
Abstract

Keywords
American Indian and Alaska Native (AI/AN) communities draw strength from Tribal culture and traditional ways of life, but social determinants of health, such as poverty, racial discrimination, unemployment, poor housing, and inadequate access to health care, contribute to persistent health disparities.1-3 Despite their resilience, AI/AN communities have disproportionate rates of obesity, diabetes, and other chronic and infectious diseases, including influenza, pneumonia, and COVID-19.4-9 The public health infrastructure required to address these inequities, however, is under-resourced and underdeveloped.10-12 The COVID-19 pandemic compounded these long-standing health inequities, elevating the need to address gaps in the current public health infrastructure.13-21
In national health initiatives, Healthy People 2030,22,23 Public Health 3.0, 24 and the 10 Essential Public Health Services framework, 25 strategies to address social determinants of health and health equity, are multifaceted and complex and require robust public health infrastructure. To address infrastructure needs in AI/AN communities, the Centers for Disease Control and Prevention (CDC) developed the Tribal Epidemiology Center Public Health Infrastructure (TECPHI) program, a 5-year investment (2017-2022) to address gaps in data and build public health capacity to promote health and prevent disease in AI/AN communities.26,27 The impetus for the TECPHI program came from recommendations from the CDC/Agency for Toxic Substances and Disease Registry Tribal Advisory Committee, which supports CDC’s government-to-government relationship with Tribes and allows for engagement with Tribal leaders on approaches to promote health in AI/AN communities. 28
TECPHI Model Description
With input from the Tribal Advisory Committee, CDC designed TECPHI to supplement the 12 existing Tribal Epidemiology Centers (TECs) to strengthen public health infrastructure and capacity, improve health by identifying and addressing health risks, and support disease prevention and control.26-28 The TECPHI model illustrates how collaboration, community-focused engagement, and leveraging resources across the 12 TECs can address common priorities while tailoring public health services to meet regional and local needs (Figure). The TECPHI model encourages CDC and TECs to continuously engage with the communities they serve. Unlike other previous CDC-supported public health infrastructure programs at state and local agencies,26-34 development of the TECPHI model and evaluation were led by recipients. The TEC-based Network Coordinating Center (NCC) facilitated recipient engagement in the design, implementation, monitoring, and evaluation of the program.
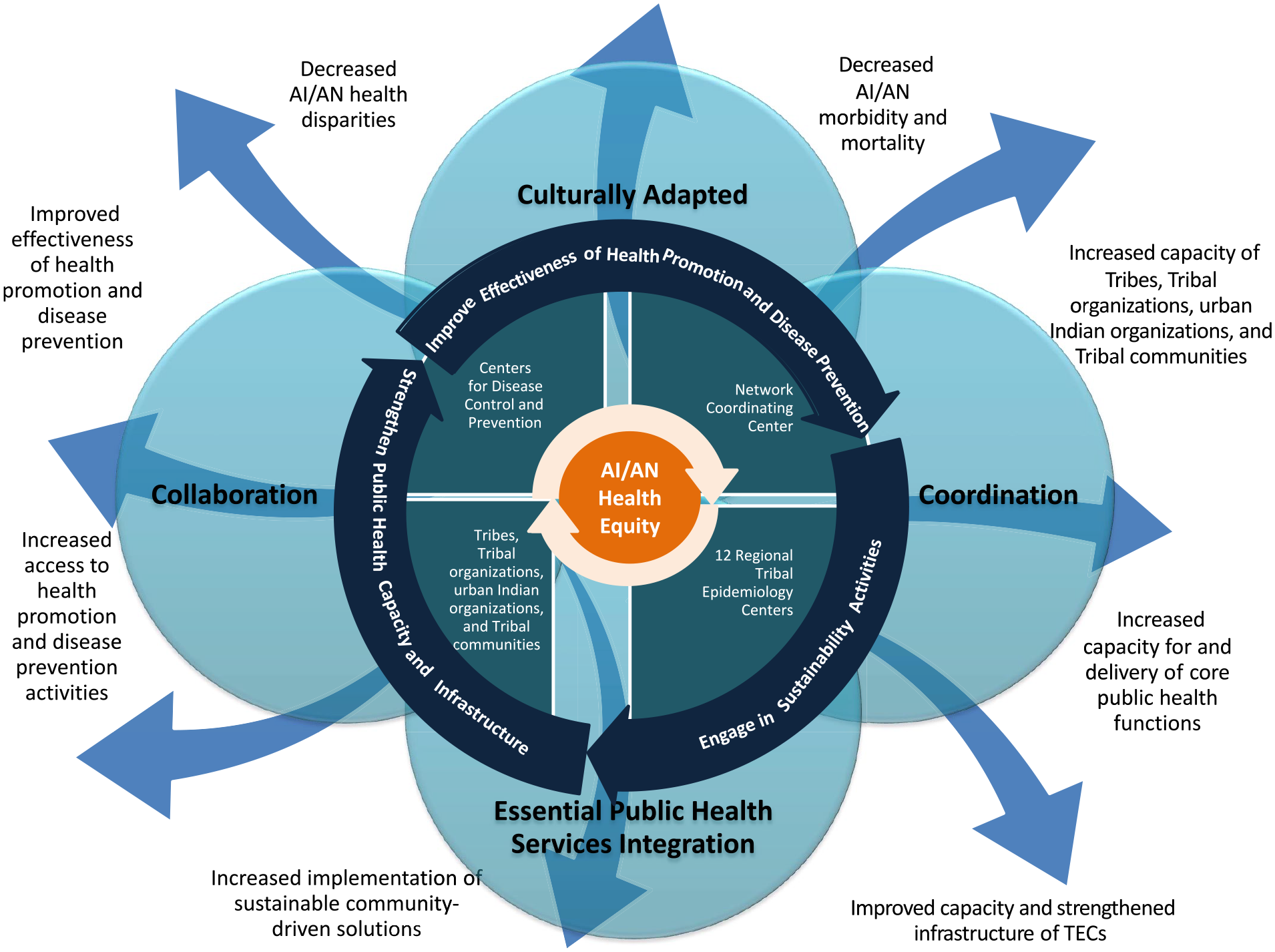
Tribal Epidemiology Centers public health infrastructure program model. The arrows are not specific to the individual outcomes; they are coming from the collective inputs, activities, and core values representing an Indigenous process and approach to achieving the outcomes. Abbreviations: AI/AN, American Indian/Alaska Native; TEC, Tribal Epidemiology Center.
Purpose
Community engagement is a key driver of improving health and achieving health equity. 4 Community input is particularly critical in AI/AN communities because Tribes, as sovereign nations, own and control the use and dissemination of their data. We describe the participatory, culturally responsive, highly collaborative approach CDC took to enhance Tribal public health infrastructure and capacity and the resulting measurable changes. These changes align with the 5 recommended areas described in Public Health 3.0 to improve public health services: (1) workforce development, (2) data and information systems, (3) partnerships and collaboration, (4) funding and sustainability, and (5) foundational infrastructure. 24 We also demonstrate how infrastructure developed in the first 2 years of the program and how the flexibility of the TECPHI model enabled TECs to pivot from performing programmatic work to supporting COVID-19 responses, highlighting how investments in TEC infrastructure enhanced services for Tribes and AI/AN communities.
Evaluating the Success of the TECPHI Model
Using participatory methods, the NCC developed and implemented a mixed-methods evaluation with input from all TECs. The TECPHI evaluation design was guided by the overarching question, “What can TECs do now that they were not able to do before TECPHI?” The NCC and CDC collect and analyze recipient data annually, including quantitative performance measures and reports that summarize findings from local TEC evaluations; collected data respond to the overarching question. The national TECPHI program evaluation plan is adapted collaboratively to incorporate changing contexts and new data annually. This approach resulted in supplemental recipient-identified evaluation projects and written narratives derived from Indigenous and culturally responsive evaluation methods such as PhotoVoice, storytelling, interviews, focus groups, and case studies to contextualize the data on performance measures and demonstrate successes. Because of this adaptive framework, the NCC and TECs were able to incorporate the outcomes related to unprecedented events, such as COVID-19, into the evaluation.
The data and results presented here were from years 1 through 3 (2017-2019). The NCC collects data on performance measures and results of qualitative evaluation components from TECs using REDCap, an online survey data collection system. The NCC analyzes and synthesizes data and disseminates results annually. Results are shared by strategies prioritized by TECPHI and align with the 5 Public Health 3.0 recommendations. 24
Workforce Development
A diverse workforce trained in core public health competencies is a cornerstone of public health infrastructure and development.3,4 The TEC workforce increased by 72%, from 204 in year 1 to 351 in year 3. The proportion of TEC staff with any health-related degree also increased, from 45% in year 1 to 72% in year 3. TECPHI’s staffing support helped increase the representation of AI/AN TEC staff, who now comprise approximately one-third of all TEC staff. Recruitment and retention of an AI/AN public health workforce is critical for sustainability and ensuring incorporation of cultural perspectives.
TECPHI funds contributed to developing a pipeline for public health practitioners, supporting 33 internship opportunities across TECs. With new staff, TECs increased their capacity to develop and implement systems to support technical assistance requests from Tribal and urban Indian organization (UIO) partners. These systems allowed for better tracking and increased response to technical assistance requests, from 660 in year 1 to 1712 in year 3.
To further support TEC staff development, the NCC partnered with the TRAIN Learning Network and the Public Health Foundation to establish learning management systems to support core public health competencies (https://www.train.org/main). By year 3, TECs had delivered 566 trainings. In year 3 alone, more than 40 000 individuals across the country were reached through 287 training opportunities supporting TEC staff, Tribal partners, and UIO partners with topics such as data visualization, grant writing, grant management, evaluation, chronic disease prevention, and COVID-19.
Data Information Systems
Acquisition and use of data to characterize health disparities and inform interventions is a critical component of public health infrastructure and a core function of TECs.26,27 Respecting and supporting Tribal data sovereignty, identifying appropriate data sources, and working across multiple jurisdictions (Tribal, county, state, federal) requires partnerships to support data access. Development of data-sharing agreements among Tribal and UIO partners, TECs, CDC, and the Indian Health Service is challenging but essential to streamline public health efforts and avoid duplicative work across sectors. In 3 years, TECs tripled the number of data-sharing agreements, with 70% (266 of 380) of new or expanded agreements representing Tribal partnerships. Eight TECs reported enhanced collection and surveillance of health data. In addition, TEC staff strengthened their capacity to access, analyze, and use data by attending a variety of TECPHI-supported trainings.
This increased capacity resulted in the production and dissemination of more than 1660 publications (eg, journal articles, AI/AN-specific fact sheets, educational materials) by TECs in year 3. The NCC led the development of a supplement in the Journal of Public Health Management and Practice to highlight TECs’ peer-reviewed work. 35 Furthermore, the increased systems capacity for data collection, management, analysis, and dissemination enabled TECs to support COVID-19 response efforts, provide data for AI/AN communities, and assist with culturally tailored health messaging. 16
Developing Partnerships and Collaboration
Public Health 3.0 states that strategic partnerships across sectors and with communities are essential to leverage resources and work toward collective action. 24 In addition to the aforementioned partnerships established to increase data access, in year 3, TECs reported establishing 537 new or expanded partnerships, 59 of which were with Tribal or state health departments. These partnerships included formalized contractual agreements and subawards. In years 1 through 3, 10 TECs provided 82 subawards totaling more than $2 million directly to Tribes, Tribal health programs, and UIOs to support public health infrastructure development and chronic disease prevention. Subawardee activities included community health assessments, data collection for the Tribal Behavioral Risk Factor Surveillance Survey, adverse childhood events surveillance, other health-related surveys, quality improvement activities, and the development, implementation, and evaluation of culturally relevant and appropriate health promotion and disease prevention activities.
The NCC developed TEC Connect, a private, password-protected information-sharing platform for TEC staff, to strengthen communication and collaboration among TECs. The platform currently has more than 360 registered users. Information shared includes grant announcements, training opportunities, data products, and other resources (eg, toolkits, relevant literature) to support program activities. By the end of year 3, 237 publications had been downloaded from TEC Connect. The NCC also supports robust communities of practice for evaluation, data management, and program management. In the first 3 years, more than 260 participants attended 38 community of practice meetings to share and learn best practices.
Funding and Sustainability
Maintaining increases in public health infrastructure support for Tribes and UIOs beyond TECPHI is an important component of the program. Early on, the NCC coordinated the development of a strategic plan for TECs. The implementation and monitoring of the strategic plan are ongoing NCC efforts. The TECs identified the need to improve outreach and communication about the role and work of the TECs as a main objective during the strategic planning process, and in year 3, the NCC developed a TEC communications plan to better convey the contributions of TECs to constituents, external partners, and funders. In addition, the NCC sponsored sustainability planning training for TECs who then provided this support to Tribes and UIO partners. By year 3, most TECs had developed or were monitoring individual strategic plans: 10 TECs had provided strategic planning support and training to Tribes and UIOs, 7 TECs had completed and implemented sustainability plans, and 6 TECs had provided training and support to develop sustainability plans.
In Public Health 3.0, flexible and sustainable funding is a key driver of leveraging resources and achieving goals across sectors. 24 TECPHI funding provided TECs the flexibility to invest in foundational capacity and infrastructure. In years 2 and 3, 7 TECs and the NCC offered grant-writing and management-training opportunities to TEC staff, Tribes, and UIOs, contributing to an increase in the number of TEC-supported grant applications, from 170 in year 1 to 236 in year 3.
Foundational Infrastructure
The importance of strong public health infrastructure has been highlighted throughout the COVID-19 pandemic.9,13 AI/AN communities were disproportionately affected by COVID-19.3,8 The need for timely, relevant, and accurate data reflecting the incidence of disease and the importance of culturally relevant communication materials were critical to inform local, Tribal, and UIO COVID-19 policy making and interventions. Although all TECs reported challenges stemming from the COVID-19 pandemic, such as transitioning to virtual methods to maintain partner and community engagement, the aforementioned successes and the underlying infrastructure and partnerships established through TECPHI in the first 2 years were critical in supporting TEC engagement in response activities. All 12 TECs reported that the capacity developed through TECPHI strengthened their ability to support COVID-19 responses. Nine TECs reported leveraging TECPHI-supported infrastructure for COVID-19 coordination activities among local and state public health entities, Tribes, and Tribal health programs. Building on existing partnerships established through TECPHI to gain access to additional federal, state, local, and Tribal COVID-19 datasets, 8 of the 12 TECs supported the development of COVID-19 data dashboards and provided more than 1000 situational reports for Tribal and UIO communities. Seven TECs conducted COVID-19 contact tracing and case investigations for Tribes, Tribal organizations, and UIOs using TECPHI-supported capacity, and 9 TECs assisted with new COVID-19 surveillance data collection systems to support Tribal communities. One-third or about 510 of the more than 1700 technical assistance requests responded to in year 3 were for COVID-19–related data. TEC directors were also able to leverage the TECPHI-supported NCC infrastructure to establish weekly communities of practice to address COVID-19–related issues. Thanks in part to TECPHI-supported infrastructure, as additional COVID-19–specific funding became available, TECs were able to apply and transition COVID-19 response activities from TECPHI to other funding sources.
Discussion: The TECPHI Ripple Effect
The TECPHI program contributed to strengthening and supporting the TECs to enhance a culturally responsive, community-driven public health infrastructure so AI/AN communities are better equipped to address social determinants of health and advance health equity. The early success of the TECPHI program prompted CDC to expand TECPHI through a $13 million supplement in 2018 to combat the opioid epidemic in AI/AN communities. 34 These supplemental funds leveraged the enhanced infrastructure developed through TECPHI to improve opioid surveillance and further address racial misclassification. Although TECPHI was launched before Healthy People 2030 measures were finalized, it supported a culturally responsive approach to capturing outcomes that align with those tracked by Healthy People 2030 and Public Health 3.0 recommendations. TECPHI showed measurable effects on the workforce by increasing the number of staff trained in core public health competencies and establishing pipelines to support inclusion of AI/AN professionals in the public health workforce. Data collection, management, analysis, and dissemination were enhanced to identify and characterize the multidimensional factors that contribute to health disparities, allowing for the implementation and evaluation of culturally informed interventions while honoring Tribal sovereignty. The partnerships developed between TECs and with external partners, as well as the technical assistance and, in some cases, funding provided to Tribes and UIOs, expanded opportunities for collaboration and supported individual Tribal and UIO public health infrastructure.
Challenges
While the TECPHI model contributed to a more community-based engagement than other previous public health infrastructure programs at state and local agencies, the approach is time-consuming and can have sustainability challenges. As with other approaches to health promotion and disease prevention, intentional multisector collaboration, partnership, and strategic integration of activities require support from leadership and invested constituents. The longer-term systems-based approach can be challenging in AI/AN communities because of a lack of workforce expertise, difficulties with recruitment and retention, complex jurisdictional issues, cultural considerations, funding opportunities that work in isolation, and turnover in Tribal leadership. Unique data challenges also exist. Data for AI/AN communities are limited and often misclassified, fragmented, unrepresentative, or unavailable, and the infrastructure for data management and sharing is limited.33,35 While TECs have public health authority status, which should allow access to protected health data for public health purposes, 36 how public health authority is recognized and applied varies across state and federal agencies. TECPHI has made inroads in supporting the collection, access, and use of data while honoring Tribal data sovereignty, but more work needs to be done.
Future Steps
The excess incidence of COVID-19 and other infectious and chronic diseases in AI/AN communities6-9,16 highlights the need to continue public health infrastructure efforts with TECs. Continued dedicated funding for public health infrastructure-building activities in AI/AN communities and additional mechanisms for strengthening public health infrastructure for individual Tribes and UIOs are needed to continue advancing toward health equity.
Aligning public health infrastructure development for TECs, Tribes, and UIOs with existing public health infrastructure efforts such as the 10 Essential Public Health Services, Public Health 3.0, Healthy People 2030, public health accreditation standards, and national efforts to support public health workforce development 18 is critical. These national initiatives provide a roadmap for public health infrastructure development that allows TECs, Tribes, and UIOs to leverage existing resources and partnerships across sectors to ensure the inclusion of AI/AN communities in public health initiatives. It is important that these efforts not work in isolation and remain grounded in culturally responsive practices. TECs are connected to clinical health infrastructure supported by the Indian Health Service33,37 and public health partners at the national, state, local, and Tribal levels and are accountable to the communities they serve. These unique partnerships set the stage for collaborative opportunities to bridge clinical health care and public health services. Strengthening communication and funding to support TECs in these efforts is needed to nurture continued alignment and partnership with the clinical health care system. Finally, supporting data collection efforts, strengthening data management systems, and expanding data-sharing agreements with federal, state, and other public health data stewards to address these data challenges is crucial.
Building public health infrastructure is a complex endeavor. While AI/AN communities face unique challenges, the TECPHI program demonstrated success in incorporating community engagement to support the development and implementation of culturally responsive approaches and was successful in building the public health capacity of TECs and, by extension, the capacity of Tribes and UIOs. Continuing these efforts is critical to build a culturally informed and responsive public health infrastructure to address social determinants of health and, ultimately, achieve health equity.
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Tribal Epidemiology Centers Public Health Infrastructure Program is funded through cooperative agreement no. CDC-RFA-DP17-1704PPHF17.