
Abstract
In the United States, persistent health disparities and preexisting gaps in local public health infrastructure led to disproportionate effects of COVID-19 across populations at high risk of COVID-19–related morbidity and mortality. In Pima County, Arizona, equity-centered local government engagement and policy action, multipronged community-based responses, and expansion of historically underfunded local public health infrastructure improved equitable outcomes and addressed multiple systemic factors. This case study examined Pima County’s 3-pronged public health response to COVID-19 using an equity-based approach. As a result, COVID-19 was the third leading cause of death in Pima County in 2021, compared with being the leading cause of death in Arizona. Strong political support from local elected officials created the authorizing environment for the Pima County Health Department to advance health equity. Passage of a resolution in December 2020, which framed the racial and ethnic health and socioeconomic inequities as a public health crisis, supported innovation and fostered the creation of an Office of Health Equity, a public health policy program, and a data and informatics program. New structures for community engagement were formed, including an ethics committee and a community advisory committee, to ensure a formalized process for community participation in public health actions, during and after the pandemic response. Key lessons learned included (1) the importance of local government support, codified to allow implementation of creative strategies; (2) opening avenues for community voice and engagement in planning and implementation to respond in areas of greatest need; and (3) having flexible funding to sustain an equitable response.
Pima County is the second largest county in Arizona, with more than 1 million residents residing in rural and urban areas. 1 The county is predominantly non-Hispanic/Latino White (51.2%), followed by Hispanic/Latino (37.8%), American Indian and Alaska Native (4.4%), and non-Hispanic/Latino Black/African American (4.2%). 2 It borders Mexico and shares jurisdiction with 2 sovereign Tribal Nations with an urban Tribal population. Pima County’s poverty rate is higher than the state average (14.9% vs 12.8%). 2 The Pima County Health Department (PCHD) is the public health authority for all nonTribal government entities in the county, via a decentralized public health system. County rather than state employees perform key functions. Tribal Nations led their own COVID-19 pandemic response efforts. PCHD worked collaboratively with Tribal Nations on emergency management and public health response efforts.
Social Vulnerability Index (SVI) scores and COVID-19 Community Vulnerability Index (CCVI) scores serve as proxy variables to the social determinants of health (SDH). 3 SVI scores use socioeconomic status, household composition, disability, racial and ethnic minority status, language, housing type, and transportation to predict community response to external stressors. 4 CCVI considers SVI and incorporates specific COVID-19 risk factors that help public health agencies better understand the full range of vulnerabilities in a given community. As with SVI, CCVI is a nationwide comparison that is scaled from 0 to 1, where 1 is most vulnerable and 0 is least vulnerable to COVID-19. 5 These variables guided the pandemic response in geographic areas disproportionately affected by COVID-19. Pima County has an overall SVI score of 0.91 6 and a CCVI score of 0.84; 41% of the population has high or very high vulnerability to COVID-19. 7 Early 2020 national COVID-19 data revealed age-related, socioeconomic, and racial and ethnic differences, highlighting existing health inequities. 8 Pima County data demonstrated that poverty, population density, race and ethnicity, occupation, and communal living settings increased the susceptibility to COVID-19 infection, severe illness, and death. 9 Years of disinvestment in federal, state, and local public health left local public health infrastructure ill-equipped to respond to the pandemic and underresourced to address SDH. In December 2020, the Pima County Board of Supervisors committed to advancing health equity by passing a resolution that declared racial and ethnic health inequities and income inequality a public health crisis. 10
In January 2021, Arizona became the COVID-19 “hot spot of the world, with the worst new infection rate of any state in the nation.” 11 Mortality from COVID-19 in the United States by the end of 2021 was 249 cases per 100 000 people and in Arizona was 332 cases per 100 000 people. The mortality rate was 167 per 100 000 people for the same period in Pima County (Table 1). Despite having a very high SVI/CCVI score, Pima County achieved vaccination rates above average for both completed series vaccination and boosters. As of January 7, 2022, Pima County’s vaccine uptake was 10 percentage points higher than in other large Arizona counties. The average for all census tracts with a high CCVI score was 87% of people aged ≥65 years having received ≥1 dose of the COVID-19 vaccine (unpublished data, PCHD, October 18, 2022). Seventy-two percent of adults aged ≥18 years in areas of high CCVI have received ≥1 dose of the COVID-19 vaccine (unpublished data, PCHD, October 18, 2022). In Pima County in 2021, American Indian/Alaska Native people had the highest rate of COVID-19 vaccination series completion (87 056 per 100 000 people), while non-Hispanic White residents had the highest COVID-19 vaccine booster rates (49 070 per 100 000 people) (Table 2).
COVID-19 mortality rates, vaccination, and booster percentages in the United States, Arizona, and Pima County, Arizona, January 1–December 31, 2021
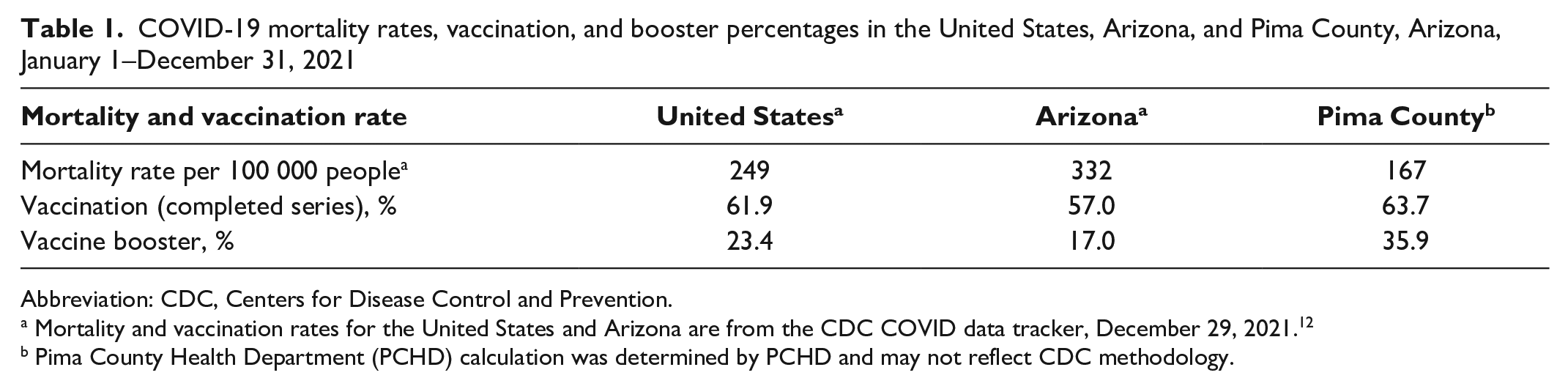
Abbreviation: CDC, Centers for Disease Control and Prevention.
Mortality and vaccination rates for the United States and Arizona are from the CDC COVID data tracker, December 29, 2021. 12
Pima County Health Department (PCHD) calculation was determined by PCHD and may not reflect CDC methodology.
COVID-19 vaccination and vaccine booster rates, by race and ethnicity, Pima County, Arizona 2021 a
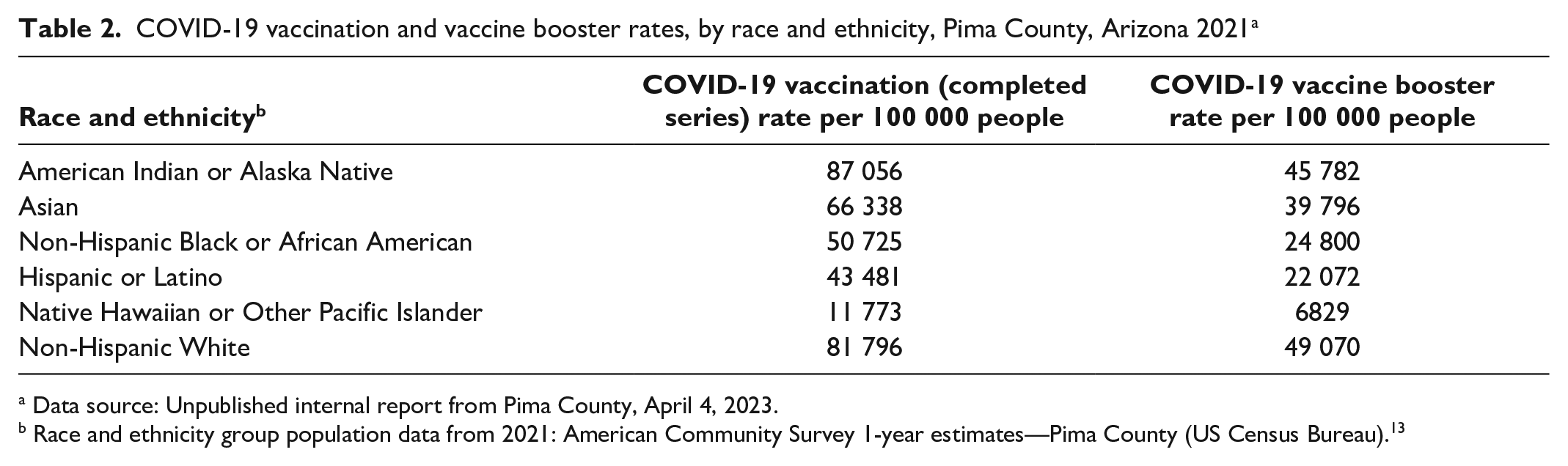
Data source: Unpublished internal report from Pima County, April 4, 2023.
Race and ethnicity group population data from 2021: American Community Survey 1-year estimates—Pima County (US Census Bureau). 13
During November 2021–September 2022, PCHD supported more than 400 mobile vaccine clinics throughout the community (unpublished data, PCHD, October 1, 2022). Grant-funded initiatives were foundational to increasing access to testing and vaccine resources and addressing barriers to health literacy. The MC3 program alone delivered testing services to 9869 people across 75 sites and 21 227 vaccines in historically underserved communities. As of October 2022, the vaccine equity program participated in 83 outreach events, engaged 4255 community members via in-person conversations about COVID-19 risks and resources related to vaccine information, and held 74 vaccination events that provided 1302 vaccines (267 first doses) (internal department communication with N. Jain, PCHD, October 1, 2022). Our health disparities grant, from October 2021 through September 2022, funded the distribution of 158 817 at-home COVID-19 tests through community partners such as public libraries (internal department communication with E. Diaz, PCHD, October 1, 2022).
Purpose
Given the county’s high SVI/CCVI scores, community-based approaches and data-driven decision-making were crucial to success. This case study explores how a local health department adopted multipronged, equity-centered policies and community-driven public health responses that expanded internal support structures, using precision data to drive place-based equity-focused strategies. These approaches remain useful for addressing systemic factors that contribute to SDH and improving health outcomes beyond the COVID-19 pandemic response. Health departments face new realities and requirements in the 21st century. Other localities can replicate the Pima County model to inform their own future equity-focused public health responses with the incorporation of 3 key components: government engagement, internal policies/processes, and community voice/engagement.
Methods
Pima County’s health equity–focused COVID-19 response emphasized 3 areas: (1) government engagement (ie, the systemic interventions undertaken by government structures), (2) internal policies and processes, and (3) community voice and engagement (ie, how those most affected by COVID-19 informed the county’s pandemic response) (Table 3). PCHD staff internally calculated data and used local, state, and nationally available datasets for the content presented in outcomes. PCHD conducted its own calculations for mortality at the county level because it did not have access to methods used by the Centers for Disease Control and Prevention (CDC) for its COVID-19 mortality calculations. Public health actions referenced in this article did not meet the requirements for review by an institutional review board; however, they were shared with the PCHD Ethics Committee to ensure they aligned with ethical public health practice.
Methods implemented by the Pima County Health Department during the COVID-19 pandemic response, Pima County, Arizona, 2021-2022
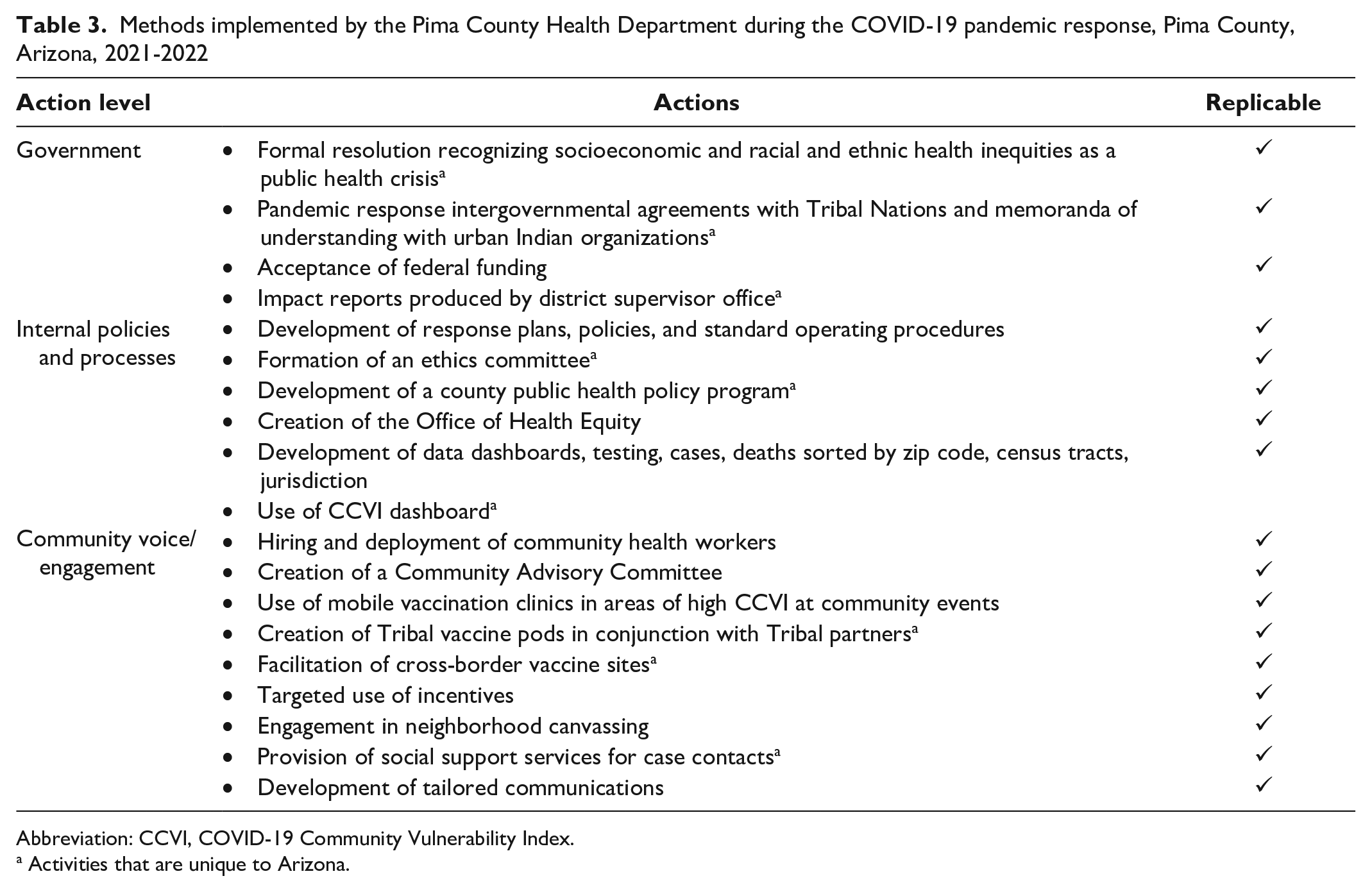
Abbreviation: CCVI, COVID-19 Community Vulnerability Index.
Activities that are unique to Arizona.
Government Engagement
Pima County Board of Supervisors
PCHD benefited from having strong local political support for an equitable pandemic response. On May 27, 2020, Pima County administration released a memorandum identifying concerns the Pima County Board of Supervisors had regarding COVID-19’s disproportionate impact on vulnerable populations, as defined by SVI. 14 Starting June 26, 2020, PCHD provided weekly COVID-19 case and hospitalization data, by race and ethnicity, to the Board of Supervisors and the public. 15 These data showed that during June 26, 2020–December 9, 2022, medically and socially vulnerable racial and ethnic minority groups at elevated risk for severe COVID-19 impacts, including Hispanic and Native American populations, comprised disproportionately high case rates and hospitalizations in Pima County at different points in the first 2 years of the pandemic. 15 In December 2020, the Pima County Board of Supervisors issued resolution 2020-92, a formal acknowledgment of the emergency status of preexisting health inequities resulting from socioeconomic status, race, and ethnicity. 10 Pima County was the only Arizona county during the height of the pandemic to have declared racism a public health crisis and remains the only one to have done so. 16 This political support allowed the development of long-term, comprehensive, community-wide responses and strategies, including vaccination rollout plans, standard operating procedures (SOPs), workforce development, community engagement, and risk communication.
Tribal collaboration
Pima County strengthened its collaboration and emergency response planning with local Tribal Nations through updated intergovernmental agreements, expanded services, and coordinated responses. Shared response efforts fostered collaboration on public health emergency preparedness, response, and clinical service coordination. PCHD used a memorandum of understanding with an urban Indian center as a tool to support shared response efforts and collaborative outreach for off-reservation Tribal members disproportionately affected by severe COVID-19. Outreach included weekly mobile vaccination at and testing events at community-based organizations (CBOs) serving this population, community centers, schools, and neighborhoods, as well as social and cultural events, such as health fairs and the annual powwow. PCHD secured additional funding to support the distribution of gift cards at vaccination events in communities with low vaccine uptake and high SVI/CCVI. Weekly meetings between Tribal and county emergency response teams streamlined communication, coordination, and sharing of resources. The intergovernmental agreements and memoranda of understanding with Tribal partners created the authorizing environment for collaboration on and off Tribal land.
Federal
PCHD used American Rescue Plan Act and Coronavirus Aid, Relief, and Economic Security (CARES) Act funding to support the enhancement of existing infrastructure to better address COVID-19 disparities.17,18 In 2021, PCHD received 2 CDC grants that focused on advancing equitable COVID-19 responses: the National Initiative to Address COVID-19 Health Disparities and the COVID-19 Vaccination Equity Funding. Both grants addressed health disparities by expanding access to vaccination and testing. In 2022, PCHD partnered with the Center for Global Health Innovation on a Health Resources and Services Administration–funded Vaccine Access and Training project, enabling the deployment of an additional 8 community health workers (CHWs) in communities with high SVI/CCVI scores.
CHWs were central to implementation of an equitable response. Using federal epidemiology and laboratory capacity funds for the prevention and control of emerging infectious diseases early in the pandemic, PCHD established what would become a model program, “Mitigating COVID-19 in Communities of Color” (MC3), in partnership with CBOs. MC3 provided health information, testing, social support resources, and COVID-19 care coordination in underresourced communities. Addressing the SDH through government and policy actions enabled PCHD to implement an equity-focused COVID-19 response, but what actualized the policy intentions was increased federal funding, which created pathways for community engagement and partnership.
Internal Policies and Processes
Resolution 2020-92 mandated equity in the COVID-19 response and recovery efforts and input from underresourced communities. 10 PCHD built internal capacity to meet both objectives. The department publicly committed to ambitious testing and vaccination goals, including an initial target of administering 300 000 single doses in a 3-month period through March 31, 2021. 19 The intent of the equity-focused vaccine rollout plan was to create the necessary infrastructure and guidelines so that the only factor limiting vaccine administration was the lack of vaccine rather than the lack of personnel. Personal information collected by PCHD was limited to name, date of birth, and history of adverse events. Personal identification was not required.
Community engagement and communication plans reflected the needs of the identified community, data goals, logistics, and appropriate communication styles, format, and languages. SOPs iteratively produced throughout the pandemic included workplans and guidance such as enumeration, prioritization, and identification of populations at risk of contracting COVID-19. 8 Workplans and SOPs included but were not limited to immunization acceleration, phase 1 vaccination planning, outreach to underresourced populations and populations vulnerable to severe outcomes from COVID-19, high SVI/CCVI scores, adolescent vaccination, vaccination for homebound populations, rural outreach, and COVID-19 boosters.20-26
Creation of publicly available data tracking that aggregated COVID-19 cases by census tract enabled precision-targeted vaccine and testing sites and made data readily accessible. Geographic information systems–driven dashboards were developed that incorporated the SVI and American Community Survey information. 15 Creation of these dashboards facilitated development of the public-facing Pima County Vaccine Solutions Dashboard, a CCVI dashboard developed with Surgo Ventures. 27 Dynamic dashboards permitted users to modify views, rank census tracts based on multiple criteria, and evaluate the impact of interventions on a daily and weekly basis. These data informed local policy makers and guided placement of mobile clinics.
In November 2020, PCHD established an ethics committee to integrate ethical decision-making into public health actions and practice. Members of the ethics committee represented cross-sector and historically underrepresented groups, Tribal communities, CBOs, faith-based organizations, schools, social services, and 2 Pima County Board of Health representatives. The ethics committee advised the PCHD director on equity-focused approaches in pandemic response policies and plans. The committee provided guidance on a range of issues that included COVID-19 vaccination prioritization plans, which incorporated community needs and disparities, and fair and equitable vaccine rollout in populations vulnerable to severe COVID-19, such as those who were disabled, incarcerated, or in undervaccinated cross-border communities.
Community Voice and Engagement
Medically and socially vulnerable communities experienced a disproportionate impact from COVID-19 as a result of persistent structural inequities. PCHD addressed these vulnerabilities via community engagement approaches through CBOs, trusted leaders, networks and coalitions, deployment of CHWs, use of mobile clinics, and targeted use of incentives. Strategies involved giving away electric fans in areas where housing lacked cooling infrastructure, offering mobile vaccine clinics in remote villages, and creating sector-based initiatives with school districts and business communities to better reach people where they were via their trusted institutions. Using pandemic grant funding, PCHD provided regranting opportunities with grassroots CBOs to expand outreach to communities they serve. PCHD supported vaccination efforts for Tribal communities by offering mobile vaccination clinics, sharing communications, making public service announcements, developing health education materials, offering trainings, supplying personal protective equipment, and administering COVID-19 tests.
The community advisory committee was created as a formal community engagement structure. Established in April 2021, the committee comprised diverse partners such as neighborhood leaders, nonprofit employees, and current and former clinicians representing CBOs from multiple sectors, including, but not limited to, disability rights, senior-citizen services, and refugee resettlement. The committee guided community response efforts and enhanced collaboration in historically underserved communities.
PCHD collaborated with various community groups to codesign response strategies and activities and ensure access to social services, such as eviction and legal support, financial assistance, transportation resources, and behavioral health. Partners In Health, an international nonprofit public health organization, provided technical assistance to PCHD from the early stages of the pandemic on all areas of response. A partnership with Chicanos Por La Causa, a nonprofit social service and advocacy organization in Tucson, Arizona, serving Mexican American/Latino communities, connected people in communities at high risk of contracting COVID-19 with food, housing, and medical resources. PCHD and Partners In Health contracted with nonprofit organizations that traditionally canvassed for civic engagement to provide information on COVID-19 resources to neighborhoods with severe COVID-19 impacts. Beginning in December 2020, PCHD began working through the community advisory and ethics committees, community leaders, groups (faith-based organizations, businesses and employers, educational partners, labor unions, and neighborhood and home owner associations), and academic institutions to host COVID-19 vaccination and testing sites. One such partnership took a unique approach and hosted vaccination sites in collaboration with the US–Mexican consulate and Tribal Nations at the United States–Mexico border to reach citizens at risk of severe COVID-19 and Tribal members on both sides of the border.
Outcomes
At the beginning of the pandemic, PCHD lacked necessary funding streams and infrastructure. Much of the federal guidance on vaccine eligibility did not fully consider local realities. Many workplans and SOPs needed to be created and updated as new interventions and availability of supplies emerged. The response needed fluidity but enough support to ensure equity remained the focus. Consequently, PCHD used fiscal and human resources to identify community need in historically underserved populations, track delivery of comprehensive COVID-19 services, and guide the epidemiological response to the pandemic. Expanded actions included workforce expansion to support disease surveillance, data analytics, and community-based public health; strengthening of equity-centered infrastructure; and delivery of equitable services to the hardest-hit communities. With additional pandemic response funding, PCHD rebuilt its previously underresourced infrastructure into an equity-centered, well-equipped, 21st-century health department. A new internal infrastructure for equity in PCHD emerged from Resolution 2020-92 10 and enhanced funding through 2 federal rescue plans, which allowed the department’s continued emphasis on equity and data-led approaches throughout all programming.17,18 PCHD now has an internal policy program, an Office of Health Equity, and a data and informatics program. The Pima County Board of Supervisors, in its last 3 legislative agendas, prioritized protecting local public health authority.
As a result of our approaches, COVID-19 was only the third leading cause of death in 2021 for Pima County compared with Arizona, where it was the leading cause of death. The methods PCHD used were unique to Arizona at the time of initial implementation. Establishment of the ethics committee guided equity-focused and community-driven efforts based on public health ethical principles, which informed the development of locally tailored policies, workplans, and SOPs. Strong local political support for acceptance of federal funding and equity-centered approaches was uncommon across Arizona. PCHD was and still is the only health department in Arizona with both a policy program and Office of Health Equity.
Lessons Learned
Future initiatives will rely on foundational exemplars created for COVID-19, such as workplans, protocols, response SOPs, data infrastructure, and publicly shared dashboards. Establishment and maintenance of relationships with historically underserved groups is crucial to a shared public health response that addresses inequities. Strategies for future initiatives include additional objective datasets incorporated into our community resilience evaluation, human-centered design approaches that inform and evaluate interventions, and additional training for CHWs. Other jurisdictions could replicate PCHD’s government engagement, policy actions, SOPs, data modernization and democratization, and foundational community partnerships. PCHD has made its COVID-19 plans and SOPs available online for other health departments to view and use.20-26
During the summer 2022 mpox response, PCHD used SOPs and workplans developed during the COVID-19 pandemic to guide placement of vaccine sites (mobile and fixed) and creation of community-driven messaging. The community advisory committee and ethics committee kept equitable practices at the forefront to help address community concerns and design community messaging. Without this infrastructure, PCHD’s response rate to mpox would likely have been greatly diminished.
Pima County leadership demonstrated their commitment and understanding of the critical role government plays in support of public health. This support was essential to PCHD’s efforts to provide an equitable pandemic response. Pima County accepted all COVID-19 federal funds and received direct allocation of relief funds from the federal government. Sustained, stable, and flexible public health funding for local health departments is necessary to adequately address health inequities and respond to emerging public health threats. Support for public health infrastructure must include obtaining funding necessary for workforce expansion, maintaining equity, and improving community public health outcomes. Working across local health departments, communities, and political structures is critical.
Footnotes
Acknowledgements
The authors acknowledge Chicanos Por La Causa, Partners In Health, the Pima County Board of Supervisors, Pima County administration, the Pima County Health Department (PCHD), including the ethics committee and community advisory committee, Zach Gerbarg, MD, consultant to Pima County Health Department, and Surgo Ventures, for their support in executing this response model. The authors also acknowledge Amanda Sapp, MPH, and Emma Najibi, MPH, of PCHD for providing data analysis and visualization assistance.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The following awards received by PCHD were referenced in the document: MC3-COVID-19 Communities of Color Grant award amount $936 483 (6 NU50CK000511-01-08), National Initiative to Address COVID-19 Health Disparities award amount $6 510 503 (6 NH75OT000063-01-01), COVID-19 Vaccination Equity funding award amount $9 559 161 (6 NH23IP922599-02-04), and Vaccine Access and Training Grant award amount $89 900 (1 U3UHS45470-01-00). The contents of this article are those of the authors and do not necessarily represent the official views of, nor an endorsement by, CDC, the US Department of Health and Human Services, the Health Resources and Services Administration, or the US government. None of the funding awards formally sponsored the research or authorship of this article.