
Abstract
Objective:
Immigrants typically experience poor health outcomes after disasters but are often excluded in disaster studies. We assessed physical and mental health outcomes among Houston-area Vietnamese American residents after Hurricane Harvey and hurricane-related characteristics associated with poor health outcomes.
Methods:
We conducted in-person structured surveys among 120 Vietnamese Americans from November 2018 through February 2019. We used the physical and mental component scores of the 12-Item Short-Form Health Survey to assess health outcomes. We used descriptive statistics for health outcomes and hurricane-related effects and examined the associations between hurricane-related characteristics and health outcomes.
Results:
Overall mean (95% CI) physical and mental component scores were 39.8 (29.7-49.9) and 32.6 (27.6-37.6), respectively. The odds of poor physical health poststorm were significantly higher among participants reporting ≥5 versus <5 depressive symptoms (odds ratio [OR] = 3.04; 95% CI, 1.11-8.29; P = .03) and significantly lower among participants with versus without health insurance (OR = 0.25; 95% CI, 0.09-0.71; P = .01). The odds of experiencing poor mental health more than a year after the hurricane were significantly higher among those sustaining versus not sustaining a serious injury/illness because of the hurricane (OR = 3.34; 95% CI, 1.12-9.94; P = .03) and among those who were married/partnered versus not married/partnered (OR = 4.16; 95% CI, 1.32-13.07; P = .02). Receiving versus not receiving free health care services after the hurricane and having high versus low levels of acculturation protected against poor mental health (P < .05 for both).
Conclusions:
Our findings highlight the inequalities of postdisaster health outcomes in this immigrant population and emphasize the need for improved disaster recovery programs that account for these factors.
On August 25, 2017, Hurricane Harvey made landfall as a category 4 hurricane. It brought widespread flash flooding across most of Harris County, Texas, resulting in a third of the area being under water. 1 The hurricane destroyed >12 000 homes and affected 13 million people in Kentucky, Louisiana, Mississippi, Tennessee, and Texas.2-4 After Hurricane Katrina, Hurricane Harvey ranked as the second-costliest storm to mainland United States since 1990. 5
Home to a rapidly growing population of Asian Americans, the Houston, Texas, metropolitan area has the second-largest Vietnamese community in the country: >90 000 Vietnamese immigrants reside in the area. 6 However, little is known about their Hurricane Harvey experiences and the impact of the storm on their health. Immigrants have a limited capacity to prepare for, respond to, or recover from disasters and, thus, are particularly vulnerable to their ill effects.7,8 Coupled with low levels of English-language skills, social acculturation, and socioeconomic status, immigrants are more prone than other US residents to poor recovery and poor physical and mental health outcomes after a disaster.9-19 In 2019, 65% of Vietnamese immigrants aged ≥5 years had limited English proficiency, and postdisaster challenges among immigrants with limited English fluency, especially Vietnamese immigrants, are evident.20,21 One year poststorm, Hurricane Katrina–affected Vietnamese immigrants experienced displacement, property loss, and trauma, which led to a concerning 26% experiencing partial or full posttraumatic stress disorder, particularly among those who lost property. 22 They also experienced shortages in access to health care and medications, and 40% reported difficulties in obtaining health care 1 year after the hurricane.23,24
Literature on flooding disasters in Texas highlighted that non–US citizens and Hispanic people were more likely than non-Hispanic White residents to experience poor health postdisaster and that people with low socioeconomic status had an elevated risk for posttraumatic stress as compared with others.1,25,26 Studies concluded that exposure to Hurricane Harvey and property damages were associated with an increase in the number of posttraumatic stress symptoms, repeated disturbing memories of the hurricane, and poor physical and mental health.1,26 Despite evidence of the negative effects of Hurricane Harvey on the residents along the storm’s path, not much is known about its impact on the area’s Vietnamese population. Our study examined the effects of Hurricane Harvey on Vietnamese residents, who are often excluded from postdisaster studies, by addressing 2 questions: (1) How did Hurricane Harvey affect the physical and mental health of Vietnamese American residents of the Houston metropolitan area? and (2) What Hurricane Harvey–related consequences and sociodemographic characteristics were associated with poor health outcomes among Vietnamese American residents of Houston after the storm?
Methods
Data Collection and Sample
We conducted 120 in-person interviews using a structured survey from November 2018 through February 2019. In partnership with Boat People SOS (BPSOS)–Houston, a nonprofit organization that primarily serves first-generation Vietnamese immigrants in the Houston area, we selected participants randomly from a list of 600 BPSOS–Houston clients. Participant selection criteria were (1) being a Vietnamese American aged ≥18 years, (2) having experienced Hurricane Harvey, and (3) having received some hurricane-related assistance (directly or indirectly) through BPSOS–Houston. The survey included questions about hurricane-related damages and losses, self-rated health, and health care after the hurricane. We also collected information on sociodemographic characteristics, social support, English-language skills and language preference, and other social vulnerability domains. Interviewers were volunteers trained by the principal investigator (M.D.) and conducted interviews in English or Vietnamese, based on the participant’s preference. The institutional review board of Tulane University reviewed and approved this study.
Although we did not directly ask about nativity (US-born vs non–US-born), the mission of BPSOS–Houston and the age range of our sample provide confidence that our data accurately reflect the narrative of Vietnamese immigrants. First, BPSOS–Houston primarily serves first-generation immigrants, especially those of limited English proficiency. Second, the influx of Vietnamese immigrants to the United States began in 1975; the mean age of the sample (>43 years) indicates arrival in the United States as a child in 1975 or later. Fewer than 12% were aged <43 years, but they are unlikely to be second-generation Vietnamese Americans; alternatively, they may be immigrants as part of family-sponsored migration processes. Because of the historical trends and pathways to residency of Vietnamese immigrants in the United States, it is unlikely that many study participants were born to US-born parents of Vietnamese descent.
Variables
Our outcomes of interest were postdisaster physical health and mental health. We assessed both outcomes by component scores of the 12-Item Short-Form Health Survey (SF-12) version 1.27,28 The SF-12, which assesses self-rated mental and physical health, consists of 8 indicators: physical function, role physical, bodily pain, and general health for the physical component score (PCS) indicators; vitality, social functioning, role emotional, and mental health for the mental component score (MCS) indicators. We derived the PCS and MCS, ranging from 0 (poorest) to 100 (best), from these 8 indicators using methods by Hays et al and Ware et al.27-29 Ware et al developed the SF-12 instrument based on the longer 36-Item Short-Form Health Survey in association with the Medical Outcomes Study.28,30 Typically, the standardized scores are compared with a national norm of 50; therefore, a score <50 is considered below the US average. 31 However, we generated 2 binary variables—poor physical health and poor mental health—using the sample medians of the PCS (40.0) and MCS (32.9) to reflect disparities among participants beyond their tendency toward lower-than-national norms.
The dichotomization of the outcomes was motivated by 2 reasons: (1) the results would help identify those most vulnerable (ie, those with low PCS and/or MCS relative to others) and provide straightforward interpretations of the implications for policies and programs; and (2) given the small sample size, binary outcomes may be more likely to detect differences between outcome categories than between incremental increases in continuous outcomes. Furthermore, Vietnamese Americans have disproportionately poorer health status than other Asian American population groups and national norms. 32 Rather than using national averages as cutoffs, which would reiterate poor overall health outcomes among the study sample as compared with the general population, we operationalized poor physical health and poor mental health at the sample median to show that disparities exist even within this subpopulation group. Also, operationalizing poor physical health and poor mental health at the sample median rather than the sample mean helped avoid any potential outlier biases. We coded participants with a PCS or MCS below the median score as 1; otherwise, they were coded as 0.
Key independent variables were those related to Hurricane Harvey: a damaged home (yes/no), any sustained injury or illness from the storm (yes/no), receipt of any free health care services after the storm (yes/no), and depressive symptoms (≥5 or <5 symptoms) experienced at the time of interview. We coded these storm-related variables as binary (1 = yes, 0 = no). When a participant indicated that the level of damages to his or her house and in-home assets was beyond the minimal level, we categorized this damage as sustained. We derived the depressive symptom score from 18 factors that convey emotional distress that participants may have experienced within 7 days before data collection. The factors centered on loss of appetite, loss of concentration, and exposure to persistent pain, as well as the exhibition of hopelessness, tiredness, sadness, frustration, discouragement, desperation, exhaustion, disgrace, anger, and craziness. We dichotomized responses from each participant as high or low level of depressive symptoms (≥5 vs <5), using the sample median cutoff of 5 symptoms, rather than the mean, to avoid potential outlier bias.
Sociodemographic characteristics were age, sex, monthly income, marital status, education level, religious affiliation, and acculturation level. We coded all basic sociodemographic characteristics as binary variables of 0 or 1, except for religious affiliation: age (<65 or ≥65 years), sex (female or male), monthly income (<$1500 or ≥$1500), marital status (married or living with spouse/partner and never married or divorced/widowed), and highest education level (≤12th or >12th grade). We categorized religion as Catholic, Buddhist, or no religion/other. We selected the age cutoff of 65 years to distinguish between older adults and working-age adults. We determined acculturation levels according to English-language fluency and cultural preferences selected by participants. We first derived an overall acculturation score for each participant through factor analysis of one’s responses. Then we grouped levels of acculturation as low (0; <−0.0022766) or high (1; ≥−0.0022766) using the median acculturation score. Higher scores indicate higher levels of assimilation to US society and better English proficiency.
We used binary coding of no (0) and yes (1) to identify health care access and social capital characteristics: has health insurance, employed before the hurricane, living at the same address for ≥5 years, had routine physical examination within the 12 months before the interview, able turn to someone for comfort or support, and able to obtain help during emergencies. We measured the ability to turn to someone for comfort or support by whether participants had ≥1 person in their social network to whom they could turn during a negative event. We measured the ability to get help during emergencies by participants’ perceived ability to obtain help within their social network during a crisis, comparable with others in the community.
Analysis
We conducted descriptive summary statistics calculations and bivariate and multivariable analyses using Stata version 16 (StataCorp LLC). We used bivariate analyses to assess differences in physical and mental health outcomes by Hurricane Harvey–related variables and sociodemographic characteristics. We used multivariable logistic regression modeling to assess the factors associated with post–Hurricane Harvey physical and mental health outcomes while controlling for sociodemographic factors. We calculated odds ratios (ORs) and 95% CIs for each variable within each predictive model, with P ≤ .05 indicating significance.
Ancillary analysis operationalizing the outcomes and hurricane-related predictor variables as continuous measures produced similar results in terms of substance and significance, providing confidence in our decision to dichotomize these originally continuous variables. The direction of the relationships between the outcome and predictor variables were the same, regardless of whether we used continuous or dichotomous forms.
Results
Although the prevalence of home damage from the storm was high (75.8%), only 24.2% of participants experienced injuries or illness due to the storm. After the storm, 52.5% experienced ≥5 depressive symptoms (Table 1). Perceived social support was high among participants: 80.0% indicated that they could turn to someone for comfort or support, and 65.8% indicated that they could obtain help during an emergency.
Hurricane Harvey–related and sociodemographic characteristics among a sample of Vietnamese Americans (N = 120) in Houston, Texas, 2018-2019 a
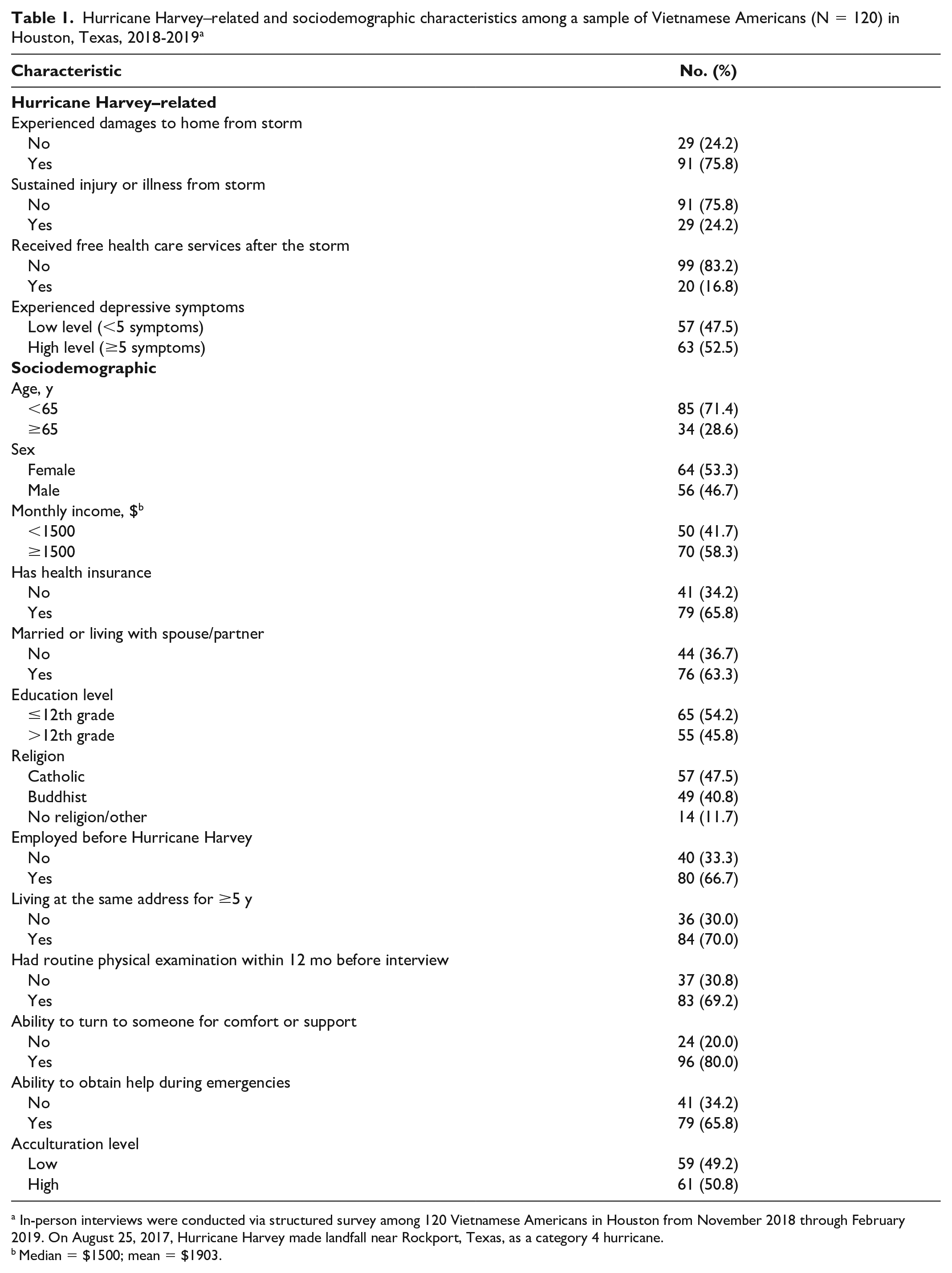
In-person interviews were conducted via structured survey among 120 Vietnamese Americans in Houston from November 2018 through February 2019. On August 25, 2017, Hurricane Harvey made landfall near Rockport, Texas, as a category 4 hurricane.
Median = $1500; mean = $1903.
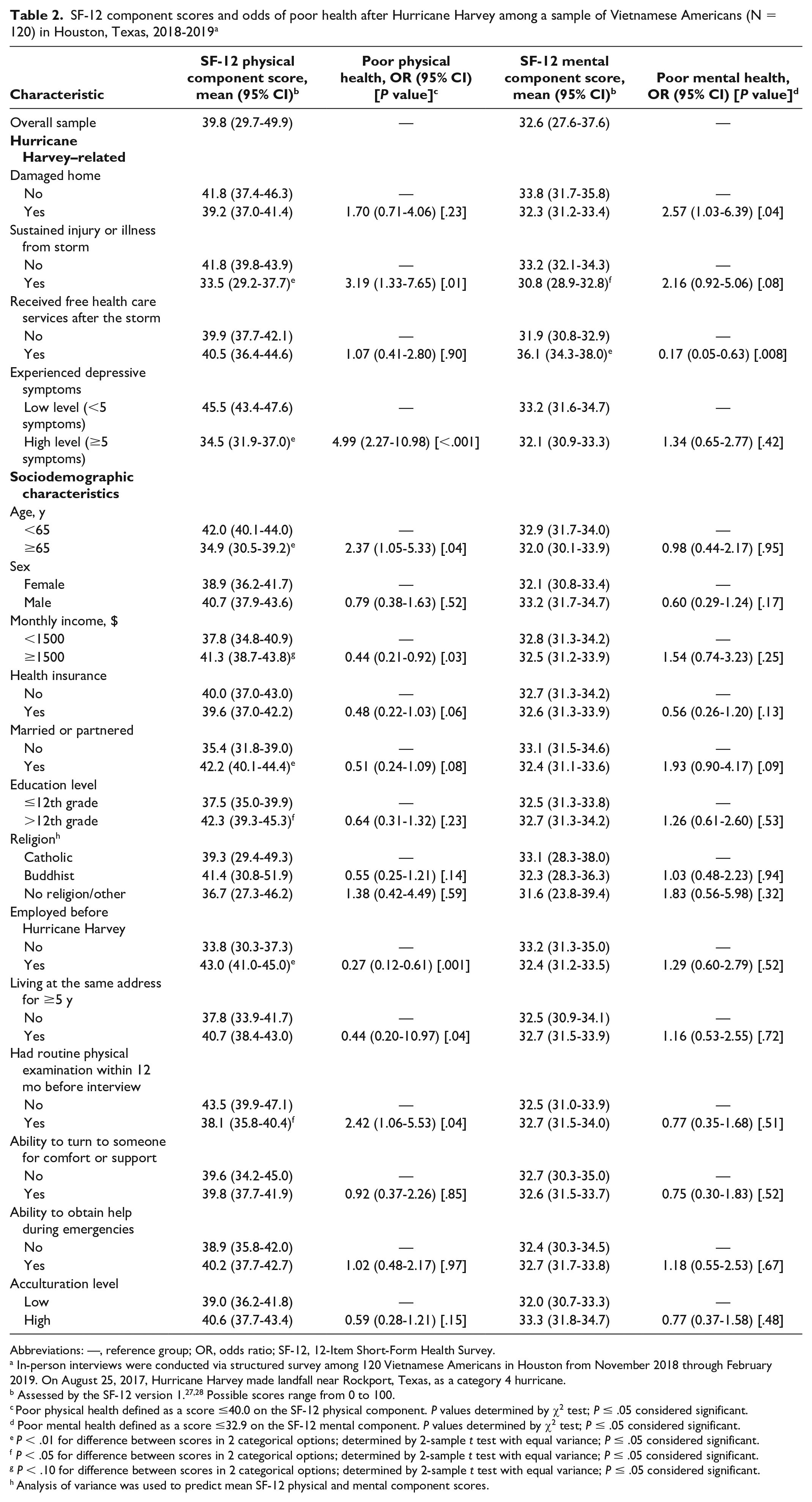
The mean (95% CI) PCS and MCS were 39.8 (29.7-49.9) and 32.6 (27.6-37.6), respectively (Table 2). The likelihood of poor mental health was >2 times higher among participants with damaged homes than without damaged homes (OR = 2.57; 95% CI, 1.03-6.39; P = .04). As compared with those without serious injury or illness, participants who sustained serious injury or illness from the storm were >3 times as likely to have poor physical health (OR = 3.19; 95% CI, 1.33-7.65; P = .01) after the storm. The MCS was lower among participants who had versus had not sustained a serious injury or illness from the storm (30.8 vs 33.2; P = .04) and higher among those who received versus did not receive free health care services after the storm (36.1 vs 31.9; P < .001). Participants who experienced ≥5 versus <5 depressive symptoms were almost 5 times as likely to report poor physical health (OR = 4.99; 95% CI, 2.27-10.98; P < .001).
SF-12 component scores and odds of poor health after Hurricane Harvey among a sample of Vietnamese Americans (N = 120) in Houston, Texas, 2018-2019 a
Abbreviations: —, reference group; OR, odds ratio; SF-12, 12-Item Short-Form Health Survey.
In-person interviews were conducted via structured survey among 120 Vietnamese Americans in Houston from November 2018 through February 2019. On August 25, 2017, Hurricane Harvey made landfall near Rockport, Texas, as a category 4 hurricane.
Poor physical health defined as a score ≤40.0 on the SF-12 physical component. P values determined by χ2 test; P ≤ .05 considered significant.
Poor mental health defined as a score ≤32.9 on the SF-12 mental component. P values determined by χ2 test; P ≤ .05 considered significant.
P < .01 for difference between scores in 2 categorical options; determined by 2-sample t test with equal variance; P ≤ .05 considered significant.
P < .05 for difference between scores in 2 categorical options; determined by 2-sample t test with equal variance; P ≤ .05 considered significant.
P < .10 for difference between scores in 2 categorical options; determined by 2-sample t test with equal variance; P ≤ .05 considered significant.
Analysis of variance was used to predict mean SF-12 physical and mental component scores.
Participants aged ≥65 versus <65 years were more likely to report poor physical health (OR = 2.37; 95% CI, 1.05-5.33; P = .04). When compared with participants who were not married or partnered, those who were married or partnered had a higher PCS (35.4 vs 42.2; P < .001). Participants with >12th-grade education versus ≤12th-grade education had a higher PCS (42.3 vs 37.4; P = .01), and those who were unemployed versus employed before the storm had a lower PCS (33.8 vs 43.0; P < .001). Participants who had a routine physical examination within 12 months before the interview were more likely than those without one to experience poor physical health (OR = 2.42; 95% CI, 1.06-5.53; P = .04) (Table 2).
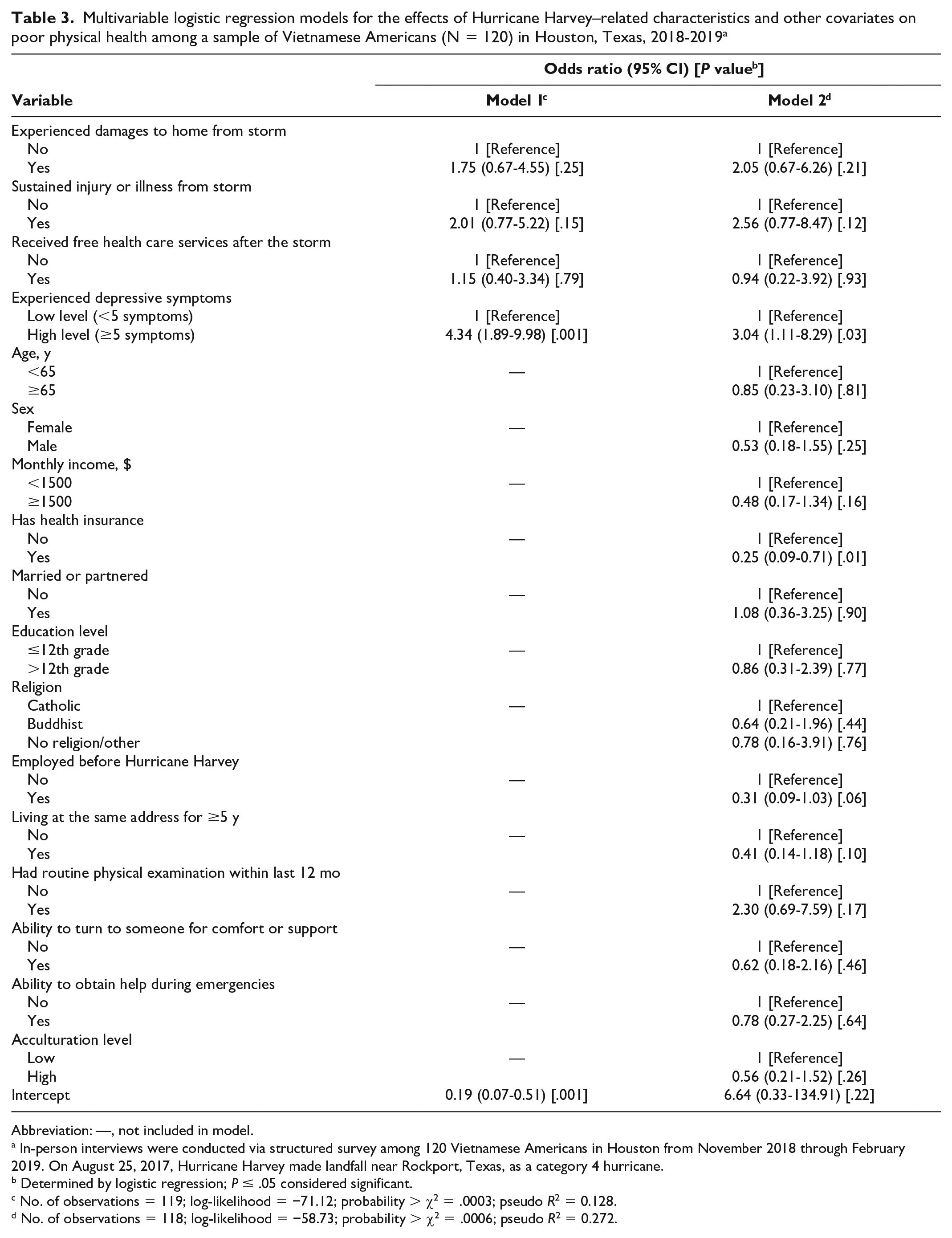
In model 1 (Table 3), which examined storm-related characteristics and physical health, the odds of poor physical health were significantly higher among participants with ≥5 versus <5 depressive symptoms (OR = 4.34; 95% CI, 1.89-9.98; P = .001). Controlling for other characteristics, in model 2 the odds of poor physical health were significantly higher among those with ≥5 versus <5 depressive symptoms (OR = 3.04; 95% CI, 1.11-8.29; P = .03). Having health insurance protected against poor physical health (OR = 0.25; 95% CI, 0.09-0.71; P = .01) among study participants when controlling for other key characteristics.
Multivariable logistic regression models for the effects of Hurricane Harvey–related characteristics and other covariates on poor physical health among a sample of Vietnamese Americans (N = 120) in Houston, Texas, 2018-2019 a
Abbreviation: —, not included in model.
In-person interviews were conducted via structured survey among 120 Vietnamese Americans in Houston from November 2018 through February 2019. On August 25, 2017, Hurricane Harvey made landfall near Rockport, Texas, as a category 4 hurricane.
Determined by logistic regression; P ≤ .05 considered significant.
No. of observations = 119; log-likelihood = −71.12; probability > χ2 = .0003; pseudo R2 = 0.128.
No. of observations = 118; log-likelihood = −58.73; probability > χ2 = .0006; pseudo R2 = 0.272.
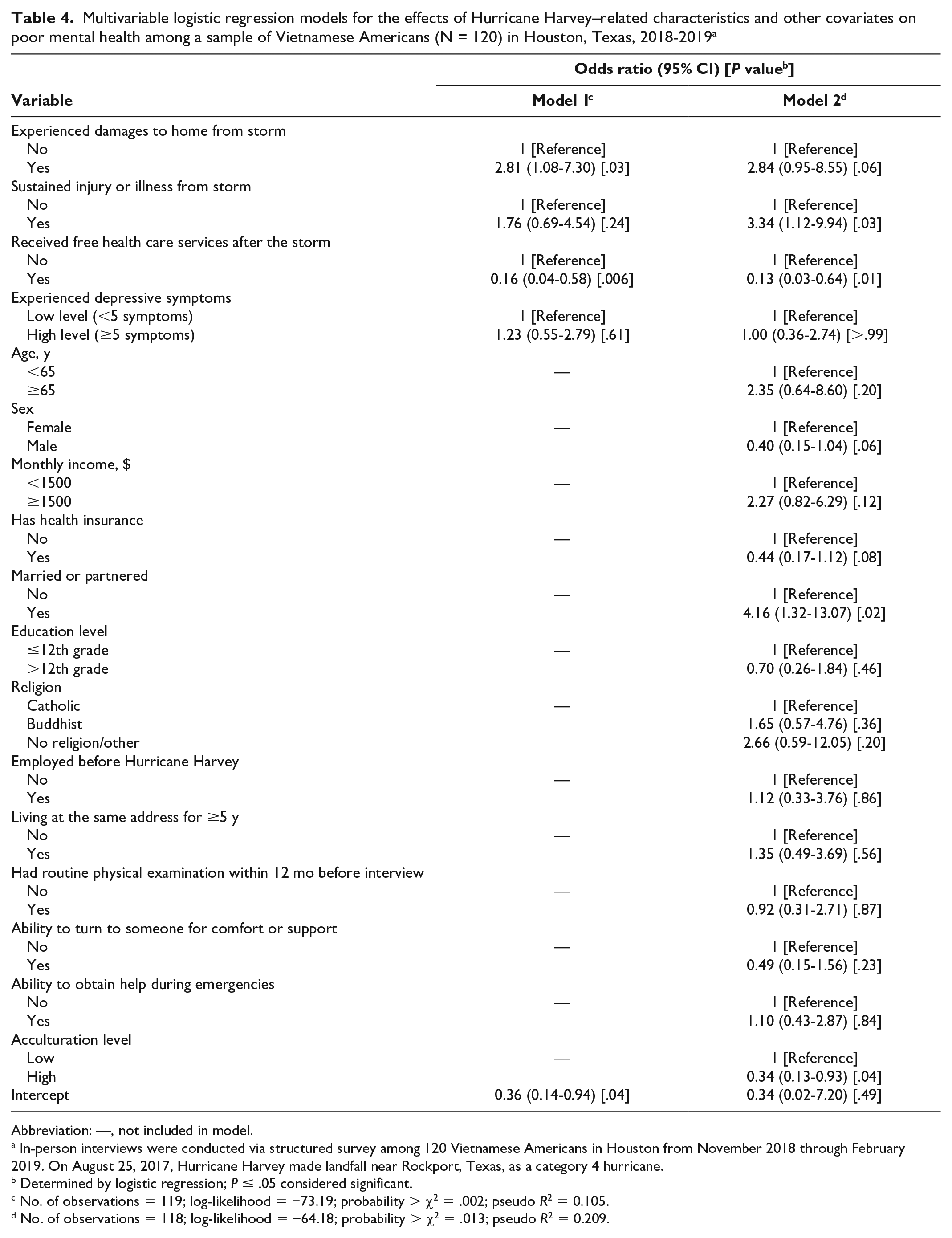
In model 1 (Table 4), which examined storm-related characteristics and mental health, receiving free health care services after the storm protected against poor mental health (OR = 0.16; 95% CI, 0.04-0.58; P = .006), and experiencing home damages due to the storm was positively associated with poor mental health (OR = 2.81; 95% CI, 1.08-7.30;P = .03). Receiving free health care services after the storm still protected against poor mental health in model 2 (OR = 0.13; 95% CI, 0.03-0.64; P = .01), and experiencing home damages due to the storm remained positively associated with poor mental health (OR = 2.84; 95% CI, 0.95-8.55;P = .06), although the finding was no longer significant. The odds of having poor mental health increased from model 1 to model 2 (OR = 3.34; 95% CI, 1.12-9.94; P = .03) among those sustaining a serious injury or illness because of the storm. Participants who were married or had a partner versus not were significantly more likely to have poor mental health (OR = 4.16; 95% CI, 1.32-13.07; P = .02). Finally, high levels of acculturation protected against poor mental health (OR = 0.34; 95% CI, 0.13-0.93; P = .04).
Multivariable logistic regression models for the effects of Hurricane Harvey–related characteristics and other covariates on poor mental health among a sample of Vietnamese Americans (N = 120) in Houston, Texas, 2018-2019 a
Abbreviation: —, not included in model.
In-person interviews were conducted via structured survey among 120 Vietnamese Americans in Houston from November 2018 through February 2019. On August 25, 2017, Hurricane Harvey made landfall near Rockport, Texas, as a category 4 hurricane.
Determined by logistic regression; P ≤ .05 considered significant.
No. of observations = 119; log-likelihood = −73.19; probability > χ2 = .002; pseudo R2 = 0.105.
No. of observations = 118; log-likelihood = −64.18; probability > χ2 = .013; pseudo R2 = 0.209.
Discussion
We found that the PCSs and MCSs among our study sample were lower than national mean scores. 31 More so, the MCSs of Vietnamese American participants were lower than those in a study that used the SF-12 among 1086 Texas Gulf Coast residents exposed to Hurricane Harvey. 33 Our sample also had lower PCSs and MCSs than those in a study that examined SF-12 outcomes among 153 racial and ethnic minority Houston-area residents with low socioeconomic status affected by Hurricane Harvey. 34
More than half of participants had ≥5 depressive symptoms, and they were more likely to experience poor physical health as compared with others, highlighting the potential vulnerability of cascading health issues due to poststorm psychological distress. Receiving free health care services after the storm decreased the likelihood of poor mental health, which is not surprising, because access to free services may alleviate emotional and financial burdens caused by the storm. People with versus without health insurance may be more likely to seek health care services during the onset of symptoms; thus, having health insurance may have protected against poor physical health in our study sample.
High acculturation levels may alleviate distress by increasing knowledge of and access to recovery resources and overcoming the detrimental impacts of home damages. The same rationale can be applied to why the key predictor of injury or illness due to the storm in the multivariable logistic regression models for poor mental health was not significant in model 1 but was significant in model 2, when we controlled for other factors. Furthermore, recovering from injury or illness may take longer than rebuilding a home; thus, the effect of recovery on health remained 1 year after the storm when we accounted for other factors.
In the multivariable logistic regression models for poor mental health, the key predictor was storm damages to home. The change in its level of significance, after accounting for Hurricane Harvey–related variables and sociodemographic characteristics, may have been due to stronger relationships between (1) mental health outcomes and (2) marital status and acculturation levels as compared with other key predictor variables. Furthermore, in a small sample size (N = 120), the association between storm damages and mental health outcome was likely masked when control variables were included; therefore, meaningful suppressor effects are observed rather than misspecification due to multicollinearity among variables in our analysis. We further assessed multicollinearity in the logistic regression models by using the uncentered variance inflation factor (VIF) metric. None of the VIF values were high, while the mean VIF value was 2.93, which indicated that multicollinearity was not a concern. In addition, a correlation matrix revealed that predictor variables were not highly correlated to one another.
Our findings suggest that Houston-area Vietnamese immigrants may be vulnerable to the health effects of a natural disaster for a long time after the disaster. More than a year after the storm, about half of participants had ≥5 depressive symptoms, which highlights the need to examine the long-term mental health effects of natural disasters. The burden of rebuilding and disruptions to daily life may have contributed to a high level of depressive symptoms that then cascaded to poor health outcomes among study participants. Such results emphasize that response and recovery efforts for Vietnamese residents should be sensitive to the unique needs of immigrants, including immediate physical health and safety and psychological well-being, and account for acculturation level. Future partnerships between government agencies and community organizations such as BPSOS–Houston may help improve access to and uptake of recovery resources among Vietnamese residents and alleviate storm-related distress.
Inconsistent with existing literature, our findings showed that women were not at higher risk than men for poor mental health after a disaster.33-36 Traditionally, after disasters, women maintain responsibilities inside the home (eg, child care 36 ), and Vietnamese families expect females to maintain household activities and prioritize family responsibilities over their own needs and health. 23 Hurricane Katrina–related studies revealed patterns of poor mental health among women, so it was surprising that we did not observe the same among Vietnamese women in our study.37,38 Our finding may be due in part to the availability of Vietnamese-serving organizations in the Houston area, such as BPSOS–Houston, which enhanced access to support and resources to alleviate the psychosocial distress typically placed on Vietnamese women affected by disasters.
Our finding that marriage and partnership did not protect against poor mental health conflicts with the findings of previous studies, which revealed that having a spouse or partner before a hurricane protected against mental distress poststorm.39-42
Limitations
Limitations included a small sample size and recruitment from a list of clients from a single organization. The cross-sectional data also did not allow us to assess the physical and mental health status of participants before the storm, which limited causal inferences about the storm’s impacts. Finally, our sample consisted of middle-aged Vietnamese Americans and may not be generalizable to all Vietnamese Americans affected by Hurricane Harvey in Houston.
Conclusion
To our knowledge, our study is the first to assess the effects of Hurricane Harvey on the Vietnamese American population. It adds to the limited literature on the inequalities of postdisaster health outcomes among immigrants and the Vietnamese immigrant population. Larger and more powerful hurricanes are expected to make landfall in the US Gulf Coast region in the coming years,43,44 and the physical and mental health of residents, especially those vulnerable to poor poststorm outcomes, such as Vietnamese Americans, should be prioritized by local public health preparedness practitioners and disaster response entities. Findings emphasize the need for the design and implementation of future disaster interventions that account for the unique vulnerabilities of these populations.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by Tulane University’s Carol Lavin Bernick Faculty Grant and the Tulane Japan Friendship Award with Mai Do, MD, DrPH, as principal investigator.