
Abstract
Objective:
To better understand health experiences among Two Spirit and lesbian, gay, bisexual, transgender, and queer and questioning (LGBTQ+) American Indian/Alaska Native (AI/AN) people, we examined experiences with access to health care of 223 AI/AN Two Spirit and LGBTQ+ people.
Methods:
Participants of the Pride and Connectedness 2020 survey, conducted through the Northwest Portland Area Indian Health Board, were asked about barriers to seeking and accessing care through a 10-question scale. We compared cisgender and gender-diverse participant demographic and scale responses to explore potential differences based on gender identity using the Pearson χ2 test of independence and ordinal logistic regression, respectively.
Results:
Both cisgender and gender-diverse participants experienced at least some difficulties accessing health care. Finances, lack of psychologists/other mental health support, and lack of psychological support groups for Two Spirit and LGBTQ+ communities were the top 3 barriers to care experienced by all participants (84%, 82%, and 80%, respectively). Compared with cisgender participants, gender-diverse participants were more likely to report difficulties accessing care for nearly all questions on the 10-question scale and nearly 3 times more likely to report fear of being mistreated within the health care system based on their gender identity (adjusted odds ratio = 2.9; 95% CI, 1.8-4.9; P < .001).
Conclusions:
Increased access to mental health services and improved health care provider training that focuses on culturally relevant and gender-affirming practices would benefit the health and well-being of AI/AN people who identify as Two Spirit and LGBTQ+.
There are more than 574 federally recognized Tribes in the United States and even more state-recognized and unrecognized Tribes. Each Tribe has its own culture, history, knowledge, and way of referring to itself. Throughout this article, we use the term “Native” to refer to the Indigenous people of the United States and Canada. We use Two Spirit and LGBTQ+ to refer to our Two Spirit, lesbian, gay, bisexual, transgender, and queer and questioning relatives, as well as all relatives with minority sexual orientations and gender identities. These individuals may be cisgender and queer or transgender. We separate Two Spirit because many within this community will resonate with that either separately or to the exclusion of more Westernized terms invoked by the LGBTQ+ identification. At minimum, Two Spirit identity is a recognition of the intersection between Indigeneity and variance in gender identity and/or sexual orientation, while for many it is a firm acknowledgment of one’s self-identification with roles and ways of being that have been in Indigenous communities beyond Western binary thought since time immemorial.
Health-related research on American Indian/Alaska Native (AI/AN) Two Spirit and lesbian, gay, bisexual, transgender, and queer and questioning (LGBTQ+) (2SLGBTQ+) populations is limited. Health disparities among AI/AN 2SLGBTQ+ people are considerable, and AI/AN people who are transgender or Two Spirit are less likely to access health care and receive preventive health care than their cisgender counterparts are, which can lead to health disparities including higher rates of sexually transmitted infections, substance use, mood disorders, and suicide.1,2 Furthermore, stigma, discrimination, and lack of gender-affirming care limit the ability of AI/AN people who are transgender and Two Spirit to engage in and benefit from health care settings. 3
Although gender identity and diversity within Native communities was once widely accepted and venerated, the process of colonization often altered the status of Two Spirit people in their communities, forcing assimilation into a Eurocentric culture that rejected such diversity. 4 Today, as a result of such colonization, AI/AN 2SLGBTQ+ people are often associated with health and social disparities, which are likely traceable to barriers to seeking and accessing health care, especially for Two Spirit and transgender people. According to a national survey of 319 AI/AN people who identified as transgender, half reported a negative experience within the health care system relating to their gender identity, including being verbally harassed and sexually assaulted. 1
While some data exist on experienced barriers to care for the non-Native LGBTQ+ community, there is a dearth of literature on AI/AN 2SLGBTQ+ people and their experiences with accessing health care. To address this gap, we aimed to improve understanding of the current health status of 2SLGBTQ+ people, including risk factors such as barriers and access to health care, to support initiatives that promote quality care and improved health outcomes for 2SLGBTQ+ people. Although we were interested in the responses and experiences of all participants in the study, we explored responses based on cisgender and gender-diverse identities to better understand differences in experiences, if any, that exist between the 2 groups.
Methods
Survey Design
The survey questions used for this analysis were part of the Pride and Connectedness survey, a larger survey that focused on myriad topics, including pride, community connectedness, self-rated health, mental health, intimate partner violence, barriers to health care access, and current health needs. The survey design process was guided by the CIRCLE Framework, an Indigenous framework for program design that incorporates Western concepts of community capacity building while building mutual trust between researchers and Native communities to minimize the potential for exploitation or abuse of power.5,6 2SLGBTQ+ people and national Two Spirit workgroups were involved in the survey development to ensure community and cultural relevance.
Because we cannot assume that scales that have been verified in majority-White populations are relevant to or adequate for AI/AN populations, original scales for the survey were created; however, non-Native scales that assess LGBTQ+ connectedness and pride, including those from the Lesbian Gay Bisexual Identity Scale, 7 the Trans PULSE Project, 8 the Trans Identity Survey, 9 and 2 literature reviews of surveying instruments measuring pride and connectedness,10,11 informed survey design. For example, the measure, “I’m proud to be part of the LGB community” from the Lesbian, Gay, Bisexual Identity Scale appeared in multiple forms (“I’m proud to be Indigenous,” “I’m proud to be Two Spirit,” or “I’m proud to be transgender or genderqueer”) because of the necessity of recognizing and making space for nuances of AI/AN and non-AI/AN understandings of gender and sexuality and ensuring we come to understand the true source of pride for AI/AN 2SLGBTQ+ people. Questions about health care access were adapted from the Alaska Native LGBTQ survey completed by the Alaska Native Tribal Health Consortium (C. Jessen, MA; J. Richards, MS; G. Day, MPH, M. Daniel, PhD; unpublished data, 2020).
Overall, the survey included 189 fields; 18 were open ended, and the rest were either multiple choice or parts of matrices. These fields were divided into 5 sections: demographic characteristics, acceptance/discrimination, Native/2SLGBTQ+ pride and community, self-rated physical/mental health and safety, and access to health care.
Survey design and protocol were submitted to the Portland Area Institutional Review Board in March 2020 and approved in August 2020; the survey was live from August 26 through September 3, 2020. Online survey results were collected via the REDCap platform housed at the Alaska Native Tribal Health Consortium, which is a member of the REDCap consortium and allows researchers to use this tool for data collection and management. The REDCap server resides in a secure data center on the Alaska Native Tribal Health Consortium campus that is compliant with the Health Insurance Portability and Accountability Act. All communications with the REDCap server are encrypted in transit. All participant data were deidentified to protect the confidentiality of survey participants and community members.
Participant Eligibility and Recruitment
Northwest Portland Area Indian Health Board (NPAIHB) staff collaborated to develop recruitment media that provided relevant information about the study. Materials were then posted on the NPAIHB social media accounts (@2SLGBTQ) and short message service (SMS) texting platforms.
To participate in the survey, individuals had to identify as Indigenous, reside in the United States, be aged >15 years, and identify as Two Spirit or LGBTQ+. Because of the difficulty of reaching AI/AN 2SLGBTQ+ people using traditional sampling methods, a nonprobability chain-referral sampling method was used, which involves identification and recruitment of a small number of “seed” participants via word of mouth and social media or text outreach; these participants then provide contact information for other potential participants.5,12 Initial seed participants were carefully chosen and interviewed to fulfill sampling needs created by gaps in existing research, caused by difficulties of penetrating effectual social networks in this hard-to-reach community. 13 Seed participants recruited other participants through either weak ties (acquaintances) or strong ties (friends). Each seed had a fixed number of coded coupons (a maximum of 3) that they could use to recruit peers from their social network. Upon completion of the survey, recruits were given a set of coupons for a second wave of peers. Those who completed the survey were given $100. This amount is meant not only to compensate the individual for taking the time to complete the survey but also as an acknowledgment of the knowledge and experiences they shared on the survey form. Participant consent was obtained through a digitally signed consent form that included a written description detailing the purpose and content of the project, confidentiality, and how the data will be collected, stored, and used.
Measures and Analysis
We calculated descriptive statistics to report demographic characteristics of participants, including age (15-19, 20-24, 25-29, 30-34, and ≥35 y), education (<high school, high school degree/General Educational Development, some college, associate’s degree), employment (employed full-time, employed part-time, not employed/not listed, other [ie, employed in traditional lifestyle, retired, full-time caregiver, student, or vocational training]), annual household income (<$20 000, $20 000-$39 999, $40 000-$59 999, $60 000-$79 999, ≥$80 000), health insurance status (insured, not insured), and geographic location (rural vs urban; living on reservation vs not living on reservation; Alaska, Hawai’i, Midwest, Northeast, Pacific Northwest, South, Southwest region, and Western/California regions). Particpants were also asked to rate their health on a scale ranging from 1 (poor) to 5 (excellent). A 10-question scale on health care access was used to assess barriers to seeking and accessing care. Response options were no problem at all, barely a problem, a significant problem, an extreme problem, or does not apply. Due to small cell sizes (ie, the count of responses for each response option), some response options were combined and coded as 1 (no problem at all/does not apply), 2 (barely a problem), or 3 (a significant or extreme problem). Participants could also write in additional experienced barriers to seeking and accessing care. We calculated the Cronbach α coefficient of reliability to determine the internal reliability of the 10-question scale, which was equal to 0.85 for the survey sample. 14 We compared cisgender and gender-diverse participants to examine any possible differences in challenges related to accessing care. We categorized participants as gender diverse if they answered yes to the question, “Do you consider yourself to be transgender or gender diverse?” We used the Pearson χ2 test of independence to compare demographic characteristics, and we used ordinal logistic regression to compare the Likert-scale responses of cisgender and gender-diverse participants at the significance level of P < .05. Cisgender participants were the reference group. We controlled for annual household income because of the observed differences in income between the comparison groups. We completed all analyses using SAS version 9.4 (SAS Institute Inc).
Results
Of 549 survey responses, 326 were fraudulent. Despite security measures, which included a separately submitted consent form and ReCAPTCHA, the survey was hacked 56 hours after it opened. After the survey was hacked, we received numerous fraudulent entries in addition to legitimate entries. The fraudulent entries followed distinct themes. They listed “Native” or “Tribe,” when responding to Tribal affiliation, which led us to believe the hacker was unlikely to be Indigenous. They also left free-response questions blank or provided nonsensical answers. Furthermore, the time for completion dropped to <5 minutes. (Average response time for legitimate entries was 26 minutes.) Using these patterns, we were able to manually identify and disqualify fraudulent responses. After this process, 223 responses were deemed legitimate and kept for analysis.
Sociodemographic Characteristics of Participants
Twenty-four percent of participants were from the Southwest, 20% from the Pacific Northwest, 17% from the West/California, 14% from the Midwest, 5% from Alaska/Hawaii, and 4% from the Northeast. Participant ages ranged from 15 to 55 years, with an average age of 26.7 years and a mode of 21 years. One hundred thirteen (51%) participants self-identified as cisgender and 110 (49%) self-identified as gender-diverse (Table 1). Thirty-eight percent (n = 43) of cisgender participants identified as Two Spirit, and 76% (n = 84) of gender-diverse participants identified as Two Spirit.
Sociodemographic characteristics of AI/AN Two Spirit and LGBTQ+ participants in the Pride and Connectedness Survey, United States, 2020 a
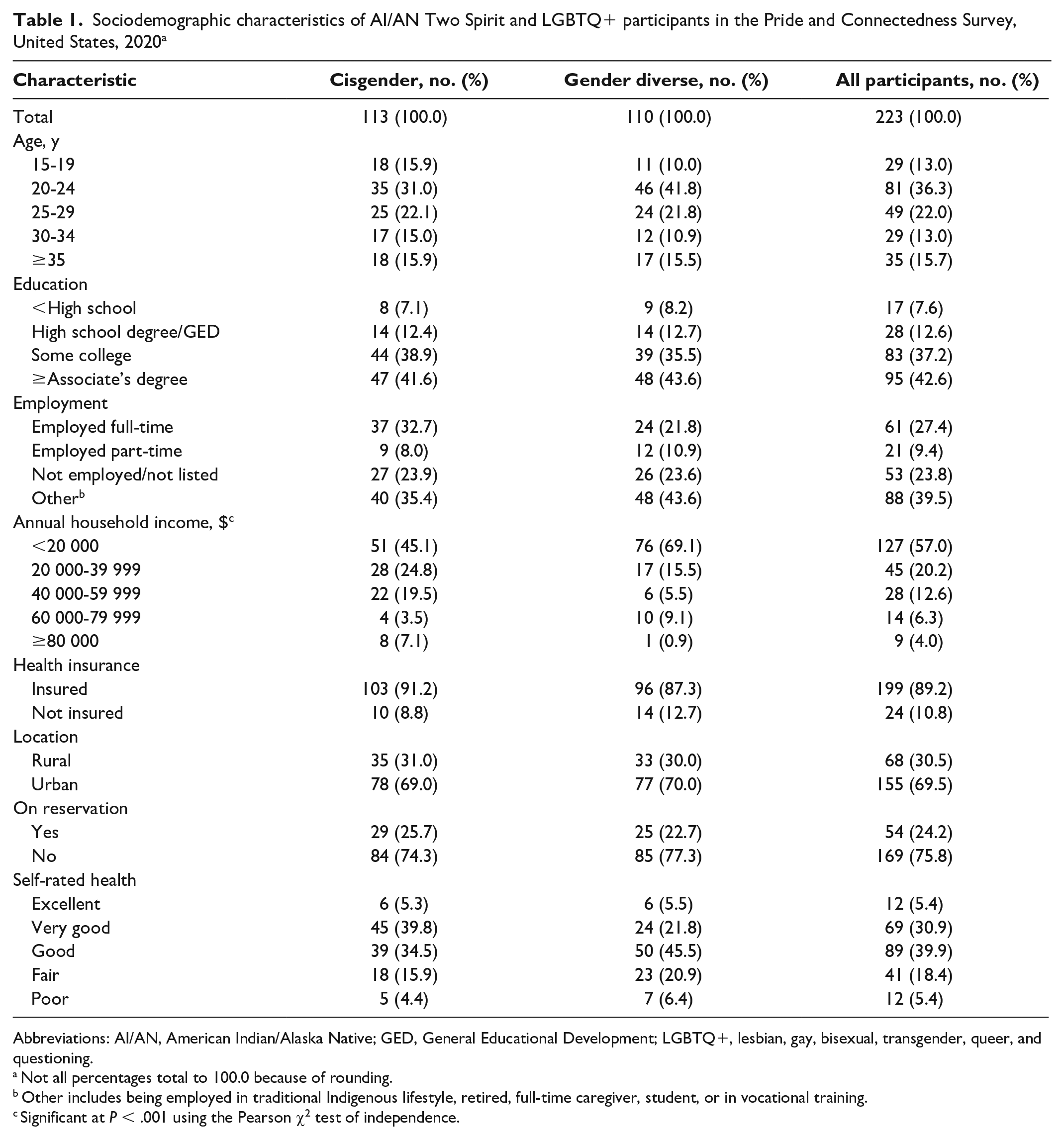
Abbreviations: AI/AN, American Indian/Alaska Native; GED, General Educational Development; LGBTQ+, lesbian, gay, bisexual, transgender, queer, and questioning.
Not all percentages total to 100.0 because of rounding.
Other includes being employed in traditional Indigenous lifestyle, retired, full-time caregiver, student, or in vocational training.
Significant at P < .001 using the Pearson χ2 test of independence.
Among gender-diverse participants, there were 270 responses on gender identity (participants could check >1 response option on how they identify). Of gender-diverse participants, 63.6% (n = 70) identified as Two Spirit, 50.0% (n = 55) as nonbinary, 33.6% (n = 37) as women, 23.6% (n = 26) as gender fluid, 20.0% (n = 22) as gender queer, 15.5% (n = 17) as transgender, 10.9% (n = 12) as trans women, 10.9% (n = 12) as men, 8.2% (n = 9) as trans men, 5.5% (n = 6) as not listed, and 3.6% (n = 4) as agender. Among cisgender participants, 65.5% (n = 74) identified as women, 32.7% (n = 37) as men, and 1.8% (n = 2) as not listed.
With the exception of annual household income, we found no significant differences between cisgender and gender-diverse participants by key sociodemographic indicators (Table 1). Most participants (n = 155, 69.5%) were located in urban settings, and 54 (24.2%) reported living on a reservation. Nearly 80% of all participants had at least some college education. Approximately 42% of participants reported being employed either full-time or part-time, and 39% reported other employment. Seventy-six percent of all participants rated their health as excellent, good, or very good, and most participants (n = 199, 89.2%) had health insurance.
Health Care Access
Both cisgender and gender-diverse participants had at least some experience with difficulties in accessing quality health care across all indicators (Figure). Finances, lack of psychologists/other mental health support, and lack of psychological support groups for Two Spirit and LGBTQ+ communities were the top 3 experienced barriers to quality care for both groups, with personal finances being the top barrier. Participants wrote in that finances were a source of concern in combination with health insurance constraints. One participant noted, “I’m living out of state of my parent’s insurance,” while another participant said, “Finances limit me to what is covered on insurance.”
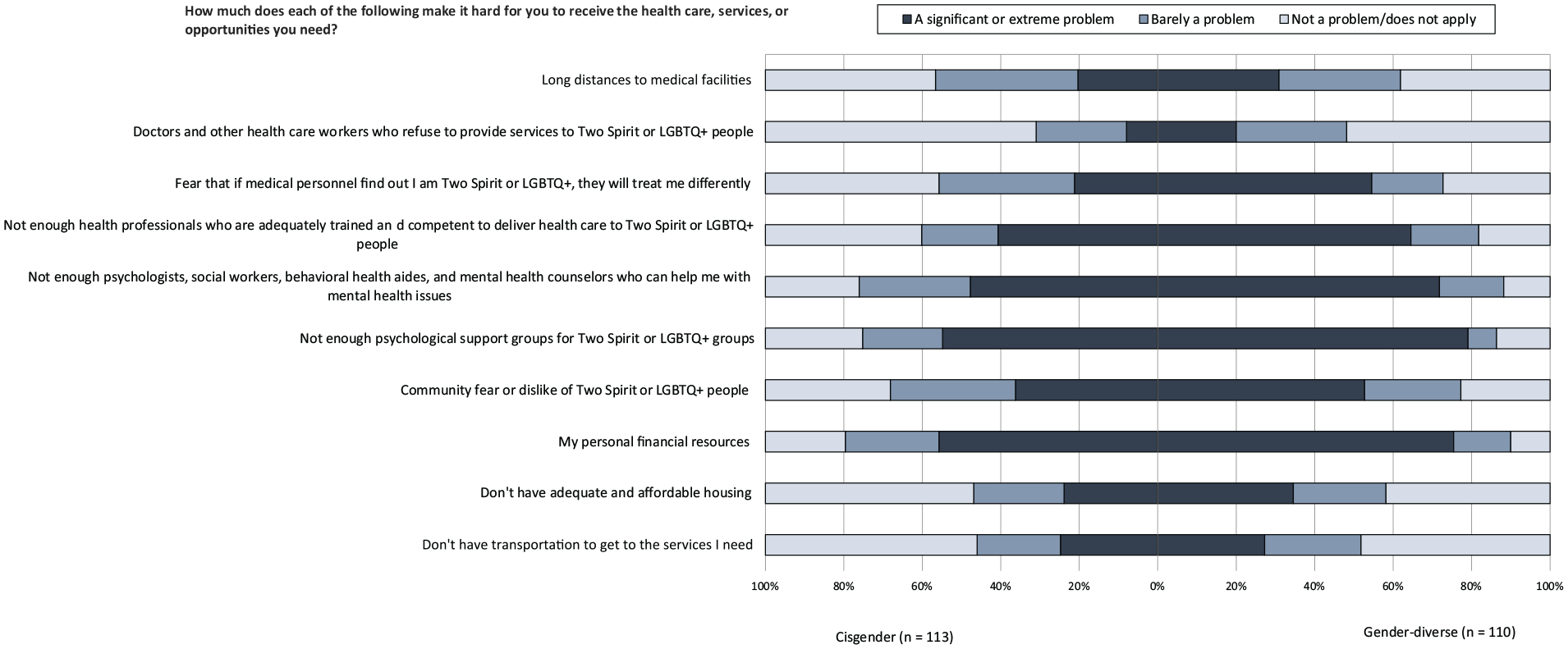
Perceived difficulties of cisgender and gender-diverse American Indian and Alaska Native people (n = 223) in accessing quality health care, by barriers to care, Pride and Connectedness Survey, United States, 2020. Abbreviation: LGBTQ+, lesbian, gay, bisexual, transgender, queer, and questioning.
Gender-diverse participants were more likely than cisgender participants to report difficulties accessing quality care for nearly all questions on the scale (Table 2). While 158 (70.9%) participants reported a lack of adequately trained health professionals in Two Spirit and LGBTQ+ care as a barrier to care, gender-diverse participants were significantly more likely to have experienced this barrier than their cisgender peers (adjusted odds ratio [aOR] = 2.8; 95% CI, 1.7-4.8; P < .001). Expanding on this concern, participants wrote in that being Indigenous is an important aspect of who they are and impacts the way they feel seen and heard within the health care system:
Differences between AI/AN Two Spirit and LGBTQ+ cisgender and gender-diverse participants in responses to health care access indicators from the Pride and Connectedness Survey, United States, 2020
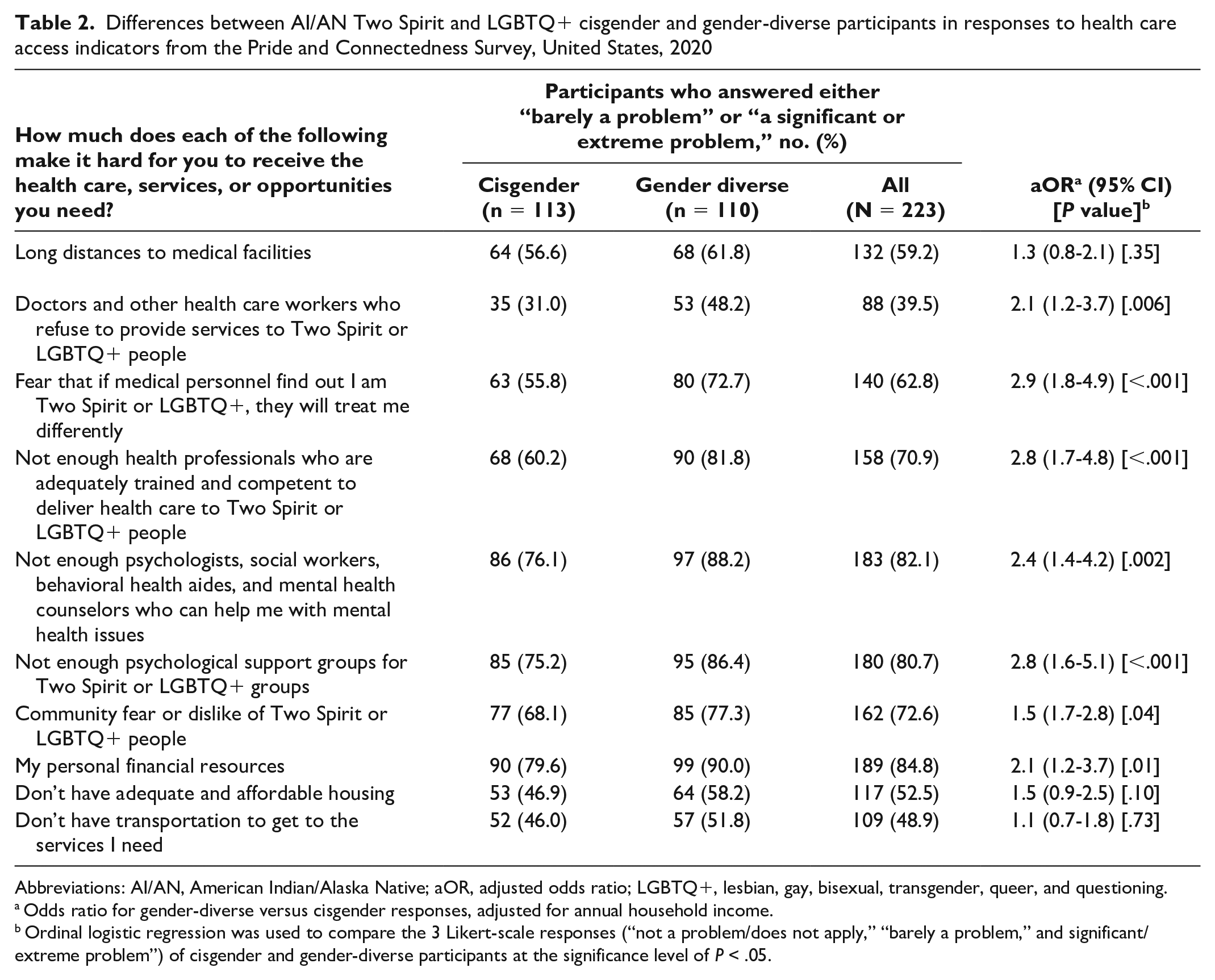
Abbreviations: AI/AN, American Indian/Alaska Native; aOR, adjusted odds ratio; LGBTQ+, lesbian, gay, bisexual, transgender, queer, and questioning.
Odds ratio for gender-diverse versus cisgender responses, adjusted for annual household income.
Ordinal logistic regression was used to compare the 3 Likert-scale responses (“not a problem/does not apply,” “barely a problem,” and significant/extreme problem”) of cisgender and gender-diverse participants at the significance level of P < .05.
I’ve had non-Natives [providers] for the most part and although they may be used to working with Natives, I can’t determine whether they truly can grasp the experience of a Native who identifies as LGBTQ+ and/or Two Spirit.
Health care providers in general seem to know little to none about Indigenous identity.
My health care provider is a middle-aged White woman. She does not fully understand the dynamics of the Native community, let alone the history of the Two Spirit community.
Nearly 73% of gender-diverse participants feared their health care providers would treat them differently if they learned of their gender identity/sexual orientation, compared with 55.8% of cisgender participants (aOR = 2.9; 95% CI, 1.8-4.9; P < .001). One participant wrote about difficulties interacting with medical staff, stating: It is in how they interact with me and when I speak about me being Two Spirit and being a trans woman they have this deer-in-a-headlight look that they don’t realize is on their face when we were talking about this, but I have to find the higher road access and just ignore it because my medical needs are very important. Also, one time they just automatically marked me off as Asian and I had to correct them and told them I was Native American. They didn’t ask me or anything; they just marked me as an Asian.
Another participant elaborated on a recent experience with a mental health professional: I recently had to stop seeing my counselor because she has been really Survivor blaming, anti-Indigenous . . . and not good with my gender and sexual identities, as though she was just keeping her heteronormative agenda to herself except for in certain situations after my break-up with my ex. I need to find a counselor who is affirming in both my Indigenous identity as well as my gender identity and sexuality and trauma. I really need to process the abuse of my last relationship.
While 39.5% of all participants reported health care providers refusing care to 2SLGBTQ+ patients as a problem, the proportion increased to 48.2% for gender-diverse participants, compared with 31.0% for cisgender participants (aOR = 2.1; 95% CI, 1.2-3.7; P = .006). Nearly 60% (n = 132) of all participants reported that they experienced at least some difficulties in accessing care because of long distances to facilities, but we found no significant difference between cisgender and gender-diverse participants (aOR = 1.3; 95% CI, 0.8-2.1; P = .35). Many of the write-in responses reinforced these challenges AI/AN Two Spirit and LGBTQ+ people face when seeking and accessing care.
Discussion
With regard to geographic location (rural/on reservation vs urban/regional location) and health care coverage, the demographic breakdown of the study participants mirrored that of the general AI/AN population as well as the AI/AN LGBTQ+ community throughout the United States15-18; only self-rated health was slightly higher than the larger AI/AN LGBTQ community. 19 However, our findings on health care access illustrate noteworthy gaps in the health care system, regardless of location, among AI/AN 2SLGBTQ+ people particularly in obtaining quality care that fulfills the health needs of these communities. These gaps often perpetuate poor health outcomes and lack of engagement in health care. 20 While many participants had health insurance and had accessed care in the past, the lack of quality care and costs beyond health insurance (particularly costs not often covered by health insurance, such as gender-affirming medications or surgeries) often deter people from continuing care, rendering the experience of care itself a barrier to continuation of care.20,21 As one study participant wrote, “I have a lot of institutional fatigue and medical burnout from years of bad experiences.” Although the results of our study are similar to the results of non-Native LGBTQ+ reports,20,22 the unique health care needs of AI/AN 2SLGBTQ+ people must be considered when training health care providers and staff in specialty care, especially given the demonstrated pride and sense of community participants feel toward their Indigenous identity.
While health care providers working in Native health care settings receive some training in Indigenous culture, many do not receive training in Two Spirit and LGBTQ+ care or the limitations of colonial approaches to gender and sexuality as they relate to Indigenous concepts, including the nuances of Two Spirit identity, which transcends gender identity. 3 Moreover, the participants’ experienced fear associated with gender identity/sexual orientation exposure in the health care system echoes the findings of national surveys from 2015 1 and 2020, 23 reaffirming the need for gender-affirming environments in the health care system, especially when considering the unique health care needs of gender-diverse people. As some participants in our study indicated, their health care providers were unsure and unaware of how to treat and care for them once their gender identity was disclosed. The significant differences between cisgender and gender-diverse responses across almost all indicators in this scale exemplify the additional need for health care providers who understand and are experienced in caring for gender-fluid people. Engaging in simple yet effective strategies that enhance the patient–provider relationship, such as improving patient–provider communication through cultural appreciation and celebration, using culture as treatment, collecting current gender and pronouns at intake, and creating inviting/inclusive spaces, can improve care participation and health outcomes for AI/AN 2SLGBTQ+ people.24-26
A lack of resources for mental health services was one of the most cited experienced barriers to care for both cisgender and gender-diverse participants, illustrating a disparity in mental health providers not only who are trained to address the mental health concerns of AI/AN 2SLGBTQ+ people but also who are Indigenous and understand what it means to be Two Spirit and/or LGBTQ+. The mental health concerns of people who identify as LGBTQ+ are well documented and include higher rates of depression, suicidal ideation, and suicide attempts than non–LGBTQ people. 20 Given the higher rates of these mental health concerns, coupled with the collective historical trauma AI/AN 2SLGTBTQ+ communities face as a result of colonization and continued oppressive colonial practices, including transphobia and homophobia, health care providers should be equipped with the knowledge, compassion, and tools to facilitate appropriate intervention for those seeking mental health services within the context of AI/AN culture. Furthermore, provided the historical prominence of roles that Two Spirit people played within many Native nations prior to colonization, the diversity of gender and sexual orientation must be approached in the health care setting using a culturally relevant, strength-based framework rooted in Indigenous knowledge and community inclusiveness.23,24
Limitations
Two limitations should be considered when interpreting these results. First, because of the survey design, sampling method, and online implementation, our study biased the sample toward younger, more technologically savvy participants, potentially producing selection bias. Although the survey was hacked, we believe 2-layer ReCaptcha and participant eligibility verification would mitigate these concerns should the study be replicated. Second, because of the small sample size, our results may not be generalizable to all AI/AN people or Native/Tribal regional differences. However, the results of the study are informative for future public health practice and suggest that further investigation and exploration of these topics, potentially with a larger sample, would be beneficial.
Conclusion
The findings from this study have implications for the public health action and policies relating to health care services for AI/AN Two Spirit and LGBTQ+ communities. More training for health care providers and inclusive, culturally responsive gender-affirming spaces are essential in advancing health care access and reducing health-related disparities. Likewise, a shift from systemic colonial health care practices as well as improved mental health services that acknowledge the lived experiences of AI/AN gender-diverse people will improve both access to care and overall well-being for all 2SLGBTQ+ people and Indigenous communities.
Footnotes
Acknowledgements
The authors acknowledge the Two Spirit and LGBTQ+ community who participated in this survey, as well as the Alaska Native Tribal Health Consortium HIV/STI Prevention Program, for their foundational work in this area that made this survey possible.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this project was made possible by the Indian Health Service and Minority HIV/AIDS Fund.