
Abstract
Objectives:
Surveillance of cigarette smoking behavior provides evidence for evaluating the impact of current tobacco control measures. We examined temporal changes and demographic differences in the incidence and mean age of starting to smoke cigarettes regularly in the United States.
Methods:
We conducted retrospective birth-cohort and cross-sectional analyses using self-reported data from the 1997-2018 National Health Interview Survey to evaluate trends and demographic differences in the incidence and mean age of starting to smoke cigarettes regularly among participants aged 18-84 years. We estimated the incidence and mean age of starting to smoke cigarettes regularly by using Poisson and linear regression.
Results:
Among adults born during 1950-1999, the incidence of starting to smoke cigarettes regularly before age 35 years decreased by 18.8% (95% CI, 17.0%-20.7%) per 10 years, with a peak incidence at age about age 18 years. Male, non-Hispanic White, and US-born people had a higher incidence of starting to smoke cigarettes regularly than female, other racial and ethnic, and non–US-born people, respectively (P < .001 for all). From 1997 to 2018, the mean age of starting to smoke cigarettes regularly decreased by 0.4% (95% CI, 0.2%-0.6%) per 10 years among adults who ever smoked.
Conclusion:
The incidence of starting to smoke cigarettes regularly decreased dramatically at all ages during the study period, which suggests a positive impact of current tobacco control measures. For evaluating trends in starting to smoke cigarettes regularly, incidence can be a more sensitive indicator of temporal change than mean age. Differences in smoking incidence by demographic subgroup suggest that additional opportunities exist to further reduce the incidence of starting to smoke cigarettes regularly.
Keywords
Cigarette smoking is the leading cause of preventable disease and death in the United States. 1 The use of nicotine-containing products can harm the developing brain and increase susceptibility to addiction among adolescents. 2 An early age of starting cigarette smoking is associated with an increased risk of all-cause mortality, 3 educational disparities, and smoking more cigarettes later in life.4,5 Changes in the incidence and age of starting to smoke cigarettes regularly have implications for smoking prevention measures. Continuously monitoring temporal and demographic changes is essential for programs that evaluate, develop, and implement equitable interventions and policies to prevent initiation and discourage the progression from smoking experimentation to regular smoking. 6
During the past several decades, the United States has implemented multiple tobacco control strategies tailored toward adolescents; these strategies can affect the age of starting to smoke regularly in the United States. 7 Studies on smoking regularly commonly use the age at which a person starts cigarette smoking daily or regularly as an indicator. Previous studies used the mean age of starting to smoke from either cross-sectional data or simulation models to demonstrate the temporal change of smoking initiation or smoking daily.8-10 However, a person’s reported age of starting to smoke regularly was the same regardless of when the interview was conducted during the person’s lifetime. Therefore, findings can hardly be interpreted as an association between preventive tobacco interventions and temporal changes in mean age by survey year. The incidence of starting to smoke cigarettes regularly is a time-sensitive metric for trend analysis.
By using National Health Interview Survey (NHIS) data from 1997 through 2018, we investigated temporal changes in the incidence of starting to smoke cigarettes regularly by birth cohort from 1950 through 1999 and temporal changes of the mean age of starting to smoke cigarettes regularly by survey year from 1997 through 2018. We also assessed the association of age of starting to smoke cigarettes regularly with the highest level of educational attainment and the average number of current cigarettes smoked daily at interview date among adults who currently smoke.
Methods
Data Source
The NHIS is an ongoing annual nationally representative survey of the civilian noninstitutionalized population in the United States and uses a complex sampling design. 11 We combined publicly available, deidentified data from the NHIS years 1997 through 2018 (1997-2018). The National Center for Health Statistics Research Ethics Review Board approved the protocol of the NHIS. All NHIS participants provided verbal consent prior to participation. 11
Inclusion and Exclusion Criteria
Age ≥85 years was top coded as 85 years in public-release files. We excluded people aged >84 years (n = 17 313; 2.6%) from the study. 11 We excluded 5383 (1.0%) adults because of missing data on smoking status and 333 adults with missing data on the number of cigarettes smoked per day. For analyses related to age of starting to smoke cigarettes regularly, we excluded 6432 (2.3%) adults who were uncertain about having smoked at least 100 cigarettes in their entire lifetime and 4102 (1.5%) adults who smoked but did not know their age of starting to smoke cigarettes regularly. In related analyses, we excluded the following: participants who refused to answer the question on birthplace (n = 536 [0.1%]) or were uncertain about (n = 91 [<0.05%]) or did not know (n = 119 [<0.05%]) their birthplace and people who refused to answer the question on educational attainment (n = 2315 [0.4%]) or for whom the information was uncertain (n = 23 [<0.05%]) or unknown (n = 2598 [0.4%]). The final analytical samples for the mean age of starting to smoke cigarettes regularly by survey years from 1997 through 2018 consisted of 649 633 participants aged 18-84 years at interview. Most people who start cigarette smoking start when they are aged <30 years. 12 For the incidence of starting to smoke cigarettes regularly estimated by year of birth from 1950 through 1999, we restricted these analyses to participants aged 18-35 years at the time of the interview to minimize potential survivorship bias due to premature death as a competing risk. We excluded participants who did not respond to the question about the age of starting to smoke cigarettes regularly (n = 16 018) and participants born before 1950 and after 1999 (n = 195 398). The birth cohort sample consisted of 460 280 participants followed up to age 35 years.
Smoking-Related Variables
Participants who had smoked at least 100 cigarettes in their lifetime were categorized as ever smoked; participants who had not smoked at least 100 cigarettes in their lifetime were categorized as never smoked. Those who currently smoke every day or some days were categorized as currently smoked; those who ever smoked but were not currently smoking were categorized as formerly smoked. Thus, a cigarette smoking status could be 1 of 3 categories: current smoking, former smoking, or never smoking. Age of starting to smoke cigarettes regularly among participants who currently or formerly smoked was recalled by the question, “How old were you when you first started to smoke fairly regularly?” An age of <6 years was recorded in public-use data as 6 years. The answers to the average number of current cigarettes smoked per day during the past 30 days ranged from 1 to ≥94. We grouped the number of current cigarettes smoked per day into 4 categories by quartiles as observed among participants who smoke: 1-5, 6-10, 11-20, and >20 cigarettes.
Demographic Variables
Self-reported demographic characteristics assessed included age (years), sex (female, male), race and ethnicity (Mexican American, non-Hispanic Asian, non-Hispanic Black, non-Hispanic White [hereinafter, White], Other Hispanic [not Mexican American], and Other non-Hispanic [other than previous categories]), birthplace (US-born, non–US-born), and educational attainment. We defined participants as US- born if they were born in 1 of the 50 states, the District of Columbia, or the 5 US territories; all others were defined as non–US-born. For analyses using responses from adults aged ≥18 years, we used a 3-level highest educational attainment variable (<high school graduate, high school graduate, >high school graduate). For our association analysis of age of starting to smoke cigarettes regularly and level of educational attainment for participants aged ≥25 years, we used a 4-level highest educational attainment variable (<high school, high school graduate, some college, and college graduate).
Statistical Analysis
Incidence of starting to smoke cigarettes regularly, by birth cohort
We treated starting to smoke cigarettes regularly as an incident event from the year at birth to the year at interview and adult age and calendar year during the follow-up as time-varying variables. We aggregated participants into 5 groups based on year of birth: 1950-1959, 1960-1969, 1970-1979, 1980-1989, and 1990-1999. The total years of follow-up using retrospective information were from the year of birth to the reported year of starting to smoke cigarettes regularly or at age 35 years or year at survey, whichever was reached first. We used Poisson regression to estimate the incidence of starting to smoke cigarettes regularly with quadratic terms for age during the follow-up by birth cohort. 13 The incidence was reported per 100 person-years. We used the interaction terms of the birth cohort with age (as a continuous variable), sex, and race and ethnicity to examine differences in incidence rates by those variables. No participant born in the latest birth cohort (1990-1999) would attain age ≥29 years at interview; we partially projected the age-specific incidence rates for this period by using age as a continuous variable.
Mean age of starting to smoke cigarettes regularly, by survey period
We reported the mean age of starting to smoke cigarettes regularly by survey year group (1997-1999, 2000-2004, 2005-2009, 2010-2014, and 2015-2018). We used linear regression to estimate crude and adjusted means for age of starting to smoke cigarettes regularly.
We used both the difference in incidence and the percentage change in incidence of mean age of starting to smoke cigarettes regularly to examine temporal trends in incidence and mean age of starting to smoke cigarettes regularly. We used the average differentiation of estimate in a 10-year unit to estimate the average difference, and we used the average differentiation of log-transformed estimate in a 10-year unit to estimate relative change.
For examining the association of education and number of current cigarettes smoked with the grouped age of starting to smoke cigarettes regularly (<12, 12 or 13, 14-17, 18-25, 26-50 years), we limited the analytical sample to adults who currently smoke from ages 25-50 years; we used multinomial logistic regression to model these associations.
All analyses accounted for the complex sampling design according to NHIS analytic guidelines. 11 We used the Taylor linearization approach to calculate SEs and 95% CIs. We used the delta method to compute the SE and 95% CI for differences or the ratio of independent estimates. 14 We used Stata version 17.0 (StataCorp, LLC) for data analysis. We reported the 95% CIs and P values for population inference. We used t tests to compare means for continuous variables and Wald χ2 tests to compare proportions for categorical variables. We considered a 2-sided P value <.05 to be significant.
Results
Across survey periods, the average age of participants increased from 44.1 to 46.5 years (P < .001) (Table 1). By sex, the proportion of female compared with male participants was consistent (P = .43). While the proportion of White adults decreased, the proportion of Hispanic and non-Hispanic Other adults increased (P < .001). The proportion of adults with a high school education or more increased with each survey period (P < .001), as did the proportion of non–US-born adults (P < .001). By survey year, the proportion of adults who never smoked increased (P < .001). Among US adults who currently smoked, the proportion of those who smoked >20 cigarettes per day decreased (P < .001), and more adults who ever smoked started to smoke cigarettes regularly at age ≥18 years (P < .001).
Weighted estimates of characteristics of adults aged 18-84 years, by survey period, National Health Interview Survey, 1997-2018 a
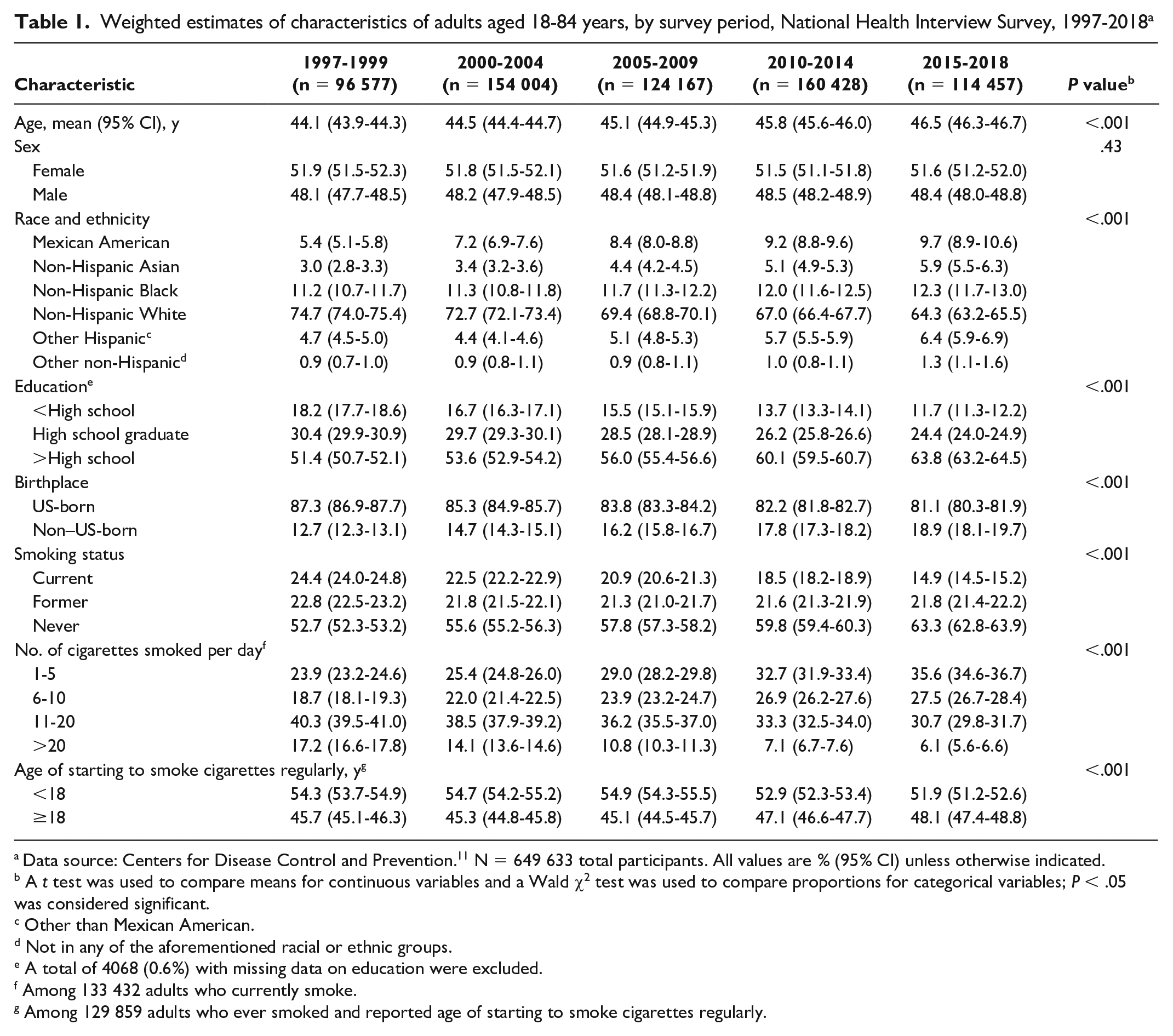
Data source: Centers for Disease Control and Prevention. 11 N = 649 633 total participants. All values are % (95% CI) unless otherwise indicated.
A t test was used to compare means for continuous variables and a Wald χ2 test was used to compare proportions for categorical variables; P < .05 was considered significant.
Other than Mexican American.
Not in any of the aforementioned racial or ethnic groups.
A total of 4068 (0.6%) with missing data on education were excluded.
Among 133 432 adults who currently smoke.
Among 129 859 adults who ever smoked and reported age of starting to smoke cigarettes regularly.
The incidence of starting to smoke cigarettes regularly per 100 person-years decreased substantially from 1950 to 1999 by age group, sex, race and ethnicity, and birthplace (Table 2) (P < .05 for all). The largest absolute decrease in the incidence of starting to smoke cigarettes regularly by age group was in the group aged 14-17 years, with a 0.5% (95% CI, 0.5%-0.6%) absolute reduction per 10-year increment. The largest percentage decrease in the incidence of starting to smoke cigarettes regularly by age group was seen in the group aged 26-35 years (decreased 21.5% [95% CI, 16.3%-26.7%]) and in the group aged 6-11 years (decreased 21.3% [95% CI, 17.7%-24.9%]). Males had a higher incidence of starting to smoke cigarettes regularly than females did. White adults had an overall higher incidence and smaller decrease in the incidence of starting to smoke cigarettes regularly than adults of other racial and ethnic groups. US-born participants had a higher incidence and greater absolute decrease in the incidence of starting to smoke cigarettes regularly than non–US-born participants.
Adjusted incidence of starting to smoke cigarettes regularly, per 100 person-years by birth cohort, 1950-1999, National Health Interview Survey, 1997-2018 a
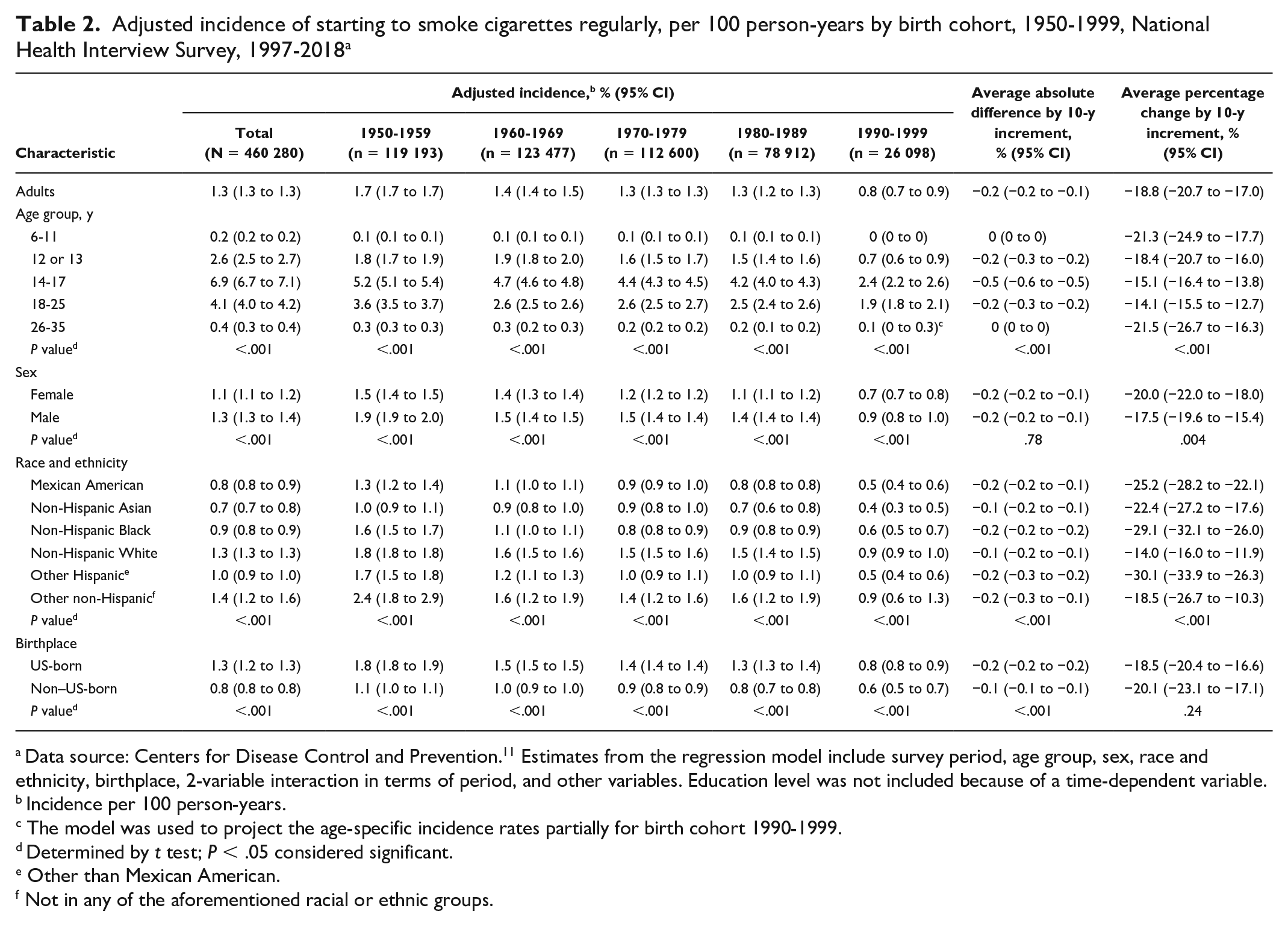
Data source: Centers for Disease Control and Prevention. 11 Estimates from the regression model include survey period, age group, sex, race and ethnicity, birthplace, 2-variable interaction in terms of period, and other variables. Education level was not included because of a time-dependent variable.
Incidence per 100 person-years.
The model was used to project the age-specific incidence rates partially for birth cohort 1990-1999.
Determined by t test; P < .05 considered significant.
Other than Mexican American.
Not in any of the aforementioned racial or ethnic groups.
From 1997 to 2018, after adjusting for age, sex, race and ethnicity, and birthplace, the average difference in mean age of starting to smoke cigarettes regularly among adults who ever smoked was significant but not meaningful in public health practice (decreased 0.1 years per 10-year increment) (Table 3). The mean age of starting to smoke cigarettes regularly increased by 0.3 (95% CI, 0.2-0.4) years per 10-year increment among adults aged 18-29 years but decreased by 0.7 (95% CI, 0.6-0.8) years per 10-year increment among adults aged 70-84 years. The age of starting to smoke cigarettes regularly decreased by 0.3 years per 10-year increment among females but increased by 0.1 year per 10-year increment among males. The mean age of starting to smoke cigarettes regularly decreased by 0.3 (95% CI, 0.2-0.5) years per 10-year increment among Mexican American adults. We observed no significant differences in changes in mean age of starting to smoke cigarettes regularly by education or birthplace (P > .30 for all).
Adjusted mean age of starting to smoke cigarettes regularly among adults aged 18-84 years who ever smoked cigarettes, by period, National Health Interview Survey, 1997-2018 a
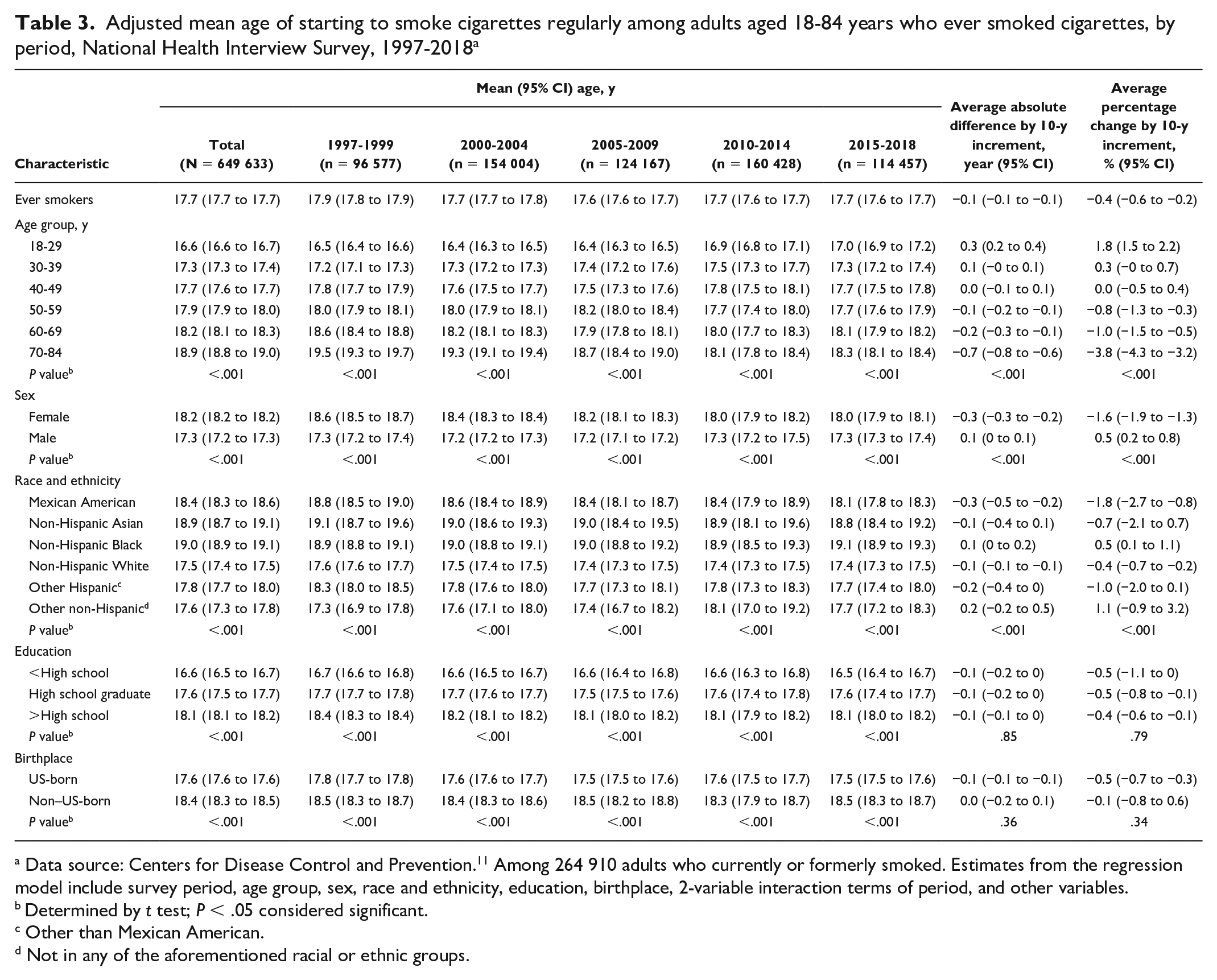
Data source: Centers for Disease Control and Prevention. 11 Among 264 910 adults who currently or formerly smoked. Estimates from the regression model include survey period, age group, sex, race and ethnicity, education, birthplace, 2-variable interaction terms of period, and other variables.
Determined by t test; P < .05 considered significant.
Other than Mexican American.
Not in any of the aforementioned racial or ethnic groups.
Across birth cohorts, during the lifetime, adolescents aged 14-17 years had the highest incidence of starting to smoke cigarettes regularly: the adjusted average incidence was 6.9% (95% CI, 6.7%-7.1%) (Table 2). The age of peak incidence of starting to smoke cigarettes regularly was relatively stable at the age of about 18 years (Figure). In modeled projections for adults aged ≥29 years born during 1990-1999, the distribution of incidence of starting to smoke cigarettes regularly shifted a little, but the incidence for each age decreased significantly. Compared with those born during 1950-1989, those born during 1990-1999 had a consistently lower incidence of starting to smoke cigarettes regularly.
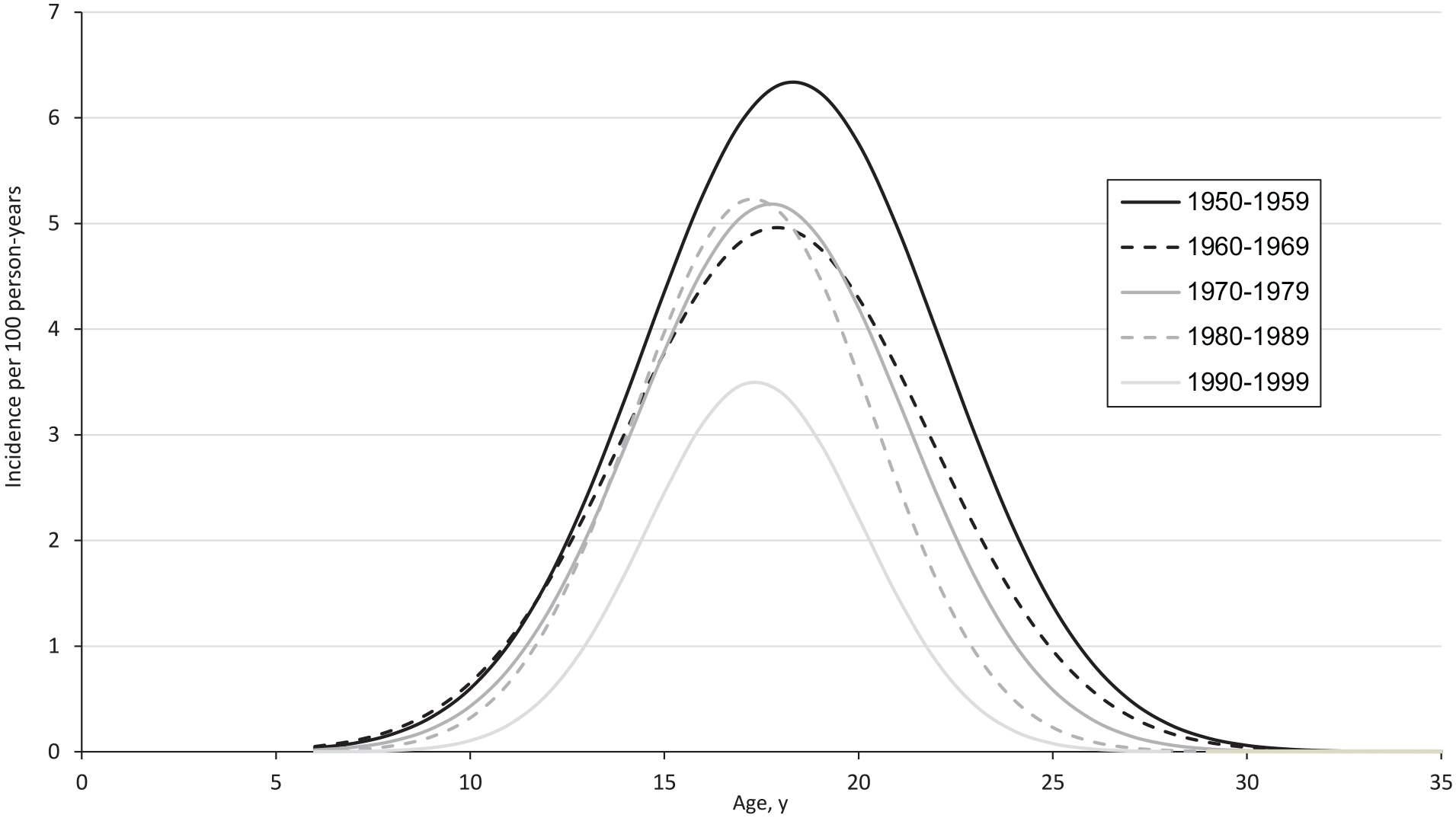
Incidence of starting to smoke cigarettes regularly, adjusted for sex and race and ethnicity, among the US population, by age and birth cohort, United States, National Health Interview Survey, 1997-2018. No participant born in the latest birth cohort (1990-1999) would attain age ≥29 years in 2018 at interview; the model was used to project the age-specific incidence rates for age ≥29 years of birth cohort 1990-1999. Data source: Centers for Disease Control and Prevention. 11
Among adults aged 25-50 years who currently smoke, those who started to smoke cigarettes regularly when aged 6-11 years were more likely to have less than a high school education and to smoke more than 20 cigarettes per day than those who started smoking cigarettes regularly at a later age (Table 4). As age of starting to smoke cigarettes regularly increased among adults who currently smoke, the percentage of adults who were college graduates increased, as did the percentage of adults who smoked 1-5 cigarettes daily, whereas the percentage of adults with less than a high school education and the percentage of adults who smoked >20 cigarettes daily decreased.
Adjusted proportion of educational attainment and cigarettes smoked per day by age of starting to smoke cigarettes regularly among adults aged 25-50 years who currently smoke cigarettes, National Health Interview Survey, 1997-2018 a
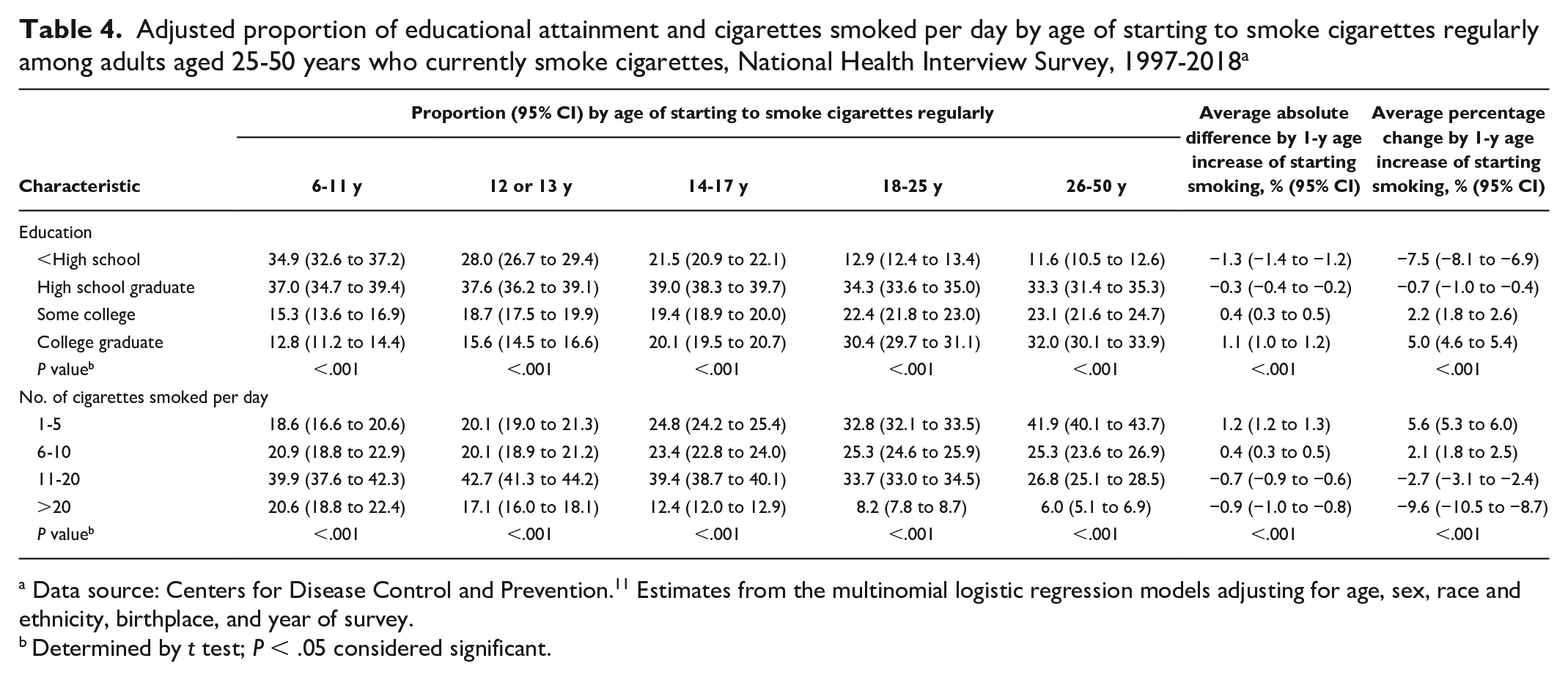
Data source: Centers for Disease Control and Prevention. 11 Estimates from the multinomial logistic regression models adjusting for age, sex, race and ethnicity, birthplace, and year of survey.
Determined by t test; P < .05 considered significant.
Discussion
Using NHIS data from 1997-2018, this study examined temporal trends and differences in incidence and mean age of starting to smoke cigarettes regularly from both lifetime and cross-sectional perspectives, by age, sex, race and ethnicity, and birthplace. Overall, the incidence of starting to smoke cigarettes regularly decreased dramatically from early to later birth cohorts across all age, sex, race and ethnicity, and birthplace groups. From age 6 to 35 years, people aged approximately 18 years had the highest incidence of starting to smoke cigarettes regularly. In addition, White people and males had a higher incidence of starting to smoke cigarettes regularly, and their incidence decreased relatively more slowly than that of other racial and ethnic groups and females. The adjusted mean age of starting to smoke cigarettes regularly was approximately 18 years and changed little across survey years. We found significant but small differences in mean age of starting to smoke cigarettes regularly by age at interview, sex, race and ethnicity, and birthplace.
Nicotine exposure during adolescence can harm the developing brain and increase the risk of nicotine dependence.2,15-17 The age at which a person starts smoking is inversely associated with the risk of cardiovascular mortality. 18 The United States has launched multiple mass media and educational campaigns about these dangers designed for young audiences.6,7,19 A previous study of people aged <24 years found that the proportion of smoking initiation and daily smoking changed from 2002 to 2018, and the mean age of smoking initiation changed from 15.0 years in 2002 to 16.5 years in 2018. 8 Our study showed that the reported mean age of starting to smoke cigarettes regularly increased among adults aged 18-39 years and decreased among adults aged ≥40 years. This difference in directional change among younger versus older age groups could be due in part to a decrease in incidence across all age groups with a relatively consistent peak age of starting to smoke cigarettes regularly. Such findings were gleaned by using age-specific incidence rates of starting to smoke cigarettes regularly to complement findings beyond those offered by examining the mean age of starting cigarette smoking.
By using the birth-cohort approach, our study demonstrated that the incidence of starting to smoke cigarettes regularly in the United States decreased significantly across the entire population. The age of peak incidence of starting to smoke cigarettes regularly had little change and was around age 18 years. We saw the largest absolute decrease but less relative change in the incidence of starting to smoke cigarettes regularly among adolescents aged 14-17 years; however, adolescents aged 14-17 years still had the highest incidence of starting to smoke cigarettes regularly, which is consistent with other studies.9,20,21
Our study showed that the variation in incidence of starting to smoke cigarettes regularly was substantial for all ages, both sexes, all racial and ethnic groups, and US-born and non–US-born people. 22 Meanwhile, the temporal change in mean age of starting to smoke cigarettes regularly was small. To guide tobacco prevention and control policies and interventions to reach populations at elevated risk for smoking, it is important to monitor changes in the incidence of starting to smoke cigarettes regularly. Our study affirmed that the age of starting to smoke cigarettes regularly was positively associated with higher educational attainment level among adults and inversely associated with the current daily number of cigarettes smoked among people who ever smoked.5,20,21,23
Limitations
The findings of this study were subject to several limitations. First, our study was an observational study based on cross-sectional data; thus, causal relationships cannot be inferred. Second, age of starting to smoke cigarettes regularly, smoking status, and other variables were self-reported and subject to misclassification; however, self-reported data on age of starting to smoke cigarettes regularly are sufficiently reliable for epidemiological study. 24 Third, our study did not capture data on patterns of use of other tobacco products such as cigars, electronic cigarettes, and smokeless tobacco; we need to interpret findings extended to the entire array of tobacco products with caution. Fourth, the incidence of starting to smoke cigarettes regularly among people aged ≥29 years from the latest birth cohort was partially modeled and projected and could not capture data on the actual incidence for those people. Finally, our study did not explore other potential factors accounting for changes, such as social, environmental, and policy-related factors; we made conclusions on those associations without considering those factors.
Conclusion
During the past few decades, the incidence of starting to smoke cigarettes regularly decreased dramatically among people in the United States, which suggests a positive impact of current tobacco control measures. For exploring trends in starting to smoke cigarettes regularly, we found that incidence is a better indicator than mean age is. In identifying the variations in smoking incidence by age, sex, race and ethnicity, educational attainment, and birthplace, additional opportunities exist to further reduce the incidence of starting to smoke cigarettes regularly among various subgroups for continued public health progress. Continued surveillance of tobacco product use and implementation of tobacco prevention strategies are necessary to ensure continued progress in smoking initiation and the reduction of tobacco-related disease and death. 25
Footnotes
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.