
Abstract
Objective:
Disaggregated data on the mental health of Asian/Asian American people are needed to inform public health interventions related to reports of racism during the COVID-19 pandemic. We describe the prevalence of psychological distress and unmet mental health needs among Asian/Asian American adults during the COVID-19 pandemic across various sociodemographic subgroups.
Methods:
We used cross-sectional, weighted data from the US-based 2021 Asian American and Native Hawaiian/Pacific Islander COVID-19 Needs Assessment Study (unweighted n = 3508) to estimate prevalence rates of psychological distress and unmet mental health needs, overall and by nativity status. We conducted population-weighted multivariable logistic regression analyses to examine sociodemographic factors associated with these mental health outcomes.
Results:
About one-third (1419 of 3508) of Asian/Asian American adults (32.9%; 95% CI, 30.6%-35.2%) reported psychological distress; odds of psychological distress were increased among adults who were female, trans, and nonbinary; aged 18-44 years; US-born; Cambodian; multiracial; and low income. Of those reporting psychological distress (638 of 1419), 41.8% (95% CI, 37.8%-45.8%) reported unmet mental health needs; unmet mental health needs were highest among Asian/Asian American adults who were aged 18-24 years; Korean, Japanese, and Cambodian; US-born female; non–US-born young adults; and non–US-born with ≥bachelor’s degree.
Conclusions:
The mental health of Asian/Asian American people is an important public health concern, with some groups more vulnerable and in need of services than others. Mental health resources need to be designed for vulnerable subgroups, and cultural and systemic barriers to mental health care need to be addressed.
The COVID-19 pandemic, in addition to causing death and severe debilitating illness, brought changes to daily life, such as social distancing, remote work, and job loss, as well as challenges including decreased health care access and reduced social services providing necessary food and housing resources.1,2 For Asian/Asian American people and other historically marginalized groups, these COVID-19 stressors occurred within the context of racial and ethnic inequities and discrimination. 3
Reporting of anti-Asian hate incidents in the United States rose during COVID-19, 4 driven by anti-Asian racism and xenophobia combined with blame for COVID-19, 5 and continued a historical pattern of stereotyping and scapegoating Asian/Asian American people for introducing diseases (eg, “Yellow Peril” in the 19th century, the 2003 SARS outbreak). 6 Among Asian/Asian American people, COVID-19–related discrimination and vicarious racism are synergistically intertwined with other COVID-19 stressors. Syndemic theory, which explains how 2 or more co-occurring and intertwined health conditions may exacerbate one another and be rooted in and affected by social, political, historical, and/or ecological factors, can be used to frame the mental health experiences of Asian/Asian American people during the pandemic.7,8
Asian/Asian American people have generally reported lower prevalence rates of psychological distress and mental health service use than people in other racial and ethnic groups.9 -11 Substance Abuse and Mental Health Services Administration (SAMHSA) data from the 2019 National Survey on Drug Use and Health showed that 9% of Asian/Asian American adults reported symptoms of serious psychological distress in the past 12 months, compared with 12.7% of non-Hispanic White adults. 11 These data also showed that 7% of Asian/Asian American adults received mental health services in the past 12 months compared with 19.8% of non-Hispanic White adults. 11 SAMHSA data from 2008-2012 showed that Asian/Asian American and Native Hawaiian/Pacific Islander adults with a mental illness used mental health services the least among all racial and ethnic groups. 12 Because racism is associated with increased symptoms of depression and anxiety,13 -16 within the context of COVID-19–related stressors and anti-Asian racism, Asian/Asian American people may be more vulnerable to psychological distress and have increased mental health needs now than before the pandemic. It is important to examine differences in the Asian/Asian American population to understand who is most vulnerable to psychological distress and has unmet mental health needs.
We describe the prevalence of psychological distress and unmet mental health needs among Asian/Asian American adults during the COVID-19 pandemic. Although the US Census Bureau’s Household Pulse Survey (HPS) documented psychological distress and service use during the COVID-19 pandemic among Asian/Asian American people, 17 HPS data were collected only in English and Spanish, thereby missing critical data on the two-thirds of Asian/Asian American people who speak a non-English language at home. 18 We made population estimates using weighted data from a large study of Asian/Asian American people conducted in multiple languages. We also paid particular attention to differentiating vulnerabilities between non–US-born and US-born Asian/Asian American adults, because first-generation immigrants often have more difficulty accessing mental health care than US-born Asian/Asian American people as a result of structural, cultural, and linguistic barriers.10,19
Methods
Participants and Sample Design
Data for this study came from the Asian American and Native Hawaiian/Pacific Islander COVID-19 Needs Assessment Project, which itself is part of a larger study examining the impact of COVID-19 on racial and ethnic minority communities. 20 This national cross-sectional survey was conducted by a multidisciplinary team led by the second author (A.S.) on behalf of the Asian American Psychological Association to examine Asian/Asian American and Native Hawaiian/Pacific Islander experiences during the pandemic in areas such as mental health, discrimination, health, health care access, economic and housing impact, food security, and education.
Asian/Asian American and Native Hawaiian/Pacific Islander adults aged ≥18 years living in the United States were recruited through multiframe sampling: 68% of participants through community organization events (eg, vaccination drives, food deliveries) and outreach (eg, email lists, flyers, word of mouth) and 32% through an online Qualtrics panel. The survey could be completed online, on paper, or by telephone, and participants completed the survey from January 18 through April 9, 2021. We received ethics approval from the Association of Asian Pacific Community Health Organizations Institutional Review Board (IRB; IRB approval no. 2010-AAPCHO-02N-California-AAPI-COVID19-Needs-Assessment). Panel participants received a $10 gift card or equivalent compensation.
For the current study, we focused solely on the Asian/Asian American subsample. Five Asian groups were targeted during study recruitment: Chinese, Filipino, Korean, Vietnamese, and specific South Asian ethnicities (eg, Indian, Bangladeshi, Pakistani). Adults of other Asian ancestries, although not the focus of these sampling strategies, were not excluded from participating and were included in the final analytic sample. The survey was translated from English into the following languages based on recruitment strategy and community partner requests: Bangla, Chinese (traditional and simplified), Hindi, Khmer, Korean, Tagalog, Urdu, and Vietnamese.
We included in analyses 3508 respondents who self-identified as Asian race, including multiracial adults and respondents who did not have missing data on ethnicity.
Measures
We developed the survey with input from national and community organization partners. It included validated and recent COVID-19 pandemic–related measures, items taken from HPS, and items developed in collaboration with community partners. Study data were collected (or, in the case of paper/telephone surveys, entered into) and managed using Qualtrics.
Psychological Distress
We calculated psychological distress from the modified version of the Patient Health Questionnaire–4 (PHQ-4) used by HPS,21 -23 which comprises the 2-item Generalized Anxiety Disorder scale (GAD-2) and the 2-item Patient Health Questionnaire–2 (PHQ-2), 22 assessing symptoms during the last 7 days (rather than 14 days) with the following items: “Over the last 7 days, how often have you been bothered by the following problems: (a) feeling nervous, anxious, or on edge; (b) not being able to stop or control worrying; (c) having little interest or pleasure in doing things; and (d) feeling down, depressed, or hopeless.” Response options were not at all (0), several days (1), more than half the days (2), and nearly every day (3). We summed scores for anxiety (items a and b) and depression (c and d). Summed scores of at least 3 suggest anxiety/depression. 23 We then dichotomized psychological distress as follows: yes, experiencing psychological distress (scoring ≥3 on either the anxiety or depression subscales); no, not experiencing psychological distress (scoring ≤2 on both the anxiety and depression subscales).
Unmet Mental Health Needs
We calculated unmet mental health needs for those experiencing psychological distress and reporting needing help accessing mental health services. Need for mental health services was assessed with 1 item developed for this study in consultation with community partners: “Which of the following do you need more help getting during the COVID-19 pandemic? Select all that apply.” Participants selected as many options as were applicable from an 11-item list including mental health services (as well as food, housing, utilities, internet, unemployment, health services, mental health services, emergency services, legal assistance, childcare, faith-based or spiritual care, and other). Participants experiencing psychological distress who selected needing help accessing mental health services were categorized as having unmet mental health needs (1). Participants experiencing psychological distress who did not select needing help accessing mental health services were categorized as not having unmet mental health needs (0). Participants who were not experiencing psychological distress were excluded in analyses of this outcome.
Correlates
Participants were asked to select their racial and ethnic identity(ies) from the following: Asian, Native Hawaiian or Pacific Islander, Native American or Alaska Native, African American or Black, non-Hispanic/Latino White, Hispanic/Latino, or Middle Eastern or North African. Participants could select as many racial and ethnic identities as applicable, and we categorized respondents who identified with >1 racial and ethnic group as multiracial. Participants who reported Asian as their race were additionally asked to select from the following list terms that “best express how [they] describe [their] ethnic identity”: Chinese, Filipino, Indian, Vietnamese, Korean, Japanese, Pakistani, Cambodian, Hmong, Thai, Laotian, Bangladeshi, Burmese, Indonesian, Nepalese, Sri Lankan, Malaysian, Bhutanese, Mongolian, Okinawan, and Other. Participants could select as many ethnic identities as applicable; respondents who identified with >1 ethnic group were categorized as multiethnic. Ethnic identity categories with <40 responses were combined into the Other category in analyses. The categories for this variable were also mutually exclusive, such that if a participant was classified as multiethnic, the participant was not counted again within his or her identified ethnic groups. Ethnic identity categories were the following: Chinese, Filipino, Indian, Vietnamese, Korean, Japanese, Pakistani, Cambodian, Other, multiethnic, or multiracial. Other sociodemographic variables included gender identity, age group, annual household income, and education. Years living in the United States was calculated based on participants’ reported country of birth and number of years living in the United States, if reporting a country of birth other than the United States. Those reporting a country of birth other than the United States were categorized as non–US-born. Survey language (English, another language) was calculated based on the language of survey completion (English [n = 3021], Chinese [n = 378], Korean [n = 91], Khmer [n = 12], Urdu [n = 3], and Vietnamese [n = 3]). US region was calculated based on participants’ reported zip codes and categorized according to the 4 US Census regions (Northeast, Midwest, South, West). 24
Data Analysis
We created sample weights using the ranking method to match the Asian population estimates from the 2019 US Census American Community Survey (ACS) 1-year estimates. Thus, sample weights reflect the representative Asian/Asian American population in the United States as of 2019 and account for multiracial Asian/Asian American adults. 24 We based weights on the following variables: ethnicity, nativity (non–US-born vs US-born), education, annual household income, gender identity, and age. The 2019 ACS provides the most up-to-date population information for the United States by Asian ethnic groups.
Annual household income had the most missing values (n = 62; 1.8% missing). To generate the correct parameter estimates, we used multiple imputation methods to account for missingness, creating 25 imputed datasets to calculate pooled results.
We computed the population-weighted prevalence of psychological distress and unmet mental health needs, stratified by ethnicity, gender identity, age, annual household income, education, number of years in the United States, survey language, and US region. We used weighted Rao–Scott statistics to test the significance of differences between proportion estimates, with P < .05 considered significant. 25 We computed multivariable logistic regression models to examine the effect of the demographic variables on both outcomes. We selected most reference groups for the demographic variables based on previous research that suggested that the group had the lowest prevalence of each outcome; where research findings were mixed or not available, we selected the reference group as the group on one extreme of the ordinal variable (eg, number of years in the United States). For ethnicity, we selected Chinese as the reference group because it was the largest subsample. For region, we selected Northeast as the reference group arbitrarily. We calculated the weighted odds ratios (ORs) and 95% CIs for the overall, US-born, and non–US-born models for both outcomes. We conducted all analyses in R version 4.0.3 (in RStudio version 1.4.1106) (R Foundation for Statistical Computing) using the stats and survey packages.
Results
Overall, 32.9% (95% CI, 30.6%-35.2%) of Asian/Asian American adults reported psychological distress (1419 of 3508), and 24.1% (95% CI, 22.1%-26.1%) reported needing help accessing mental health services (638 of 1419). Of those who reported psychological distress, 41.8% (95% CI, 37.8%-45.8%) reported needing help accessing mental health services and, thus, having unmet mental health needs (Table 1).
Unweighted sample sizes and population-weighted rates of psychological distress and unmet mental health needs among Asian and Asian American adults (N = 3508) during the COVID-19 pandemic, United States, January 18–April 9, 2021
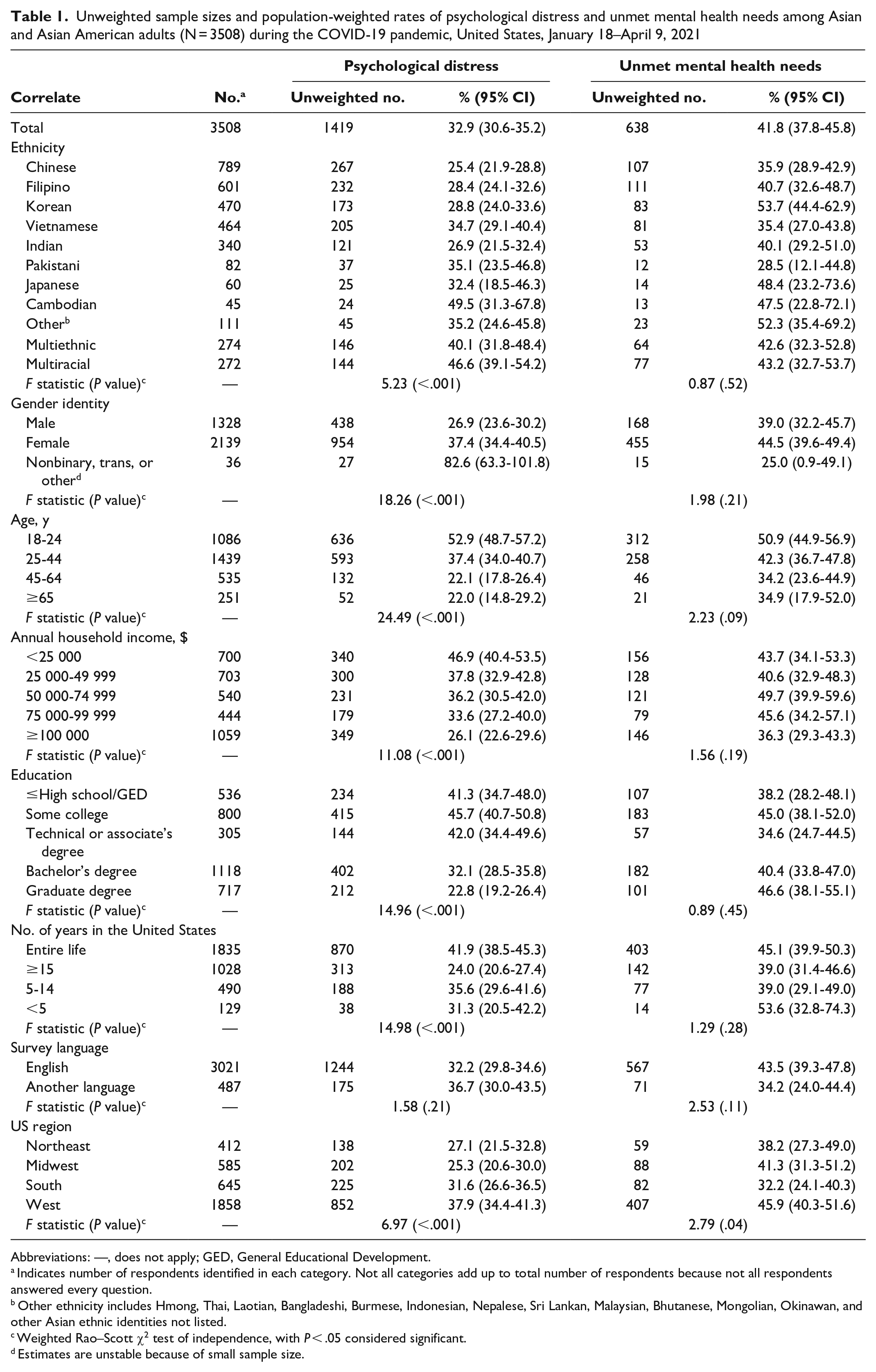
Abbreviations: —, does not apply; GED, General Educational Development.
Indicates number of respondents identified in each category. Not all categories add up to total number of respondents because not all respondents answered every question.
Other ethnicity includes Hmong, Thai, Laotian, Bangladeshi, Burmese, Indonesian, Nepalese, Sri Lankan, Malaysian, Bhutanese, Mongolian, Okinawan, and other Asian ethnic identities not listed.
Weighted Rao–Scott χ2 test of independence, with P < .05 considered significant.
Estimates are unstable because of small sample size.
Psychological Distress
Rates of psychological distress differed significantly for all correlates except survey language: ethnicity: F = 5.23, P < .001; gender: F = 18.26, P < .001; age: F = 24.49, P < .001; annual household income: F = 11.08, P < .001; education: F = 14.96, P < .001; years in the United States: F = 14.98, P < .001; and US region: F = 6.97, P < .001 (Table 1). In logistic regression models, we found increased odds of psychological distress among Cambodians (adjusted OR [aOR] = 2.12), particularly non–US-born (aOR = 1.94) and multiracial (aOR = 1.54; particularly US-born [aOR = 1.90]) Asian/Asian American adults (vs Chinese adults); women (aOR = 1.50) and trans or nonbinary adults (aOR = 9.09) (vs men); adults aged 18-24 years (aOR = 3.04) and 25-44 years (aOR = 2.05) (vs adults aged ≥65 y); and those who had lived their entire life in the United States (aOR = 0.08) (vs lived in the United States for <5 years) (Table 2). Overall, the odds of psychological distress increased as income category decreased, particularly among non–US-born Asian/Asian American adults; those with annual household income <$25 000 had 3 times higher odds of psychological distress than those with annual household income ≥$100 000. US-born Asian/Asian American adults with an annual household income of $75 000-$99 999 had 1.88 times higher odds of psychological distress than those with annual household income ≥$100 000. Having some education (ie, technical degree, associate’s degree) increased the odds of psychological distress (aOR = 1.67), particularly among non–US-born Asian/Asian American adults (aOR = 1.89); however, those with less education did not have increased odds of psychological distress. Among US-born Asian/Asian American adults, those who completed the survey in an Asian language had increased odds of psychological distress (aOR = 2.63).
Population-weighted logistic regression models of psychological distress among Asian and Asian American adults (N = 3508) during the COVID-19 pandemic, United States, January 18–April 9, 2021
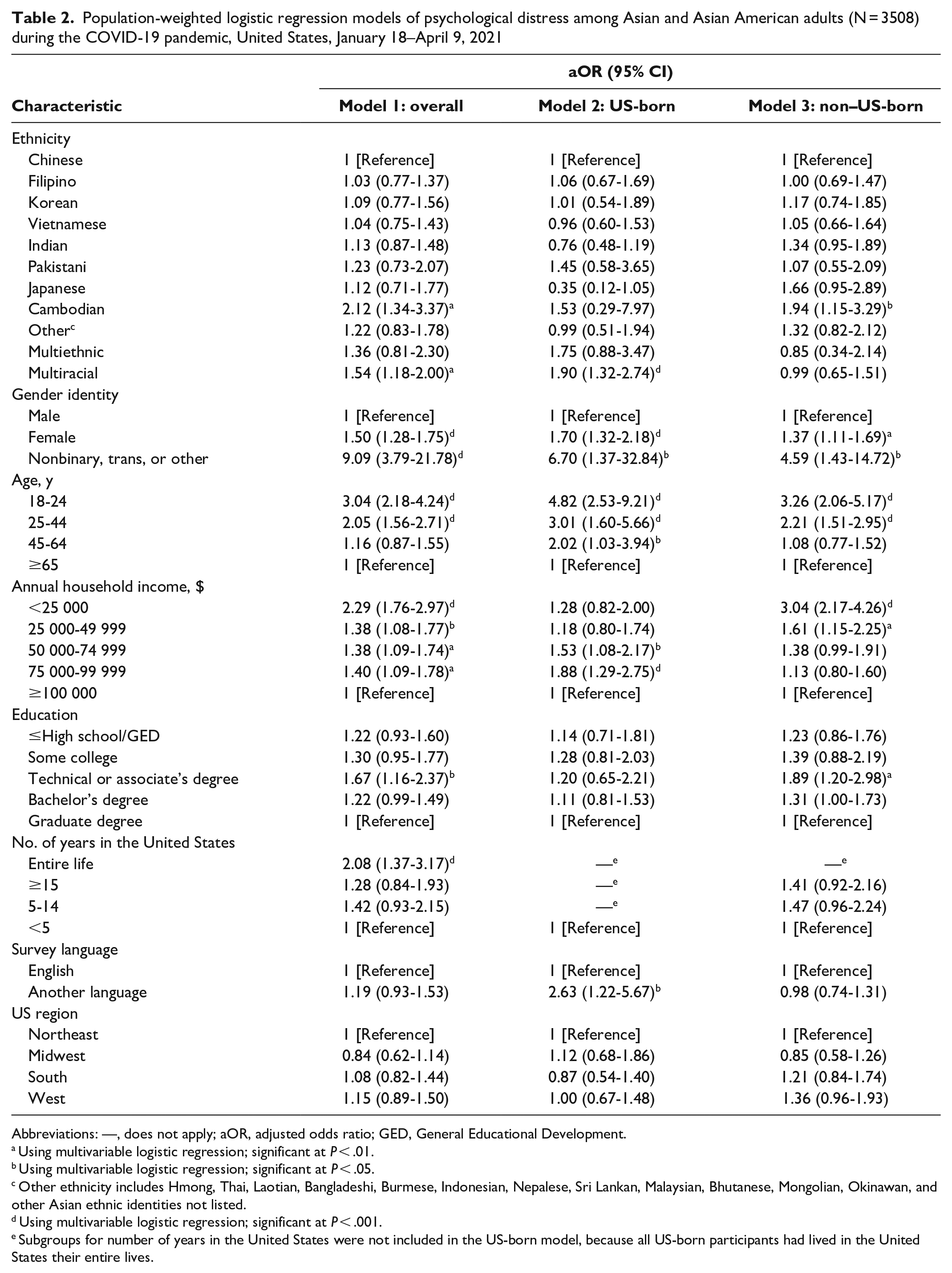
Abbreviations: —, does not apply; aOR, adjusted odds ratio; GED, General Educational Development.
Using multivariable logistic regression; significant at P < .01.
Using multivariable logistic regression; significant at P < .05.
Other ethnicity includes Hmong, Thai, Laotian, Bangladeshi, Burmese, Indonesian, Nepalese, Sri Lankan, Malaysian, Bhutanese, Mongolian, Okinawan, and other Asian ethnic identities not listed.
Using multivariable logistic regression; significant at P < .001.
Subgroups for number of years in the United States were not included in the US-born model, because all US-born participants had lived in the United States their entire lives.
Unmet Mental Health Needs
Rates of unmet mental health needs were not significantly different for any correlates except US region; 45.9% (95% CI, 40.3%-51.6%) of Asian/Asian American adults residing in the West had unmet mental health needs (F = 2.79, P = .04) (Table 1). In logistic regression models, the odds of having unmet mental health needs were higher among adults aged 18-24 years (aOR = 2.58), particularly non–US-born adults (aOR = 4.01), than among adults aged ≥65 years, and among Korean adults (aOR = 2.53), particularly non–US-born Korean (aOR = 2.87), Japanese (aOR = 2.56), Cambodian (aOR = 2.43), and other Asian/Asian American (aOR = 1.94) adults, than among Chinese adults (Table 3). US-born women had 1.50 times higher odds of unmet mental health needs than men, but we found no significant differences by gender for non–US-born women. Generally, adults with low education levels had decreased odds of unmet mental health needs; this finding was particularly apparent among non–US-born Asian/Asian American adults with a high school diploma/General Educational Development or <high school diploma (aOR = 0.36), some college (aOR = 0.41), or a technical or associate’s degree (aOR = 0.25). Among non–US-born Asian/Asian American adults, those living in the United States for 5-14 years had lower odds of unmet mental health needs (aOR = 0.45) than adults living in the United States for <5 years. Non–US-born Asian/Asian American adults living in the West, however, had increased odds of unmet mental health needs (aOR = 2.23) compared with adults living in the Northeast.
Population-weighted logistic regression models of unmet mental health needs among Asian and Asian American adults (N = 3508) during the COVID-19 pandemic, United States, January 18–April 9, 2021
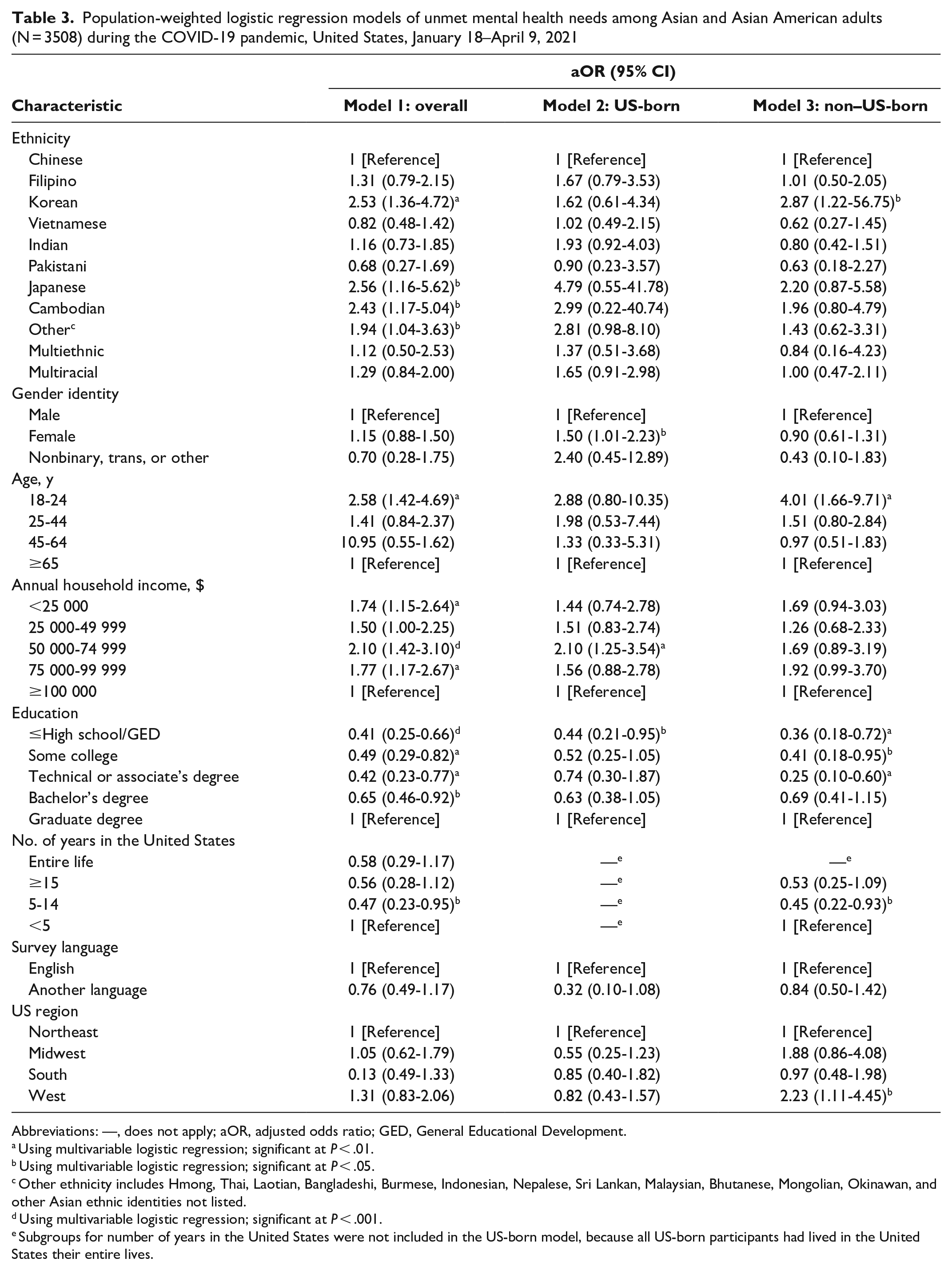
Abbreviations: —, does not apply; aOR, adjusted odds ratio; GED, General Educational Development.
Using multivariable logistic regression; significant at P < .01.
Using multivariable logistic regression; significant at P < .05.
Other ethnicity includes Hmong, Thai, Laotian, Bangladeshi, Burmese, Indonesian, Nepalese, Sri Lankan, Malaysian, Bhutanese, Mongolian, Okinawan, and other Asian ethnic identities not listed.
Using multivariable logistic regression; significant at P < .001.
Subgroups for number of years in the United States were not included in the US-born model, because all US-born participants had lived in the United States their entire lives.
Discussion
The increased stress, social isolation, and anti-Asian racism and discrimination brought on by the COVID-19 pandemic have magnified mental health challenges among Asian/Asian American people. Even prior to the pandemic, accessing quality mental health care was challenging for Asian/Asian American people because of inadequate funding for mental health services, uneven geographic distribution of health care providers, and lack of coordination between health care providers. 13 Our findings suggest unprecedented mental health needs among Asian/Asian American adults and may inform the design of public health and other social policies for Asian/Asian American subgroups with the greatest mental health needs. To our knowledge, the current study is the largest study assessing the mental health needs of Asian/Asian American adults during the pandemic in multiple Asian languages and English.
Although rates of psychological distress among Asian/Asian American adults (32.9%) in our study were lower than rates among the general US adult population assessed by the 2020-2022 HPS (conducted only in English and Spanish) during the same period (41.5%), 21 we found higher rates of psychological distress among Asian/Asian American adults during the pandemic than before the pandemic (9% as of 2019 SAMHSA data) 11 and using HPS data (4-week average of 20%; Lee et al, unpublished data, 2022). In addition, results from our study point to sociodemographic subgroups in the Asian/Asian American community with high rates of psychological distress. Similar to 2020 California Health Interview Survey (CHIS) data, 26 our data showed that Asian/Asian American adults aged 18-24 years reported more symptoms of psychological distress than Asian/Asian American adults aged ≥25 years. Our findings also confirmed 2020 CHIS data on gender identity differences among Asian/Asian American people, 26 finding that women generally had higher rates of psychological distress than men. Our study additionally found that nonbinary and trans Asian/Asian American adults had higher rates of psychological distress than Asian/Asian American men; 2020 CHIS data comparing transgender and cisgender people were unstable. 26
Consistent with previous research, we found that Asian/Asian American people had high rates of unmet mental health needs.10,13,27 Compared with national estimates during the same period, Asian/Asian American people in our study reported greater unmet mental health needs (41.8% vs 11.7%). 28 Furthermore, we identified demographic subgroups with high levels of unmet mental health needs. Contrary to the 2002-2003 National Latino and Asian American Study (NLAAS), 27 which found that number of years in the United States was not associated with greater unmet mental health needs among non–US-born Asian American people, our study found that Asian/Asian American adults living in the United States for <5 or >15 years had higher rates of unmet mental health needs than Asian/Asian American adults living in the United States for 5-14 years. Although the NLAAS did not find ethnic differences, in our study we found that, compared with Chinese respondents, Korean and Cambodian respondents had higher rates of unmet mental health needs. Of note, those categorized into the Other ethnic category because of insufficient sample sizes also had high rates of unmet mental health needs, underscoring the importance of oversampling distinct ethnic groups to draw more precise conclusions about them.
A syndemic lens indicates that the effects of the synergistic interplays of poor health and health care access, anti-Asian racism, and other COVID-19–related stressors are not uniform across Asian/Asian American people. 8 Accordingly, subgroups with intersecting marginalized identities, such as women, trans and nonbinary Asian/Asian American people, and Asian/Asian American people with low income and education levels, have faced disproportionate stressors, such as discrimination 29 and job loss, 30 that increase the odds of psychological distress and unmet mental health needs. Consistent with the syndemic framework, other sociodemographic subgroups, such as Cambodian people, may have high levels of mental health needs because of historical trauma coupled with ongoing structural violence and inadequate community resources.31,32
Generally, our findings confirm other research that US-born people have worse mental health than non–US-born people. 33 Yet, stratifying results for non–US-born Asian/Asian American people highlights subgroups, such as Cambodian people, young adults aged 18-44 years, women, trans and nonbinary people, and those with low income, who are most vulnerable to psychological distress; as well as Korean people, young adults aged 18-24 years, those with higher education levels, and those residing in the West, who are most vulnerable to unmet mental health needs. Although research is not yet available to explain all the subgroup differences we found, we are hopeful that our findings can help direct resources and policy toward specific Asian/Asian American subgroups with high mental health needs and provide a foundation for future research.
During the period of data collection, a shooting occurred in the Atlanta area that killed 8 people, including 6 Asian women. Immediately after the March 2021 shooting, mainstream and social media coverage of anti-Asian racism and discrimination likely increased, raising risks for poor mental health. 34 In exploratory post hoc analyses, we found that significantly more respondents reported psychological distress after the Atlanta-area shooting than before the shooting, suggesting that Asian/Asian American adults were affected. Further research is needed to explore how distinct subgroups of Asian/Asian American people were broadly affected and may continue to be affected by this event and other events.
Limitations
This study had several limitations. First, although we oversampled some Asian ethnic groups for data disaggregation, our conclusions were still limited for the smallest subgroups. Our subsample of nonbinary and trans Asian/Asian American adults was small, resulting in unstable estimates. Future research should focus on recruitment of these and other groups for whom adequate data are currently lacking to better illuminate the experiences of health inequities and drive policy change and resource allocation. Second, our study was limited in its cross-sectional view of mental health during a few months of the pandemic; we cannot conclude longitudinal or causal relationships between the correlates and mental health outcomes.
Conclusion
Connecting Asian/Asian American people with high mental health needs to culturally and linguistically appropriate mental health services is critical. Doing so requires long-term investments in training culturally responsive mental health providers; expanding the general and Asian/Asian American–specific mental health workforce; incentivizing mental health providers to serve Asian/Asian American communities, particularly those most vulnerable to mental health distress; increasing accessibility to affordable health insurance that covers mental health services; and decreasing mental health care costs. Furthermore, taking a syndemic approach, it is important to address the drivers of psychological distress—specifically, the multitude of pandemic- and racism-related stressors that negatively impact Asian/Asian American mental health, such as poor working conditions, violent hate incidents, discrimination in health care, and anti-Asian political and social rhetoric. As anti-Asian racism continues, entwined with other repercussions from the COVID-19 pandemic, future research examining the long-term mental health impacts of the COVID-19 pandemic through a syndemic lens is needed.
Footnotes
Acknowledgements
The authors thank Aggie Yellow Horse, PhD, MA, for her work in weighting the data. The authors also acknowledge the research team members of the Asian American & Native Hawaiian/Pacific Islander COVID-19 Needs Assessment Project who collaborated to develop and make this project possible: Nia Aitaoto, PhD, MS; Raynald Samoa, MD; Janice Y. Tsoh, PhD; Stella S. Yi, PhD, MPH; and Lan N. Đoàn, PhD, MPH. We also thank the Chicago Asian American Psychology Lab members for their supporting work in setting up, collecting, and cleaning data for this project: Shreya Aragula, MA; Wendy de los Reyes, MSEd; Nancy Mai, MPH; Jay Mantuhac, MPH; Samantha Nau, MA; Afshan Rehman, BA; and Sabrina Salvador, BA. In addition, we thank the many community organizations and community partners who worked with us to develop the survey and collect data from community members, including the following: Arkansas Coalition of Marshallese, Asian Business Association of San Diego, Asian Pacific Community in Action, Asian Pacific Partners for Empowerment, Asian & Pacific Islander American Health Forum, Association of Asian Pacific Community Health Organizations, Canvasback Wellness Center, Center for Pan Asian Community Services, Chinese-American Planning Council, Chuuk Community Health Center, Chuuk Women’s Council, Coalition for a Better Chinese American Community, Coalition for Asian American Children + Families, Community & Advocacy Network Partners, Advocacy, and Leadership, Empowering Pacific Islander Communities, Faith in Action Research and Resource Alliance, Filipino American National Historical Society, First Chuukese Washington Women’s Association, HANA Center, Hanul Family Alliance, Hawaii COVID-19 Native Hawaiian/Pacific Islander Response, Recovery, and Resilience Team, Hiệp Lực VN Teamwork Inc, Kalusugan Coalition, Kosrae Community Health Center, Kwajalein Diak Coalition, Marianas Health, Marshallese Women’s Association, National Council of Asian Pacific Americans, National Indo-American Museum, National Tongan American Society, Native Hawaiian and Pacific Islander Alliance, Northern California COVID-19 Response Team, Oregon Pacific Islander Coalition, Oregon Pacific Islander COVID-19 Response Team, Pacific Islander Community Association of Washington, Pacific Islander Health Board of Washington, Pacific Islands Primary Care Association, Palau Community Health Center, Papa Ola Lokahi, Pasefika Empowerment and Advancement, PolyByDesign, Pui Tak Center, Regional Pacific Islander Taskforce, Search to Involve Pilipino Americans, SoCal Pacific Islander COVID-19 Response Team, Tinumasalasala A Samoa Student Organization, Utah Pacific Islander Civic Engagement Coalition, Utah Pacific Islander Health Coalition, UTOPIA Portland, UTOPIA Seattle, and We Are Oceania.
Disclaimer
The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the funders. No funders had any role in the writing of the article or the decision to submit it for publication. No authors were paid to write this article by any company or agency. All authors accept responsibility to submit for publication.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Ford Foundation, JPB Foundation, W.K. Kellogg Foundation, California Endowment, Weingart Foundation, and California Wellness Foundation through the fiscal sponsorship of the National Urban League to the Asian American Psychological Association.