
Abstract
Objectives:
COVID-19 vaccines are widely available, but uptake is suboptimal. To develop strategies to increase vaccination rates, we sought to (1) characterize adults initially hesitant to be vaccinated for COVID-19 who later received the vaccine and (2) identify factors associated with their vaccination decision.
Methods:
In January 2021, we conducted an online survey of US adults via Prolific that assessed vaccination intent, COVID-19–related knowledge and attitudes, and demographic characteristics. In May 2021, we recontacted respondents to assess vaccination status and factors influencing their vaccination decision. We used χ2 statistics and t tests to examine associations between respondents’ vaccination status and their characteristics, knowledge, and attitudes. We analyzed reasons for vaccination using thematic analysis.
Results:
Of 756 initially vaccine-hesitant respondents, 529 (70.0%) completed the follow-up survey. Nearly half of those initially not sure about vaccination (47.3%, 112 of 237) were vaccinated at follow-up, while 21.2% (62 of 292) of those initially planning not to be vaccinated were vaccinated at follow-up. Of those initially not sure, higher educational attainment, greater knowledge of COVID-19, and a doctor’s recommendation were associated with vaccination. Of those initially intending not to be vaccinated, male sex, Democratic political affiliation, receipt of an influenza shot within 5 years, being more worried about COVID-19, and having greater COVID-19 knowledge were associated with increased likelihood of being vaccinated. Of 167 respondents who gave reasons for vaccination, protecting oneself and others (59.9%), practical issues (29.9%), social influences (17.4%), and vaccine safety (13.8%) were the main reasons.
Conclusion:
Providing information on the protective value of vaccination, implementing rules that make remaining unvaccinated burdensome, making vaccination easy, and providing social support may influence vaccine-hesitant adults to accept vaccination.
The COVID-19 pandemic has resulted in more than 1.1 million deaths in the United States as of March 2023. 1 COVID-19 vaccines have been widely available for adults in the United States since April 2021, with well-established safety and efficacy.2-5 Although COVID-19 vaccination protects against infection and severe outcomes, such as hospitalization and death,6-8 vaccine uptake is suboptimal. 9
Vaccine hesitancy has been defined as a “delay in acceptance or refusal of vaccines despite availability of vaccine services.” 10 Numerous surveys have examined COVID-19 vaccine hesitancy. 11 In the United States, lower educational attainment, Black race, younger age, female sex, and Republican political affiliation are associated with increased likelihood of reporting vaccine hesitancy, although these associations vary by survey.12-16 Reasons for COVID-19 vaccine hesitancy include concerns about vaccine safety and side effects, distrust of the development process, the “newness” of the vaccine, and beliefs about risk and disease severity.12,14-17
While research into predictors of COVID-19 vaccine hesitancy has burgeoned, far less research has been conducted on factors that influence initially hesitant individuals to accept vaccination. One study found that fewer than 1 in 10 vaccine-hesitant respondents had been vaccinated 2 to 3 months later, 18 while another study reported that approximately 1 in 3 initially hesitant adults were vaccinated for COVID-19 approximately 3 to 6 months later. 19 Neither study explored why vaccine-hesitant individuals ultimately accepted vaccination, nor did they explore associations with degree of vaccine hesitancy. The Kaiser Family Foundation (KFF) surveyed US adults in January 2021 and conducted a follow-up survey 6 months later but did not compare those who were vaccinated at follow-up with those who were not vaccinated at follow-up. 20 A better understanding of whether, how, and why willingness to accept vaccination changes over time is needed.
Our objective was to assess the relationship between COVID-19 vaccine hesitancy in January 2021, just as the vaccines were becoming available in the United States, and vaccination status approximately 5 months later, when COVID-19 vaccines were widely available. We characterized people who were initially vaccine hesitant but were later vaccinated and identified the factors associated with vaccine acceptance.
Methods
In January 2021, we recruited participants via Prolific Academic Ltd (https://prolific.co), an online research platform. The questionnaire was available in English to adults residing in the United States. We restricted the sample to panel members who had identified as White, Black, or Hispanic, and we oversampled those who identified as Black or Hispanic because members of these groups had been identified as more likely to be vaccine hesitant than those from other racial and ethnic groups.12,21
The initial survey, programmed in REDCap,22,23 was open from January 12 through February 1, 2021, when we achieved our target sample size of approximately 1800 respondents.
In May 2021, we recontacted respondents to the initial survey. After excluding participants who reported already being vaccinated in January, we invited 1688 participants for the follow-up survey, which was open from May 27 through July 8. Nonrespondents received email reminders every 2 days. Respondents received $1.50 for each survey.
Questionnaire Items
The initial survey assessed vaccination intent with the following question: “If you could get vaccinated for COVID-19 today, would you?” Response options were “yes,” “no,” “not sure,” and “already vaccinated.” Those responding “no” or “not sure” were categorized as vaccine hesitant. Other items on the initial survey assessed COVID-19 knowledge (assessed by 7 true/false statements developed by the study team), beliefs, and attitudes about COVID-19 (eg, worry about getting COVID-19) and the COVID-19 vaccine, and respondent characteristics (age, sex, race and ethnicity, education, marital status, region of residence, political affiliation, employment status, self-rated mental or emotional health, influenza shot in the past 5 years).
Questions on the follow-up survey were tailored to vaccination intent as reported on the initial survey. We assessed vaccination status with 1 question: “Have you been vaccinated against COVID-19?” Response options were “yes” or “no.” A recent study found that self-report of COVID-19 vaccination is a valid metric of vaccination status. 19 Respondents were asked about factors that may have influenced their vaccination decision. Unvaccinated respondents were asked about their desire to be vaccinated, barriers to vaccination, and reasons for not being vaccinated. Vaccinated respondents were asked an open-ended question, “What made you decide to get vaccinated?” This question was followed by a set of items introduced with the question, “To what extent, if any, did each of the following affect your decision to be vaccinated?” Nine potential factors were provided (eg, a conversation with a friend or family member, wanting to protect the people around them). Response options were “not at all,” “a little,” “somewhat,” and “very much.” Other items on the follow-up survey assessed whether respondents had a conversation with a doctor about the COVID-19 vaccine and had a history of COVID-19. A small number of demographic items (political affiliation, financial stress) were included on the follow-up survey (eTable 1 in Supplemental Material).
Analyses
The analytic sample included respondents who responded “no” or “not sure” in January 2021 to the item assessing vaccination intent and responded to the follow-up survey. We described participant characteristics and responses by using frequencies and percentages. We used cross-tabulations and Pearson χ2 tests to examine the unadjusted bivariate association between vaccination intent and participant characteristics and experiences on the initial survey, with vaccination status as reported on the follow-up survey. We used t tests to examine differences in COVID-19–related knowledge as assessed on the initial survey by vaccination status at follow-up. We constructed separate multivariable logistic regression models according to extent of initial vaccine hesitancy (no or not sure). We selected independent variables that are known to be associated with vaccine hesitancy (eg, education, political affiliation, receipt of the influenza shot) and variables that we hypothesized would be associated with accepting vaccination (eg, doctor recommendation, history of COVID-19, worry about COVID-19, COVID-19 knowledge). We also included demographic variables (age, sex, race and ethnicity). In supplemental analyses, we used Pearson χ2 tests to examine the association between reason for vaccine hesitancy at the time of the initial survey and vaccination status at follow-up. Stratifying by baseline initial hesitation (“no” or “not sure”), we conducted bivariate analyses using SPSS version 28.0 (IBM Corp), and we conducted multivariable analyses using SAS version 9.4 (SAS Institute, Inc). The latter analyses included all predictors with P < .10 for either initial stratum and key sociodemographic variables.
We used thematic analysis to characterize responses to the open-ended question, “What made you decide to get vaccinated?” Four team members (K.A.F., K.M.M., R.W., M.D.) generated an initial coding scheme and then revised it through iterative application and discussion. Our analysis was informed by the major concepts of the increasing vaccination model, 24 which groups factors that may influence vaccination into those that affect what people think and feel, social processes, and practical issues. However, we were not limited by these constructs and prioritized capturing the meaning apparent in the responses in defining codes and overarching themes. When codes were finalized, 2 analysts (M.D., R.W.) independently coded all responses. Coders discussed coding discrepancies with an investigator with extensive qualitative experience (K.A.F.), who adjudicated any disagreements. Codes were applied in Microsoft Excel and then merged into SPSS version 28.0 (IBM Corp) to facilitate manipulation and summarization.
The UMass Chan Medical School Institutional Review Board reviewed and approved this study and deemed it exempt from further institutional review board review (approval number H00022244) because the identity of the human subjects cannot be readily ascertained. Respondents provided online written informed consent.
Results
A total of 756 respondents to the initial survey did not intend to get vaccinated or were not sure whether they would get vaccinated, 529 (70.0%) of whom completed the follow-up survey and were included in the analytic sample. Overall, 32.9% (174 of 529) of those initially vaccine hesitant reported they had been vaccinated at follow-up. Of those who had received a vaccine that required a second dose (n = 150), most had received a second dose (n = 117, 78.0%) or reported that their second appointment was pending (n = 31, 20.7%); 2 respondents had missed their second dose. Of the 355 initially vaccine-hesitant respondents not vaccinated at follow-up, 45 (12.7%) indicated a desire to be vaccinated, 141 (39.7%) were not sure whether they would be vaccinated, and 169 (47.6%) did not want to be vaccinated.
The extent of vaccine hesitancy expressed on the initial survey was strongly associated with vaccination status at follow-up. Of 237 respondents who were initially not sure about vaccination, 112 (47.3%) had been vaccinated at follow-up; only 62 of 292 (21.2%) respondents who initially intended not to be vaccinated had been vaccinated at follow-up (P < .001). Concerns that the vaccine might not be safe and that vaccine development was too rushed were the most common reasons for vaccine hesitancy provided on the initial survey, among both respondents who were initially not sure about or said no to vaccination. More respondents who initially said no to vaccination (43 of 292; 14.7%) cited not trusting the vaccine as the main reason for their hesitancy than respondents who initially indicated being not sure (10 of 237; 4.2%). Of initially “no” respondents whose main reason for being hesitant was not trusting the vaccine, most (41 of 43; 95.3%) remained unvaccinated at the follow-up survey (eTable 3 in Supplemental Material).
Analyses of bivariate associations between vaccine receipt and selected characteristics among respondents who were initially not sure about vaccination found 3 significant associations: respondents with ≤high school diploma were less likely to report being vaccinated than respondents with ≥4-year college degree (33.8% vs 64.2%; P = .004), respondents who had a conversation with their doctor and received a recommendation for the vaccine were more likely to get vaccinated than respondents who did not receive a recommendation (59.0% vs 12.5%; P = .048), and those who had been vaccinated had higher COVID-19 knowledge scores than those who had not been vaccinated (mean score, 5.3 vs 5.0; P = .04) (Table 1). In bivariate analyses of those who were initially most hesitant, men were significantly more likely than women (28.2% vs 16.9%; P = .02), Democrats were significantly more likely than Republicans or Independents (34.0%, 11.7%, and 13.4%, respectively; P < .001), those who reported receipt of an influenza shot in the prior 5 years were more likely than those who had not had or were unsure whether they had had an influenza shot (33.3% vs 14.4%; P < .001), and those who were more worried about COVID-19 were significantly more likely than those who were less worried about COVID-19 (31.8% vs 16.7%; P = .004) to be vaccinated. Those who were vaccinated had significantly higher COVID-19 knowledge scores than those who were not vaccinated (mean score, 5.0 vs 4.3; P = .007).
Characteristics of respondents to a survey of US adults conducted in 2021 on COVID-19 vaccination intent, by initial vaccination intent and COVID-19 vaccination status, United States
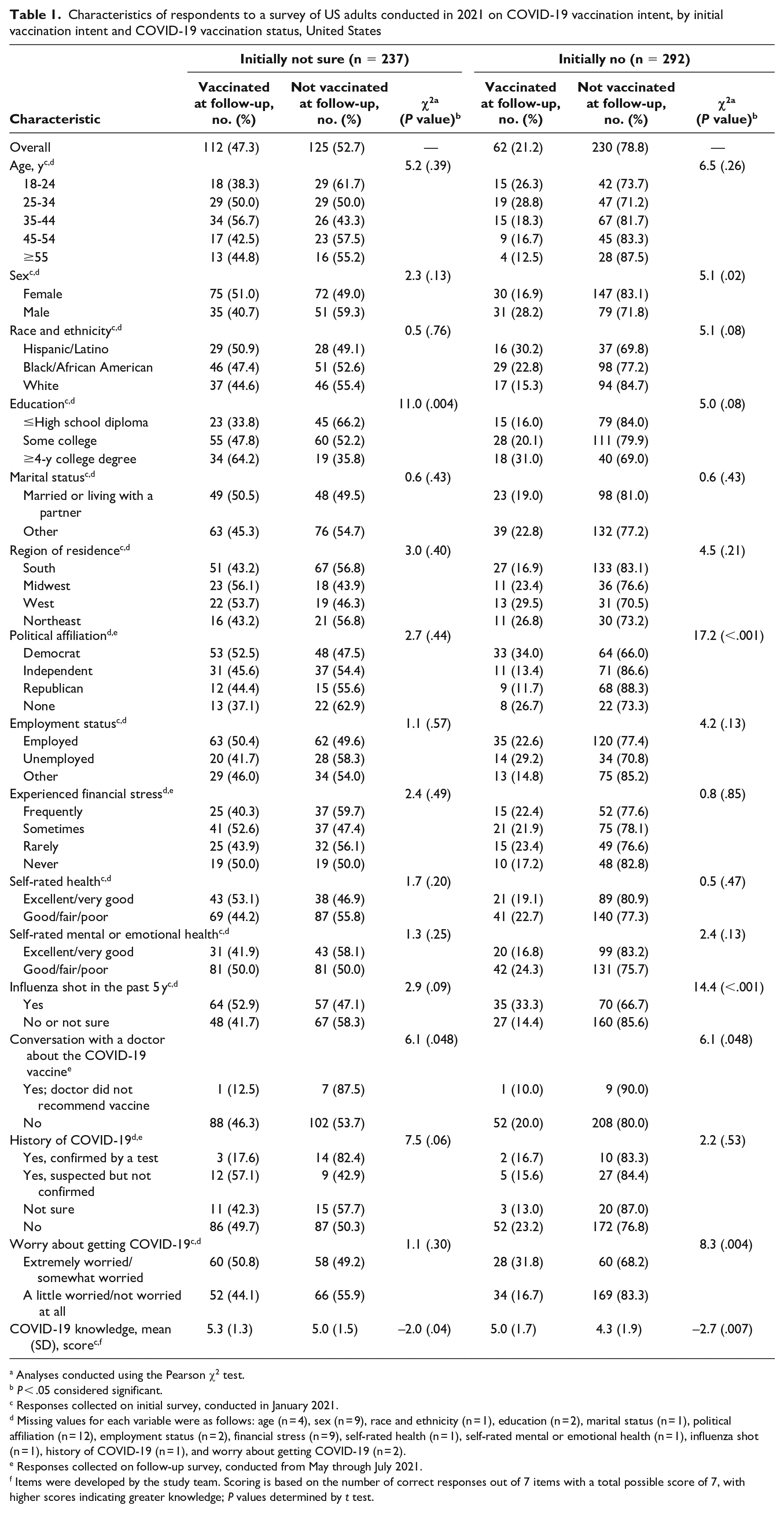
Analyses conducted using the Pearson χ2 test.
P < .05 considered significant.
Responses collected on initial survey, conducted in January 2021.
Missing values for each variable were as follows: age (n = 4), sex (n = 9), race and ethnicity (n = 1), education (n = 2), marital status (n = 1), political affiliation (n = 12), employment status (n = 2), financial stress (n = 9), self-rated health (n = 1), self-rated mental or emotional health (n = 1), influenza shot (n = 1), history of COVID-19 (n = 1), and worry about getting COVID-19 (n = 2).
Responses collected on follow-up survey, conducted from May through July 2021.
Items were developed by the study team. Scoring is based on the number of correct responses out of 7 items with a total possible score of 7, with higher scores indicating greater knowledge; P values determined by t test.
The results of the multivariable models were generally consistent with the bivariate analyses, although associations were attenuated (eTable 2 in Supplemental Material). Among initially “not sure” respondents, having ≤high school diploma, having a conversation with a doctor about the COVID-19 vaccine and not receiving a recommendation, and having a history of COVID-19 that was confirmed by a test were associated with a decreased likelihood of being vaccinated at follow-up. Among initially “no” respondents, being female and not getting an influenza shot in the past 5 years were associated with a decreased likelihood of being vaccinated at follow-up. Identifying as a Democrat or as having no political affiliation and scoring higher on the COVID-19 knowledge items were associated with an increased likelihood of being vaccinated at follow-up.
Most respondents (n = 99, 57.2%) reported that the desire to protect others “very much” influenced their decision about vaccination (Table 2). Other factors rated as very influential by at least one-quarter of respondents were anticipation of vaccination requirements (31.6%), worry about getting COVID-19 (28.9%), and conversations with friends and family (26.4%). Becoming convinced that the vaccine was safe was rated very influential by about 1 in 5 of those who were initially not sure and only about 1 in 10 of those initially not intending to be vaccinated, despite being the most common reason for being COVID-19 vaccine hesitant at the time of the initial survey (eTable 3 in Supplemental Material). Among respondents who cited vaccine safety as the main reason for their hesitancy and were vaccinated at the time of the follow-up survey (n = 60), only 9 (15.0%) indicated that being convinced of vaccine safety “very much” influenced them to get vaccinated. Only 19 (10.9%) respondents indicated a conversation with a doctor was very influential. Only 79 (14.9%) respondents had had such a conversation with a doctor (Table 1).
Factors “very much” influencing respondents’ decision to be vaccinated against COVID-19 in a survey of US adults conducted from May through July 2021, United States
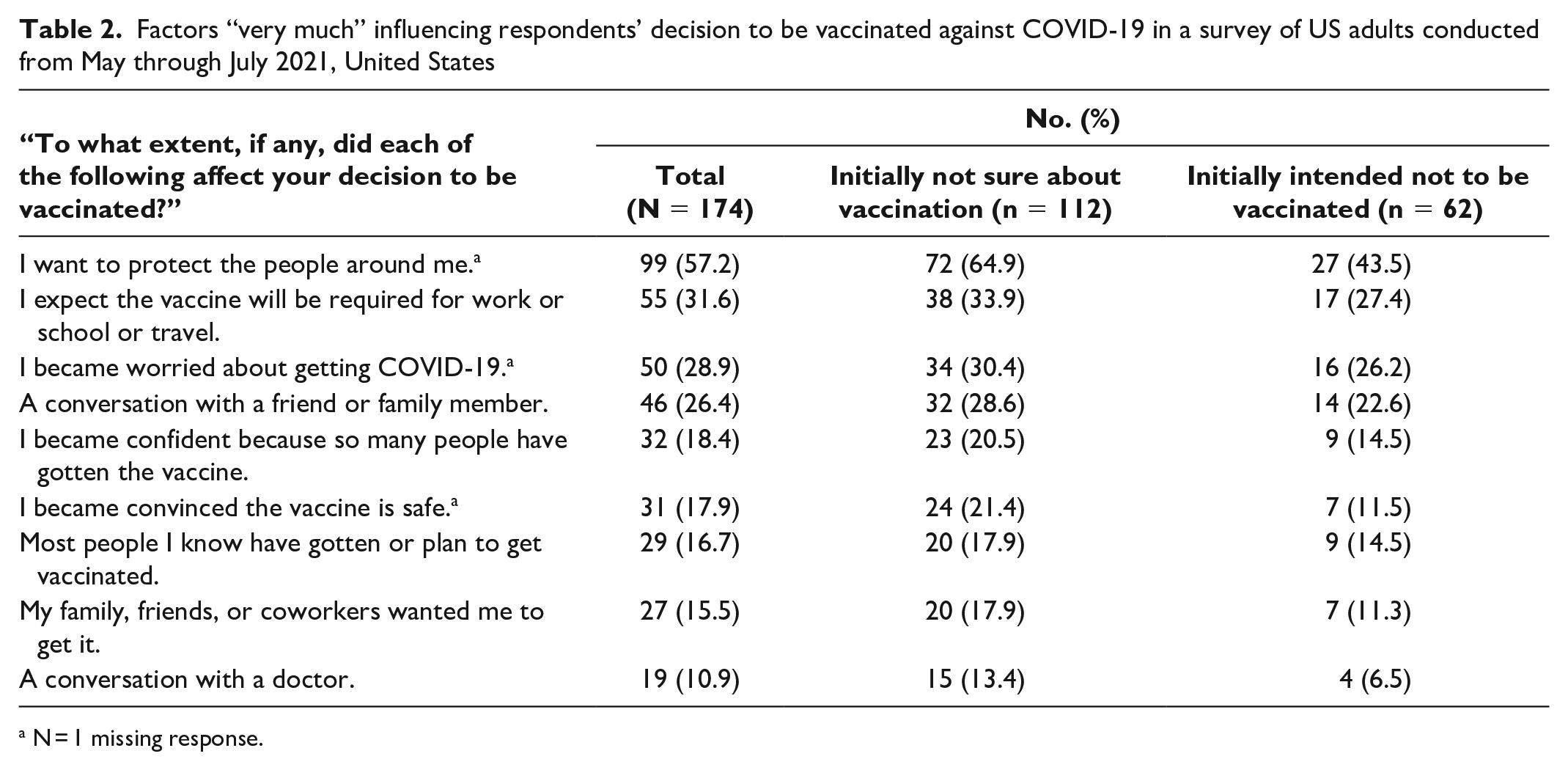
N = 1 missing response.
Of 174 respondents who reported having been vaccinated, 167 (96.0%) provided a reason (Table 3). Four overarching themes emerged from the analysis: protect self and others, practical issues and impact on life, social influences, and perception of vaccine safety. The theme “protect self and others” was most prevalent overall and within each level of initial vaccine hesitancy and included reference to perceiving oneself to be at risk of COVID-19 infection because of reopenings of schools, places of business, and other public venues or decreased compliance with social distancing or wearing face masks. Practical issues and impact on life were cited by nearly one-third of vaccinated respondents. Many comments that were coded referred to a desire to return to normal as well as convenient and easy vaccine access. Some respondents accepted an impromptu offer of a vaccine while shopping. Other comments referenced rules or mandates (actual or anticipated) that required vaccination or added testing requirements for the unvaccinated. Social influences, including both active efforts to influence the respondent (eg, a family member’s request, a doctor’s recommendation) and a general perception that vaccination is common, were referenced by about one-quarter of vaccinated respondents. References to changes in respondents’ perceptions of vaccine safety were relatively infrequent.
Reasons for getting vaccinated against COVID-19, among respondents who were hesitant to be vaccinated on an initial survey conducted in January 2021 and vaccinated at the time of a follow-up survey conducted from May through July 2021, United States
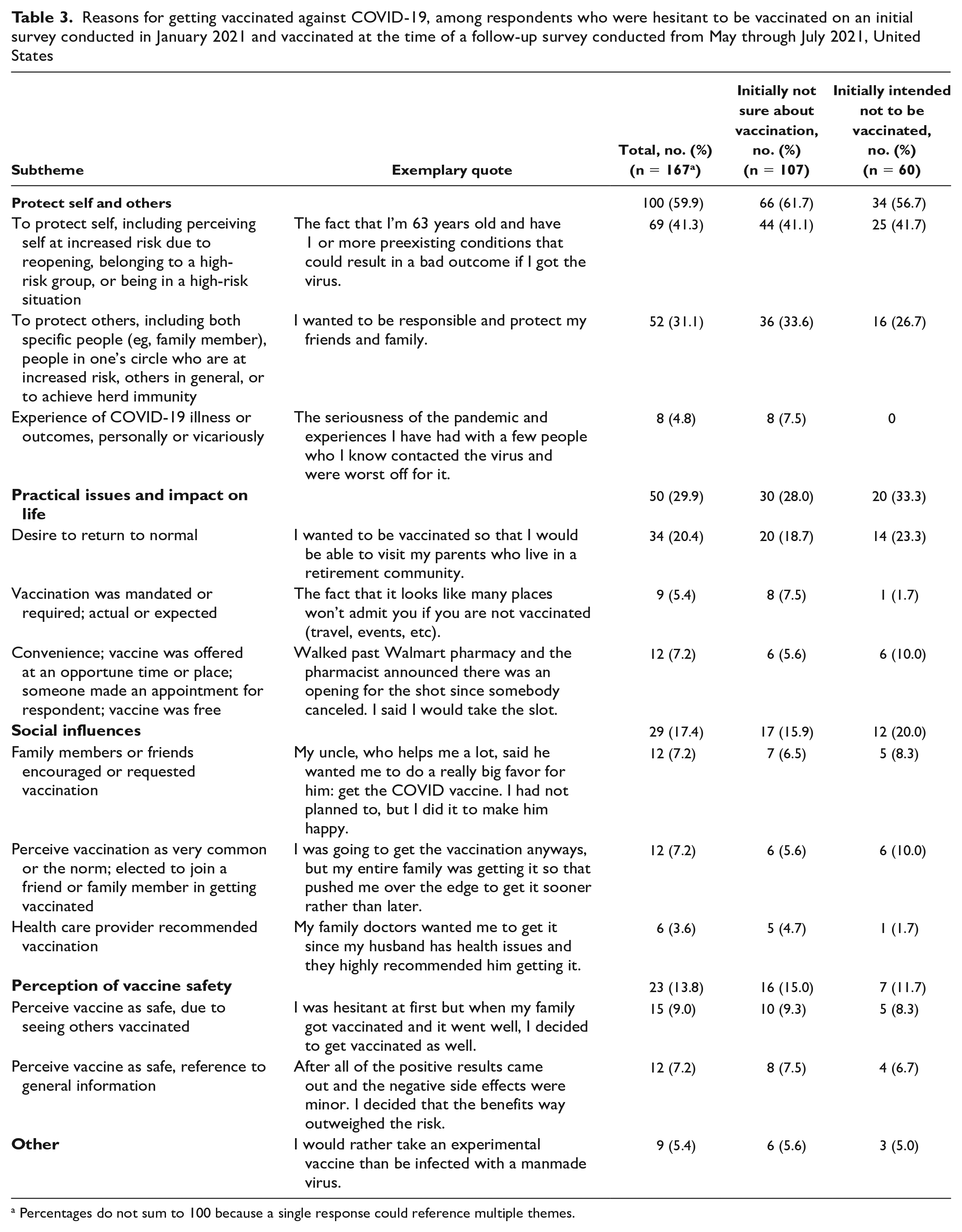
Percentages do not sum to 100 because a single response could reference multiple themes.
Discussion
Overall, about 1 in 3 participants in this study, all of whom were hesitant about the COVID-19 vaccine in January, were vaccinated at the time of the follow-up survey approximately 5 months later. The percentage of vaccination was higher among respondents who were initially not sure about vaccination than among those who initially planned not to be vaccinated. While differences in survey timing, samples, and items make it difficult to directly compare our results with the results of other studies, our findings are generally consistent with Siegler et al, 19 who reported that about 1 in 3 initially vaccine-hesitant respondents were later vaccinated, and the KFF poll, 20 which reported that about 1 in 2 of those who were somewhat hesitant were later vaccinated and only 1 in 4 of the most strongly hesitant respondents were later vaccinated. It appears that vaccine hesitancy is mutable, and that even those who are firmly opposed to being vaccinated at one time may ultimately accept a vaccine.
The desire to protect oneself and others and being worried about COVID-19 had a positive influence on vaccination. Such influences could be conceptualized under “what people think and feel” in the increasing vaccination model described by Brewer et al 24 and are consistent with the results of the KFF poll, which identified “to protect myself/reduce risk” as the top reason people had been vaccinated. 20 Our results provide insight into experiences that may have made these considerations prominent, causing people to move from hesitancy to acceptance. Specifically, the relaxing of social distancing and wearing face masks increased perceived risk for some, and direct experience with people who had become very ill with COVID-19 caused others to recognize the seriousness of the disease.
Fewer than 1 in 5 vaccinated participants referred to vaccine safety as influencing their decision to be vaccinated; concerns about vaccine safety have been among the most commonly cited reasons for not being vaccinated in other studies.12,21 One possible explanation for this finding is that while some participants came to view vaccines as safe, others simply shifted their attention from the issue of safety to other considerations, such as the desire to return to normal or to avoid looming restrictions. Some respondents explicitly acknowledged that they had been vaccinated despite persistent concerns about safety.
Our findings on the importance of practical issues and impact on life relate to the concept of “direct behavior change” in the increasing vaccination model, or “practical influences” in the World Health Organization adaptation of this model. 25 It is not surprising that many respondents desired a return to normal and were willing to be vaccinated to achieve that or that convenient access to vaccines was important. Less expected responses were those in which respondents accepted an impromptu offer of vaccination, suggesting that situations that discourage deliberation may be helpful for some people. This finding also suggests that offering vaccinations at multiple locations to provide many opportunities for vaccination may be helpful.
Our findings confirm that social factors influence vaccination. Some respondents were influenced by the perception that getting vaccinated for COVID-19 is normative, socially desirable behavior, consistent with the “social processes” concept in the increasing vaccination model. Conversations with friends and family members, including explicit requests or encouragement, led to vaccination for some respondents. Some respondents agreed to get vaccinated in partnership with a friend or family member. These findings are consistent with findings from the KFF poll, which also identified social factors as important influences. 20 Our results provide further evidence of the importance of a health care provider’s recommendation in promoting vaccination.
Overall, our findings reveal that for some initially vaccine-hesitant respondents, the decision to get vaccinated resulted from a shift in focus and in the relative weight assigned to certain considerations, rather than from correction of misinformation or a new belief in vaccine safety. We posit that circumstances, conversations, exposure to specific information, or other experiences may have differentially activated cognitions that favored vaccination (eg, a desire to keep oneself and others safe and return to a normal life), without changing other, previously dominant cognitions (eg, beliefs about the dangers of vaccination). Overall, correction of misinformation appears not to have been the lever that moved these respondents from vaccine hesitancy to vaccine acceptance. Some respondents’ comments suggest they moved from vaccine hesitancy to acceptance but still lacked confidence in the vaccine.
Based on these findings and supported by other studies, we offer recommendations that may help increase the uptake of COVID-19 vaccination among hesitant adults. First, we recommend that vaccine promotion messages include explicit and accurate information on the value of vaccines in protecting oneself and others. 26 Second, we recommend continuing vaccine mandates and rules that make remaining unvaccinated burdensome.27,28 Third, we recommend that vaccine promotion efforts leverage the social environment—both actual and virtual—to amplify messages about the prevalence of vaccination, conveying that millions of people have been vaccinated and have not had lasting adverse effects. People who have been vaccinated may be best positioned to encourage the people they care about to get vaccinated. We suspect personal requests will be most effective if framed as a favor rather than as a demand. 29 We also suggest making vaccination a social event, where friends or family members get vaccinated together. Fourth, we recommend continuing efforts to make getting vaccinated easy and convenient, ideally adding opportunities for spontaneous, spur-of-the-moment acceptance. Making vaccination widely available at physician offices could be an effective way of achieving greater vaccine uptake because it would allow for impromptu acceptance in combination with the proven social influence of a physician recommendation. 30 Excellent recommendations for increasing COVID-19 vaccine confidence and acceptance exist31,32; we hope our recommendations will contribute to these efforts.
Limitations
This study had several limitations. First, our findings were based on responses from people who were hesitant to be vaccinated for COVID-19 as the vaccine was first becoming widely available in the United States, in January 2021, and were vaccinated by early summer of that year. We do not know whether the factors that influenced these respondents were the same factors that might influence those who had still declined to be vaccinated, as the latter would likely be more resistant. Second, our study may have been underpowered to identify influences with smaller effect sizes. Third, our findings do not shed light on the current problem of low rates of COVID-19 booster uptake, which might be related to low levels of awareness, pandemic fatigue, inertia, and the potential that individuals may become vaccine hesitant even after accepting primary vaccination. Fourth, our findings were limited by the extent to which respondents have insight into the factors that influence their vaccination decision and are willing to report honestly on those insights. Lastly, these findings were limited by the extent to which respondents had exposure to specific potential influences, such as a conversation with a physician.
Conclusions
This study provides evidence that vaccine hesitancy is mutable, and those who are opposed to being vaccinated at one time may later become vaccinated. Accurate information on the protective value of vaccines, rules and mandates that make remaining unvaccinated burdensome, easy access, and social support may all contribute to moving vaccine-hesitant people toward vaccine acceptance.
Supplemental Material
sj-docx-1-phr-10.1177_00333549231176006 – Supplemental material for From COVID-19 Vaccine Hesitancy to Vaccine Acceptance: Results of a Longitudinal Survey
Supplemental material, sj-docx-1-phr-10.1177_00333549231176006 for From COVID-19 Vaccine Hesitancy to Vaccine Acceptance: Results of a Longitudinal Survey by Kimberly A. Fisher, Ngoc Nguyen, Hassan Fouayzi, Sybil Crawford, Sonal Singh, May Dong, Ruth Wittenberg and Kathleen M. Mazor in Public Health Reports
Supplemental Material
sj-docx-2-phr-10.1177_00333549231176006 – Supplemental material for From COVID-19 Vaccine Hesitancy to Vaccine Acceptance: Results of a Longitudinal Survey
Supplemental material, sj-docx-2-phr-10.1177_00333549231176006 for From COVID-19 Vaccine Hesitancy to Vaccine Acceptance: Results of a Longitudinal Survey by Kimberly A. Fisher, Ngoc Nguyen, Hassan Fouayzi, Sybil Crawford, Sonal Singh, May Dong, Ruth Wittenberg and Kathleen M. Mazor in Public Health Reports
Supplemental Material
sj-docx-3-phr-10.1177_00333549231176006 – Supplemental material for From COVID-19 Vaccine Hesitancy to Vaccine Acceptance: Results of a Longitudinal Survey
Supplemental material, sj-docx-3-phr-10.1177_00333549231176006 for From COVID-19 Vaccine Hesitancy to Vaccine Acceptance: Results of a Longitudinal Survey by Kimberly A. Fisher, Ngoc Nguyen, Hassan Fouayzi, Sybil Crawford, Sonal Singh, May Dong, Ruth Wittenberg and Kathleen M. Mazor in Public Health Reports
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work presented in this article was funded by the National Library of Medicine, National Institutes of Medicine, under cooperative agreement UG4LM012347 with UMass Chan Medical School and the National Center for Advancing Translational Sciences, National Institutes of Health (NIH) through grant no. UL1TR001453. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIH.
Data Access Statement
The datasets used for the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online. The authors have provided these supplemental materials to give readers additional information about their work. These materials have not been edited or formatted by Public Health Reports’s scientific editors and, thus, may not conform to the guidelines of the AMA Manual of Style, 11th Edition.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.