
Abstract
Objectives:
A need persists for graduates with public health training in government public health roles; however, earnings for these positions tend to be lower when compared with earnings for people with undergraduate or graduate training who are working in other sectors, such as private health care or pharmaceuticals. This study assessed federal student loan debt associated with education for public health, with an aim to quantify the need that may be met through the federal Public Health Workforce Loan Repayment Program (PHWLRP), which is one tool that policy makers have proposed to incentivize people with public health training to pursue employment in government public health.
Methods:
We analyzed federal student loan data provided by the National Center for Education Statistics College Scorecard for the 2018-2019 academic year. We merged these data with the Integrated Postsecondary Education Data System to estimate the number of degrees awarded. We used Spearman rank correlation to compare associations between debt and annual earnings by award level (bachelor’s, master’s, and doctoral degrees).
Results:
Across all award levels, the median level of federal student loan debt associated with education for public health was $33 366. The median annual earnings 1 year after graduation were $80 687 for graduates with doctoral degrees and $33 279 for graduates with bachelor’s degrees.
Conclusions:
As policy makers attempt to strengthen the public health workforce with a focus on funding and implementing the PHWLRP, the existing levels of student debt should be considered to ensure that programs such as the PHWLRP are funded and reflect the needs of graduates and government public health employers.
The US government public health workforce has seen its responsibilities grow in recent years and has seen additional stressors, with the most substantive in recent memory being COVID-19. 1 The public health workforce has long been inadequately staffed to meet the challenges of its day; 2 decades ago, the Institute of Medicine offered solutions to strengthen the capacity of government public health, but the solutions have mostly gone unfunded federally. 2 Inadequate staff numbers and underprepared workers underscore the chronic underinvestment in public health3-5 and the lack of people with public health training who pursue careers in government public health (eg, local, state, tribal, federal public health agencies). In 2021, only about 10% of recent public health graduates were working in local, state, or tribal public health. 5 This low rate raises questions about public health education and the incentives, or lack thereof, to work in government public health.
Accredited public health degree programs exist at the baccalaureate, master, and doctoral levels; nonaccredited certificates and associate’s degrees in public health are also available. The genesis of public health education dates back to 1915, when the Welch–Rose report outlined that public health should target infectious diseases with a population focus and be university based, research intensive, and taught separately from medical schools. 6 Although accreditation organizations have made efforts to elevate education opportunities in public health and to instill core competencies to prepare graduates who are entering the public health workforce, accreditation criteria have not historically been focused on the rising costs associated with education. As the prices of tuition, fees, and living expenses associated with higher education have increased in the past 2 decades, so too has the amount of federal aid that students pursue to finance their education. 7 In 2022, total federal student loans for students who are pursuing higher education were >$1.6 trillion. 8
In 1965, the Higher Education Act created opportunities for more types of students to receive federal financial aid, beyond veterans benefiting from the GI Bill. 9 As a result, students continue to access federal grants (which do not need to be repaid) and loans to finance their education. 10 In addition to federal loans issued by the US government, students may receive loans from private lenders. Through the Health Care and Education Reconciliation Act of 2010, the US government stopped issuing subsidies to private banks for student loans, and student borrowers now receive federal aid through direct loans from the federal government. 11
In the 1990s, Congress established an income-contingent repayment plan as a resource for student borrowers to repay loans issued directly by the government in a method commensurate with their income. 12 After limited uptake of the income-contingent repayment plan, Congress created the income-based repayment plan through the College Cost Reduction and Access Act of 2007 to offer all borrowers, not only people with direct government loans, to make payments relative to their income. 13 The College Cost Reduction and Access Act included the Public Service Loan Forgiveness Program (PSLF). Through PSLF, graduates work full-time in the government or at a nonprofit agency, make 120 qualifying monthly payments on their student loans through an income-based repayment plan, and have the remaining balance of their Federal Direct student loans forgiven. 14 We present information about these and other federal student loan repayment programs (Figure).15-17 Other programs, such as the National Health Service Corps, have been established to address workforce challenges and to drive students toward specific health professions and work in hard-to-staff locations. The National Health Service Corps program increased staffing and the availability of medical and behavioral health services, with no increased costs of these services. 18
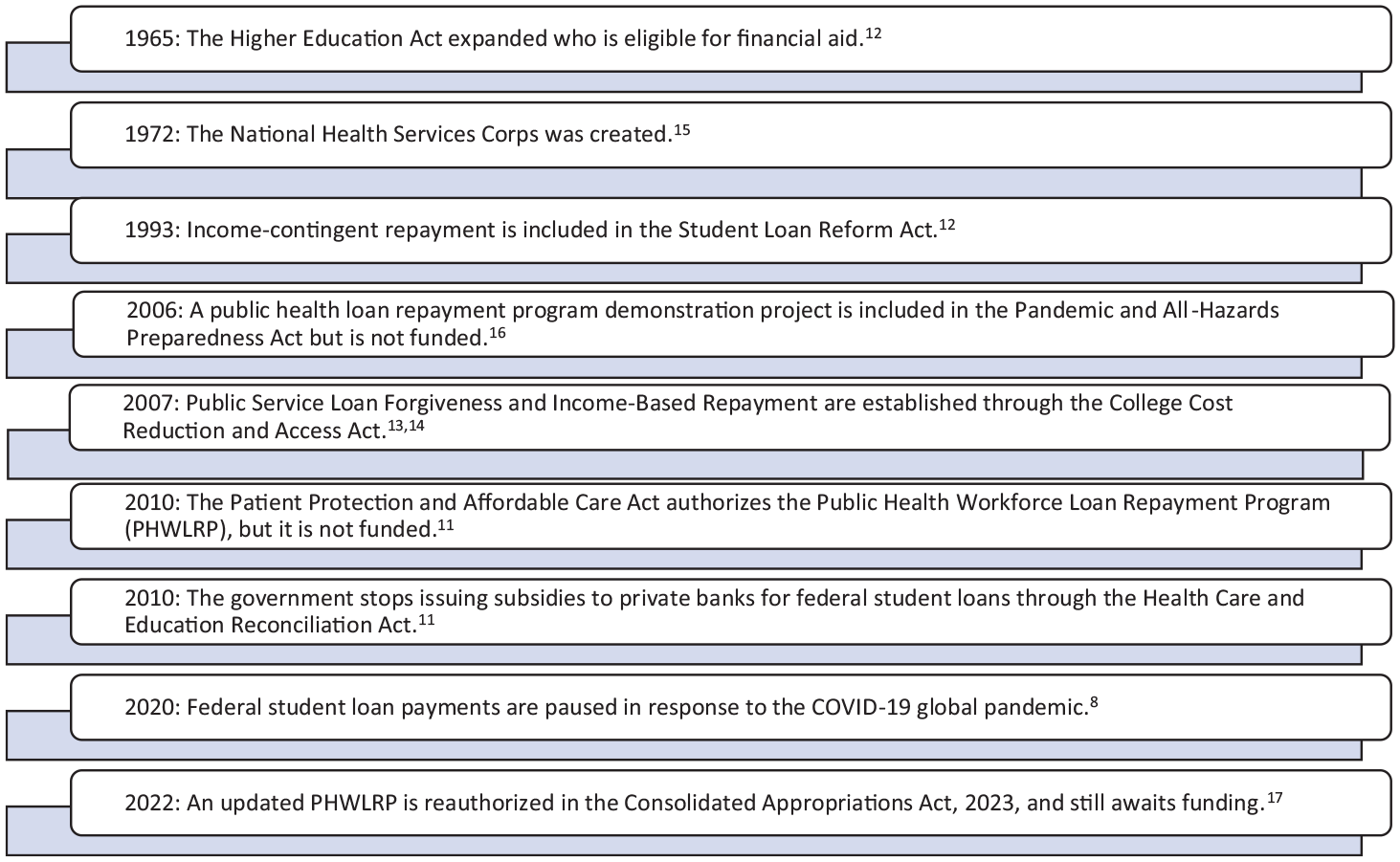
Timeline of federal student loan repayment policy activity, United States, 1965-2022.
The loan and career choices of a borrower are affected by the type of student loan repayment program available. 19 A loan repayment plan specific to people with public health education and with repayment options proportionate to loan burden may motivate more graduates to pursue different public health careers, including those in government. Although workers in public health also have opportunities for loan repayment through the federal PSLF, 14 federal policies have not addressed the unique workforce needs of government public health. These needs include recruiting a workforce that is diverse and equipped to work with and in communities to deliver services that advance health and racial equity. 20
Specific approaches are needed for the multiple workforce challenges in government public health departments. Challenges include the funding of new positions, the recruitment of qualified applicants for openings, and the long-term retention of workers. Policy makers have tried to address these issues in previous legislation. For example, a pilot program was created in the 2006 Pandemic and All-Hazards Preparedness Act to allow National Health Service Corp participants to work in some local, state, and tribal public health departments, 16 and a Public Health Workforce Loan Repayment Program (PHWLRP) was authorized for 5 years in the 2010 Affordable Care Act but never funded (and so was never, practically, implemented). 11 During the 117th Congress, updated legislation to authorize such a program was included in the PREVENT Pandemics bill that became law as part of the 2023 appropriations bill. 17 This legislation reauthorized and updated the 2010 program to broaden the eligible professions and to include local, state, and tribal public health departments; the legislation also included an evaluation component to better support the goal of recruiting and retaining workers in public health departments. Although funding for the program has not yet been determined, if funded, this program could aid in recruiting new graduates to public health jobs. This initiative includes $3 billion in federal funding aimed at supporting the government public health workforce. 21 If funded, the PHWLRP would support graduates with public health certificates or degrees who work for 3 consecutive years in government public health at local, state, or tribal public health departments, with loan repayment of up to $50 000 a year and not to exceed $150 000. 17
The objective of this study was to estimate the financial costs and federal student loan debts associated with education for public health. Understanding these estimates can inform whether proposed loan repayment programs, including the recently authorized PHWLRP, have adequate funding, whether loan repayment programs provide incentives for students to work in public health, and whether further advocacy efforts related to loan repayment for workers in government public health agencies are needed.
Methods
Data
We used 3 data sources to create a final dataset to estimate the financial burden and distribution of student debt associated with education for public health and the cost of public health program attendance in the United States. In using the term education for public health, we refer to undergraduate and graduate degree programs in public health. We used data from the National Center for Education Statistics (NCES), which provides the number and type of degrees conferred at US-based institutions through the Integrated Postsecondary Education Data System (IPEDS). We used IPEDS—which comprises data from every college, university, and technical and vocational college that awards federal student financial aid in the United States 22 —to determine the number of public health degrees conferred. Within IPEDS, we limited our analyses to bachelor’s, master’s, and doctoral degrees with a 4-digit Classification of Instructional Program (CIP) code specific to public health (51.22). Of note, this CIP code does not include degrees in epidemiology, biostatistics, or health policy analysis; these degrees are captured in other 4-digit CIP codes and mostly include non–public health degrees. We also excluded professional degrees that were not relevant to our analysis, such as doctor of medicine, doctor of veterinary medicine, doctor of osteopathic medicine, and postbaccalaureate certificates.
We merged IPEDS data with available estimates of federal student loan debt and graduate earnings provided by the US Department of Education through the College Scorecard. The College Scorecard provides publicly available data on debt and earnings associated with institutions and specific fields of study. 23 Specifically, our estimate of degree-associated debt comprises a measure of the median Stafford and Grad PLUS loans distributed at an institution. The measure is a pooled estimate of 2 years of debt from academic years 2017-2018 and 2018-2019; it reflects federal student debt for a single degree and is not cumulative, does not reflect Parent PLUS or federal loans taken out by parents for their dependent children, 24 and does not incorporate private or personal loans that might have been used to finance education for public health. These data represent the most recent year with available data on debt and first-destination earnings in the College Scorecard dataset. Of note, our analytic sample captured total conferrals and institutions with data on student loan debt and earnings, although NCES censors data on degrees due to small cell size and these observations are excluded from the analysis. Earnings data reflect the median annual earnings 1 year after graduation from a bachelor, master, or doctoral program and among those not currently enrolled in a degree program. Some observations included a value for median debt but did not include earnings, which resulted in fewer observations for earnings (n = 335) than for debt (n = 388).
To estimate the price of earning a master’s degree—an area of education for public health that experienced considerable growth between 2000 and 2020 (the number of degrees conferred increased 253% from 5098 to 18 044) 25 —we obtained information from the Association of Schools and Programs of Public Health (ASPPH) on the net cost of a master of public health (MPH) degree.
ASPPH collects data on the base tuition, differential and/or professional tuition or fees, mandatory fees, required health insurance, and other academic costs associated with earning an MPH degree at an institution. Professional tuition and fees include costs used to cover additional resources, facilities, or program enhancements. Data from ASPPH do not reflect room and board costs and do not include any scholarships or other tuition offsets. The ASPPH data comprised self-reported data from ASPPH members about their most common MPH degree. In total, ASPPH collected these data from 102 schools and programs of public health accredited by the Council on Education for Public Health in the United States and abroad, although we used only domestic data for our study. 26 We report tuition and fees associated with the most common MPH degree at an institution, overall and stratified by public and private schools and programs, and from academic years 2021-2022 and 2022-2023. These data do not include tuition and fees associated with all degrees in our analytic sample; they reflect data from ASPPH members.
This work did not involve human subjects; therefore, per the guidelines of the University of Minnesota Institutional Review Board, formal review was not necessary.
Statistical Analysis
We used Stata version 17 (StataCorp LLC) to integrate and analyze data. We used Spearman rank correlation to compare associations between debt and annual earnings by award level. 27
Results
In academic year 2018-2019, 16 962 bachelor’s degrees were awarded from 579 institutions, 15 600 master’s degrees from 580 institutions, and 975 doctoral degrees from 193 institutions (Table 1).
Number of public health degrees conferred, by award level, United States, 2019 a
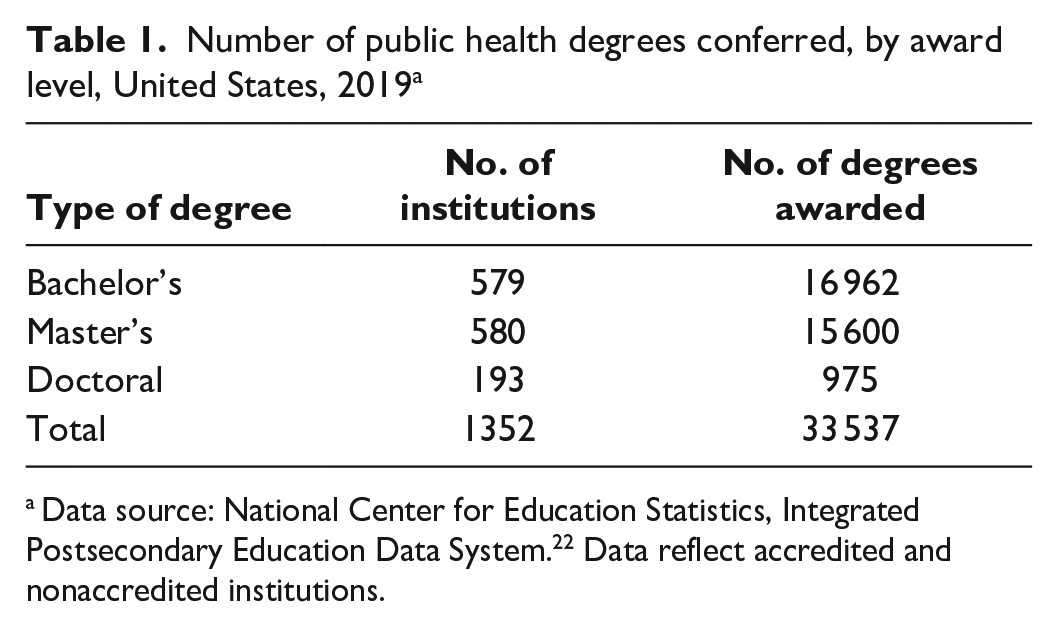
Data source: National Center for Education Statistics, Integrated Postsecondary Education Data System. 22 Data reflect accredited and nonaccredited institutions.
Across all award levels, the average of the median level of federal student loan debt from Stafford and Grad PLUS loans among institutions was $33 366, as pooled from 2 years of debt (academic years 2017-2018 and 2018-2019) (Table 2). Median debt associated with master’s degree–level training ranged from $8185 to $100 000. People with doctoral and bachelor’s degrees had median annual earnings of $80 687 and $33 279, respectively. We observed a positive association between increased federal student loan debt and earnings (Spearman rank correlation, ρ = 0.579).
Student debt at the institution conferring the academic degree and annual earnings 1 year after completion of academic degree, by type of degree, United States, pooled estimates from academic years 2017-2018 and 2018-2019 a
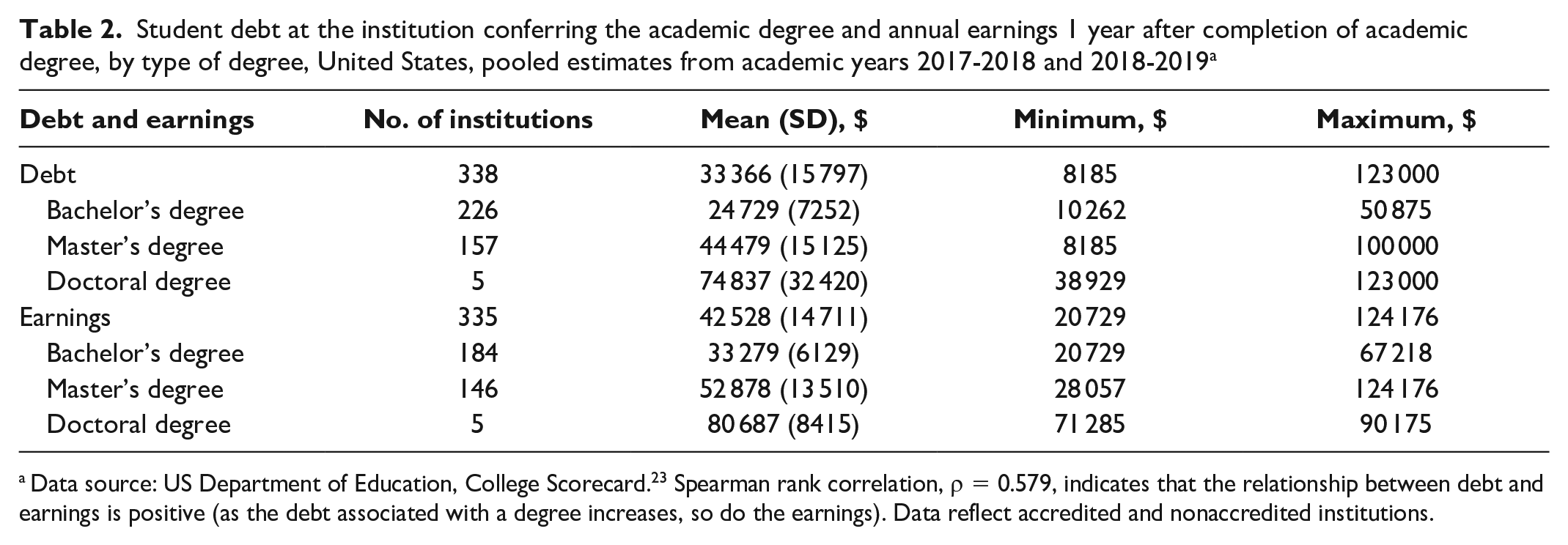
Data source: US Department of Education, College Scorecard. 23 Spearman rank correlation, ρ = 0.579, indicates that the relationship between debt and earnings is positive (as the debt associated with a degree increases, so do the earnings). Data reflect accredited and nonaccredited institutions.
Tuition costs and fees associated with earning an MPH degree were higher among private schools and programs than among public schools and programs, with wide variation in costs and fees across public and private schools and programs of public health and student residency (Table 3). Total tuition and fees were $71 645 for private schools and programs, $58 878 for out-of-state students attending public schools and programs, and $32 228 for in-state residents attending public schools and programs.
Tuition and fees associated with earning a master of public health degree, by type of school or program, United States, pooled results from academic years 2021-2022 and 2022-2023 a
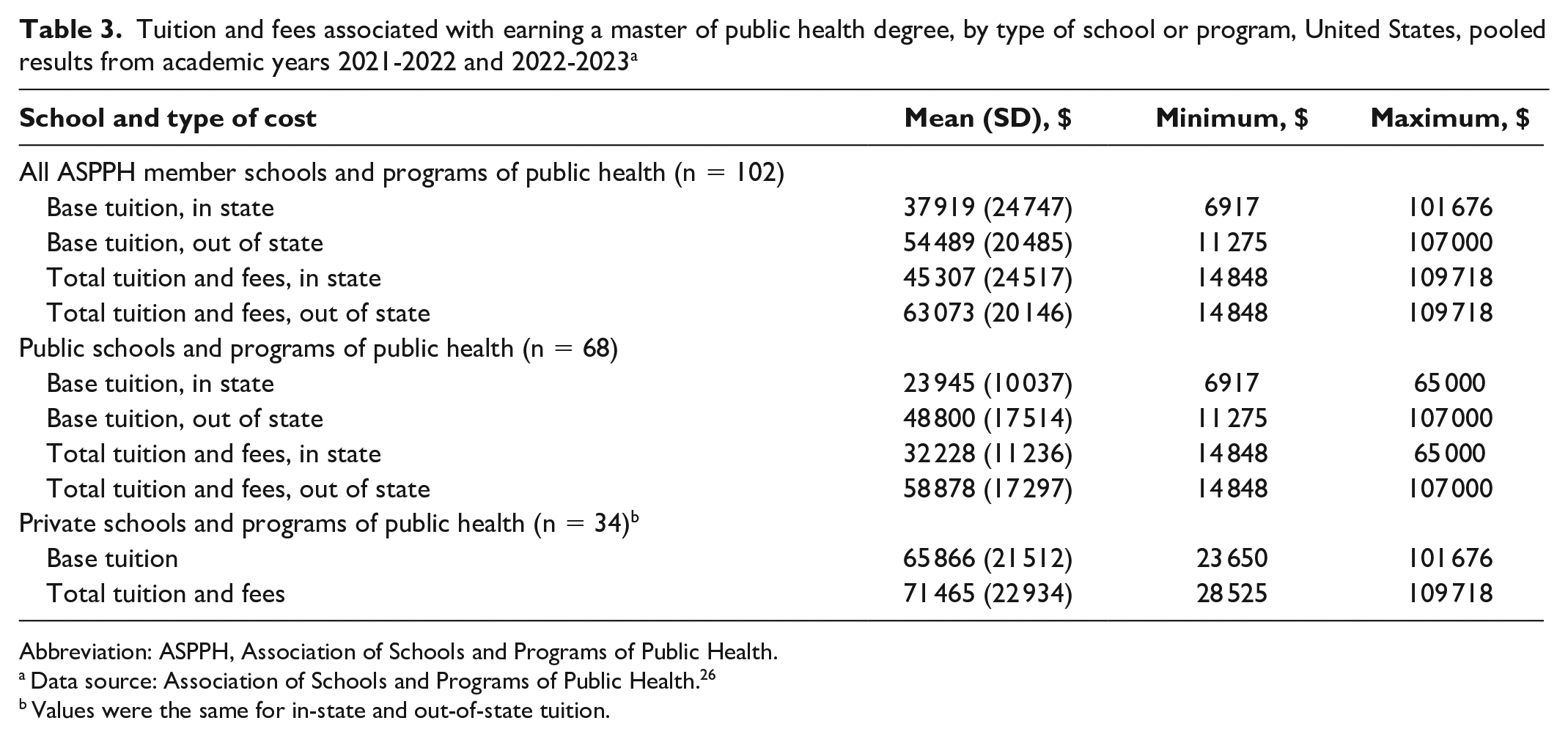
Abbreviation: ASPPH, Association of Schools and Programs of Public Health.
Data source: Association of Schools and Programs of Public Health. 26
Values were the same for in-state and out-of-state tuition.
Discussion
Student loan repayment and forgiveness programs are time-tested recruitment and retention strategies for private and public sector workers. 15 Financial challenges in recruiting new workers to the government public health workforce include student loan debt and modest earnings in the early career relative to other sectors, such as private health care or pharmaceuticals, which have a much higher annualized earning potential for comparable jobs and experience and can hire more expeditiously than the government.28,29 The earnings differential and resulting difficulties lead to challenges for government public health practices, where the need for a skilled public health workforce has increased because of ongoing demands associated with COVID-19. 30
Student debt, tuition, and fees for degrees in public health vary but are uniformly expensive relative to the expected earnings in government public health. In 2021, among staff with <5 years of experience in public health practice, which is about 36% of the workforce, graduates with a bachelor’s degree earned $55 000, with a master’s degree earned $65 000, and with a medical or doctoral degree earned $95 000, on average. 31 Our estimates of student loan debt based on NCES data were conservative, included only federal student loans per degree (not cumulative per person), and did not include debt for all public health degrees; thus, actual debt loads are likely higher than the estimates in our study.
Structuring Loan Repayment as a Recruitment Tool
If a loan repayment program for public health students becomes sufficiently funded, many graduates will benefit. With nearly 3000 eligible local, state, and tribal public health departments and with ≥80 000 workers still needed in the public health workforce to provide the most basic level of services, 32 many public health graduates, public health departments, and, in turn, communities could benefit from a loan repayment program. However, the benefits of a loan repayment program will not be realized if public health departments, where existing staffing needs prevail, are not adequately and permanently funded to support increasing needs.
Although programs to alleviate student loan debt may be an effective mechanism for incentivizing careers in government public health, they do not offer a complete solution. Schools and programs of public health and government public health agencies must consider how to better align training and opportunities so that graduates are exposed to and excited by a career in government public health. Departments must address other barriers to hiring and staff development and retention, including cumbersome and lengthy hiring processes and limited professional development, training, and career advancement opportunities. Not least in importance, any effort to alleviate student loan debt should be informed by existing efforts (namely, the PSLF) so that issues that have prevented participants from having their loans forgiven are not repeated.
Limitations
Our study had some limitations. First, some public health degrees may have been incorrectly classified in IPEDS, and data-cleaning procedures may not have removed all such degrees. As such, some degrees in our sample might not have been public health–related, which limited our ability to make general statements about education for public health. Second, available data on student debt from the College Scorecard do not reflect all degree-associated debt. Thus, we were limited in our reporting of the level of debt associated with all education for public health that individuals may have. Third, information from institutions with only a small number of graduates was withheld to maintain student confidentiality, which limited our ability to assess the burden of debt and earnings associated with all education for public health. However, we offer an estimate of how many observations were censored (eSupplement).
Fourth, we did not report degree-associated debt from all types of federal student loans (only Stafford and Grad PLUS student loans). In addition, data on degree-associated debt did not capture (1) data on federal student loan debt for students who began a degree at one institution but completed it elsewhere and (2) data on compounded student loan debt from multiple degrees; our analysis relied on a measure of the debt reported by the institution associated with where a degree was completed. Fifth, certain common majors offered by schools and programs of public health are classified as outside of public health by NCES (eg, epidemiology, CIP 26.1309; biostatistics, CIP 26.1102) and, thus, were not included in the 4-digit public health data. If we had included the 4-digit CIP codes for epidemiology, biostatistics, or health policy analysis, our sample would have reflected too many non–public health degrees (eg, ecology or biology, which are reported with epidemiology). Some people with these degrees may pursue government public health and may receive high salaries given their training, and this analysis underreported debt and earnings without these degrees.
Sixth, public health degree data were combined across an award level, including somewhat different degree programs, most notably the MPH and master of hospital administration and doctor of philosophy degrees across various subfields. Combining data limited our ability to provide degree program–specific estimates of debt and earnings, such as the amount of debt among those obtaining a master of hospital administration as compared with an MPH. Seventh, information from ASPPH did not reflect the costs of all master’s degree–level public health training, because information did not include scholarships or other financial aid that institutions offer and may not be what students ultimately pay. Lastly, our data did not reflect recent inflation or salary increases resulting from the COVID-19 pandemic; therefore, current debt and earnings may be higher than our results.
Conclusions
As policy makers attempt to strengthen the public health workforce with a focus on funding and implementing the PHWLRP, the existing levels of student debt should be considered to ensure that programs such as the PHWLRP are funded and reflect the needs of graduates and government public health employers. Legislation should consider the debt estimates provided in this study to determine whether the repayment amounts are enough of an incentive to recruit and retain public health graduates to government public health departments. Given the student loan debt burden, a functioning public health workforce loan repayment program would offer an important incentive to relieve student loan debt and add value to the salary and benefits offered to prospective public health workers.
Supplemental Material
sj-docx-1-phr-10.1177_00333549231223712 – Supplemental material for Federal Student Loan Debt in Public Health and the Opportunities for Loan Repayment Programs
Supplemental material, sj-docx-1-phr-10.1177_00333549231223712 for Federal Student Loan Debt in Public Health and the Opportunities for Loan Repayment Programs by Margaret Tait, Emily Burke, Tim Leshan, Adriane Casalotti, Heather Krasna and Jonathon P. Leider in Public Health Reports
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The National Association of County and City Health Officials, the Association of Schools and Programs of Public Health, and Columbia as organizations have advocated for public health student loan repayment programs. Heather Krasna, PhD, MS, EdM, discloses that she is engaged around student loan repayment advocacy work as an independent organizer.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online. The authors have provided this supplemental material to give readers additional information about their work. The material has not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.