
Abstract
Objectives
Although research shows that public health is substantially affected during and after disasters, few studies have examined the health effects of Hurricane Harvey, which made landfall on the Texas coast in August 2017. We assessed disparities in physical health, mental health, and health care access after Hurricane Harvey among residents of the Houston–The Woodlands–Sugar Land, Texas, metropolitan statistical area (ie, Houston MSA).
Methods
We used structured survey data collected through telephone and online surveys from a population-based random sample of Houston MSA residents (n = 403) collected from November 29, 2017, through January 6, 2018. We used descriptive statistics to describe the prevalence of physical health/mental health and health care access outcomes and multivariable generalized linear models to assess disparities (eg, based on race/ethnicity, socioeconomic status, disability) in health outcomes.
Results
Physical health problems disproportionately affected persons who did not evacuate (odds ratio [OR] = 0.41; 95% confidence interval [CI], 0.19-0.87). Non-Hispanic black persons were more likely than non-Hispanic white persons to have posttraumatic stress (OR = 5.03; 95% CI, 1.90-13.10), as were persons in households that experienced job loss post-Harvey (vs did not experience job loss post-Harvey; OR = 2.89; 95% CI, 1.14-7.32) and older persons (OR = 1.04; 95% CI, 1.01-1.06). Health care access was constrained for persons whose households lost jobs post-Harvey (vs did not lose jobs post-Harvey; OR = 2.73; 95% CI, 1.29-5.78) and for persons with disabilities (vs without disabilities; OR = 3.19; 95% CI, 1.37-7.45).
Conclusions
Our findings underscore the need to plan for and ameliorate public health disparities resulting from climate change–related disasters, which are expected to occur with increased frequency and magnitude.
Hurricane Harvey made landfall on the Texas coast in August 2017. Harvey was an unprecedented tropical storm; total rainfall for the Houston, Texas, area was 36-48 inches. 1 Rainfall caused flooding across the Houston–The Woodlands–Sugar Land metropolitan statistical area (ie, Houston MSA), resulting in about $125 billion in damages, making it the second costliest disaster in US history, after Hurricane Katrina in 2005. 1 Although research shows that public health is substantially affected during and after disasters, 2 -9 few studies have examined the health effects of Harvey, none of which have been population based.
Persons in racial/ethnic minority groups, older persons, persons with disabilities or infirmities, and persons of low socioeconomic status (SES) disproportionately experience poor health outcomes after disasters occur. 10 -15 Research on Harvey found disparities in flood exposure based on race/ethnicity and SES. 16 -18 For example, after a flood event in El Paso, Texas, non–US citizens (vs US citizens) and persons of Hispanic ethnicity (vs non-Hispanic white persons) were more likely to have physical health problems such as allergies, headaches, coughing and wheezing, and throat, nose, eye, and skin irritations. 10 A literature review published in 2012 concluded that men (vs women) and older persons (vs younger persons) tend to have a higher risk of physical health problems during and after flood events. 2 In addition, women and persons of low SES had an increased risk of having posttraumatic stress (PTS) after Hurricane Ike, which occurred in 2008. 19 In the El Paso study, non–US citizens were more likely to have mental health problems than US citizens. 10
Public health issues resulting from Harvey have been inadequately documented in the literature. Studies have relied on small convenience samples of local residents. At a convention center in Houston, researchers found more than 200 evacuees seeking mental health treatment, many of whom had no access to needed medications. 20 Another study found that many persons who relocated to shelters after Harvey had high levels of anxiety as a result. 21 A survey of 41 persons in the Houston MSA found that hurricane exposure and property damage were associated with increased symptoms of PTS. 22 Although these studies identified health effects resulting from Harvey, they were not based on representative, population-based samples but instead were based on convenience samples. To advance knowledge of Hurricane Harvey’s health effects, we conducted a population-based study based on a random sample of residents in the Houston MSA.
Our study addressed 2 research questions: (1) To what extent did Hurricane Harvey affect the physical health, mental health, and health care access of Houston MSA residents? and (2) How were factors of social vulnerability, disaster experiences, home site effects, and access to aid associated with physical health, mental health, and health care access outcomes among Houston MSA residents, during and soon after Hurricane Harvey?
Methods
Data Collection and Sample
We collected data through telephone and online surveys of a random sample of Houston MSA residents from November 29, 2017, through January 6, 2018. The sampling frame consisted of adults aged ≥18 with cellular telephones in the Houston MSA (n = 1240). Using random-digit dialing within a random sample of cellular telephone numbers across this area, interviewers from a survey research firm screened respondents for eligibility, which was based on permanent residence in the Houston MSA at the time of Hurricane Harvey (August 25, 2017) and the ability to speak Spanish or English (Figure 1). Cellular telephone numbers were important because they allowed us to reach persons who had relocated (temporarily or permanently) because of Harvey. 24 Respondents could take the survey by cellular telephone in English or Spanish; the average time for survey completion was 46 minutes. We augmented the sample with completed surveys from respondents to a representative, probability-based survey focused on flood hazards conducted in 2012; we updated their contact information and recontacted them as part of our 2017 post-Harvey survey. 25,26
Counties of the Houston–The Woodlands–Sugar Land, Texas, metropolitan statistical area, 2017. Data source: The flooded area is based on the Hurricane Harvey Inundation Footprint from the Federal Emergency Management Agency Region 6. 23
Of 988 eligible respondents we contacted, 439 (44.4%) took the survey: 368 were new respondents from the cellular telephone sample and 71 were resurveyed respondents from the 2012 survey (Figure 2). 25 This calculation follows the American Association for Public Opinion Research Cooperation Rate 2 guidelines. 27 We excluded 36 respondents who did not complete at least 50% of the survey items relevant to this analysis, leaving a final sample of 403 survey respondents.
Data collection process for a post–Hurricane Harvey survey in the Houston–The Woodlands–Sugar Land, Texas, metropolitan statistical area (ie, Houston MSA), 2017.
Survey respondents were generally representative of adult residents in the Houston MSA in terms of race/ethnicity, income, and age. The 2016 average annual household income for respondents was $66 400, whereas the 2016 median annual household income for Houston MSA residents was $61 708. 28 The survey sample was 34% non-Hispanic white, 38% Hispanic/Latino, and 19% non-Hispanic black. In the Houston MSA in 2016, non-Hispanic white adults comprised approximately 36%, Hispanic/Latino adults comprised 37%, and non-Hispanic black adults comprised 17% of the adult population. The median age of survey respondents was 49.6; the average age for the adult population in the Houston MSA was 46. 28
We adapted the survey instrument from previously administered post–flood disaster survey instruments. 10,13,29 -31 Through the survey, we collected data from participants on health problems experienced during and after Harvey, lack of access to health care during and after Harvey, and other domains (ie, social vulnerability, disaster experiences, home site effects, and access to aid). We geocoded data on respondents’ home addresses and integrated the data with Federal Emergency Management Agency (FEMA) estimates of the Harvey flood extent for areas surrounding their home sites.
Dependent Variables
We included 3 dichotomous dependent variables: physical health problems, PTS, and lack of access to health care. We assessed data on physical health problems based on respondents’ answers to 24 items about having physical health problems during or any time after Hurricane Harvey. We recoded the variable such that respondents who did not have any physical health problem were coded 0, and respondents who had at least 1 physical health problem were coded 1. We measured PTS by using the Post-Traumatic Stress Disorder Checklist-S (PCL-S), 32 a 17-item self-reported measure that includes questions about experiences that occurred at any time since Harvey. Responses to each item were on a 5-point Likert-type scale, where 1 = not at all, 2 = a little bit, 3 = moderately, 4 = quite a bit, and 5 = very much. Overall scores can range from 17 to 85. Although various thresholds have been used to screen persons for PTS, 32 we used a threshold of 40 based on previous studies assessing disaster-induced PTS. 22,33 Respondents with a PTS score <40 were coded as 0 (no or low PTS), and respondents with a PTS score ≥40 were coded as 1 (high PTS). For the lack of access to health care variable, we coded respondents who had continuous access to health care during or soon after Harvey as 0 and respondents who went without access to health care during or soon after Harvey as 1.
Independent Variables
We classified independent variables into 4 domains: (1) social vulnerability, (2) disaster experiences, (3) home site effects, and (4) access to aid (Table 1).
Survey question and summary statistics for variables analyzed among adult respondents (N = 403) to a post–Hurricane Harvey survey in the Houston–The Woodlands–Sugar Land, Texas, metropolitan statistical area, 2017
aUnmet needs items were as follows: you went without a comfortable place to sleep for some time; you went without adequate drinking water for some time; you went without adequate clothing for some time; you went without a bathroom for some time; you went without running hot water for some time; you went without electricity for some time; you went without adequate food for some time; you went without adequate transportation for some time; you lacked money for living expenses for some time; or you went without clean piped water for some time.
bAdverse events items were as follows: you saw someone drowning or in danger of drowning; you lost a pet or had to abandon one; you worried about crime; you had to perform a dangerous activity; you were stranded in an unsafe place during the disaster; you lost irreplaceable items such as photographs, family mementos; you thought at least once that you might be injured or killed; you worried about family members or friends; you had to split up from household members; you were separated from your children; you experienced unsanitary living conditions; or you experienced crowded living conditions.
cPersonal exposure items were as follows: you were present when major flooding or hurricane damage occurred; you were a victim of a crime; you smelled unpleasant chemical odors; you inhaled smoke from chemical fires; or you made physical or skin contact with chemicals or contaminants.
dDerived using the Federal Emergency Management Agency estimates of Harvey flood extent for areas surrounding respondents’ home sites. 23
eSocial support items were as follows: suggest some action that you should take; give, loan, or offer you money or something else you needed; comfort you with a hug or another sign of affection; let you know they would be around if you needed them; express interest and concern in your well-being; offer or provide you with a place to stay; help you with cleaning up or improving your property; or bring you food or cook for you.
Physical health problems experienced by respondents to a post–Hurricane Harvey survey (N = 403) in the Houston–The Woodlands–Sugar Land, Texas, metropolitan statistical area, 2017
Posttraumatic stress symptoms experienced by respondents to a post–Hurricane Harvey survey (N = 403) in the Houston–The Woodlands–Sugar Land, Texas, metropolitan statistical area, 2017
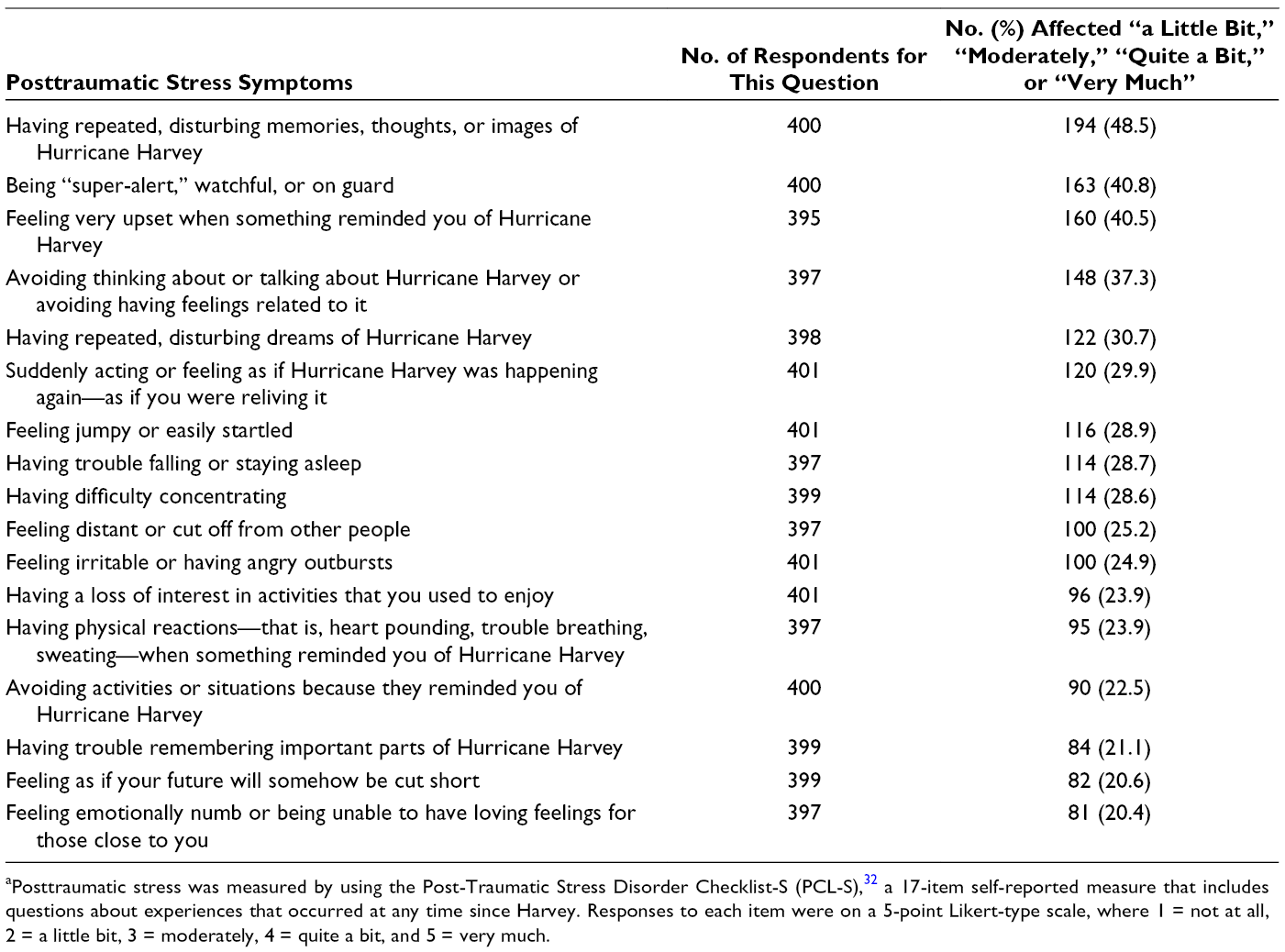
aPosttraumatic stress was measured by using the Post-Traumatic Stress Disorder Checklist-S (PCL-S), 32 a 17-item self-reported measure that includes questions about experiences that occurred at any time since Harvey. Responses to each item were on a 5-point Likert-type scale, where 1 = not at all, 2 = a little bit, 3 = moderately, 4 = quite a bit, and 5 = very much.
Social vulnerability
We treated age as a continuous variable. Female respondents were the reference category (0), and male respondents were the response category (1). We operationalized race/ethnicity as a construct including dichotomous variables for Hispanic, non-Hispanic black, and non-Hispanic multiple/other race (nonwhite); in the multivariable models, results for those variables are interpretable in reference to the non-Hispanic white group. We coded respondents born outside the United States as 0 and respondents born in the United States as 1. Annual household income in 2016 was a 10-category measure (<$10 000, $10 000-$19 999, $20 000-$29 999, $30 000-$39 999, $40 000-$49 999, $50 000-$74 999, $75 000-$99 999, $100 000-$149 999, $150 000-$249 999, ≥$250 000).
Disaster experiences
We coded respondents without a disability as 0 and respondents with a physical or emotional disability that influenced their ability to evacuate as 1. We coded respondents who did not evacuate as 0 and respondents who did evacuate as 1. Losing a job because of Harvey was a dichotomous variable: we coded respondents whose households did not experience job loss as 0 and respondents whose households did experience job loss as 1. We created a variable for unmet needs by summing responses to 10 checklist-type items (with yes = 1 and no = 0): you went without a comfortable place to sleep for some time; you went without adequate drinking water for some time; you went without adequate clothing for some time; you went without a bathroom for some time; you went without running hot water for some time; you went without electricity for some time; you went without adequate food for some time; you went without adequate transportation for some time; you lacked money for living expenses for some time; or you went without clean piped water for some time. We determined the extent of adverse events experienced by summing 12 checklist-type items: you saw someone drowning or in danger of drowning; you lost a pet or had to abandon one; you worried about crime; you had to perform a dangerous activity; you were stranded in an unsafe place during the disaster; you lost irreplaceable items such as photographs, family mementos or heirlooms, jewelry, or documents; you thought at least once that you might be injured or killed; you worried about family members or friends; you had to split up from household members; you were separated from your children; you experienced unsanitary living conditions; or you experienced crowded living conditions. We assessed personal exposures by summing 5 checklist-type items: you were present when major flooding or hurricane damage occurred; you were a victim of a crime; you smelled unpleasant chemical odors; you inhaled smoke from chemical fires; or you made physical or skin contact with chemicals or contaminants.
Home site effects
We derived the flood extent by using Harvey’s Inundation Footprint, a cartographic product developed by the FEMA Region 6 Mitigation Division. 23 This raster map layer contains flood depth values for each grid pixel (3×3 m) in the study area and was used in recent Harvey studies. 16 -18 Using ArcGIS Desktop version 10.5.1, 34 we generated a flood extent value for each survey respondent by creating a circular buffer (100-m radius) around each geocoded home location and summing all flooded pixels (nonzero depth) areas within the buffer. Next, we divided the flooded area sum by the area of the circular buffer (square meters) to derive the proportion of the area surrounding the respondent’s home that was flooded because of Harvey. The level of home damage was a self-reported measure ranging from 0 (not damaged at all) to 5 (completely destroyed). The square footage of mold present in the respondent’s home was a self-reported measure ranging from 1 (none) to 5 (>100 ft2).
Access to aid
We coded respondents who did not help clean or repair flooded homes as 0 and respondents who did help clean or repair flooded homes as 1. We measured social support by summing respondents’ answers to 8 questions about how often they received the following types of help from family, friends, neighbors, or coworkers: suggest some action that you should take; give, loan, or offer you money or something else you needed; comfort you with a hug or another sign of affection; let you know they would be around if you needed them; express interest and concern in your well-being; offer or provide you with a place to stay; help you with cleaning up or improving your property; or bring you food or cook for you.
Data Analysis
To answer research question 1, we used descriptive statistics for the dependent variables and individual indicators comprising the physical health problems and PTS measures. To answer research question 2, we began by using multiple imputation, which is a best practice for reducing bias when analyzing data with missing values. 35,36 We tabulated the percentage of missing values for each variable in the original data set; the percentage of respondents with missing information for our analysis variables ranged from 0% for physical health problems to 11.4% for flood extent (Table 1). As is recommended, we performed multiple imputation to create 20 data sets with imputed values for all missing data points. 10,18,37,38 We specified all ordinal variables as continuous variables, which is recommended in the multiple imputation literature, because rounding imputed values to conform to discrete ordinal variable specifications results in more biased parameter estimates than treating ordinal variables as continuous in multivariable models. 37,39 -41
We used the multiple imputation data in binary logistic generalized linear modeling 10 to predict the 3 dichotomous dependent variables. The physical health model did not include social support as an independent variable because social support has not been previously linked to postdisaster physical health outcomes. Social support was included in the PTS model because evidence indicates that social support protects against mental health problems (eg, depression, PTS) after disasters. 42,43 The PTS model did not include cleaning activities because these activities are not known to predict PTS. The access to health care model included only social vulnerability variables and having an evacuation disability. For each model, we used Akaike information criterion values to assess goodness of fit. Diagnostic testing indicated that the models were not affected by multicollinearity. We report pooled results from analyses of the 20 multiply imputed data sets for each of the 3 dependent variables. We conducted all analyses by using SPSS version 25. 44
Results
Research Question 1
More than half of respondents (226 of 403, 56.1%) had ≥1 physical health problem (Table 1). On average, respondents had 3 physical health problems, and 45 (11.2%) respondents had ≥10 physical health problems. The most common physical health problems were allergies or hay fever (n = 132, 32.8%), headaches (n = 114, 28.3%), nose irritation (n = 110, 27.3%), and throat irritation (n = 107, 26.6%; Table 2). Sixty-seven of 371 (18.1%) respondents had PTS scores ≥40. Of the 17 items on the PCL-S, having repeated, disturbing memories, thoughts, or images of Harvey was the most reported experience (n = 194 of 400, 48.5%; Table 3). Eighty-eight of 393 (22.4%) respondents reported going without access to health care during or soon after Harvey.
Research Question 2
Respondents who evacuated after Harvey had 59% lower odds than those who did not evacuate of having ≥1 physical health problem (odds ratio [OR] = 0.41; 95% confidence interval [CI], 0.19-0.87). For each additional adverse event experience, respondents had 36% greater odds of reporting ≥1 physical health problem (OR = 1.36; 95% CI, 1.15-1.60). In addition, each scale unit increase in square feet of mold in the home resulted in a 39% increase in the odds of experiencing ≥1 physical health problem (OR = 1.39; 95% CI, 1.05-1.86; Table 4).
Generalized linear models predicting physical health problems, posttraumatic stress, and lack of access to health care among respondents to a post-Hurricane Harvey survey (N = 403) in the Houston–The Woodlands–Sugar Land, Texas, metropolitan statistical area, 2017 a
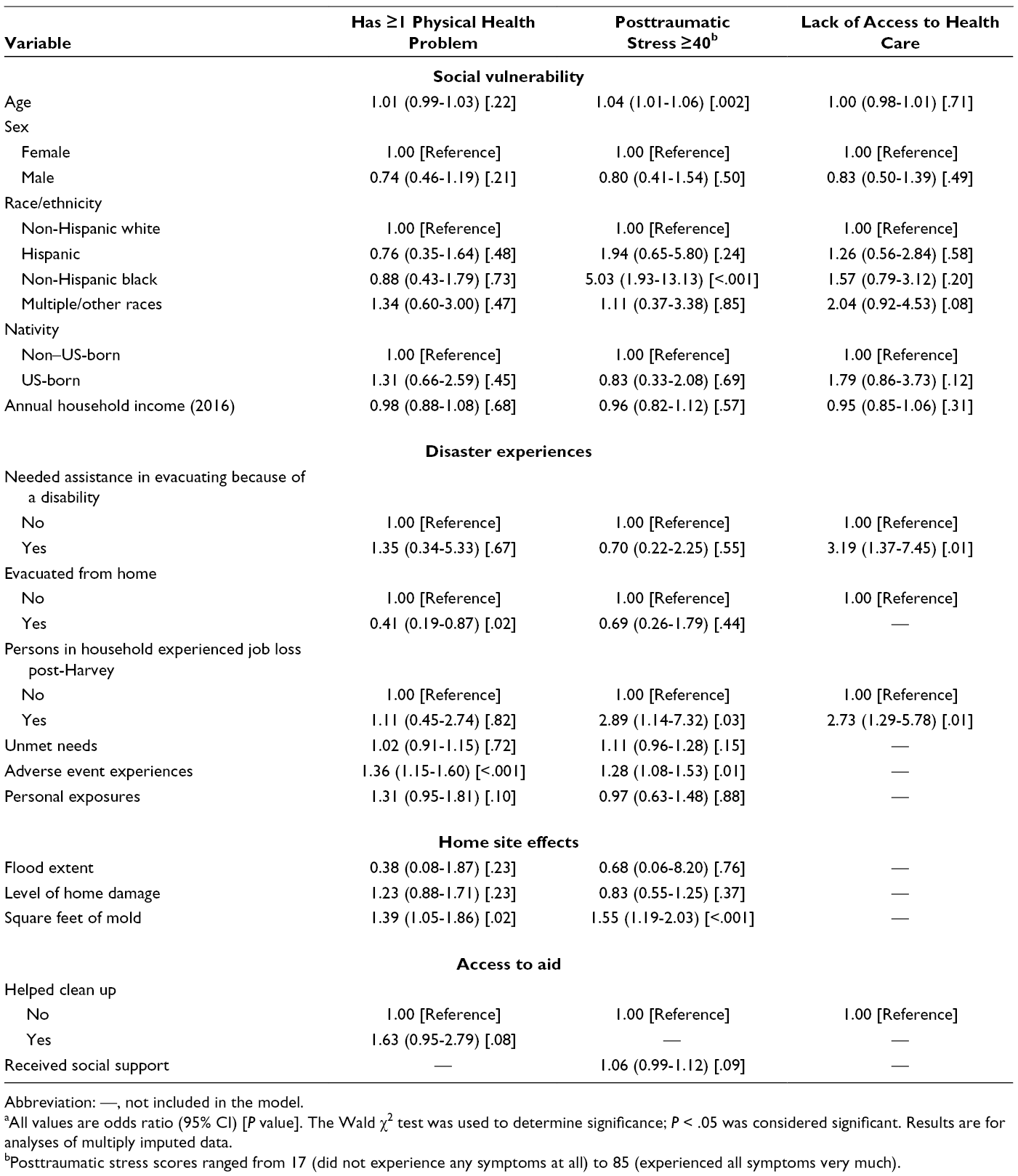
Abbreviation: —, not included in the model.
aAll values are odds ratio (95% CI) [P value]. The Wald χ2 test was used to determine significance; P < .05 was considered significant. Results are for analyses of multiply imputed data.
bPosttraumatic stress scores ranged from 17 (did not experience any symptoms at all) to 85 (experienced all symptoms very much).
Each additional year in age was associated with a 4% increase in the odds of having a PTS score ≥40 (OR = 1.04; 95% CI, 1.01-1.06; Table 4). Being non-Hispanic black versus non-Hispanic white was associated with a 403% increase in the odds of having a PTS score ≥40 (OR = 5.03; 95% CI, 1.93-13.13). Having a household member experience job loss because of Hurricane Harvey was associated with a 189% increase in the odds of having a PTS score ≥40 (OR = 2.89; 95% CI, 1.14-7.32). Each additional adverse event experience during or soon after Hurricane Harvey resulted in a 28% increase in the odds of having a PTS score ≥40 (OR = 1.28; 95% CI, 1.08-1.53). A scale-unit increase in square feet of mold present in the home was associated with a 55% increase in the odds of having a PTS score ≥40 (OR = 1.55; 95% CI, 1.19-2.03).
Having a disability that interfered with evacuation was associated with a 219% increase in the odds of going without access to health care after Harvey (OR = 3.19; 95% CI, 1.37-7.45; Table 4). Also, having a household member experience job loss because of Harvey was associated with a 173% increase in the odds of going without access to health care (OR = 2.73; 95% CI, 1.29-5.78).
Discussion
Descriptive statistics indicated the prevalent effects of Hurricane Harvey on the physical health, mental health, and lack of access to health care among residents of the Houston MSA. Physical health problems were prevalent in more than half of the sample. PTS affected approximately one-fifth of the population, which manifested most frequently in having repeated or disturbing memories of the hurricane. Nearly one-quarter of respondents reported going without adequate health care services during or after Harvey. These results align with previous findings after Hurricane Katrina. 45 -47
Our multivariable statistical models clarified important predictors of the 3 health-related outcomes. Evacuating at any time was protective, whereas more adverse event experiences (vs fewer adverse event experiences) and greater mold exposure (vs less mold exposure) increased the odds of having physical health problems after Harvey. The protective effect of evacuation was likely due to the evacuated residents’ absence during flooding, which reduced their odds of experiencing physical harm, highlighting the importance of evacuating during high-magnitude flood events. Adverse event experiences were also risk factors in the odds for greater severity of PTS, aligning with previous literature. 10 Increased surface area of mold present in one’s home after Harvey was another substantial risk factor for greater severity of PTS. Studies have tested the relationship between mold exposure and mental health, but few have found significant relationships. 48 Exposure to mold may induce physical discomfort or respiratory distress, which could exacerbate the stress response. Also, exposure to mold can impair cognitive function. 49 Having a household member experience job loss because of Harvey played a substantial role in respondents’ mental health, significantly increasing their odds of having PTS. Older age also had a significant effect on respondents’ risk for PTS, which contradicts findings from most, but not all, postdisaster studies on PTS. 13 Non-Hispanic black persons were disproportionately affected by PTS, highlighting environmental justice issues associated with flooding in the Houston MSA. These findings are also consistent with previous studies on mental health and disasters. 8,19,50,51 Respondents whose households experienced job loss because of Harvey (vs households that did not experience job loss) and respondents whose disabilities made it difficult to evacuate (vs respondents without disabilities) faced greater odds of lacking access to health care after the event. These findings are concerning from a public health perspective. Disparate risks for populations with disabilities in the Houston MSA were also highlighted in a study that showed neighborhoods with higher (vs lower) proportions of residents with disabilities had more extensive flooding because of Harvey. 17
Limitations
Although our sample was generally representative of the Houston MSA population, the data had some limitations. First, measurement error inevitably propagates in self-reported data, which were the basis for this study. 52 Second, our analysis lacked the reference frame needed to attribute the health effects we documented directly to Harvey. For example, because we did not account for pre-Harvey health care access, we could not infer that Harvey exacerbated preexisting disparities in health care access. Thus, future postdisaster health research should seek to strengthen casual inferences using pre- and postevent designs and/or appropriate control groups. Finally, our PTS variable was not a diagnostic measure. It was a screening measure of PTS symptomatology based on a conventionally applied threshold.
Conclusion
To our knowledge, this study is the first to use a population-based random sample to analyze the physical health, mental health, and health care access outcomes among residents in the Houston MSA after Hurricane Harvey. Using structured survey data allowed us to determine which residents were disadvantaged in physical health, mental health, and access to health care. Our results indicate that Harvey had substantial effects on Houston MSA residents, highlighting racial/ethnic, age, and socioeconomic disparities, aligning with previous findings on environmental justice in the region. 16,17,25,53 -56 This study indicates a need to enhance knowledge of the role of race/ethnicity and SES in creating population health vulnerabilities in order to improve public health interventions, as some residents’ social disadvantages were associated with post-disaster health disparities. Our findings also indicate the need for improvements to flood hazard mitigation and public health response efforts in the Houston MSA. Public health officials can use this information to provide health services to disadvantaged populations in future flood events to ameliorate disparities. These efforts have become essential as similar events are more likely to occur now rather than 20 years ago in the Houston MSA because of climate change. 57
Footnotes
Acknowledgments
The authors thank Mark English, the Hazard and Performance Analysis’s Geospatial Unit Lead with FEMA under Disaster Operations within the Mitigation Branch, for contributing to the creation of Harvey’s Inundation Footprint, a data product used in our analysis.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the US National Science Foundation (award no. 1841654). Any opinions, conclusions, or recommendations expressed in this article are those of the authors and do not necessarily reflect the views of the National Science Foundation.