
Abstract
Objective:
Food safety progress depends on the ability of public health agencies to detect and investigate foodborne disease outbreaks. The Integrated Food Safety Centers of Excellence identify and implement best practices and serve as resources for public health professionals who investigate enteric disease outbreaks. To target the needs of this diverse workforce, the Integrated Food Safety Centers of Excellence developed and assessed a professional tier framework and competencies.
Methods:
We described the characteristics of public health professionals who investigate enteric disease outbreaks in the epidemiology role in a conceptual tiered framework. We mapped core competencies to each tier and disseminated a survey to practitioners at local (June 2019) and state (August 2018) US public health agencies to evaluate the importance and frequency of each competency.
Results:
We developed 15 competencies on surveillance, outbreak detection, interview skills, investigation team, specimen testing, data analysis, hypothesis generation, study design, communication, enteric disease biology, control measures, legal authority, quality improvement, environmental health, and reporting to surveillance. The 286 survey respondents selected interview skills, surveillance, control measures, and hypothesis generation as the competencies most important to their work and most frequently performed.
Conclusion:
The Integrated Food Safety Centers of Excellence created the first published workforce framework and competencies for public health professionals who detect and investigate enteric disease outbreaks in the epidemiology role, in collaboration with local, state, and federal public health agencies and national organizations. These tools have been integrated into existing programs and can be used to develop training curricula, assess workforce competency over time, and identify priorities for continuing education and training.
Foodborne illness is common in the United States, with an estimated 48 million illnesses each year, resulting in 3000 deaths.1,2 Ensuring the safety of the food supply is the primary responsibility of the US Food and Drug Administration, the US Department of Agriculture’s Food Safety Inspection Service, and the food industry. However, progress in food safety depends on foodborne disease surveillance and outbreak investigations that identify priority pathogens and link them with specific foods. The 2012 Food Safety Modernization Act called on the Centers for Disease Control and Prevention (CDC) to strengthen public health surveillance and response networks in partnership with state and local public health agencies, as part of the development of a modern system focused on prevention. 3 In response, CDC established Integrated Food Safety Centers of Excellence to identify and implement best practices and to serve as a resource for public health professionals at state and local public health departments. 4
Since their establishment in 2012, the Integrated Food Safety Centers of Excellence have expanded the number of trainings and continuing education opportunities for public health professionals who detect and investigate enteric disease outbreaks. On-the-job training and continuing education are critical to developing and maintaining an effective public health workforce because many public health professionals do not have formal public health training. 5 Moreover, the practice of foodborne disease surveillance and outbreak response is constantly evolving, and professionals need training on emerging approaches, such as whole genome sequencing and culture-independent diagnostic testing. 6
A complicating factor in providing training is the diversity of the workforce who detect and investigate enteric disease outbreaks. Specifically, roles and responsibilities differ depending on the state’s public health legal infrastructure, which may be centralized or decentralized, and the size of the population served. For example, public health nurses and communicable disease investigators working at small local public health departments may be responsible for a range of public health services and may investigate few outbreaks, whereas state and large local public health departments may employ epidemiologists specializing in enteric disease.
To better meet the needs of this diverse workforce, the Integrated Food Safety Centers of Excellence developed competencies detailing the core knowledge and skills needed for public health professionals to detect and investigate foodborne and enteric disease outbreaks. The primary goal of these competencies is to guide the development and evaluation of curricula for Integrated Food Safety Centers of Excellence training and resources; however, competencies can also be used by state and local public health departments to create workforce development plans and write job descriptions. The competencies for public health professionals engaged in environmental health are described elsewhere. 7 We describe the competencies for public health professionals in the epidemiology role and summarize the results of a survey of public health practitioners in epidemiology to assess the value of each competency.
Methods
Target Audience Framework
A working group of public health practitioners and academicians from the Integrated Food Safety Centers of Excellence created a conceptual framework to describe the diverse audience of public health professionals responsible for detecting and investigating foodborne and enteric disease outbreaks in the epidemiology role. The working group described characteristics of these public health professionals, including their background, training, and key roles and responsibilities, while also considering the type of public health agency (state, local) and the size of the population served. We then used the Dreyfus model of skill acquisition to create 3 tiers based on professional roles and responsibilities.8,9 The working group shared the framework with local, state, and federal public health practitioners and members of the Integrated Food Safety Centers of Excellence network for feedback and development of consensus that the framework reflected each tier.
We organized the 3 tiers in the conceptual framework to progress from low to high levels of skill complexity. Tier 1 included entry-level professionals or workers who were new to foodborne illness outbreak investigations and able to recognize and participate in outbreak investigations with guidance. Tier 2 included professionals who routinely detect, investigate, and respond to outbreaks and have the knowledge and skills required to conduct all aspects of the outbreak investigation. Tier 3 included professionals who were in senior, supervisory, or managerial roles and able to direct, innovate, and advance outbreak detection, response, and investigation. We considered that the level of skill required for professionals in each public health agency often increases as the frequency of outbreaks in the jurisdiction increases (Figure 1).
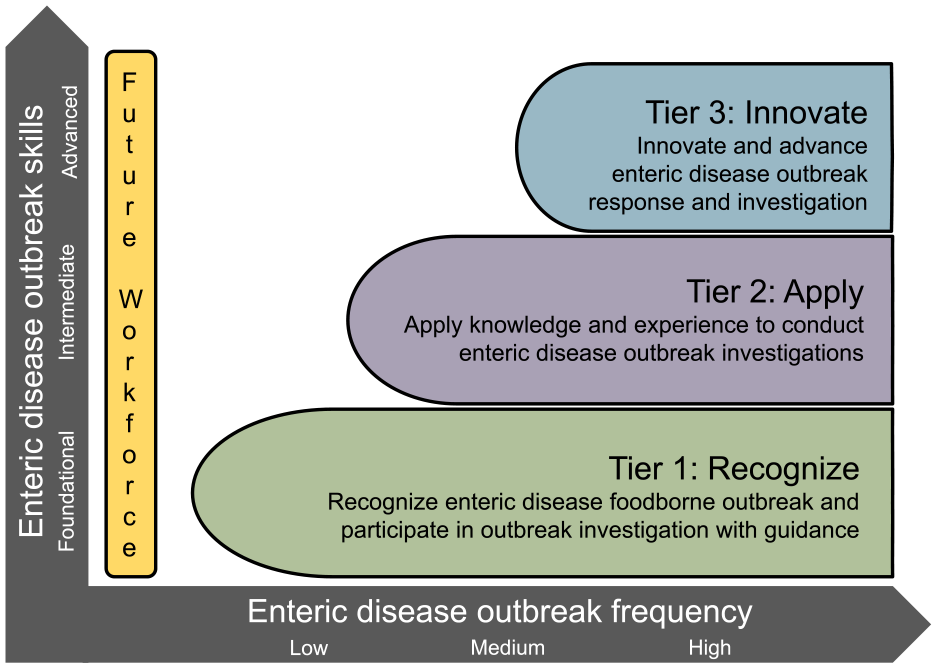
Workforce framework prepared by the Integrated Food Safety Centers of Excellence for public health professionals who detect and investigate enteric disease outbreaks in the epidemiology role. Three tiers in the framework progress from foundational to advanced levels of skill complexity on the vertical axis and low to high levels of foodborne disease outbreak investigation frequency on the horizontal axis. Tier 1 includes professionals with foundational skills working at agencies with low, medium, or high outbreak frequency. Tier 2 includes professionals with intermediate skills working at agencies with medium or high outbreak frequency. Tier 3 includes professionals with advanced skills working at agencies with high outbreak frequency.
Core Competencies
Using the conceptual framework, the working group drafted core competencies for each of the 3 professional tiers. The working group identified competency themes with the aid of existing trainings identified in an environmental scan of training websites and resources; subject matter experts reviewed the themes. The working group developed each competency using tier-specific language, with tier 1 verbs emphasizing participation and support for other tiers, tier 2 verbs being action oriented, and tier 3 verbs emphasizing leadership and innovation. For example, for the outbreak detection competency, a tier 1 investigator “recognizes how to use surveillance and other data sources to detect outbreaks,” a tier 2 investigator “detects clusters and outbreaks using surveillance and other data sources,” and a tier 3 investigator “improves methods for cluster and outbreak detection.”
The Integrated Food Safety Centers of Excellence Training and Continuing Education Working Group, consisting of academicians and public health practitioners from all Integrated Food Safety Centers of Excellence and CDC, reviewed the initial competency draft. The competencies working group made changes to the wording after this review, including verb changes to reflect the expectations more accurately for each tier.
Next, the working group convened a focus group via bidirectional video for 2 sessions. Both sessions included practicing epidemiologists from all 3 professional tiers representing local, regional, and state public health agencies, with variable tenure in the foodborne disease field (ranging from ≤2 years to >10 years). During the first session, focus group participants independently reviewed the competencies and the tiered framework and answered the following questions: (1) Are there competencies that do not apply or are not relevant to your work? (2) Are there competencies that are missing? and (3) Do the competencies match the expectation for that professional tier? During the second session, focus group participants qualitatively discussed the feedback from the first session and made modifications to the competencies by consensus. After the focus group completed the review, we shared the competencies with subject matter experts, including representatives from the Colorado Integrated Food Safety Center of Excellence Regional Steering Committee, CDC Food Safety Office, the Council of State and Territorial Epidemiologists (CSTE) Food Safety Working Group, and a senior instructional designer at the Rocky Mountain Public Health Training Center.
Practitioner Survey
We developed and disseminated an anonymous survey to public health practitioners in 2 stages: the first stage in August 2018 targeted epidemiologists working at state public health agencies and the second stage in June 2019 targeted practitioners working at local public health agencies. We included an introduction and questions about primary roles in foodborne disease outbreak investigations (“epidemiology,” “other,” and “do not investigate” for the state survey and “epidemiology,” “environmental health,” “laboratory,” “other,” and “do not investigate” for the local survey), average number of foodborne and enteric disease outbreaks annually investigated by their agency, their years of public health experience investigating foodborne and enteric disease outbreaks, and their state. Respondents self-selected their professional tier by choosing 1 of 3 short job descriptions. Based on the response to this question, the survey navigated respondents to competencies for that tier, where they rated each competency on the importance and frequency demonstrated in their practice. After state practitioners completed the survey, we made minor changes to the competencies based on feedback from the state practitioners, which were included in the survey for local public health practitioners. In addition, we asked local practitioners to choose 5 competencies they would prioritize for training opportunities, whether any of the competencies were difficult to understand, and whether they thought any competencies that were not included should be included.
We created both surveys using Qualtrics. We provided an open-ended question for respondents to provide comments and gave respondents an option to enroll in a raffle for a $20 gift card. For both the state and local surveys, we randomized the competency questions to avoid respondent fatigue.
Staff at the Colorado Integrated Food Safety Center of Excellence performed a pilot test of the survey. In August 2018, we used a CDC contact list to disseminate the survey to foodborne epidemiologists working at state or territorial public health departments. We promoted the survey using the CSTE listserv of state epidemiologists and through coordinators at each Integrated Food Safety Center of Excellence. In June 2019, Integrated Food Safety Centers of Excellence coordinators promoted the survey targeting local-level practitioners.
We used SAS version 9.4 (SAS Institute Inc) to analyze survey data. To combine survey results, we combined the state-level responses, which used a 10-point scale, to match the 5-point and 4-point response scales on the local-level survey. For our analysis, we included only respondents who answered “epidemiology” as their primary role and answered at least 50% of competency questions.
This project involved program evaluation and did not involve human subjects research; therefore, per the Colorado Multiple Institutional Review Board self-evaluation tool, institutional review board assessment was not necessary.
Results
The 15 competencies in each of the 3 tiers reflected the core set of knowledge and skills needed to detect and investigate enteric disease outbreaks in the epidemiology role (Table 1). The 15 competency topic areas were surveillance, outbreak detection, interview skills, investigation team, specimen testing, data analysis, hypothesis generation, study design, communication, enteric disease biology, control measures, legal authority, quality improvement, environmental health, and reporting to surveillance.
Integrated Food Safety Centers of Excellence competencies for public health professionals who detect and investigate enteric disease outbreaks in the epidemiology role, according to professional tier
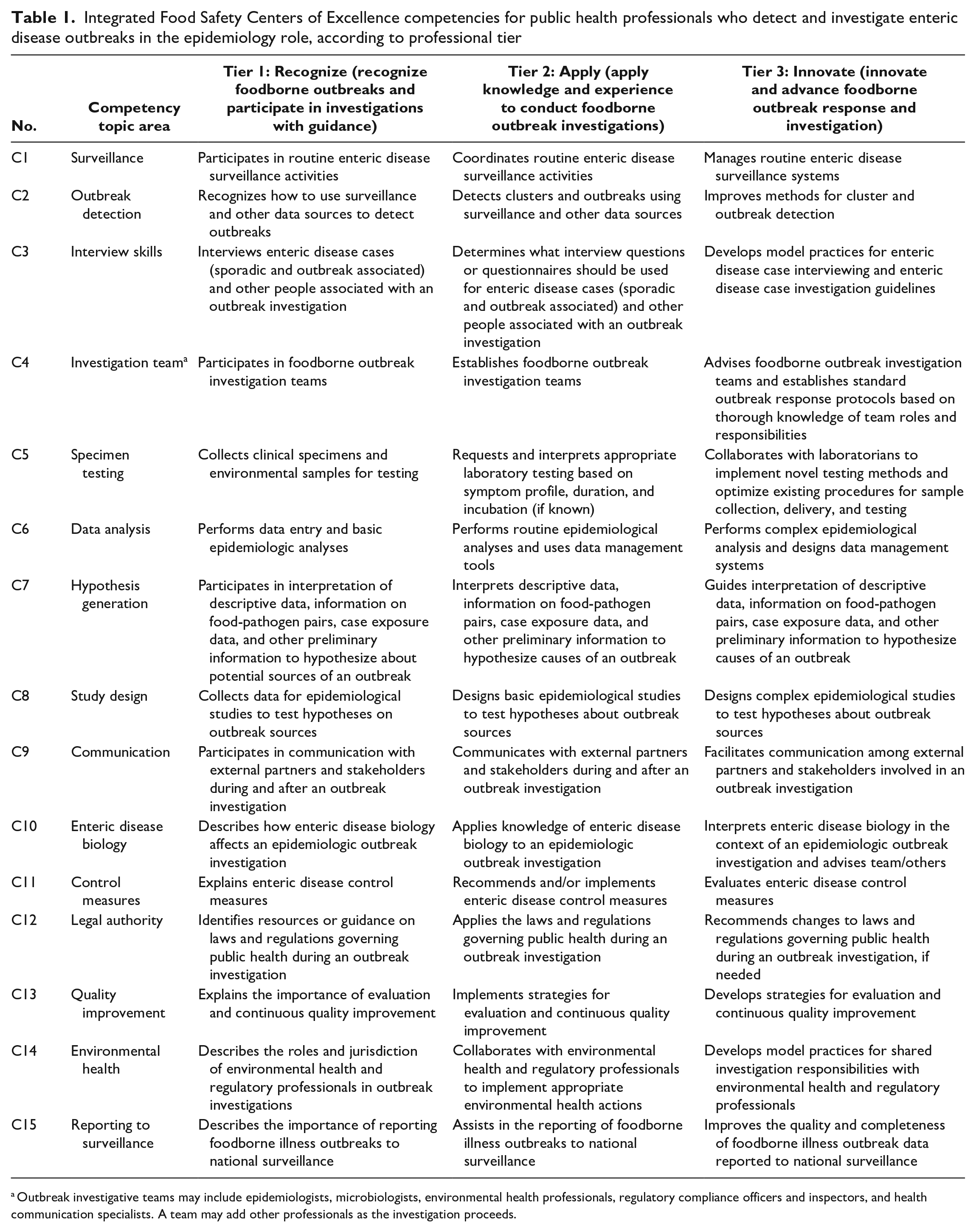
Outbreak investigative teams may include epidemiologists, microbiologists, environmental health professionals, regulatory compliance officers and inspectors, and health communication specialists. A team may add other professionals as the investigation proceeds.
Ninety-nine practitioners from state public health agencies and 187 practitioners from local public health agencies responded to the survey and reported working in enteric and foodborne disease response in the epidemiology role and completed ≥50% of questions about competency frequency and importance. Respondents represented 45 states, the District of Columbia, and Puerto Rico. Of 286 respondents included in the analyses, 129 (45.1%) self-selected as tier 1, 83 (29.0%) self-selected as tier 2, and 74 (25.9%) self-selected as tier 3. More local respondents than state respondents selected tier 1 (62.0% vs 13.1%), whereas more state respondents than local respondents selected tier 2 (46.5% vs 19.8%) and tier 3 (40.4% vs 18.2%). Tier 3 respondents were more likely than tier 1 and tier 2 respondents to report ≥10 years of experience (48.7%), and tier 2 and tier 3 respondents were more likely than tier 1 respondents to report investigating ≥5 outbreaks per year (79.5% and 83.8%, respectively) (Table 2).
Characteristics of respondents in a survey of local and state public health professionals in the United States disseminated in August 2018 and June 2019 to evaluate the Integrated Food Safety Centers of Excellence competencies for public health professionals who detect and investigate enteric disease outbreaks in the epidemiology role a
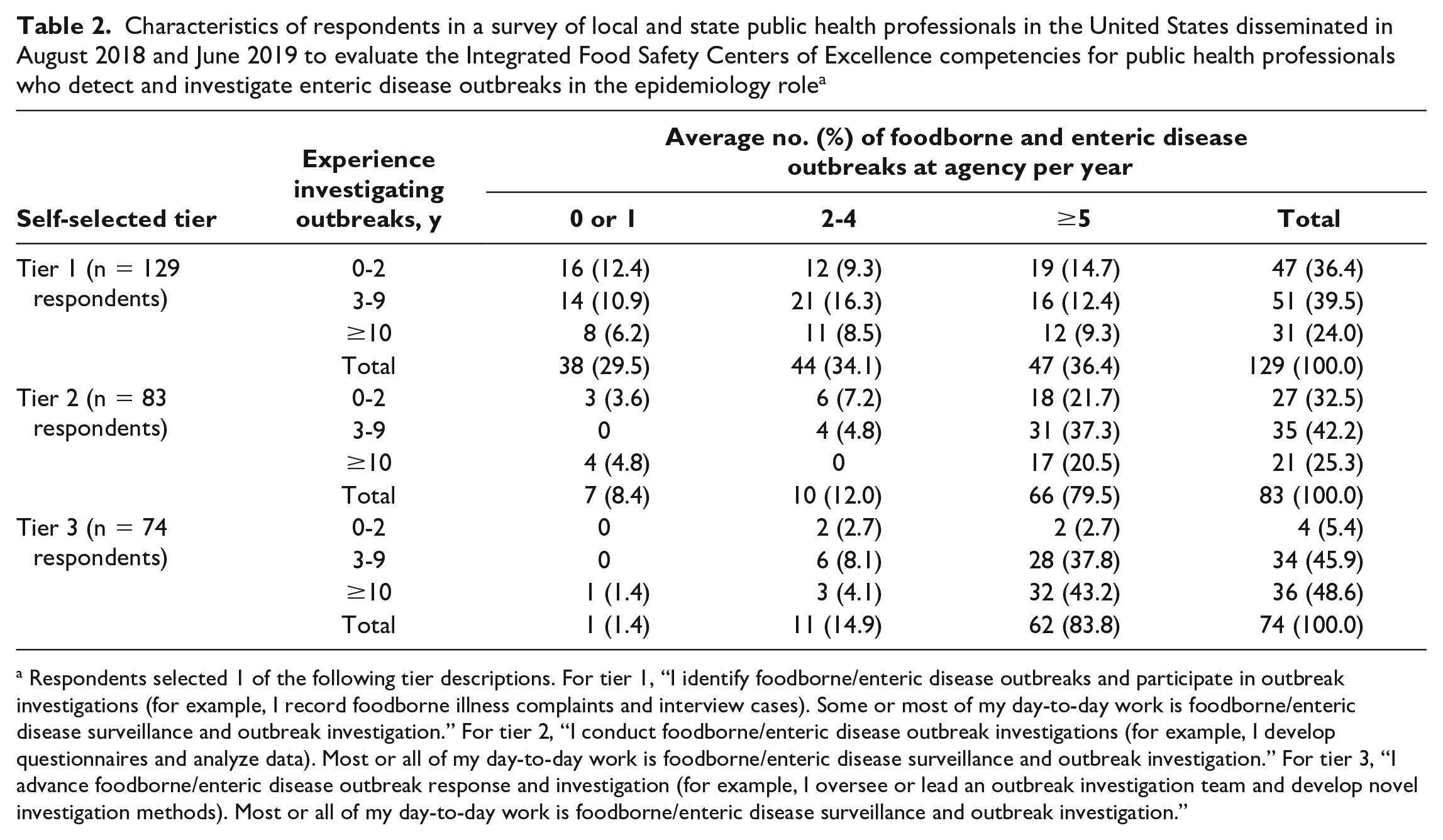
Respondents selected 1 of the following tier descriptions. For tier 1, “I identify foodborne/enteric disease outbreaks and participate in outbreak investigations (for example, I record foodborne illness complaints and interview cases). Some or most of my day-to-day work is foodborne/enteric disease surveillance and outbreak investigation.” For tier 2, “I conduct foodborne/enteric disease outbreak investigations (for example, I develop questionnaires and analyze data). Most or all of my day-to-day work is foodborne/enteric disease surveillance and outbreak investigation.” For tier 3, “I advance foodborne/enteric disease outbreak response and investigation (for example, I oversee or lead an outbreak investigation team and develop novel investigation methods). Most or all of my day-to-day work is foodborne/enteric disease surveillance and outbreak investigation.”
Respondents selected surveillance (C1), control measures (C11), interview skills (C3), communication (C9), outbreak detection (C2), and hypothesis generation (C7) as the most important and most frequent competencies. Respondents selected legal authority (C12), quality improvement (C13), and study design (C8) as the least important and least frequent competencies (Table 3). A similar proportion of respondents selected competencies as important and frequent, with the exception of specimen collection and legal authority (both 14% higher for importance than frequency) (Table 3, Figure 2).
Selection of competencies as very important or essential for importance, as sometimes or often for frequency, and as a top 5 training priority, overall and by self-selected professional tier, in a survey of local and state public health professionals in the United States disseminated in August 2018 and June 2019 to evaluate the Integrated Food Safety Centers of Excellence competencies for public health professionals who detect and investigate enteric disease outbreaks in the epidemiology role a
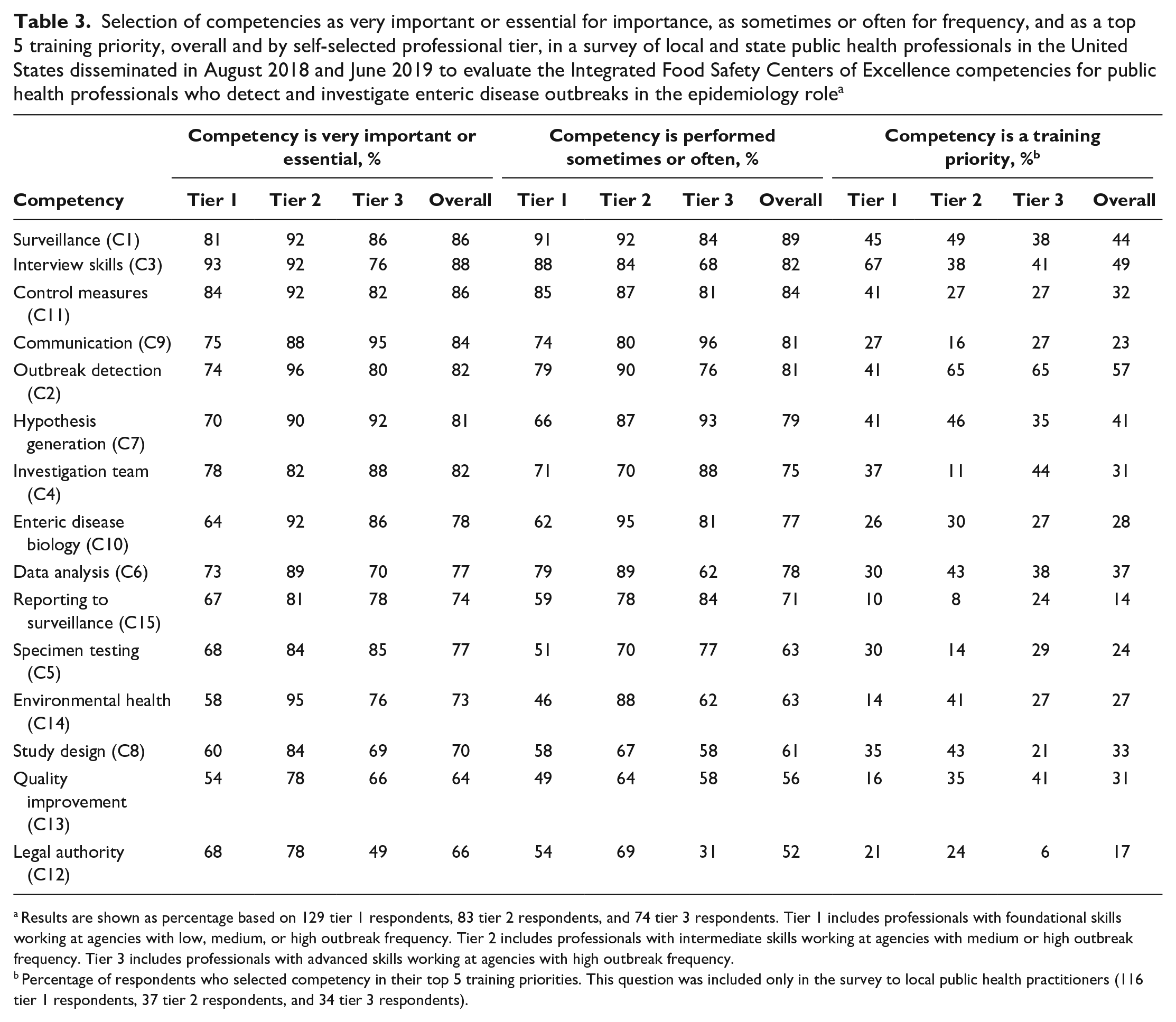
Results are shown as percentage based on 129 tier 1 respondents, 83 tier 2 respondents, and 74 tier 3 respondents. Tier 1 includes professionals with foundational skills working at agencies with low, medium, or high outbreak frequency. Tier 2 includes professionals with intermediate skills working at agencies with medium or high outbreak frequency. Tier 3 includes professionals with advanced skills working at agencies with high outbreak frequency.
Percentage of respondents who selected competency in their top 5 training priorities. This question was included only in the survey to local public health practitioners (116 tier 1 respondents, 37 tier 2 respondents, and 34 tier 3 respondents).
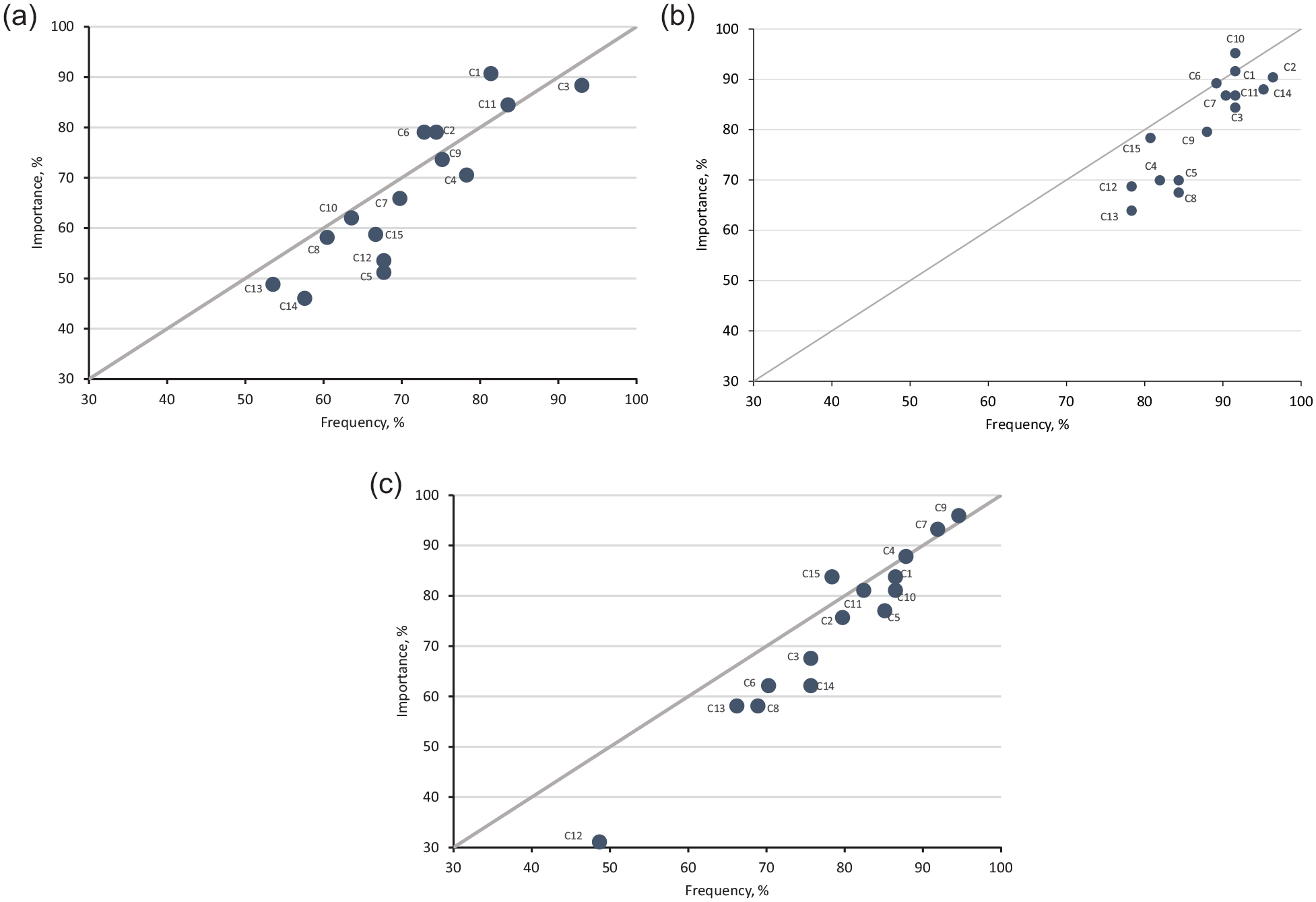
Ranking of Integrated Food Safety Centers of Excellence competencies, created for public health professionals who detect and investigate enteric disease outbreaks in the epidemiology role, according to a survey of local and state public health professionals in the United States (N = 286), by professional tier, August 2018 and June 2019. (A) Tier 1. (B) Tier 2. (C) Tier 3. Competencies (C1 through C15) were plotted by importance (percentage of respondents agreeing the competency is very important or essential) and frequency (percentage who perform the competency sometimes or often). Tier 1 included entry-level professionals or workers who were new to foodborne illness outbreak investigations and able to recognize and participate in outbreak investigations with guidance. Tier 2 included professionals who routinely detect, investigate, and respond to outbreaks and have the knowledge and skills required to conduct all aspects of the outbreak investigation. Tier 3 included professionals who were in senior, supervisory, or managerial roles and able to direct, innovate, and advance outbreak detection, response, and investigation. C1, surveillance; C2, outbreak detection; C3, interview skills; C4, investigation team; C5, specimen testing; C6, data analysis; C7, hypothesis generation; C8, study design; C9, communication; C10, enteric disease biology; C11, control measures; C12, legal authority; C13, quality improvement; C14, environmental health; and C15, reporting to surveillance.
Competency importance and frequency differed by tier, with professionals in tier 1 ranking interview skills (C3), surveillance (C1), and control measures (C11) as the most important and most frequent competencies. Respondents in tier 2 ranked enteric disease biology (C10), outbreak detection (C2), and surveillance (C1), and professionals in tier 3 ranked communication (C9), hypothesis generation (C7), and investigation team (C4) as the most important and most frequent competencies (Figure 2). Some differences in state and local respondents were noted (eTable 1 and eTable 2 in Supplemental Material).
The competencies most often selected as training priorities included interview skills (C3), outbreak detection (C2), surveillance (C1), hypothesis generation (C7), and data analysis (C6). Training priorities differed by tier; for example, tier 3 was the only group that identified quality improvement (C13) and investigation team (C4) in their top 5 priorities, and tier 2 was the only group that identified study design (C8) and data analysis (C6) (Table 3).
Discussion
In this collaborative effort across Integrated Food Safety Centers of Excellence with local, state, and federal partners, we developed a conceptual framework to describe the workforce and 15 competencies for public health professionals who detect and investigate enteric disease outbreaks in the epidemiology role. In the absence of existing competencies specific to this field, the Integrated Food Safety Centers of Excellence primarily aimed to inform the development and evaluation of Integrated Food Safety Centers of Excellence trainings and curricula. In addition, practitioners can use the framework and competencies to assess competency and to map a path for continuing education and training, and supervisors can use the framework and competencies to develop staff training plans or job descriptions. The framework and competencies presented here do not represent the full scope of a position in a public health agency. Rather, they complement other models, specifically the CDC/CSTE Applied Epidemiology Competencies, which include general competencies for epidemiologists and other areas outside of epidemiology that are crucial to the field, including competencies related to communication, management and leadership, and cultural proficiency. 10
We developed a conceptual framework of professional tiers to represent the diversity of the public health workforce that detects and investigates enteric disease outbreaks. Unlike the levels defined in the CDC/CSTE Applied Epidemiology Competencies, which represent a professional continuum, the framework defined here reflects different roles that map to experience level and agency type. For example, tier 1 professionals at small local public health agencies do not investigate as many outbreaks as tier 2 and tier 3 professionals at large agencies do, and local public health agency staff are more likely than state public health agency staff to be generalists who provide multiple services. However, in many states, particularly states in which public health governance is decentralized, local public health agencies are primarily responsible for receiving complaints of enteric disease and detecting complaint-based outbreaks. 11 Therefore, trainings and resources aimed at tier 1 professionals should emphasize detecting outbreaks. Conversely, tier 2 and tier 3 professionals at large local or state public health agencies may be more specialized in communicable disease work, including enteric or foodborne diseases in particular; therefore, trainings and resources aimed at tier 2 professionals should emphasize more complex outbreak response with practice-based and critical thinking exercises. Finally, tier 3 professionals are leaders in the field, and resources should provide forums for innovation and discussion of complex outbreak investigations, including communities of practice and smaller synchronous trainings, such as live learning series. 12
Respondents to our survey ranked surveillance, control measures, interview skills, communication, outbreak detection, and hypothesis generation as highest for importance and frequency. Although some consensus existed across tiers, we observed differences, some of which are explained by tier-specific roles and responsibilities; these differences have important implications for training development. For example, tier 1 respondents ranked interview skills as the most important and most frequent competency with the highest training priority. Environmental health professionals have similarly identified interview skills as a need. 7 Interviews with case patients are the backbone of enteric disease investigation, and investigators must be familiar with enteric disease biology and questionnaires and be skilled in building rapport with case patients, collecting complete food histories, asking sensitive questions, and identifying links between cases. 13 The Integrated Food Safety Centers of Excellence have developed several interview trainings and resources, including mock interview guides, toolkits, and live learning series. 4 Although tier 2 and tier 3 respondents did not rank interview skills as highly as tier 1 respondents, they did highly rank outbreak detection and surveillance, which are closely linked to interviewing. Therefore, these topics may be appropriate for more advanced trainings that incorporate problem-solving and critical thinking skills, as well as more advanced methods, such as the iterative interviewing model. 13
In general, tier 2 respondents ranked competencies higher than tier 1 and tier 3 respondents did, perhaps because enteric disease surveillance and outbreak investigation are part of their routine work. Tier 3 respondents ranked communication and hypothesis generation as the most important and most frequent competencies. As supervisors or as experienced outbreak investigation team members, tier 3 investigators may be more likely than tier 1 or tier 2 professionals to coordinate internal and external communication during an outbreak and to take on epidemiological approaches that require more experience and expertise, such as hypothesis generation and testing. These are more complex training topic areas and require different modalities, such as the Integrated Food Safety Centers of Excellence Hypothesis Generation for Foodborne Illness Extension for Community Healthcare Outcomes series. 14
In contrast to the highest-ranking competencies, all tiers consistently ranked the lowest-ranking competencies, with all 3 tiers ranking legal authority and quality improvement lower than other competencies. These competencies could have a low priority, respondents may have found these competencies difficult to understand, or respondents did not view them as having a clear connection to their routine work. The competencies selected as high training priorities were not always competencies with high importance and frequency. For example, quality improvement was ranked low for importance and frequency among all 3 tiers but was ranked highly as a training priority for tier 3 respondents. Some competencies were ranked high for frequency and importance (eg, communication, control measures) but not for training, perhaps because sufficient training resources or on-the-job training already exist or because these competencies are challenging topics for effective and engaging training.
Local and state public health agencies report understaffing and lack of training as the most common barriers to successfully investigating enteric disease outbreaks. 5 Training is particularly important at local and regional public health agencies, because most investigators do not have formal epidemiology training and education 5 ; in addition, lack of experience has been exacerbated by the competing demands and staff turnover resulting from the COVID-19 pandemic response. 15
Limitations
Our study had several limitations. First, the workforce framework and competencies were developed by an expert committee consisting primarily of Integrated Food Safety Centers of Excellence epidemiologists. Although we made a concerted effort to reach a broad and representative audience, including practitioners at local, state, and federal agencies and across a spectrum of experience levels, individuals who provided input and responded to the survey were self-selected and may not be representative of all public health professionals. Second, respondents self-selected their professional tier. Third, the survey for local practitioners was disseminated after the state practitioner survey, and we had made minor improvements, perhaps resulting in differences in survey responses. Fourth, although respondents were instructed to respond for themselves, some may have responded on behalf of their team or jurisdiction, particularly among tier 3 respondents.
Conclusions
The Integrated Food Safety Centers of Excellence created the first published workforce framework and competencies for public health professionals who detect and investigate enteric disease outbreaks in the epidemiology role. The workforce framework and competencies have been incorporated into the Integrated Food Safety Centers of Excellence training and continuing education program 4 and can be used with existing trainings and resources to develop a training curriculum and self-evaluation tools. These competencies can also be used to assess and evaluate the workforce over time. Competency model development is an iterative process, and we plan to regularly review and update this model.
Supplemental Material
sj-docx-1-phr-10.1177_00333549231186776 – Supplemental material for Competencies for Public Health Professionals and Epidemiologists Who Detect and Investigate Enteric Disease Outbreaks
Supplemental material, sj-docx-1-phr-10.1177_00333549231186776 for Competencies for Public Health Professionals and Epidemiologists Who Detect and Investigate Enteric Disease Outbreaks by Alice E. White, Michelle R. Torok, Kirk E. Smith, Hillary Booth and Elaine Scallan Walter in Public Health Reports
Footnotes
Acknowledgements
The authors acknowledge the public health professionals who participated in focus groups and responded to our survey, as well as the individuals and organizations that provided input on the tier framework and competencies, including the Centers for Disease Control and Prevention Food Safety Office, the Colorado Integrated Food Safety Center of Excellence Regional Steering Committee, the Council of State and Territorial Epidemiologists Food Safety Working Group, the Integrated Food Safety Centers of Excellence, and the Rocky Mountain Public Health Training Center.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by the Colorado Integrated Food Safety Center of Excellence, which is supported by the Epidemiology and Laboratory Capacity for Infectious Disease Cooperative Agreement through the Centers for Disease Control and Prevention.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.