
Abstract
Objectives:
Colorectal cancer (CRC) incidence and mortality are twice as high among Alaska Native people as among non-Hispanic White people in the United States; as such, colonoscopy is a recommended screening test for Alaska Native people. Adenoma detection rate (ADR) is measured in patients at average risk of CRC undergoing initial screening colonoscopy and reflects the prevalence of precancerous polyps in a screened population. We evaluated the ADR among Alaska Native people living in Interior Alaska.
Methods:
This project evaluated the ADR among Alaska Native and American Indian adults aged ≥40 years (N = 460) living in Interior Alaska, using a retrospective medical record review of patients referred for screening colonoscopy from February 1, 2018, through March 31, 2022. The main outcome measure was ADR, stratified by age and sex.
Results:
The ADR was 45.0% overall: 43.0% among women and 47.1% among men. Among patients aged ≥50 years, the ADR was 67.1%: 62.7% among women and 70.7% among men. Among patients aged 40-49 years, the ADR was 34.4%: 35.3% among women and 33.3% among men.
Conclusions:
Measured ADR was high among Alaska Native men and women aged ≥50 years in Interior Alaska and in all age groups that were screened. These findings have implications for which CRC screening methods, intervals, and age to begin screening are most appropriate for Alaska Native people, as well as the need for future research on the pathology, etiology, and natural history of CRC in this population.
The natural history of colorectal cancer (CRC) makes it ideally suited to screening. Most CRCs develop over many years from adenomatous polyps. The identification and removal of precancerous polyps during colonoscopy are associated with reduced future CRC and CRC mortality.1-3 When CRC is found early and appropriately treated, survival is greatly enhanced, with a 5-year relative survival rate of 90%. 4
CRC is the third-most commonly diagnosed cancer in the United States and ranks second among Alaska Native people, occurring at more than twice the rate of the US non-Hispanic White population.4-6 Alaska Native people have the highest rates of CRC incidence (88 per 100 000 population) and mortality (37 per 100 000 population) in the United States. 6 CRC incidence and mortality rates among Alaska Native people are 2 times higher than rates among non-Hispanic Black people (46 and 19 per 100 000 population, respectively) and 3 times higher than among non-Hispanic White people (37 and 13 per 100 000 population).4,6 CRC incidence among Alaska Native people is higher at every age group and as high among Alaska Native people aged 40-49 years as among non-Hispanic White people aged 50-59 years.5,6 Alaska Native people also have a disproportionately high prevalence of advanced adenomas, even among those aged 40-49 years, 7 although the proportion of CRCs found at each cancer stage is similar to that of the non-Hispanic White population in the United States. 5 CRC screening rates have been increasing among the Alaska Native population, but in contrast to other racial and ethnic groups, CRC incidence rates among Alaska Native people of screening age are not declining. 8 CRC mortality among Alaska Native people is actually increasing, and no improvements have occurred in incidence, age at diagnosis, tumor size, tumor location, or stage distribution during the past 20 years; furthermore, CRC incidence is increasing among Alaska Native people aged <50 years.9,10 While some risk factors for CRC among Alaska Native people likely mirror risk factors observed in other populations, such as family history in a first-degree relative, tobacco use, and diabetes, unique genetic or lifestyle factors may contribute to the high CRC risk that have yet to be explored in this population.
Tanana Chiefs Conference is an Alaska Native nonprofit health care system also organized as Dena’ Nena’ Henash or “Our Land Speaks.” Tanana Chiefs Conference serves 42 primarily Athabascan communities (population size, 50-500 people) located in Interior Alaska. The Tanana Chiefs Conference health care system includes 36 primary care clinics, all of which are located in frontier-designed census areas and considered by the Health Resources and Services Administration as medically underserved areas/populations. More than 72% of the patient population in 2021 was at ≤200% of the federal poverty level based on data from the Federally Qualified Health Center Program Uniform Data System. 11 CRC rates are also high in this region: for the 2004-2018 period, the Alaska Native age-adjusted CRC incidence was 101.7 per 100 000 population, which was 3 times higher than among non-Hispanic White people in the United States. 6 All patients from these communities must travel to the hub community of Fairbanks, Alaska (population size, 30 000) to access screening colonoscopy.
Because of the remoteness of the region served by Tanana Chiefs Conference, cancer screening, especially CRC screening, is a challenge. The Alaska Native CRC screening rate in Interior Alaska (69.5%) is below the national Healthy People 2030 goal (74.4%) and the National CRC Roundtable goal (80%).12-14 Colonoscopy and at-home fecal immunochemical testing are used for screening, although colonoscopy is the preferred test for this population at increased risk of CRC. 15 High-quality screening to detect and remove precancerous and cancerous polyps is a Tribal health care priority for Alaska Native people. Because of high rates of CRC, Tanana Chiefs Conference follows the Alaska Native Medical Center’s CRC screening guidelines for Alaska Native people, which recommend starting screening at age 40 years. 15
Adenoma detection rate (ADR) is a quality benchmark of endoscopists’ ability to find adenomas and, with successful removal, a predictor of cancer prevention by colonoscopy.16-18 ADRs vary widely in the literature, from 14.2% to 28.9%, with lower rates among men and among patients aged <60 years.19-22 ADRs can also vary widely among endoscopists, 21 with one study reporting ADRs ranging from 7.4% to 52.5% among endoscopists. 22 Higher ADRs are associated with a reduction in interval CRC, advanced-stage interval cancer, and fatal interval cancer: with each 1% increase in ADR, there is a 3% decrease in the risk of CRC.22,23 Minimum thresholds of an ADR ≥25% overall (≥30% for men and ≥20% for women) among patients aged 50-75 years who are undergoing initial colonoscopy screening is regarded as a standard that would identify an acceptable proportion of adenoma-positive patients and, as such, is generally considered indicative of high-quality colonoscopy.16,17
Tanana Chiefs Conference endoscopists who perform screening colonoscopies observed what appeared to be a higher ADR in this population. To examine the data more fully, the Tanana Chiefs Conference cancer prevention coordinator (J.J.P.) led a medical record review and analysis to better assess the quality of colonoscopies performed among Alaska Native patients living in Interior Alaska. To our knowledge, this project is the first exploration of ADRs in a rural/remote Athabascan Alaska Native population and was intended as an initial step to assess whether changes in CRC screening methods, intervals, and age to begin screening may be warranted to improve clinical care and health outcomes in this population. We report here on ADRs among Alaska Native people in Interior Alaska, stratified by age, sex, and community size.
Methods
The Tanana Chiefs Conference cancer prevention coordinator (J.J.P.) extracted and cleaned medical record data from its electronic health record on colonoscopy examinations and pathology results completed from February 1, 2018, through March 31, 2022; patient demographic characteristics, including sex, age (40-49 and ≥50 y), and community of residence (village or hub); and the number of colonoscopies completed and the colonoscopy results for each endoscopist.
According to the literature and in consultation with subject matter experts from the American Cancer Society, we used the following ADR selection criteria: patients with Tribal affiliation listed in the electronic medical record as Alaska Native or American Indian, age ≥40 years at the time of examination, first-time screening colonoscopy or a prior incomplete screening colonoscopy with no biopsies, no CRC symptoms, no family history of CRC in a first-degree relative, comprehensive pathology data available, adequate bowel preparation and sedation, procedure completed to the cecum, and ≥1 histologically confirmed colorectal adenomas of any size (tubular, tubulovillous, villous, or high-grade dysplasia). We used endoscopic and histologic findings to determine ADR. To ensure that only patients with no screening history or family history in a first-degree relative were included, data from 4 medical record systems were extracted on the basis of retrospective review: 3 at Interior Alaska Tribal and nonTribal health systems and 1 at the Alaska Native Medical Center in Anchorage, Alaska. We calculated the overall ADR as the number of examinations with adenomas found divided by the total number of examinations. We also calculated ADR by sex, age group (40-49 and ≥50 y), and sex within age group. Lastly, we reviewed the number of colonoscopies performed by each endoscopist and calculated the ADR for each of the 4 participating endoscopists.
Tanana Chiefs Conference determined that institutional review board approval and informed consent were not required because this study was a public health surveillance project and all data were deidentified. We obtained Tribal review and approval for publication of these findings from the Tanana Chiefs Conference and the Alaska Native Tribal Health Consortium.
Quality Control and Statistical Analysis
To ensure quality control of data input, we randomly selected 32 of 460 (7.0%) eligible records for validation with the original data sources (pathology reports, medical record review); 2 records met exclusion criteria and were removed from the data set because of a prior colonoscopy (n = 1) and symptoms of CRC (n = 1). We conducted additional validation on 10 (3.0%) ineligible records and found no errors. We then entered the data on the 460 resulting colonoscopies into Microsoft Excel for analysis. For categorical factors (sex, age group, community size), we used the Pearson χ2 test to test differences in proportions between patients with and without adenomas detected. All analyses were 2-tailed, and P < .05 was considered significant.
Results
Through medical record review, we identified 790 Tanana Chiefs Conference patients referred for screening colonoscopy from February 1, 2018, through March 31, 2022. Of these, 330 (41.8%) did not meet ADR inclusion criteria and were excluded from analysis. Most exclusions were due to a family history of CRC in a first-degree relative, a screening examination that was not the patient’s first, or inadequate bowel preparation or failed sedation.
Of 460 eligible patients with colonoscopies completed, 237 (51.5%) were women, 311 (67.6%) were aged 40-49 years, and 149 (32.4%) were aged ≥50 years (Table). An overall 158 (34.3%) patients were from smaller communities (population size, ~50-500) surrounding the hub community (population size, ~30 000). At least 1 adenomatous polyp was found in 207 (45.0%) patients. We included colonoscopies from 4 endoscopists in the ADR calculation. Staff endoscopists performed 56-158 examinations each, and 2 endoscopists performed >100 total colonoscopies during the study period. The ADR by endoscopist ranged from 37.3% to 53.6% (mean, 46.1%). Provider-level data were not available for 28 examinations.
Among patients aged ≥40 years, the ADR was 45.0% (43.0% among women, 47.1% among men) (Table). The ADR was highest among patients aged ≥50 years, among whom the overall ADR was 67.1% (62.7% among women, 70.7% among men). When age was restricted to patients aged 40-49 years, the ADR was still high: 34.4% overall (35.3% among women, 33.3% among men). The ADR was 49.4% among patients living in smaller communities as compared with 42.7% among patients living in the larger hub community. Patients in the older age group (≥50 y) were significantly more likely than patients in the younger age group (40-49 y) to have adenomas (P < .001).
Demographic characteristics and adenoma detection rate among Alaska Native and American Indian patients (N = 460) in Interior Alaska, February 1, 2018, through March 31, 2022
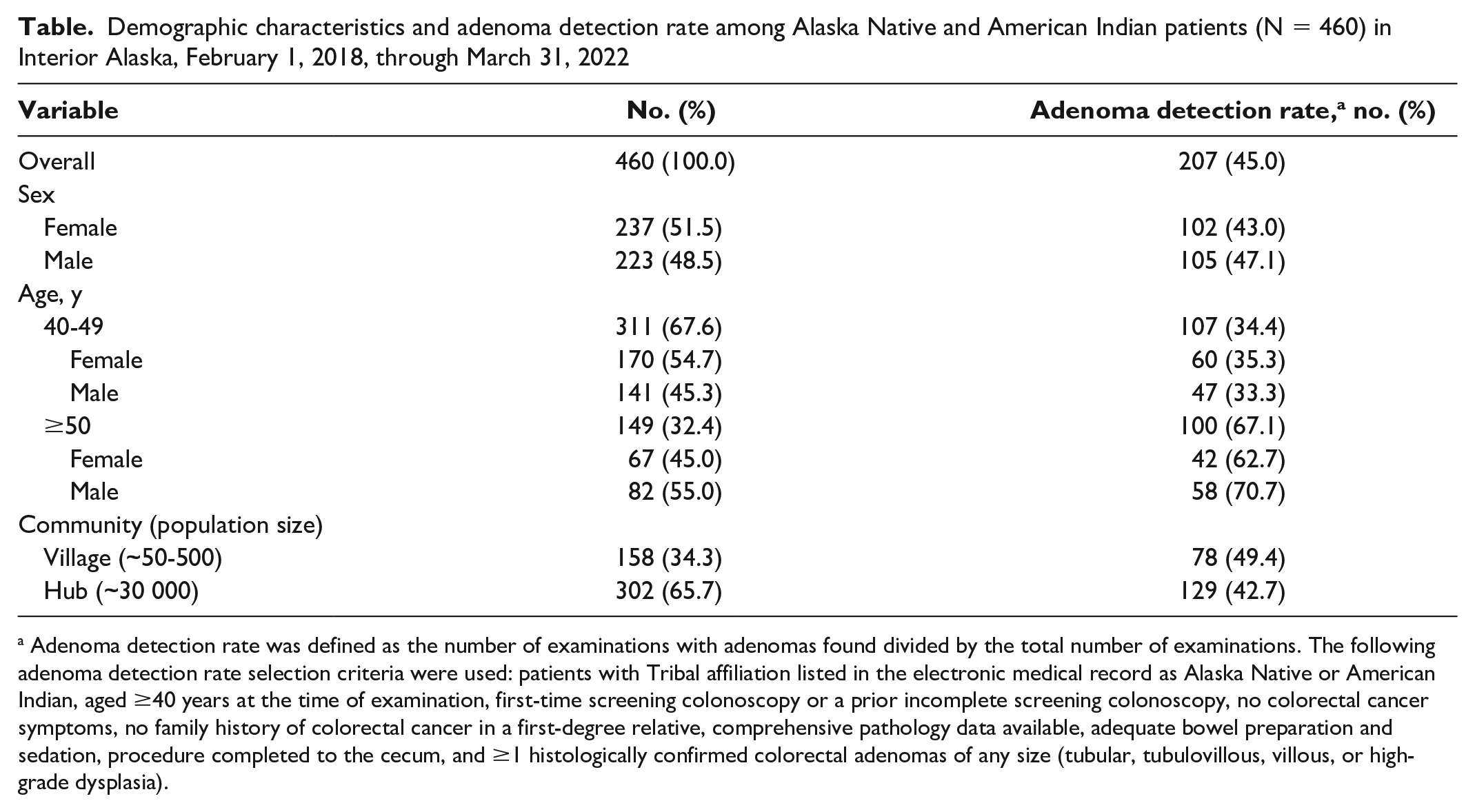
Adenoma detection rate was defined as the number of examinations with adenomas found divided by the total number of examinations. The following adenoma detection rate selection criteria were used: patients with Tribal affiliation listed in the electronic medical record as Alaska Native or American Indian, aged ≥40 years at the time of examination, first-time screening colonoscopy or a prior incomplete screening colonoscopy, no colorectal cancer symptoms, no family history of colorectal cancer in a first-degree relative, comprehensive pathology data available, adequate bowel preparation and sedation, procedure completed to the cecum, and ≥1 histologically confirmed colorectal adenomas of any size (tubular, tubulovillous, villous, or high-grade dysplasia).
Discussion
The ADR in this population of asymptomatic Alaska Native and American Indian patients with average risk of CRC was substantially higher than the ADR reported in other populations, including non-Hispanic White and non-Hispanic Black Northern California Kaiser Permanente members and community members receiving screening colonoscopies in Minneapolis and St Paul, Minnesota.20,24 Similar to the results in other studies, the ADR in this group of Alaska Native people was higher among patients aged ≥50 years (vs <50 y) and men (vs women), although the ADR was higher among women aged 40-49 years than among men aged 40-49 years. In addition, the ADRs that we observed were higher than the ADRs in a 2019 study by Conway et al of an urban Alaska Native population: that study found an ADR of 26% among people aged 40-49 years and 40% among people aged 50-59 years. 7 A key difference between the study by Conway et al and our analysis is that we excluded patients with a family or personal history of CRC or adenomatous polyps. That we found a higher ADR despite a patient population that should have been at lower risk of CRC is substantial. Additionally, the study by Conway et al was conducted among Alaska Native patients receiving CRC screening in Anchorage, Alaska, which is the most urban and acculturated region of the state. We are not able to speculate why the rates were higher in our analysis, although it is notable that both studies showed much higher ADRs among Alaska Native people than among other populations, thus suggesting that screening processes and methods in this population might need to account for the increased risk of adenomatous polyps.
Strengths and Limitations
A strength of this study was having access to laboratory, diagnostic, pathology, and radiologic records, including family history, and complete examination records to ascertain bowel preparation quality and confirmation of histologic findings, which allowed for the exclusion of noneligible patients. However, our study had several limitations. First, it was a retrospective analysis of medical records in a single Tribal health care practice setting; as such, it might not be generalizable to other Tribal or health care organization patient populations. Second, the colonoscopies that we reviewed in this project were completed by only 4 endoscopists, and scope withdrawal time was not assessed (ie, the time that an endoscopist takes to withdraw the endoscope at the end of a colonoscopy), which might have impacted the quality of the procedures completed. 25 Third, we did not quantify the number of adenomas detected per patient or the adenoma location in the colon. Future work should determine if greater numbers of adenomatous polyps found per patient or polyp location is associated with a higher likelihood of adenoma detection, as well as the quality of adenoma removal among the Alaska Native population. 25 Our analysis was not intended to determine why ADR might be higher among this population, and it did not include other factors that increase the risk of CRC, such as diabetes or tobacco use; however, future work examining the association of these risk factors with Alaska Native ADR may help pinpoint some of the reasons for the disparities that we observed.
Conclusions
These findings have implications for which CRC screening methods, intervals, and age to begin screening are most appropriate for Alaska Native people, as well as the need for future research into the pathology, etiology, and natural history of CRC in this population. Colonoscopy, with the potential for CRC prevention by polyp identification and removal, may be a more appropriate screening method than stool-based tests for Alaska Native people living in Interior Alaska, including younger patients. While Tanana Chiefs Conference currently initiates screening at age 40 years in accordance with the Alaska Native Medical Center’s CRC screening guidelines, 15 our finding of an ADR of 34% among patients aged 40-49 years suggests a need for risk identification and possible screening at an earlier age. Finally, given these findings, Tanana Chiefs Conference has adjusted our ADR quality benchmarking for endoscopists to a goal of 50% for all patients aged >40 years, with ongoing monitoring. Tanana Chiefs Conference will continue to track ADR and associated CRC incidence and mortality over time, with the goal of reducing the burden of this preventable disease among Alaska Native and American Indian people living in Interior Alaska.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Centers for Disease Control and Prevention DP17-1704 Building Public Health Infrastructure in Tribal Communities under award NU58DP006379. We acknowledge the contributions and support of Durado Brooks, MD, formerly of the American Cancer Society; the Tanana Chiefs Conference Research and Study Sub-committee and Board of Directors; the Alaska Native Tribal Health Consortium Tribal review committees for their review and approval of this article for publication; and the Alaska Native Tumor Registry, which is supported by the National Cancer Institute Surveillance, Epidemiology and End Results Program, contract HHSN2612018000014I, task order HHSN26100001. The content presented is solely the responsibility of the authors and does not necessarily represent the official views of the Centers for Disease Control and Prevention.