Human Services, under CDC contract no. 75D30119C06926.