
Abstract
Needs assessments have been successful in helping communities and congregations focus their health ministry efforts; however, most have used leader perceptions of congregational health needs. The purpose of this study was to examine and compare the self-reported needs of both church leaders and members to be addressed by their congregation. Church leaders (n = 369) and members (n = 459) from 92 congregations completed the 2019 Mid-South Congregational Health Survey. Frequencies and generalized linear mixed models (GLMM) were performed to examine the top 10 self-reported needs and associations by church role, respectively. Of the top 10 congregational needs, anxiety or depression, high blood pressure, stress, and healthy foods were ranked identically regardless of church role. Church leaders perceived obesity and diabetes to be important congregational health needs, whereas members perceived affordable health care and heart disease to be important congregational health needs. GLMM, controlling for within-church clustering and covariates, revealed church leaders were more likely than members to report obesity (odds ratio [OR]: 1.93, 95% confidence interval [CI] = [1.39, 2.67], p < .0001) and diabetes (OR: 1.73, 95% CI = [1.24, 2.41], p = .001) as congregational needs. Findings display similarities and differences in needs reported by church role. Including many perspectives when conducting congregational health needs assessments will assist the development of effective faith-based health promotion programs.
Keywords
To address health disparities, researchers have noted the importance of using community-based participatory research (CBPR) approaches, which involve the community serving as an equal partner in the research process (Berge et al., 2009; Mendenhall & Doherty, 2005). A common evaluative CBPR approach is the use of community health needs assessments (CHNA), which are critical in describing disease patterns, identifying unmet needs, influencing policymaking to enact community change, and enhancing evidenced-based health programs (Beran, 2015; Issel & Wells, 2017; Pennel et al., 2017; Wright et al., 1998). Moreover, core CBPR principles (e.g., inclusivity, diverse perspectives, and equitable contribution from all partners) must be considered when implementing and evaluating CHNAs. For example, it is important to recognize the community as a unit of identity with shared interests and needs (Israel et al., 1994, 1998, 2001; Sarason, 1984). Various factors (e.g., income, education, age, and role) present within communities lead to diverse perspectives that influence self-reported health needs (Asadi-Lari et al., 2003; Harmon, Schmidt, et al., 2021).
Leaders within communities in particular may have different knowledge of community resources and needs as well as potential influence in policy decisions (Harmon, Schmidt, et al., 2021); therefore, obtaining input from a range of community leaders and members when developing and implementing CHNAs is an important step in identifying pressing health needs. With that said, community leaders, in some cases, are asked to speak on behalf of their members when assessing community needs (Pennel et al., 2017). While community leaders and members have been noted to have some overlapping needs (Bias et al., 2017; Bopp et al., 2012), members may report needs overlooked by community leadership (Bias et al., 2017). In addition, research suggests community leaders and members may prioritize community needs differently (Bias et al., 2017; Bopp et al., 2012), increasing the potential of inaccurate assessment of community needs (Bias et al., 2017). In faith communities, church leaders (e.g., senior pastors) also play an important role in the implementation of health promotion programs and in understanding the needs of the community; therefore, researchers often prioritize their input (Baruth et al., 2015; Jo et al., 2010).
Churches are important venues for addressing the needs of individuals in the local communities they serve (Goldmon & Roberson, 2004). Assessing congregational health and health needs has proven useful when implementing faith-based health promotion strategies, education programs, and health assessments (Lynch et al., 2019; Yanek et al., 2001). Congregational needs assessments, however, have not been widely implemented. Most congregational health needs assessments, while successful, have not assessed needs reported by both church leaders and members (Berkley-Patton et al., 2018; Whitt-Glover et al., 2014), further limiting our understanding of the alignment of perceptions between church leaders and members. Having a more comprehensive understanding of the needs in congregations and whether perceptions of needs vary by role is needed. This would facilitate the development of effective and tailored health promotion programs that best align with all stated needs (Jo et al., 2010; Whitt-Glover et al., 2014). Therefore, using core CBPR principles as a guiding framework (e.g., community as a unit of identity, diverse perspectives), the purpose of this study was to examine and compare the perceived importance of needs between church leaders and members.
Method
Data Source
This study was a secondary cross-sectional analysis of data collected between February 2019 and January 2020 using the Mid-South Congregational Health Survey (MSCHS). The CBPR approach guiding the MSCHS development process was described previously (Harmon, San Diego, et al., 2021). In brief, the MSCHS is a health needs assessment tool developed through a community, health care, and research collaboration, designed to assess individual, social, and environmental health-related needs of churches served by two congregational networks in the Mid-South (e.g., North Mississippi, East Arkansas, West Corner of Tennessee). The University of Memphis and Appalachian State University Institutional Review Boards (IRB) approved the University of Tennessee Health Science Center as the IRB of record.
Procedure
Implementation staff met with church leadership (e.g., pastor or church liaison), explained the purpose of the study, assessed the church’s readiness to participate, and obtained approval for churches to participate in the study (Harmon, San Diego, et al., 2021). Once approval was obtained, implementation staff worked with each church liaison to determine the process for survey administration and strategies to facilitate participant recruitment. Church liaisons were previously established contacts within the churches who worked with network staff on health-related initiatives. These individuals were members of the congregation, but most often a formal or informal congregation leader (e.g., health ministry leader, pastor, and pastor’s spouse). Each church liaison used recruitment strategies appropriate for their congregation (i.e., word of mouth, informal conversations, announcements before service, and emails), and each sample included at least one church leader (Harmon, San Diego, et al., 2021). To reduce unequal representation from larger churches (>350–1,000 members), when data across churches were combined and to make data collection feasible for network staff, 1% of congregations were recruited from each church, with a minimum of five participants and a maximum of 30 participants per church, to complete the survey (Harmon, San Diego, et al., 2021). Given the small sample size, purposive sampling was used to enhance diversity in perspectives and ensure survey results were representative of members of each congregation (Harmon, San Diego, et al., 2021). Eligibility criteria included being a church leader or member, at least 18 years old, and able to write, read, and comprehend English.
Measures
Demographic information on congregation members who completed the survey included age (the average age of survey participants was 55, which was categorized as <55, ≥55), sex (cis male, cis female), and race/ethnicity (Black/African American, Non-Black/African American). Congregation-specific information was church role (leader [pastor/pastor’s spouse, associate pastor, elder, minister, non-clergy staff, health ministry leader, volunteer leader, parish/faith community nurse]; member) and congregation size (small: ≤ 100 members; medium: 101–350 members; large: ≥ 351 members). Congregation zip codes were categorized based on the Shelby County median income, US$51,657 (United States Census Bureau, 2019; United States Zip Codes, 2021), and were dichotomized as high median income (≥US$51,657) and low median income (<US$51,657).
The MSCHS’s 36-item health index was used to assess respondents’ health-related needs pertaining to the perceived individual (i.e., anxiety or depression, diabetes, and obesity), social (i.e., affordable health care, healthy foods, youth programs), and environmental (i.e., crime, domestic violence, homelessness) needs within their church and the community in which their church resides (Harmon, San Diego, et al., 2021). Within the health index, participants could select as many needs as they wanted (Harmon, San Diego, et al., 2021).
Data Analysis
Four churches oversampled their congregation, and sensitivity analyses were run with and without these outlier churches. For this study, the a priori outcome variables of interest were the 10 most frequently reported needs as indicated using the 36-item health index. The primary predictor variable was church role dichotomized (i.e., church leader and member). Church role categorizations were informed by expert opinion (e.g., MSCHS committee, faith-based researchers) and previous literature (Lumpkins et al., 2013; Williams et al., 2012). Missing church role data (n = 68) were imputed as church members, given each participant was at minimum a member of their respective church.
All analyses were run using SAS Version 9.4. Descriptive statistics were calculated for the predictor variable (church role) and covariates of interest (age, sex, race/ethnicity, education level, congregation size, and congregation zip code). Frequencies were run to identify the top 10 overall health needs. The top 10 overall health needs were then stratified by church role (i.e., church leader and member) and ranked by perceived importance (e.g., percentage of participants who reported the need). Health needs considered to be different in perceived importance between church roles were explored further with statistical testing. Significance level was set at p < .05.
To assess the presence of multicollinearity, correlations among church role, age, sex, race/ethnicity, education level, congregation size, and congregation zip code were examined. Weak to moderate Pearson correlations (<.50) were identified. Although variables were not highly correlated, collinearity diagnostics were run for each adjusted model. No multicollinearities were found, as indicated by tolerance level (> 0.1), and therefore all variables were retained in the model.
Due to the number of participating churches (N >10) and potential clustering within churches, generalized linear mixed models (GLMM) were performed using PROC GLIMMIX with binary distributions and logit links. “Church” was entered as the random effect to control for within-cluster correlations between churches. Intercept-only models, with church entered as the random effect, were run for each self-reported need to calculate intraclass correlations (ICCLogit) and to assess the necessity of controlling for random effects. To note, PROC LOGISTIC was used when models did not converge.
Bivariable GLMM were performed for each self-reported need differing in perceived importance with church role entered as a fixed effect to identify crude odds ratio (OR) estimates. Next, multivariable GLMM were performed to model each self-reported need as a function of church role and covariates of interest (e.g., age, race/ethnicity, sex, education level, congregation size, and congregation zip code). Within church role, multivariable GLMM were examined post hoc to further explore the relationship between the polytomous church role variable (pastor/spouse; associate pastor/elder; non-clergy staff, health ministry leader, volunteer leader, parish/faith community nurse; and church member) and self-reported needs. Church member was set as the reference category.
Results
Ninety-two churches completed 828 surveys (n = 369 church leaders, n = 459 church members). Most participants identified as church members (55%), and the largest percentage of church leaders were non-clergy staff, health ministry leaders, or volunteer leaders/deacons (29%). On average, church leaders and church members were 55.2 (SD = 15.2) and 54.3 (SD = 15.5) years old, respectively. Most church leaders and church members were cis female (63% and 78%), Black/African American (91% and 90%), and had less than a college degree (50% and 66%), respectively. Most church leaders and church members reported attending a church with fewer than 100 members (67% and 70%) in a lower income zip code (70% and 60%), respectively. See Table 1 for detailed descriptive data on the sample.
Descriptive Statistics of Participants Who Completed the MSCHS Stratified by Church Role (N = 828)
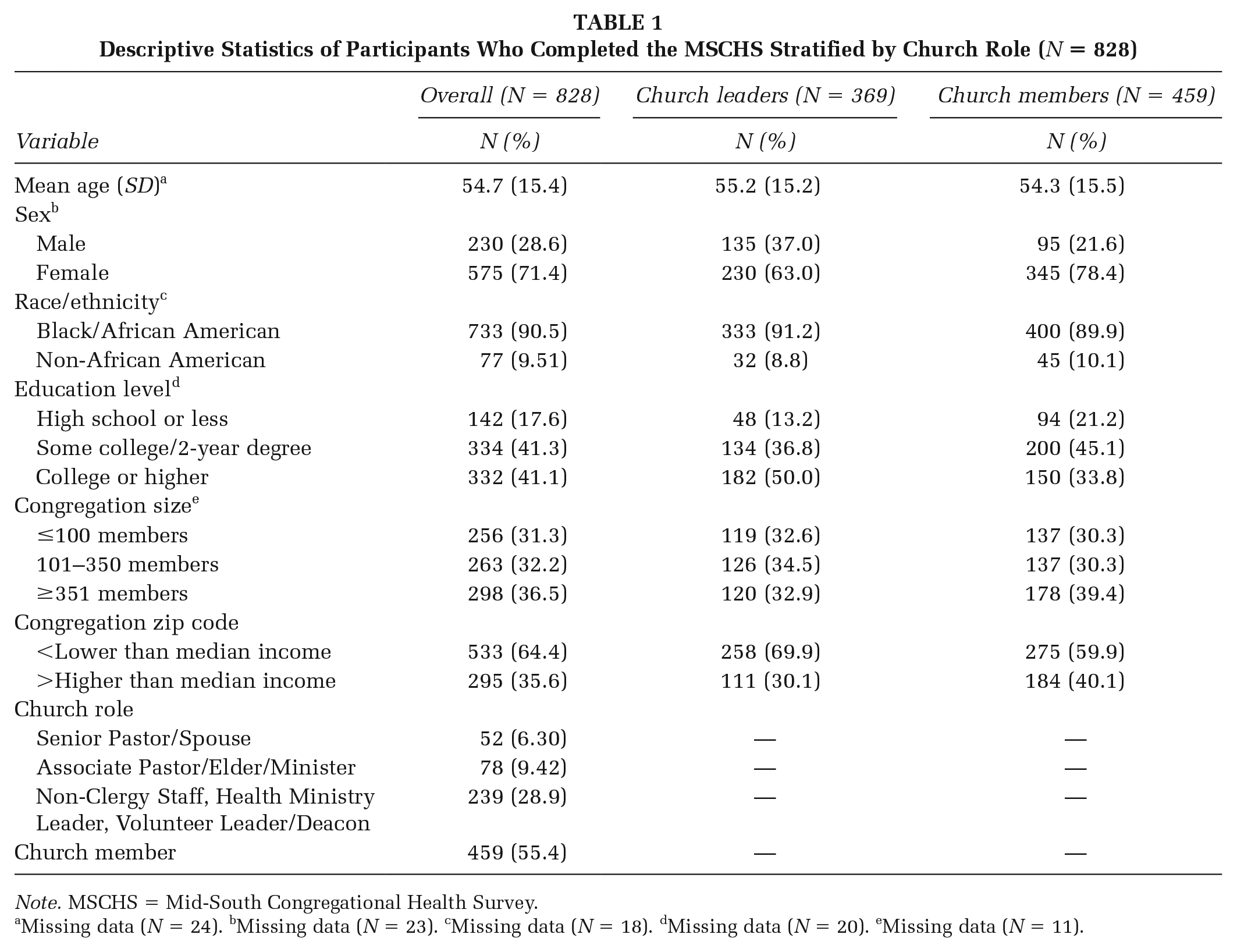
Note. MSCHS = Mid-South Congregational Health Survey.
Missing data (N = 24). bMissing data (N = 23). cMissing data (N = 18). dMissing data (N = 20). eMissing data (N = 11).
Across church leaders and members, the most frequently reported congregational needs were anxiety or depression (65%), high blood pressure (65%), stress (62%), affordable health care (60%), obesity (58%), diabetes (57%), healthy foods (57%), youth programs (57%), heart disease (57%), and neighborhood crime (56%; see Table 2). Of these, anxiety or depression (#1), high blood pressure (#2), stress (#3), and healthy foods (#6) were ranked identically by church leaders and members. Similarly ranked by church leaders and members were youth programs (#7 and #8) and crime (#9 and #7), respectively. Overall, a higher percentage of church leaders, compared with members, reported congregational needs.
Frequencies of the Top 10 Overall Health Needs Ranked by Church Leader and Member (N = 828)
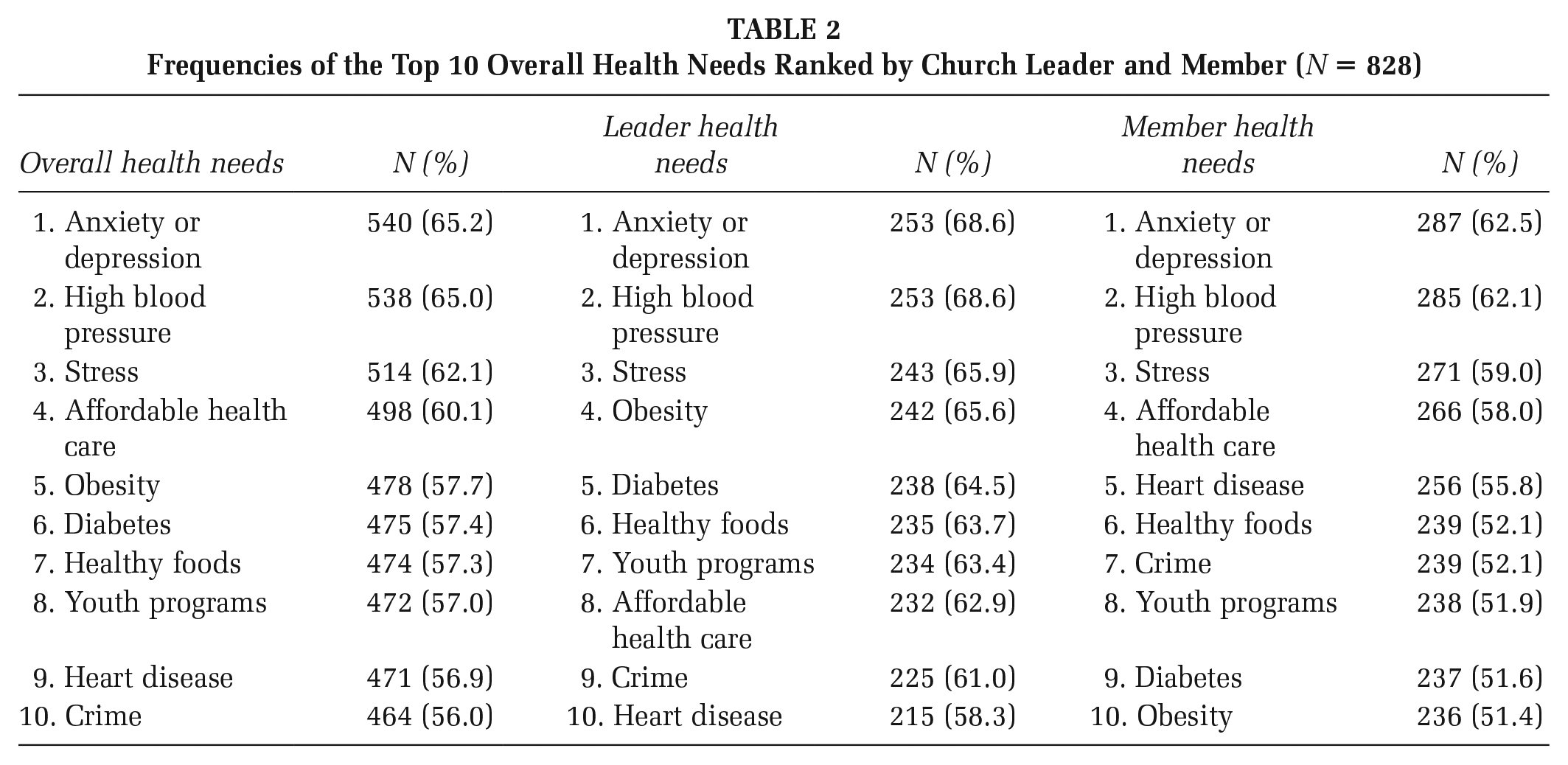
Obesity, diabetes, affordable health care, and heart disease were ranked differently between church leaders and members. Church leaders, compared with members, perceived obesity (#4 vs. #10) and diabetes (#5 vs. #9) to be important congregational health needs, respectively. Members, compared with church leaders, perceived affordable health care (#4 vs. #8) and heart disease (#5 vs. #10) to be important congregational health needs, respectively.
The bivariable and multivariable analyses comparing the reporting of specific health needs for church leaders and members are provided in Table 3. Compared with members, and after controlling for covariates of interest, church leaders were significantly more likely to report obesity as a need (OR: 1.93, 95% confidence interval [CI] = [1.39, 2.67], p = <.0001) and diabetes (OR: 1.73, 95% CI = [1.24, 2.41], p = .001). Bivariable and multivariable analyses indicated members, compared with church leaders, were not significantly more likely to report the needs of affordable health care or heart disease.
Crude and Multivariable Associations Between Church Role and Self-Reported Health Needs Among Adults Who Participated in the Mid-South Congregational Health Survey (N = 828)
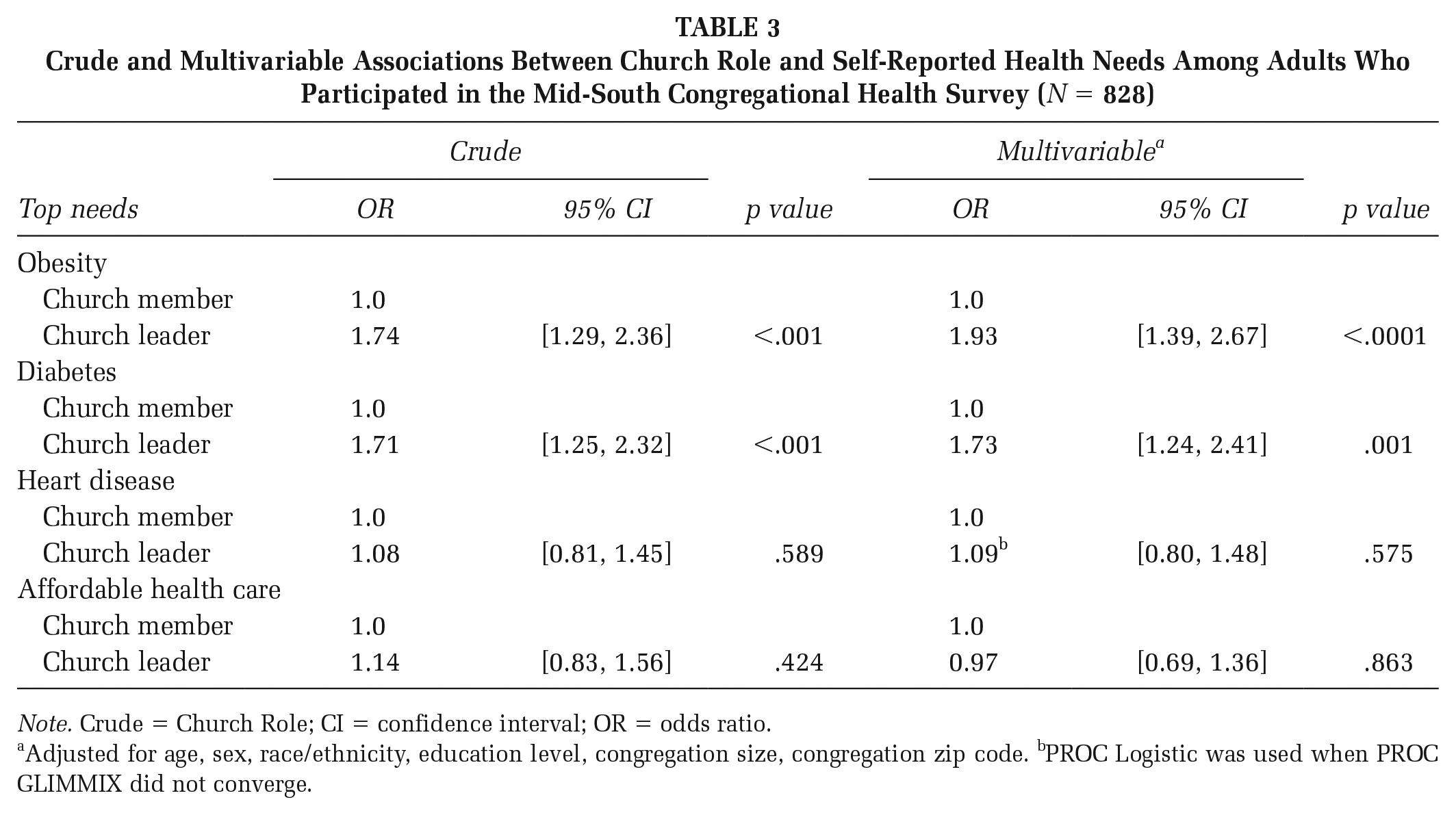
Note. Crude = Church Role; CI = confidence interval; OR = odds ratio.
Adjusted for age, sex, race/ethnicity, education level, congregation size, congregation zip code. bPROC Logistic was used when PROC GLIMMIX did not converge.
Post hoc multivariable analyses revealed non-clergy staff/ health ministry leaders/volunteer leads/deacons, compared with members, were significantly more likely to report obesity (OR: 1.78, 95% CI = [1.24, 2.56], p = .002) and diabetes (OR: 1.93, 95% CI = [1.31, 2.85], p = .001) as a need. Associate pastors/elders, compared with church members, were more likely to report obesity as a need (OR: 2.63, 95% CI = [1.45, 4.77], p = .002). No significant differences were seen in self-reported needs between senior pastor/spouse and church members.
Discussion
This study examined the top 10 overall self-reported needs of the MSCHS and adds to the limited literature examining similarities and differences in the perception of congregational health needs by church role (Williams et al., 2012). Of the 36 needs listed in the health index, the 10 most highly ranked were anxiety or depression, high blood pressure, stress, affordable health care, obesity, diabetes, healthy foods, youth programs, crime, and heart disease. Moreover, the highest ranked needs spanned the individual, social, and environmental contexts. Overall, church leaders and members ranked the top 10 congregational health needs similarly. Still, there were differences in the relative ranking of needs between church leaders (obesity and diabetes) and church members (affordable health care and heart disease). Multivariable analyses, however, revealed church leaders were significantly more likely than members to report obesity and diabetes as congregational health needs, but, among members, no significant associations were seen in reporting heart disease and affordable health care. It is evident that identifying similarities and differences in community or congregational health needs may prove useful for developing evidence-based health promotion programming. Future researchers should utilize mixed methodology (e.g., surveys and interviews) with leaders and members to assess how to properly tailor health promotion programming and address similar and differing need perceptions for each group or the community.
The congregational health needs of anxiety or depression, high blood pressure, and stress were the top three needs regardless of church role. Given the context of the study, data collection, and participant make-up (African American participants, Southern United States), these three needs may have been prioritized due to the average age of participants (e.g., 55 years) or the current racial climate in the United States (e.g., police shootings, health disparities). For example, in a nationally representative study sample of older individuals (N = 3,552), one of the highest reported chronic diseases was high blood pressure (Jih et al., 2018). In addition, previous research suggests discrimination or racism is a determinant of health as it affects health over time (Gee et al., 2012; Paradies et al., 2015). Previous findings show racism or discrimination is associated with poorer mental health outcomes (e.g., depression, anxiety, and stress; Paradies et al., 2015) and potentially physical health outcomes (e.g., hypertension) particularly among African Americans (Forde et al., 2020; Sims et al., 2012). Future MSCHS efforts should employ qualitative methodology (e.g., interviews, focus groups) to aid the development of tailored health promotion programming to address anxiety or depression, high blood pressure, and stress within Southern African American faith communities.
Consistent with study findings, African American church leaders from congregations across the country have identified diabetes and obesity as important congregational needs to be addressed (Lumpkins et al., 2013; Su et al., 2019). In the Mid-South, there is a high prevalence of obesity and diabetes (Jackson et al., 2017), which may be impacting the health of congregations in the Mid-South. The awareness from Mid-South church leaders of the current health status and behaviors in Southern communities may have influenced their reporting of obesity and diabetes. Moreover, Southern cuisine (e.g., potlucks and fried foods) is considered communal in faith communities and may be contributing to obesity and diabetes outcomes seen in the Mid-South (Cline & Ferraro, 2006). Future health promotion efforts should continue to work alongside church leaders and members to address obesity and diabetes within congregations.
Post hoc analyses indicate differences in the ranking of needs for lay leaders (e.g., health ministry leader, non-clergy staff) and associate pastors/elders versus members, suggesting the perceived importance of needs may also differ within leadership. This finding may be influenced by the notion that lay leaders or associate pastors may only work with a subset of the congregation (e.g., health ministry), further narrowing their view of pressing congregational health needs. Senior pastors, in this study, may have been more aligned with members’ need perception due to their overall engagement in the congregation and community (e.g., community resource connector; Harmon, Schmidt, et al., 2021). While previous studies have sought input mostly from senior or associate pastors (Lumpkins et al., 2013; Su et al., 2019), the current study had a small representation of senior pastors/spouses (n = 39) and a large representation of lay leaders (n = 239). The small representation of senior pastors may have been influenced by their role in this study rather than solely participating in the survey (e.g., delegating the survey to their congregations). Future studies would benefit from equal representation and a wide array of church leaders (e.g., senior pastors, associate pastors, and lay leaders), which may allow for a better comparison on how need perceptions compare within leadership.
Strengths
This study has several strengths. This study extended the work of the long-term CBPR partnership between the university and the community. In addition, this is one of the first studies to assess the perceived needs of church leaders and members simultaneously and highlight the differences and similarities of their perceptions. This study also used the MSCHS, which includes a comprehensive list of needs for participants to choose from providing a broad picture of congregational health needs. Furthermore, previous CHNAs were descriptive in nature; we built onto these efforts by conducting mixed modeling of 10 health needs and controlling for demographic differences and church clustering, which allowed for a more robust analysis of perceived needs between church leaders and members. Finally, this study included a wide range of church leadership (e.g., senior pastors and lay leaders), which allowed for greater insight of congregation health needs.
Limitations
Despite our findings and study strengths, this study is not without limitations. Data were cross-sectional, which limits our ability to make causal inferences. With that said, we were able to determine some associations between church role and health needs. Church samples were small and limited to congregations in the greater Memphis, TN area, which limits the generalizability of our findings. Although findings may not be generalizable to the entire United States, there may be other Southern cities that are able to use these findings to better understand the health needs of their congregations. Data also were self-reported, which may have led participants to report socially desirable responses. However, we ensured participants of confidentiality including that individual responses would be unknown to church leadership in our informed consent process to minimize this. In this study, church leaders and members were examined across the dataset and not grouped by the congregation, which limits our ability to interpret how needs differed between church leaders and members across congregations. Although church role categorizations were derived from the literature and expert opinion, these definitions still need to be examined. Future work classifying church leaders or members should consider assessing how different faith communities (e.g., Baptist, United Methodist, COGIC) define church roles (e.g., leader vs. member) within their congregations. Of note, these data were collected before the COVID-19 pandemic, which may have influenced or even worsened prepandemic perceived health needs (e.g., mental health). For example, the literature suggests mental health conditions, such as symptoms of anxiety or depressive disorders, increased during the COVID-19 pandemic (Czeisler et al., 2020; Vahratian et al., 2021). Thus, reassessing the health needs of Mid-South congregations might be a necessary step before developing health promotion programming aimed at addressing identified needs.
Implications for Practice
Churches remain a cornerstone in African American communities. Therefore, listening to the priorities of church leaders and congregants may be one way to reduce health disparities in the Mid-South and beyond. Congregational health needs assessments, specifically, can be used as a tool to invite these voices to the conversation. Findings from this study provide additional evidence of similar and differing need perceptions between church leaders and members. To build on our work, we recommend future researchers conducting congregational health needs assessments to continue assessing and evaluating the perspectives of both church leaders and members. We also recommend church leaders and members collaborate in action planning to set goals and identify ways to address needs identified within their congregation (Huey et al., 2022). To effectively design health promotion programs aimed at health needs and solutions identified by the congregation, however, we recommend academic partners work with congregational representatives (e.g., pastor, member, and lay leader) from their respective churches. For example, academic partners may provide evidence-based models and congregational representatives may provide culturally and spiritually sensitive knowledge to ensure health promotion programming aimed at addressing health needs is faith-based and not faith-placed (Campbell et al., 2007; Goldmon & Roberson, 2004). Overall, continued work understanding the perceived needs of both church leaders and members helps to inform the development of tailored health promotion programs that address the breadth of congregational concerns.
Footnotes
Authors’ Note:
We would like to acknowledge leaders and congregations who participated in the MSCHS. The authors thank Methodist Le Bonheur’s Congregational Health Network navigators (Donna Spencer, Jennifer Garrott, Lorie Ingram, Russell Belisle, Sheila Easterling), Lauren Hales at Church Health, and Church Health’s Congregational Health Promoters Steering committee for their contributions. Dr. San Diego was supported in part by grants UL1 TR002550 and KL2 TR002552 from the National Center for Advancing Translational Sciences, National Institutes of Health.