
Abstract
Objectives:
Understanding the health-risk behaviors of racial and ethnic groups when disaggregated is an important step in improving the health outcomes of racial and ethnic minority groups. We compared national prevalence estimates for selected health-risk behaviors and experiences of Asian American and Native Hawaiian/Pacific Islander (NHPI) students with those of non-Hispanic White, non-Hispanic Black, and Hispanic students.
Methods:
We analyzed data from the Youth Risk Behavior Survey, a nationally representative survey of US high school students. To generate a sufficient sample of Asian American and NHPI students for analyses, we combined data from 5 survey administrations, conducted in 2011, 2013, 2015, 2017, and 2019 (N = 73 074). We calculated the prevalence and 95% CIs; we analyzed data on Asian American and NHPI adolescents separately to unmask important differences.
Results:
Compared with students of other races and ethnicities, Asian American students had the lowest prevalence of alcohol use (16.7%) and marijuana use (10.3%). In contrast, NHPI students were more likely than Asian American students to participate in several health-risk behaviors and experiences, such as substance use (ranging from 4.8% for ever injecting an illegal drug to 31.5% for current alcohol use), having been in a physical fight (15.4%), and having been threatened or injured with a weapon (11.6%). Differential patterns in the prevalence of ever having missed school due to feeling unsafe among NHPI and Asian American students were observed among male and female students.
Conclusion:
Further disaggregating racial subgroups within broad categories of Asian American and NHPI populations may reveal differences from overall group prevalence, and additional strategies to identify these differences should be investigated.
Asian American and Native Hawaiian/Pacific Islander (NHPI) groups are heterogeneous groups with differences in immigration history, successive generational status, acculturation, religious beliefs, and culture. The US Census Bureau defines Asian as a person having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian subcontinent. 1 NHPI people are defined as people having origins in any of the original peoples of Hawaii, Guam, Samoa, or other Pacific Islands. 1 Starting with the 1977 standards of the US Office of Management and Budget (OMB), federal data systems specified 4 single-race categories: American Indian/Alaska Native, Asian/Pacific Islander, Black, and White. 2 In 1997, OMB standards allowed respondents to select multiple races during federal data collection activities but also asked for selection of primary race. 2 Because states provide vital statistics data to the Centers for Disease Control and Prevention (CDC) and the time frame for instituting the 1997 OMB standards varied by state, the National Center for Health Statistics, in collaboration with the US Census, developed bridged-race categories so that data on race from all states could be compared. 2 With changes in reporting standards over time and the small size of the aggregated Asian American and NHPI populations in the United States, data for these groups are not often produced or presented. Because of sample size constraints, the national Youth Risk Behavior Survey (YRBS) produces separate estimates for Asian American and NHPI high school students approximately every 5 or 6 cycles. Studies that present data for Asian American and NHPI adolescents in a combined category mask disparities in health behaviors and outcomes. 3 When data are disaggregated, there are significant differences in health-risk behaviors between Asian American and NHPI students.4,5
The objective of this study was to provide updated national prevalence estimates for 2011 through 2019 of health-risk behaviors and experiences among Asian American and NHPI high school students in behavioral and experiential domains that may increase the risk for transmission of HIV, viral hepatitis, and sexually transmitted diseases, including substance use, sexual risk behaviors, violence-related experiences, and suicidal behaviors. We also compared the prevalence of each risk behavior and experience among Asian American and NHPI students with the prevalence among non-Hispanic White, non-Hispanic Black, and Hispanic students.
Methods
Sample and Survey Administration
This study used data from the YRBS, a cross-sectional survey conducted biennially by CDC since 1991. In each survey, a similar 3-stage cluster sample design is used to obtain a nationally representative sample of US high school students in public and private schools in grades 9-12 in the 50 states and the District of Columbia. Student participation is voluntary and anonymous, and local parental permission protocols are followed. To generate a sufficient sample of Asian American and NHPI students, we combined data from 5 national YRBS cycles: 2011-2019.
In 2011, 2013, 2015, 2017, and 2019, overall response rates were 71.0%, 68.0%, 60.0%, 60.0%, and 60.3%, respectively; sample sizes were 15 425, 13 583, 15 624, 14 765, and 13 677, resulting in a sample size of 73 074 for our analysis.6-10 Data were weighted to adjust for student and school nonresponse and oversampling of Hispanic and non-Hispanic Black students; missing data were not imputed. Details on YRBS psychometric properties and sampling strategies are available elsewhere.11,12 The national YRBS was reviewed and approved by the institutional review board at CDC. 10
Measures
All YRBS data are self-reported. The YRBS assessed race by asking, “What is your race? (Select one or more responses.)” 13 Students could respond to the following options: American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or Other Pacific Islander, and White. Ethnicity was assessed with a yes/no answer to the following question: “Are you Hispanic or Latino?” Based on self-report of race and Hispanic or Latino ethnicity, we defined 5 categories of race and ethnicity: non-Hispanic Asian (hereinafter, Asian American), non-Hispanic Native Hawaiian or Other Pacific Islander (hereinafter, NHPI), non-Hispanic White (hereinafter, White), non-Hispanic Black (hereinafter, Black), and Hispanic. Because of the language of the questions and the response options for race and ethnicity, it was not possible to further disaggregate the Asian American and NHPI groups.
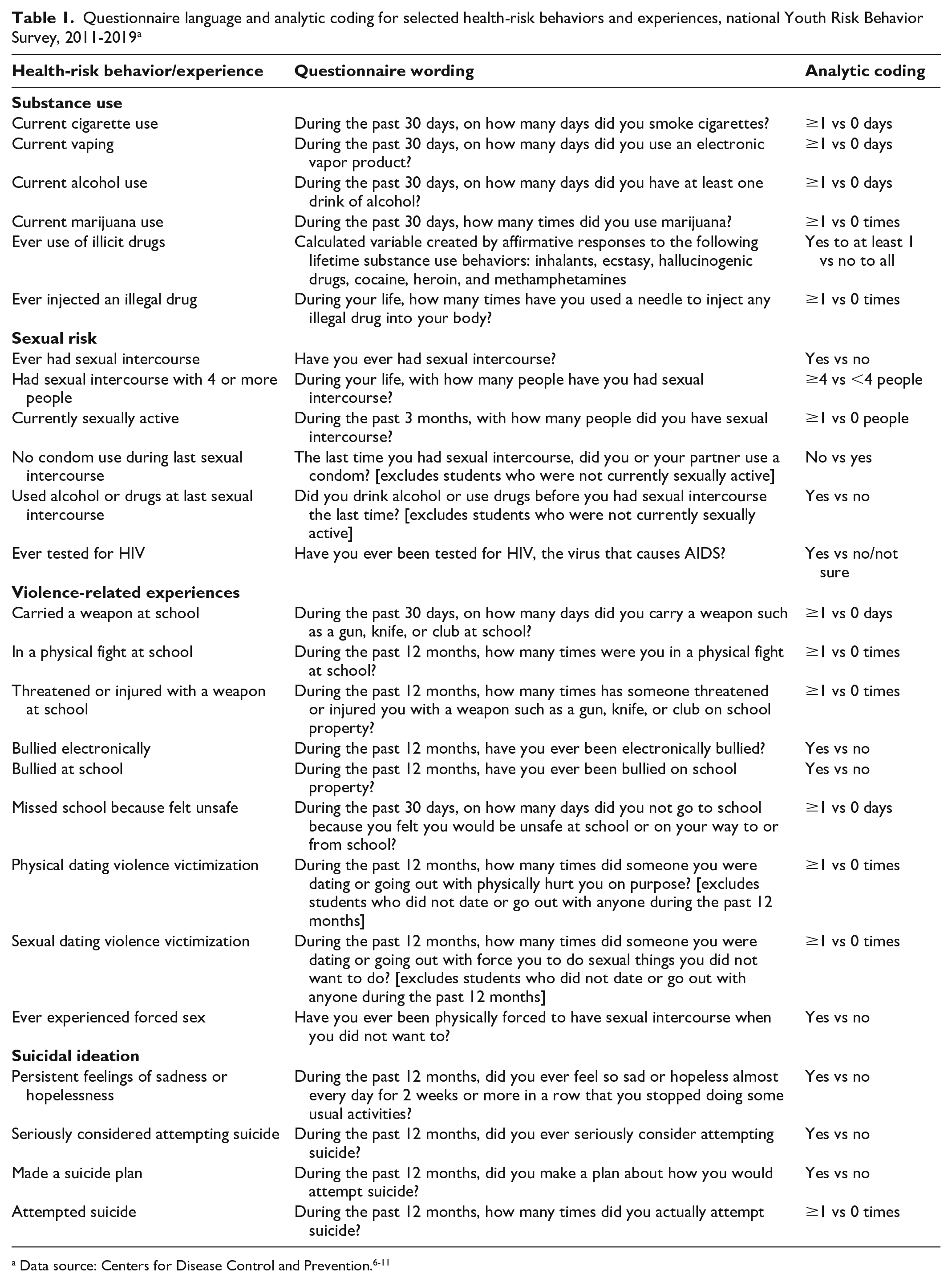
Health-risk behaviors and experiences associated with an increased risk for morbidity and mortality in adulthood were included in this study across 4 major behavioral domains: substance use, sexual risk behaviors, violence-related experiences, and suicidal thoughts and behaviors (Table 1).
Questionnaire language and analytic coding for selected health-risk behaviors and experiences, national Youth Risk Behavior Survey, 2011-2019 a
Analysis
We calculated prevalence estimates and 95% CIs overall and for each of the 5 racial and ethnic subgroups: Asian American, NHPI, White, Black, and Hispanic. Data for students in other racial and ethnic groups, such as non-Hispanic American Indian or Alaska Native and non-Hispanic multiracial (ie, >1 race), and students who did not provide racial or ethnic information were included in total population estimates but not analyzed separately because of limited interpretability. We also calculated prevalence estimates separately for male and female students. 10 We determined pairwise differences in prevalence estimates by race and ethnicity using t tests. We considered differences to be significant at P < .05. To account for the complex sample design of the survey, we conducted all analyses using SUDAAN version 11.0.1 (RTI International), which allowed use of sample weights across survey years.
Results
Sample Characteristics
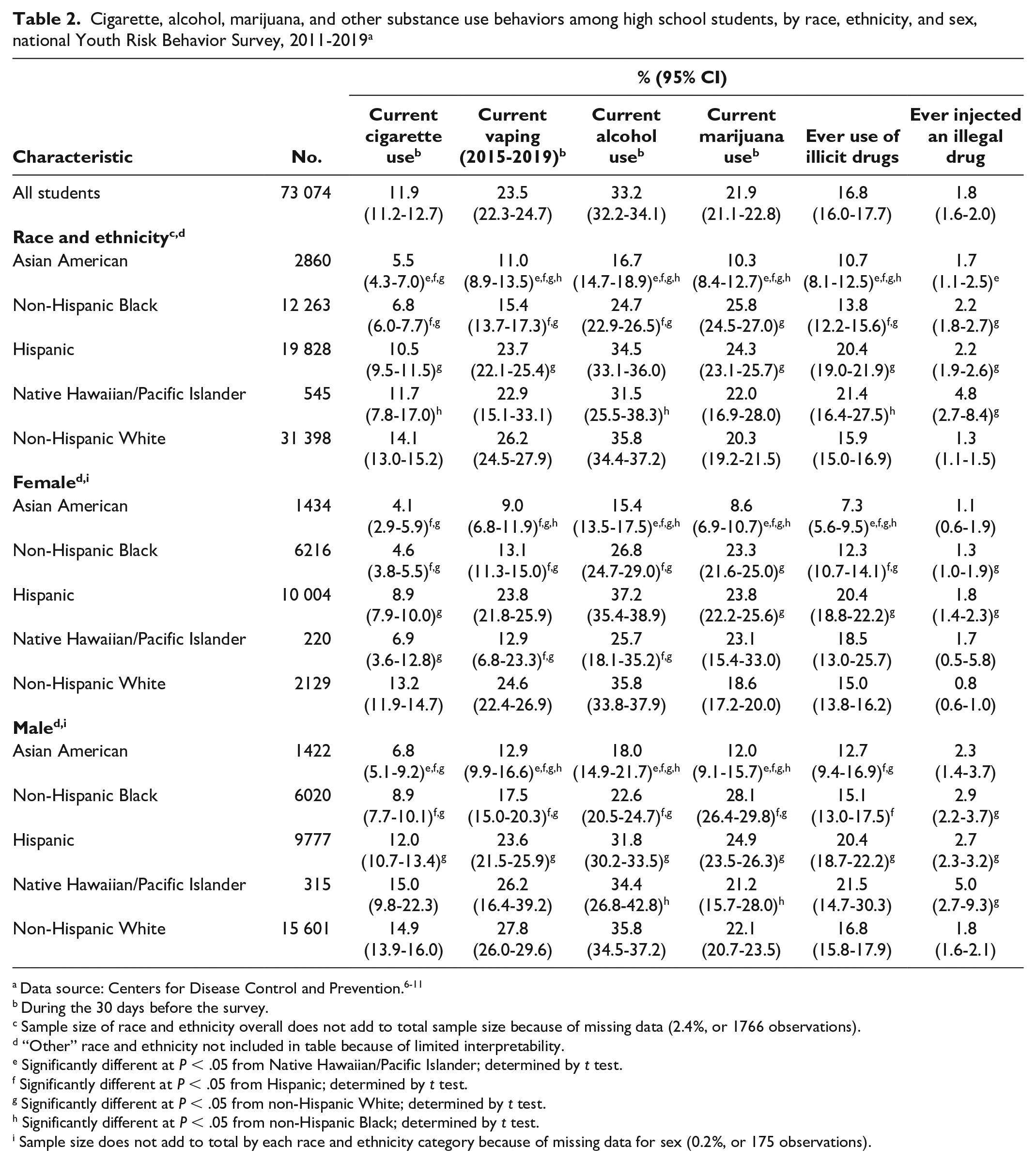
The sample included 2860 (3.7%) Asian American, 12 263 (13.6%) Black, 19 828 (22.4%) Hispanic, 545 (0.7%) NHPI, and 31 398 (54.4%) White students; 4414 (4.8%) respondents were of “other” races and ethnicities (American Indian or Alaska Native, non-Hispanic multiracial) (Table 2). We found no significant difference in the distribution of racial and ethnic groups by sex.
Cigarette, alcohol, marijuana, and other substance use behaviors among high school students, by race, ethnicity, and sex, national Youth Risk Behavior Survey, 2011-2019 a
During the 30 days before the survey.
Sample size of race and ethnicity overall does not add to total sample size because of missing data (2.4%, or 1766 observations).
“Other” race and ethnicity not included in table because of limited interpretability.
Significantly different at P < .05 from Native Hawaiian/Pacific Islander; determined by t test.
Significantly different at P < .05 from Hispanic; determined by t test.
Significantly different at P < .05 from non-Hispanic White; determined by t test.
Significantly different at P < .05 from non-Hispanic Black; determined by t test.
Sample size does not add to total by each race and ethnicity category because of missing data for sex (0.2%, or 175 observations).
Substance Use Behaviors
Compared with other racial and ethnic groups, Asian American students had a lower prevalence of all substance use behaviors except ever injecting an illegal drug (1.7%) and current cigarette use (5.5%) (Table 2). Female Asian American students had a lower prevalence than female students in all other racial and ethnic groups of current alcohol use (15.4%), current marijuana use (8.6%), and ever use of illicit drugs (7.3%). For current vaping (12.9%), current alcohol use (18.0%), and current marijuana use (12.0%), male Asian American students had a lower prevalence than students in all other racial and ethnic groups. The prevalence of current cigarette use was lower among male Asian American students (6.8%) than among male students in all other racial and ethnic groups except male Black students (8.9%).
The prevalence of current cigarette use (11.7%), current alcohol use (31.5%), and ever use of illicit drugs (21.4%) was higher among NHPI students than among Black students (6.8%, 24.7%, and 13.8%, respectively) (Table 2). We observed significant differences between Asian American and NHPI students. The prevalence of having ever injected illegal drugs among NHPI students (4.8%) was significantly greater than among Asian American (1.7%) and White (1.3%) students. Female NHPI students had a lower prevalence of vaping (12.9%) and current alcohol use (25.7%) than female Hispanic (23.8% and 37.2%, respectively) and White (24.6% and 35.8%) students, but the prevalence of smoking cigarettes (6.9%) among female NHPI students was lower than among female White students (13.2%). Male NHPI students had a significantly higher prevalence of current alcohol use (34.4%) and a significantly lower prevalence of current marijuana use (21.2%) compared with male Black students (22.6% and 28.1%, respectively). Male NHPI students had a higher prevalence of ever injecting drugs than male White students (5.0% vs 1.8%).
Sexual Risk Behaviors
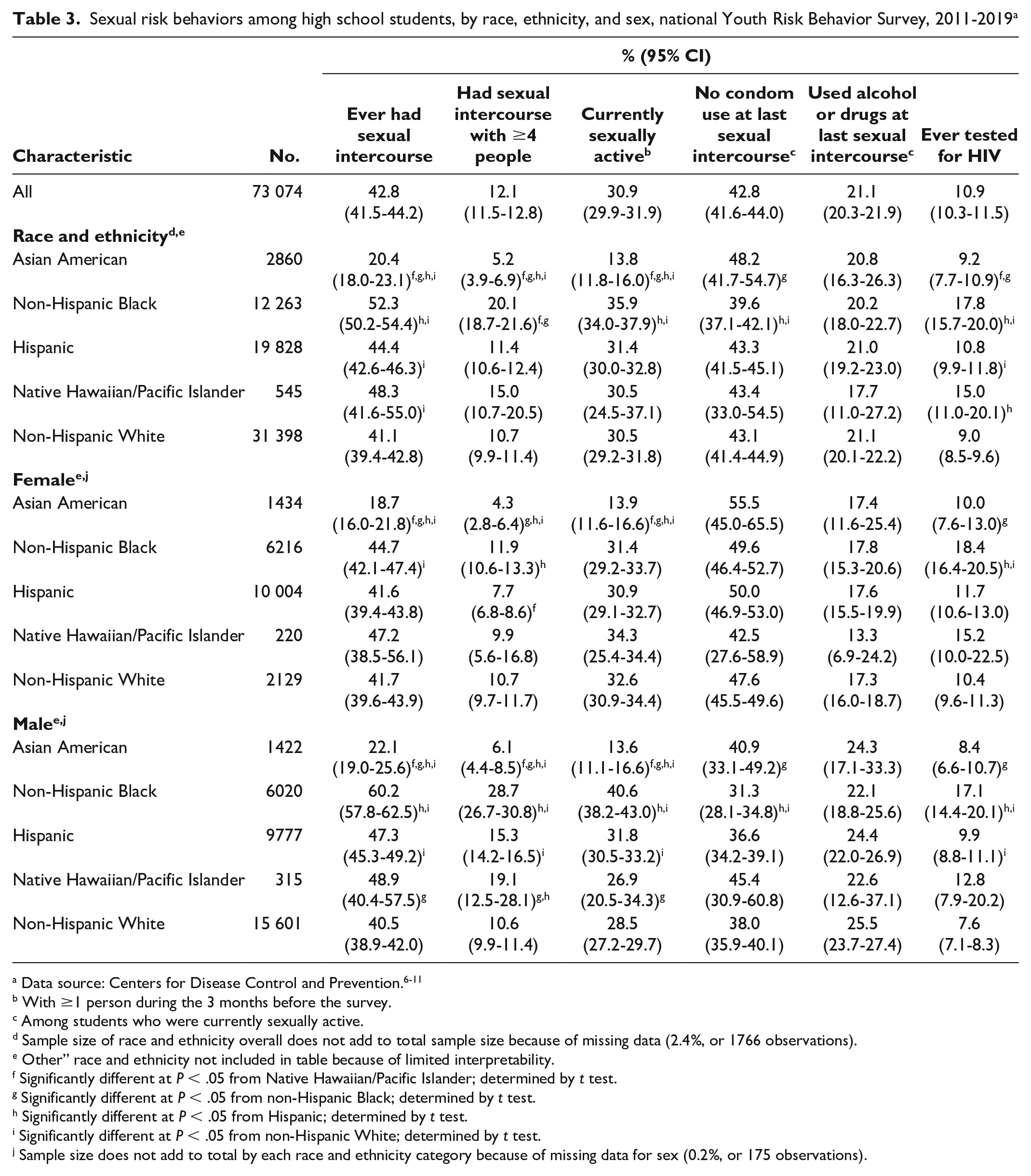
Overall, the prevalence of ever having sexual intercourse (20.4%), having sexual intercourse with ≥4 people (5.2%), and being currently sexually active (13.8%) was significantly lower among Asian American students than among students in all other racial and ethnic groups (Table 3). The prevalence of ever being tested for HIV was lower among Asian American students (9.2%) than among NHPI (15.0%) and Black (17.8%) students. Among female students, the prevalence of ever having sexual intercourse (18.7%) and being currently sexually active (13.9%) was lowest among Asian American students. Female Asian American students had a lower prevalence of having sexual intercourse with ≥4 people (4.3%) compared with female students in all other racial and ethnic groups except female NHPI students (9.9%). Among male students, the prevalence of ever having sexual intercourse (22.1%), having sexual intercourse with ≥4 people (6.1%), and currently being sexually active (13.6%) was lower among Asian American students than among students in all other racial and ethnic groups.
Sexual risk behaviors among high school students, by race, ethnicity, and sex, national Youth Risk Behavior Survey, 2011-2019 a
With ≥1 person during the 3 months before the survey.
Among students who were currently sexually active.
Sample size of race and ethnicity overall does not add to total sample size because of missing data (2.4%, or 1766 observations).
Other” race and ethnicity not included in table because of limited interpretability.
Significantly different at P < .05 from Native Hawaiian/Pacific Islander; determined by t test.
Significantly different at P < .05 from non-Hispanic Black; determined by t test.
Significantly different at P < .05 from Hispanic; determined by t test.
Significantly different at P < .05 from non-Hispanic White; determined by t test.
Sample size does not add to total by each race and ethnicity category because of missing data for sex (0.2%, or 175 observations).
The prevalence of ever having sexual intercourse was higher among NHPI students (48.3%) than among White students (41.1%), while having sexual intercourse with ≥4 people was lower among NHPI students than among Black students (15.0% vs 20.1%) (Table 3). The prevalence of ever having sexual intercourse (48.9%), having sexual intercourse with ≥4 people (19.1%), and being currently sexually active (26.9%) was lower among male NHPI students than among male Black students (60.2%, 28.7%, and 40.6%, respectively). The prevalence of having sexual intercourse with ≥4 people was higher among male NHPI students (19.1%) than among male Hispanic students (15.3%).
Violence-Related Experiences
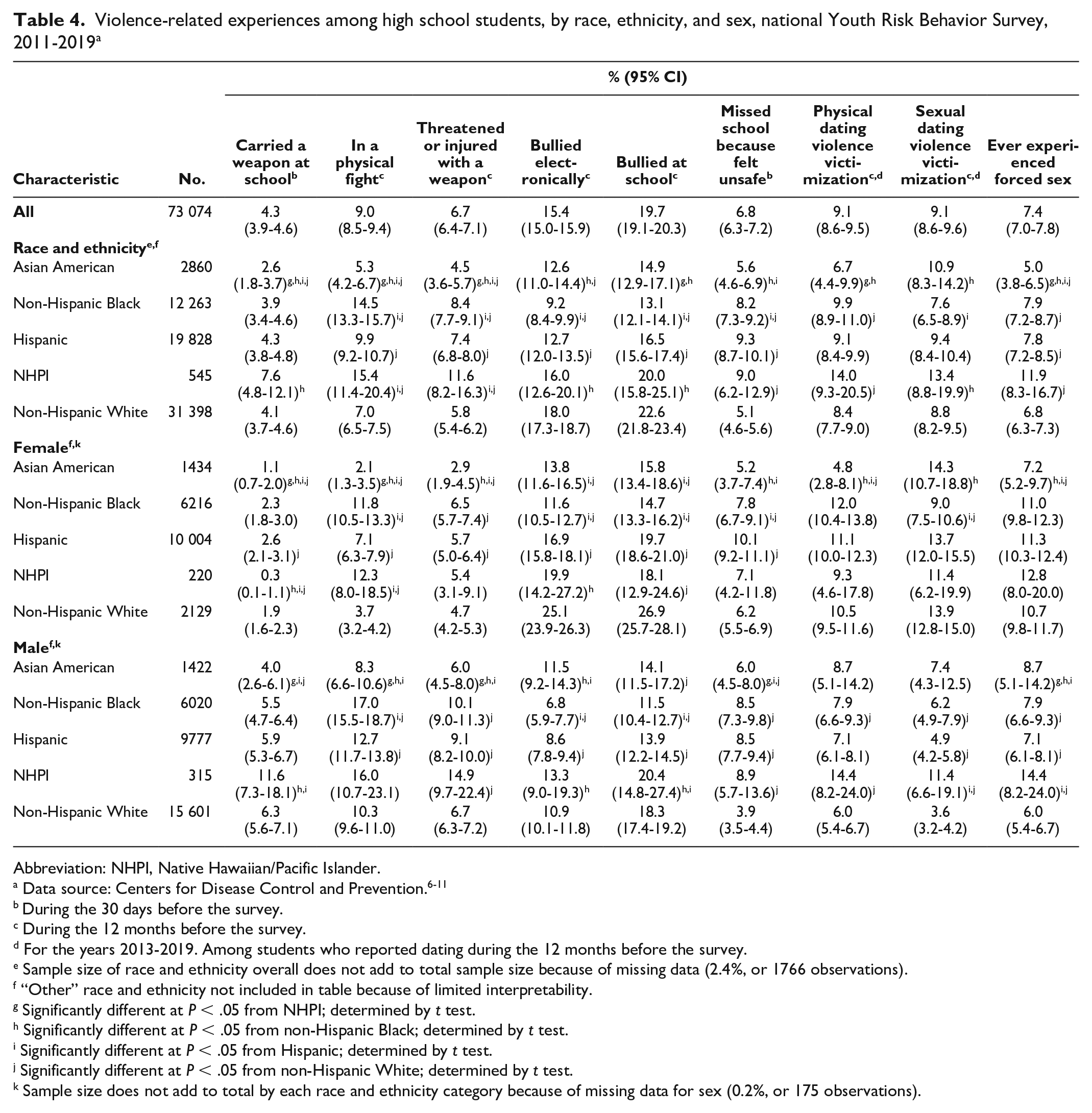
The prevalence of having carried a weapon at school (2.6%), being in a physical fight (5.3%), being threatened or injured with a weapon (4.5%), and ever experiencing forced sex (5.0%) tended to be lower among Asian American students than among students in other racial and ethnic groups (Table 4). For being bullied electronically (12.6%) and bullied at school (14.9%), the prevalence was higher among Asian American students than among Black students (9.2% and 13.1%, respectively) but tended to be lower than among students in all other racial and ethnic groups (varied pattern of significance). Asian American students had a higher prevalence of sexual dating violence victimization than Black students (10.9% vs 7.6%). The prevalence of being in a physical fight (2.1%) was lower among female Asian American students than among female students in all other racial and ethnic groups. For being bullied electronically (13.8%) and being bullied at school (15.8%), the prevalence among female Asian American students was lower than among female Hispanic and White students but not different from female students in other racial and ethnic groups. The prevalence of sexual violence victimization among female Asian American students (14.3%) was not different from the prevalence among female students in other racial and ethnic groups, except that the prevalence was higher than among female Black students (9.0%). The prevalence of carrying a weapon at school was significantly lower among male Asian American students compared with all groups except male Black students (4.0% vs 5.5%), while among male Asian American students, the prevalence of being in a physical fight and being threatened or injured with a weapon was significantly lower than the prevalence among male students of all other racial and ethnic groups except male White students.
Violence-related experiences among high school students, by race, ethnicity, and sex, national Youth Risk Behavior Survey, 2011-2019 a
Abbreviation: NHPI, Native Hawaiian/Pacific Islander.
During the 30 days before the survey.
During the 12 months before the survey.
For the years 2013-2019. Among students who reported dating during the 12 months before the survey.
Sample size of race and ethnicity overall does not add to total sample size because of missing data (2.4%, or 1766 observations).
“Other” race and ethnicity not included in table because of limited interpretability.
Significantly different at P < .05 from NHPI; determined by t test.
Significantly different at P < .05 from non-Hispanic Black; determined by t test.
Significantly different at P < .05 from Hispanic; determined by t test.
Significantly different at P < .05 from non-Hispanic White; determined by t test.
Sample size does not add to total by each race and ethnicity category because of missing data for sex (0.2%, or 175 observations).
For NHPI students, the prevalence of carrying a weapon at school (7.6%), being bullied electronically (16.0%), being bullied at school (20.0%), and sexual dating violence victimization (13.4%) was significantly higher than among Black students (Table 4). NHPI students also had a significantly greater prevalence of being in a physical fight (15.4%) or being threatened or injured with a weapon (11.6%) compared with Hispanic and White students. NHPI students had a significantly higher prevalence of missing school due to safety concerns (9.0%), physical dating violence victimization (14.0%), and ever experiencing forced sex (11.9%) compared with White students (5.1%, 8.4%, and 6.8%, respectively). For carrying a weapon at school, the prevalence among female Asian American students was higher than among female NHPI students but lower than among female students in other racial and ethnic groups. The prevalence of being in a physical fight among female NHPI students (12.3%) was significantly higher than the prevalence among female Hispanic (7.1%) and White (3.7%) students. The prevalence of electronic bullying among female NHPI students (19.9%) was significantly higher than among female Black students (11.6%), while the prevalence of being bullied at school among female NHPI students (18.1%) was significantly lower than among female White students (26.9%). Among male NHPI students, the prevalence of carrying a weapon at school and being bullied at school was significantly greater than the prevalence observed among male Black and Hispanic students. The prevalence of being threatened or injured with a weapon (14.9%), missing school because of feeling unsafe (8.9%), and experiencing physical dating violence (14.4%) was significantly greater among male NHPI students than among male White students (6.7%, 3.9%, and 6.0%, respectively). The prevalence of experiencing sexual dating violence victimization and forced sex was significantly greater among male NHPI students than among male Hispanic and White students.
Suicidal Behaviors/Experiences
The prevalence of having seriously considered suicide (18.2%) and having made a suicide plan (15.3%) was higher among Asian American students than among Black students (14.6% and 12.5%, respectively) but not different from that among NHPI, Hispanic, or White students (Table 5). The prevalence of persistent feelings of sadness or hopelessness was lower among Asian American students (28.8%) than among Hispanic students (35.7%) but not different than among NHPI students (31.8%). The prevalence of persistent feelings of sadness or hopelessness was significantly lower among female Asian American students (35.1%) than among female Hispanic students (46.8%). For persistent feelings of sadness or hopelessness (22.8%) and having made a suicide plan (12.4%), the prevalence among male Asian American students was significantly higher than among male Black students (18.7% and 8.7%, respectively). The prevalence of seriously having considered suicide was higher among male Asian American students than among Black, Hispanic, and White male students.
Mental health and nonfatal suicidal behaviors among high school students, by race, ethnicity, and sex, national Youth Risk Behavior Survey, 2011-2019 a
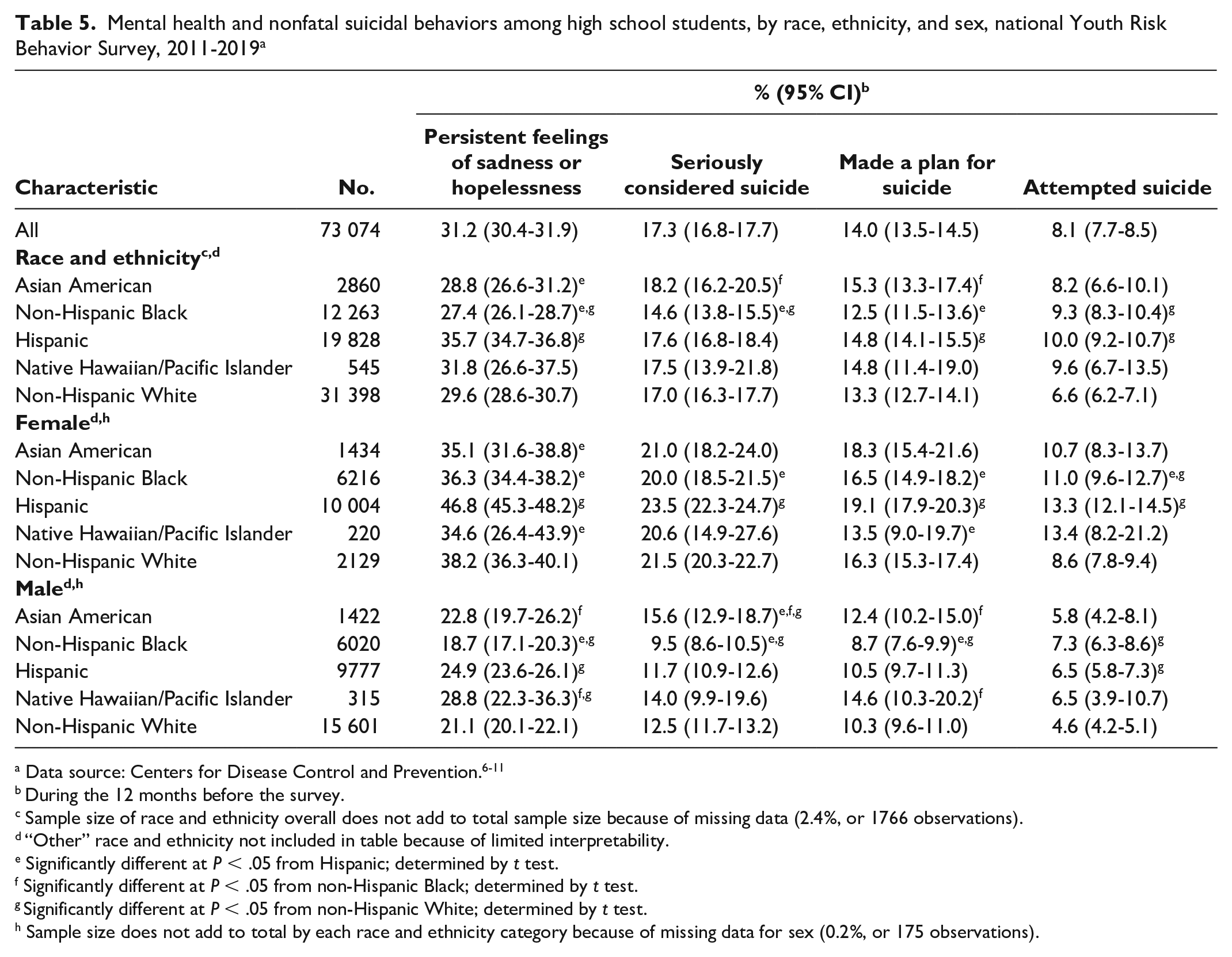
During the 12 months before the survey.
Sample size of race and ethnicity overall does not add to total sample size because of missing data (2.4%, or 1766 observations).
“Other” race and ethnicity not included in table because of limited interpretability.
Significantly different at P < .05 from Hispanic; determined by t test.
Significantly different at P < .05 from non-Hispanic Black; determined by t test.
Significantly different at P < .05 from non-Hispanic White; determined by t test.
Sample size does not add to total by each race and ethnicity category because of missing data for sex (0.2%, or 175 observations).
The prevalence of persistent feelings of sadness or hopelessness (34.6%) and having made a suicide plan (13.5%) was significantly lower among female NHPI students than among female Hispanic students (46.8% and 19.1%, respectively) (Table 5). For persistent feelings of sadness or hopelessness (28.8%), the prevalence was significantly higher among male NHPI students than among male Black (18.7%) and White (21.1%) students, while for having made a suicide plan (14.6%), the prevalence was significantly higher among male NHPI students than among male Black students (8.7%).
Discussion
Our findings are generally consistent with a 2001-2007 YRBS study, wherein Asian American students had a lower prevalence of most health-risk behaviors compared with NHPI students. 14 Asian American students had significantly lower prevalence rates than NHPI students for all substance use behaviors; most sexual risk behaviors, except no condom use and use of alcohol or drugs at last sexual intercourse; and violence-related experiences, except bullied electronically, missed school because felt unsafe, and sexual dating violence victimization. The prevalence of nonfatal suicidal behaviors did not differ between Asian American and NHPI students.
Studies have suggested differences in protective factors for substance use between NHPI and Asian American adolescents—with parental support acting as a positive buffer against engaging in substance use among Asian American adolescents but with conflicting evidence for such protection among NHPI adolescents.5,15,16 Wills et al noted that their measurement model narrowly defined a nuclear NHPI parental system and could be improved by including extended family members given the potential influence of other family members on the social environment of NHPI adolescents and their decisions on substance use. 16 Substance use among Asian American students may be explained by acculturative stress, correlated with differential rates of alcohol use; acculturation has been associated with increased alcohol consumption among Asian American students. 17 In contrast, enculturation (proximity to Asian cultural heritage) had a negative association. 17 One study suggested that a sense of ethnocultural identity may protect against substance misuse among Native Hawaiian students. 18 Nativity may also explain differences in Asian American subgroups. One study showed that US-born Asian Americans had higher rates of binge drinking than non–US-born Asian Americans. 19 When data on Asian Americans are aggregated, rates of alcohol use among Asian American populations are deceptively low, obscuring groups at high risk of alcohol misuse, such as Filipino and Korean Americans. 19 One study found that multiracial, NHPI, and American Indian/Alaska Native adolescents disproportionately engaged in illicit drug use behaviors. 20 Research has demonstrated the effectiveness of promoting protective factors for preventing substance use behaviors, such as school connectedness, and strengths-based family-centered prevention programs (eg, parent–child communication, parent training, parental modeling).21-23 One study of NHPI adolescents identified several significant protective factors for substance use among NHPI adolescents in the school context, such as school-based programs, teachers as role models, and peer relationships. 5
Studies have demonstrated that violence-related experiences are a growing concern for Asian American and NHPI adolescents.21,24 For Asian American adolescents, low levels of acculturation and cultural marginality are risk factors for fear, victimization, and bullying, but the impact of acculturation on adolescent aggression and violence can be mediated by family dynamics. 24 For Native Hawaiian adolescents, Hawaiian family structure emphasizes interconnectedness and cohesiveness. 16 Familial and cultural contexts serve as a risk and a protection for concerning behaviors among Native Hawaiian adolescents. 16 When data were not disaggregated, school interconnectedness also protected against violent attitudes among adolescents. 21 Therefore, mitigation approaches to reduce violence among Asian American and NHPI adolescents may also include culturally competent school programs that emphasize school interconnectedness and cultural and familial dynamics.
A systematic review of suicidal behaviors among Asian American and NHPI people aged ≤18 years (groups not disaggregated) provides some context that depression and suicidal ideation stem from familial conflict, perceived racial discrimination, and differences in acculturation, whereas a sense of subgroup racial identity may protect against suicidal ideation. 25 For NHPI, culturally informed prevention programs rooted in indigenous values have been found to protect against suicide. 26 Cultural beliefs and stigma about mental health may result in underreporting of psychological distress among Asian American adolescents, delaying treatment. 25 One study found that Asian American college students had low rates of mental health diagnosis but high levels of suicidal ideation and attempts. 27 Depictions of Asian American and NHPI people as “model minorities” is correlated with higher levels of psychological distress and negative perceptions of help seeking. 28 Suicide risk mitigation could involve creating family-centered approaches to mental health care and strengthening parental access to mental health resources for adolescents. 25
Health behavior data for Asian American and NHPI adolescents are needed to understand and mitigate health disparities. Combining several years of data is necessary for reliable prevalence rates because of insufficient sample sizes for generating stable prevalence estimates. Federal data that separately examine NHPI populations are also limited because of geographical dispersion.29,30 Asian American and NHPI populations are heterogeneous, and differences in historical experiences, acculturation, and beliefs may result in differential health outcomes. When differences in health behaviors are being examined, it is important to consider structural and social conditions (eg, access to health care, education, economic stability) that influence the health outcomes of racial and ethnic minority populations in the United States. 31 To improve health-risk behaviors and prevent adverse experiences among adolescents, it is important to focus on the social determinants of health. 31 In recognition of the role of social determinants of health on health outcomes, Healthy People 2030 aims to address these upstream factors with the goal of eliminating health disparities and achieving health equity. 32
Limitations
This study had several limitations. First, we combined data across 8 years, so the prevalence of some behaviors and experiences may have differed slightly over time. Second, we could not examine health disparities within Asian American and NHPI subgroups by using YRBS data. Third, because of limited interpretability, we did not present data for the 4.8% of our sample who identified as multiracial or “other.” Fourth, our study did not have data on contextual and cultural factors that might explain the behavioral patterns observed among the racial and ethnic groups examined.
Conclusion
Our study demonstrated that the prevalence of health-risk behaviors varies among Asian American and NHPI adolescents. From a health equity perspective, we should disaggregate these groups further so that potential differences in behavioral patterns can be identified and addressed. Data collection methodologies may consider oversampling populations to improve the availability and utility of data on racial and ethnic minority populations.
Footnotes
Acknowledgements
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.