
Abstract
Objectives:
During public health emergencies, people at risk of exposure or illness will likely be presented with extensive information about an unfamiliar topic and be asked to make decisions quickly. In difficult situations, people often turn to trusted leaders, including from their local faith-based congregation (FBC). We examined how people receive, interpret, and respond to health communication information from clergy and lay leaders from their local FBC during public health emergencies.
Methods:
We analyzed responses to 10 questions from a 2021 nationally representative US survey. Porter Novelli designed the survey and administered it to 4510 US adults aged ≥18 years, of whom 3553 people completed the survey. We examined sociodemographic characteristics, trust of health information from clergy and lay leaders, and willingness to engage in health behaviors recommended by their FBC and receive health services through their local FBC. All estimates were weighted. We conducted bivariate analysis with contrast t tests for proportions at α = .05.
Results:
More than half of adults (55.4%), including 65.8% of non-Hispanic Black and 58.8% of Hispanic or Latino adults, were members of an FBC. Among FBC members, a higher percentage of Hispanic or Latino (29.1%) and non-Hispanic Black (36.3%) adults than non-Hispanic White adults (20.4%) reported trust in their FBC for health information (P < .05). This trust translated into greater intent to engage in health behaviors promoted by the local FBC among non-Hispanic Black respondents (31.4%) compared with non-Hispanic White respondents (22.5%) (P < .05).
Conclusions:
Public health officials can consider ways to better understand how the cultures and practices of populations being served influence people’s health perceptions and behaviors. Collaboration between federal, state, and local public health officials and FBCs can promote health equity during public health emergencies.
During public health emergencies, federal, state, and local public health officials may advise people to get tested, adopt behaviors, or take medications or vaccines to prevent or treat illness. For example, in an anthrax incident, exposed people may need to take antibiotics and get vaccinated. 1 An Ebola outbreak might require that contacts be monitored for symptoms. 2 People may need to decide whether they will receive a newly developed vaccine, as happened during the COVID-19 pandemic. 3 People at risk of exposure or illness will likely be presented with extensive information about an unfamiliar topic and be asked to make decisions quickly. They may be inundated with unverified content, misinformation, and opinion presented as fact. Long-standing social and health inequities and systemic discrimination further complicate communication. In difficult situations, people often turn to trusted leaders, including leaders from their local faith-based congregation (FBC), for advice.4,5 However, little is known about how people interpret and respond to such communication.
Broadly speaking, it is important for public health leaders to understand the cultural aspects of how people respond to health information on unfamiliar topics. Weber and Dacin 6 described how increased public availability of information and flow across social boundaries enables individuals to combine diverse materials. Cultural analysis focuses on culture’s interface with external audiences and the public sphere, how individuals and organizations access diverse cultural materials, react to public demands and the media, and respond to third parties and public audiences. Questions arise about how individuals expand and reshape their perceptions and bring their values and preferences to their social group. For example, individuals may transition from religious logic to commercial market logic as they shift between the religious domain and the market domain. A need exists to better understand how the bidirectional transfer of culture can refresh and align culture inside and outside an organization and how individuals acquire new cultural resources but still reference their traditional norms. 6
In addition to cultural analysis, other aspects must be considered when working with FBCs. The Centers for Disease Control and Prevention’s (CDC’s) Crisis and Emergency Risk Communication (CERC) is a tool designed to educate and equip public health professionals to effectively communicate during public health emergencies. CERC provides a theoretical framework for explaining emergency risk communication and how individuals attempt to make sense of their circumstances based on past experience and personal interpretation. The goal of emergency risk communication is to provide people with the information and options to make decisions and take actions that save lives.7,8 Shapiro’s perspective contributes to this theoretical framework by considering religion as part of a causal pathway in which various factors work to affect health. 9 According to this framework, religious participation is a distinct worldview that permeates an individual’s thoughts and behaviors even when they are not performing religious acts. Shared beliefs, practices, and values can unite adherents into a cohesive group. Religious leaders may have great influence and authority not found in secular organizations, offering benefits for some behaviors and prohibitions against others. An especially high level of trust may exist among congregation members from the same group and between congregation members and their religious leaders. Attachment to an FBC is based not only on one’s intellect but also on strong emotional ties that may build up during a lifetime. 9 In addition to Shapiro’s perspective, Maselko et al 10 described religious social capital as social resources through connections with one’s religious community, including the skills and knowledge to integrate into the community and the emotional ties that keep members coming back. Bonding religious social capital refers to trust and cooperation among members of a religious community. Bridging religious social capital refers to links across religious groups, for example, the shared perception of access to a higher power, which can have important consequences for coping strategies. 10 Importantly, while social capital in general expects reciprocity from others, this expectation of reciprocity is less prevalent with religious social capital that emphasizes altruism. Thus, in a religious context, individuals might be motivated to voluntarily serve others, such as through efforts to protect people who are medically underserved and at increased risk of illness, even when they may not receive anything earthly in return. 9
We sought to determine the openness of FBC members to receive, and their reported likelihood to respond to, health communications from clergy and lay leaders in their local FBC. While this study is primarily a descriptive study, we hypothesized that there would be sociodemographic differences in openness to health communications and differences by frequency in FBC attendance.
Methods
We analyzed 10 questions from a 2021 Porter Novelli national survey (Table 1). 11 Using a 5-level Likert scale, we assessed respondents’ trust in their FBC as a health information source, perceived alignment of health information from their FBC with CDC or other public health agencies, self-reported likelihood of engaging in health behaviors promoted by their FBC and/or by CDC or other public health agencies, and likelihood of receiving health services provided at an FBC. We assessed frequent attendance at religious services, which may increase access to social supports, encourage health behaviors, promote adaptive coping mechanisms, and encourage volunteering, which are independently associated with improved health outcomes. 10
Questions included in a Porter Novelli survey of panelists aged ≥18 years representative of the noninstitutionalized US adult population, United States, September through October 2021
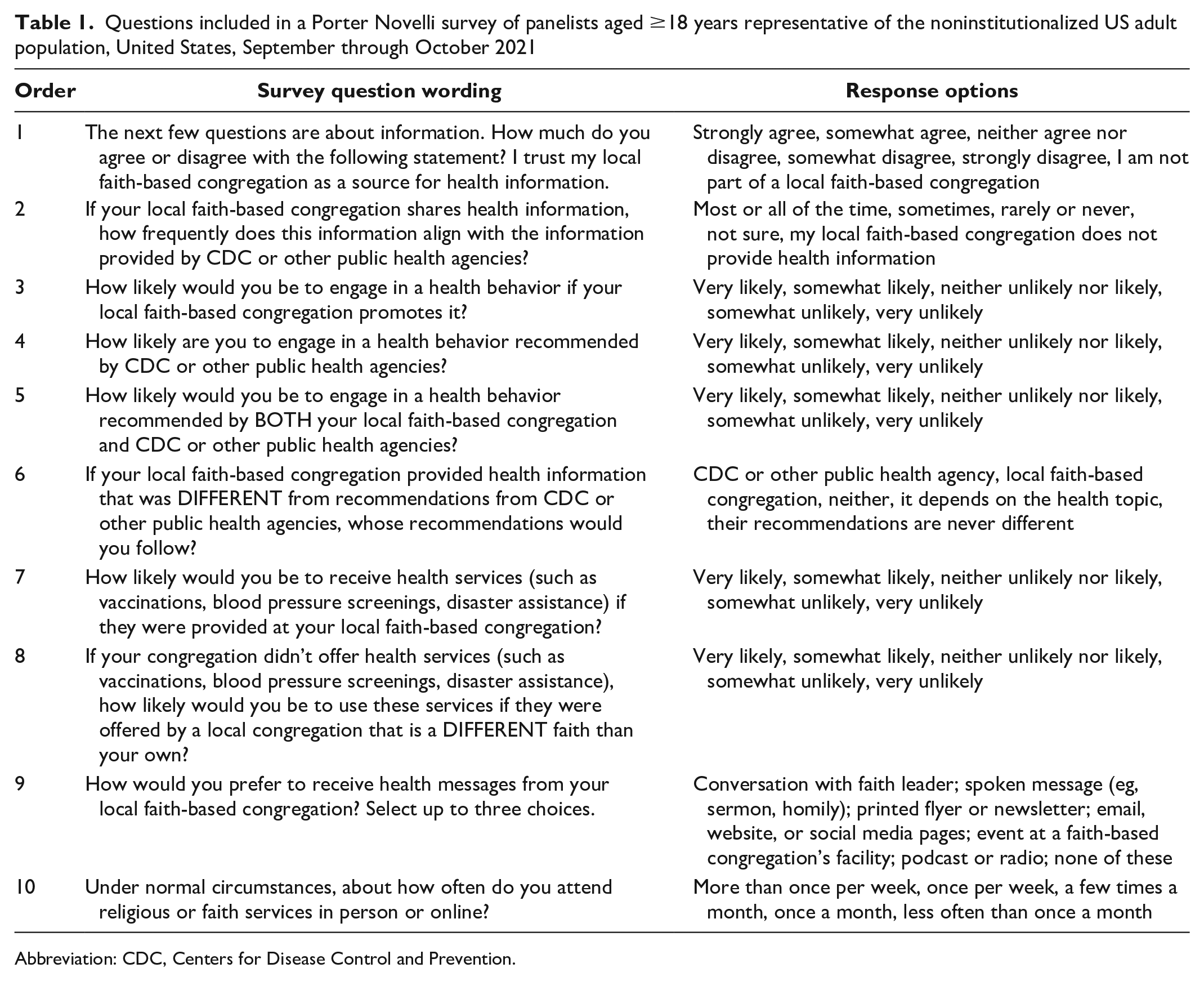
Abbreviation: CDC, Centers for Disease Control and Prevention.
Porter Novelli conducted the survey from September 24 through October 7, 2021, using Ipsos’ KnowledgePanel, an online panel survey weighted to be representative of the noninstitutionalized US population of adults aged ≥18 years. 12 Panel members were recruited by mail using probability-based sampling. Porter Novelli sent the survey to 4510 panelists aged ≥18 years; 3553 respondents completed the survey (78.8% response rate). Of these, 26 people did not respond to the “trust my FBC for health info” question used to define membership and trust in an FBC; therefore, the analytic sample size was 3527. Sociodemographic variables included respondent’s age group, education level, race and ethnicity, sex, annual household income, marital status, and metropolitan statistical area. Metropolitan residency status is defined as living in or near an urbanized area with a population ≥50 000. We conducted bivariate analysis using SAS version 9.4 (SAS Institute, Inc), and we used contrast t tests for proportions to test for group differences at α = .05; all reported differences were significant. Consistent with applicable federal law and CDC policy, CDC reviewed this analysis of precollected data and determined the analysis was not research; thus, institutional review board approval was not required.
Results
Membership and Attendance at FBCs
More than half of respondents (55.4%) were part of an FBC (Table 2). FBC membership was as follows: 65.8% non-Hispanic Black respondents, 58.8% Hispanic or Latino respondents, and 53.6% non-Hispanic White respondents. Adults with children in the household were more likely than adults without children to be part of an FBC (60.8% vs 52.9%). Adults who were currently married (60.2%) were more likely to be part of an FBC than adults who were widowed, divorced, or separated (50.8%) or never married (48.2%) (Table 3).
Characteristics of the study sample (n = 3527) from a survey of panelists aged ≥18 years representative of the noninstitutionalized US adult population, by reported membership in a faith-based congregation, United States, September through October 2021
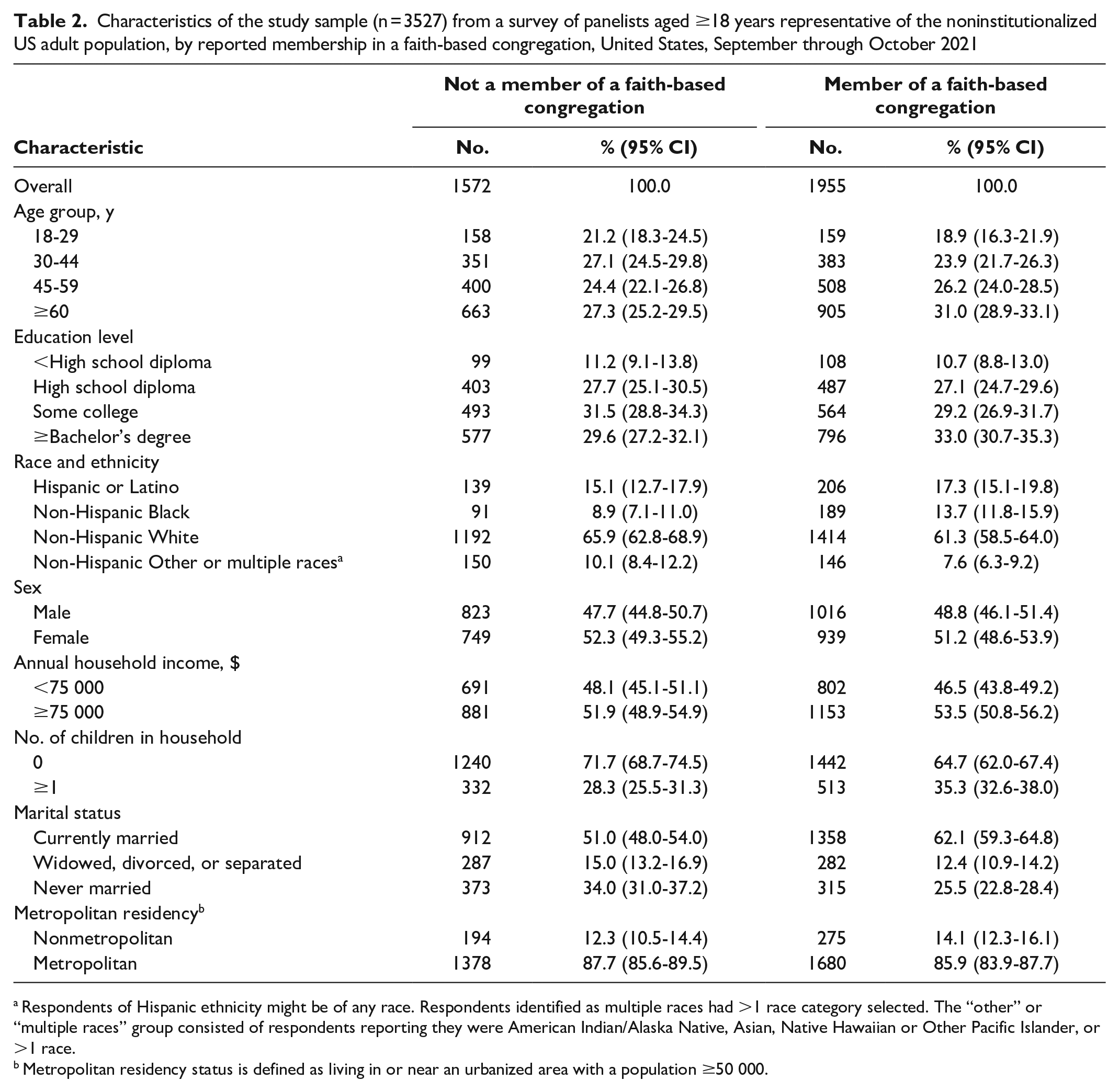
Respondents of Hispanic ethnicity might be of any race. Respondents identified as multiple races had >1 race category selected. The “other” or “multiple races” group consisted of respondents reporting they were American Indian/Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, or >1 race.
Metropolitan residency status is defined as living in or near an urbanized area with a population ≥50 000.
Characteristics associated with membership, frequent attendance, and trust in faith-based congregations (FBCs) for health information, from 3527 respondents to a survey of panelists aged ≥18 years representative of the noninstitutionalized US adult population, United States, September through October 2021
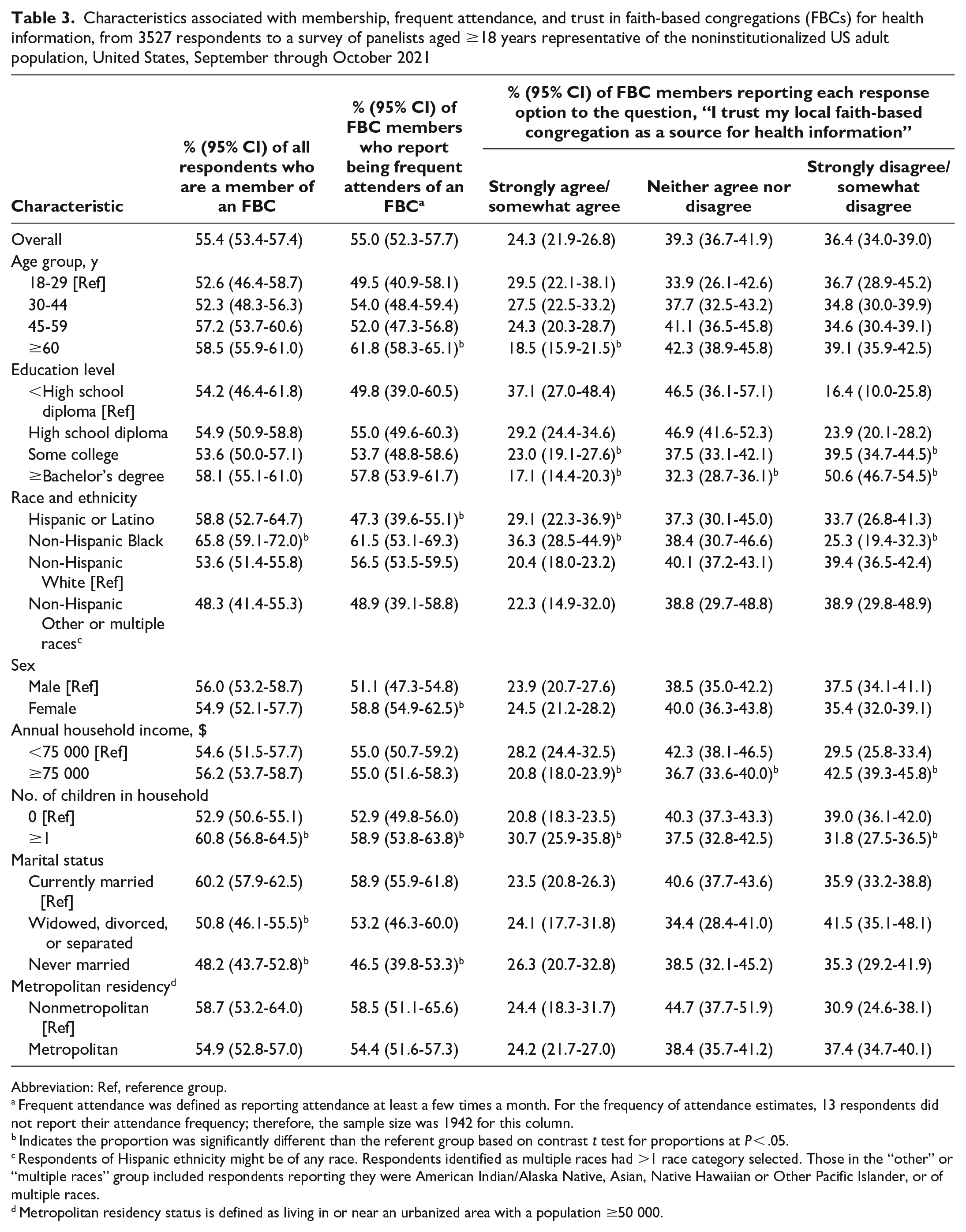
Abbreviation: Ref, reference group.
Frequent attendance was defined as reporting attendance at least a few times a month. For the frequency of attendance estimates, 13 respondents did not report their attendance frequency; therefore, the sample size was 1942 for this column.
Indicates the proportion was significantly different than the referent group based on contrast t test for proportions at P < .05.
Respondents of Hispanic ethnicity might be of any race. Respondents identified as multiple races had >1 race category selected. Those in the “other” or “multiple races” group included respondents reporting they were American Indian/Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, or of multiple races.
Metropolitan residency status is defined as living in or near an urbanized area with a population ≥50 000.
Among members of an FBC, 55.0% were frequent attenders (attended at least a few times a month). FBC members aged ≥60 years (61.8%) were more likely to be frequent attenders than FBC members aged 18-29 years (49.5%). Women (58.8%) were more likely than men (51.1%) to be frequent attenders. Those who had children in the household (58.9%) were more likely than adults without children (52.9%) to be frequent attenders. Members of an FBC who were never married (46.5%) were less likely to be frequent attenders than those who were currently married (58.9%) (Table 3).
Racial and Ethnic Minority Groups’ Trust in and Intent to Engage in Health Behaviors Recommended by Local FBCs
Among FBC members, a higher percentage of Hispanic or Latino (29.1%) and non-Hispanic Black (36.3%) adults compared with non-Hispanic White adults (20.4%) reported trust in their FBC for health information (Table 3). Among non-Hispanic Black respondents, this trust translated into intent to engage in health behaviors and receive health services (Table 4). Non-Hispanic Black respondents (31.4%) were more likely than non-Hispanic White respondents (22.5%) to report being somewhat or very likely to engage in health behaviors promoted by their FBC. Non-Hispanic Black respondents were also more likely than non-Hispanic White respondents to report being very or somewhat likely to receive health services at their local congregation (46.7% vs 31.2%) and to receive health services at a different congregation (29.0% vs 21.0%) (P < .05).
Likelihood of engaging in health behavior promoted by a faith-based congregation (FBC), CDC, or other public health agencies, among members of an FBC only, from a survey of panelists aged ≥18 years representative of the noninstitutionalized US adult population, United States, September through October 2021
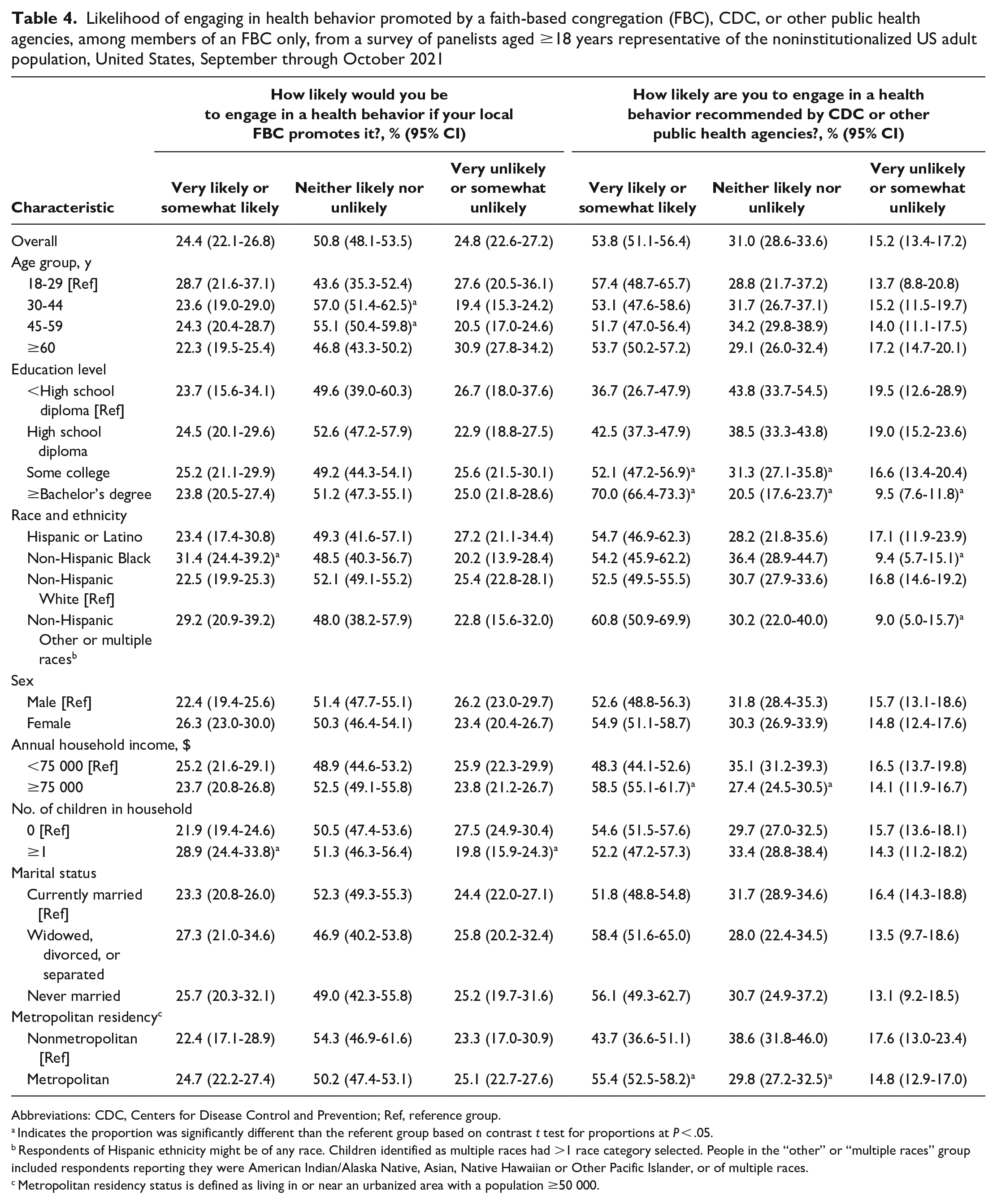
Abbreviations: CDC, Centers for Disease Control and Prevention; Ref, reference group.
Indicates the proportion was significantly different than the referent group based on contrast t test for proportions at P < .05.
Respondents of Hispanic ethnicity might be of any race. Children identified as multiple races had >1 race category selected. People in the “other” or “multiple races” group included respondents reporting they were American Indian/Alaska Native, Asian, Native Hawaiian or Other Pacific Islander, or of multiple races.
Metropolitan residency status is defined as living in or near an urbanized area with a population ≥50 000.
Sociodemographic Variations in FBC Influence
Adults who earned <$75 000 per year (vs ≥$75 000 per year) (28.2% vs 20.8%) and those with ≥1 child in the household (vs no children in the household) (30.7% vs 20.8%) were more likely to trust their FBC for health information. In contrast, a higher percentage of adults with some college (39.5%) or ≥bachelor’s degree (50.6%) compared with those who had Table 3). We did not identify differences by sex, marital status, or living in a metropolitan versus nonmetropolitan area. Among those who reported being somewhat or very unlikely to engage in a health behavior recommended by CDC or other public health officials, about one-fifth said they would engage in the health behavior if their local FBC promoted it.
Community Members’ Difficulties Identifying Reliable Information
Overall, 67.3% of FBC members reported that their congregation provides health information. Of these, 29.5% reported that the information aligns most or all of the time with the information provided by CDC or other public health agencies, 20.1% reported it aligns some of the time, 12.3% reported it aligns rarely or never, and 38.1% were not sure.
Among FBC members, frequent attenders were more likely than infrequent attenders to trust their FBC’s health information (30.1% vs 17.3%) and to report being very or somewhat likely to engage in health behaviors recommended by the FBC (34.5% vs 12.2%) (P < .001 for both comparisons). When health information from local FBCs was perceived as different from CDC and other public health agencies’ recommendations, 27.1% of members responded, “It depends on the health topic” on whose recommendation they would follow, and 25.9% said they would follow recommendations from “neither.” Only 2.6% reported, “Their recommendations are never different.”
Discussion
According to the CERC theoretical framework, emergency risk communication can provide people with the information and options to make decisions and take actions as they use their past experiences and personal interpretation to make sense of their circumstances.7,8 Several findings from this survey are noteworthy for emergency risk communication. First, our findings confirmed our hypotheses that there would be sociodemographic differences in openness to health communications and differences by frequency in FBC attendance. More than half of adults, including two-thirds of non-Hispanic Black and nearly 60% of Hispanic or Latino adults, were members of an FBC. The large number of people reporting membership in an FBC is consistent with previous reports.13,14 This finding also underscores why it is important for public health officials to understand the cultures and practices of populations being served, including their membership in an FBC and FBC attendance, and how these factors influence people’s health perceptions and behaviors, in addition to disseminating messages via mass media and new communication technologies. 7
Second, many people from racial and ethnic minority groups trust in and are likely to engage in health behaviors recommended by their local FBCs. Among FBC members in this survey, a higher percentage of Hispanic or Latino and non-Hispanic Black adults compared with non-Hispanic White adults reported trust in their FBC for health information. Among non-Hispanic Black adults, this trust translated into a higher likelihood of engaging in health behaviors and receipt of health services compared with non-Hispanic White adults. One might expect to find a high degree of religious social capital among groups that trust health information from, are willing to engage in health behaviors recommended by, and receive health services through their local FBC, as characterized by shared beliefs, practices, and values, trust, and strong emotional ties among congregation members; a shared perception of a higher power; and altruistic appeals to protect people who are medically underserved and at increased risk of illness. 9 Maselko et al 10 found that indicators of religious social capital were higher among those who frequently attended religious services compared with infrequent attenders.
Third, a concerning finding from this survey was that community members had difficulty recognizing reliable health information. Among those whose local FBC shared health information, more than one-third were unsure whether the information aligned with CDC and other public health agencies, and 12.3% reported that FBC health messages rarely or never aligned with CDC and public health recommendations. When asked about what health behavior they would engage in if health information from local FBCs was perceived to differ from CDC and public health recommendations, nearly one-third responded, “It depends on the health topic,” and more than one-quarter said they would follow “neither.” Access to diverse ideas, public availability of information, and communication flow across social boundaries enables individuals with high structural positions to be influential. 6 However, religious social capital and increased exposure to and reliance on other media sources for information does not always have a positive effect on health and may interfere with healthy behaviors or medically appropriate care seeking. 9 Perceived differences in health recommendations can be addressed in part through improved collaboration among FBCs, CDC, and state and local public health departments.15-17 Engaging trusted messengers and sustaining such collaborations is labor intensive but preferable to developing partnerships in the midst of a crisis. Having relationships and trust in place to address chronic health issues such as HIV and diabetes prior to an emergency may help to facilitate health equity in responses. 8 Sustaining collaborations may be particularly beneficial in light of hesitancy about public health guidance3,18 and in nonmetropolitan areas, where FBC attendees are less likely than those in metropolitan areas to engage in recommendations from CDC or other public health agencies.
Limitations
This assessment had several limitations. First, because the survey was cross-sectional, we do not know if and how findings may change over time. Second, questions concentrated on health information in general. Only 2 questions mentioned “disaster assistance” specifically. Third, conducting the survey during the COVID-19 pandemic may have influenced participants’ views about applicability to public health emergencies. Fourth, the survey did not ask respondents’ faith tradition, limiting our ability to assess differences among faith groups. Lastly, self-report bias and social desirability bias may have occurred.
Conclusions
We found that many people from racial and ethnic minority groups trust health information from and are likely to engage in health behaviors recommended by and receive health services through their local FBC. Cultural analysis and a theoretical framework with religion as part of a causal pathway in which various factors affect health can inform and guide practice implications for public health leaders. Ongoing collaboration between federal, state, and local public health officials and local FBCs can help promote health equity during public health emergencies.
Footnotes
Acknowledgements
The authors thank Rev. C. Burnett, ordained minister with the National Baptist Convention, USA, Inc, and former pastor of Wheat Street Baptist Church in Atlanta, Georgia, for her helpful insights. The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of CDC.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.