
Abstract
Objectives:
Minimal research has assessed COVID-19’s unique impact on the Native Hawaiian/Pacific Islander (NH/PI) population—an Indigenous-colonized racial group with social and health disparities that increase their risk for COVID-19 morbidity and mortality. To address this gap, we explored the scope of COVID-19 outcomes, vaccination status, and health in diverse NH/PI communities.
Methods:
NH/PI staff at partner organizations collected survey data from April through November 2021 from 319 community-dwelling NH/PI adults in 5 states with large NH/PI populations: Arkansas, California, Oregon, Utah, and Washington. Data were analyzed with descriptive statistics, Pearson χ2 tests, independent and paired t tests, and linear and logistic regression analyses.
Results:
During the COVID-19 pandemic, 30% of survey participants had contracted COVID-19, 16% had a close family member who died of the disease, and 64% reported COVID-19 vaccine uptake. Thirty percent reported fair/poor health, 21% currently smoked cigarettes, and 58% reported obesity. Survey participants reported heightened COVID-19–related psychosocial distress (mean score = 4.9 on 10-point scale), which was more likely when health outcomes (general health, sleep, obesity) were poor or a family member had died of COVID-19. Logistic regression indicated that age, experiencing COVID-19 distress, and past-year use of influenza vaccines were associated with higher odds of COVID-19 vaccine uptake (1.06, 1.18, and 7.58 times, respectively).
Conclusions:
Our empirical findings highlight the acute and understudied negative impact of COVID-19 on NH/PI communities in the United States and suggest new avenues for improving NH/PI community health, vaccination, and recovery from COVID-19.
Native Hawaiian/Pacific Islander (NH/PI) people are an understudied Indigenous-colonized racial group that has been reported in limited county, state, and public news sources to have among the nation’s sharpest disparities in COVID-19 morbidity and mortality.1,2 Originating from diverse nations and US territories in Polynesia, Micronesia, and Melanesia, NH/PI people are the third-fastest growing racial group in the United States, increasing in population by >60% from 2000 to 2019. 3 Despite the rapid growth of this population and its exposure to numerous cultural traumas at the hands of the United States,4 -6 reliable and targeted US public health data on NH/PI people have been largely unavailable during the COVID-19 pandemic. This lack of data has arguably hindered public health’s efforts to understand and address COVID-19’s potential negative impact on NH/PI communities while limiting the ability to prevent similar public health crises from disproportionately affecting NH/PI communities in the future.1,2
Within the sparse NH/PI health literature, NH/PI people appear to have numerous social, economic, and health disparities, including low income, poverty, and limited education, as well as high levels of stigma and discrimination, obesity, diabetes, cardiovascular disease, cancer, and substance use.7 -13 This dual burden of socioeconomic challenges and chronic disease is suspected to play a major role in increasing the risk for severe COVID-19 outcomes among the NH/PI population14,15 because tobacco use, respiratory and cardiovascular disease, diabetes, and cancer, which NH/PI people experience at high rates, are risk factors for severe COVID-19 complications and death.16 -21 Furthermore, NH/PI people have other risk factors for negative COVID-19 outcomes: (1) overrepresentation in low-wage essential jobs (eg, factory workers, food service, health care) and (2) living in large multigenerational households and dense communities that increase infection risk by limiting social distancing, isolation and quarantining, and other COVID-19–protective behaviors.15,22 -25
Local data from states with substantial NH/PI populations suggest that NH/PI people may have the highest rates of COVID-19 infections and deaths of any US racial or ethnic group. 25 In 2020, news reports and public dashboards indicated that NH/PI people experienced up to 2.2- to 3.1-times higher infection rates, 14 up to 10-times higher hospitalization rates, 26 and 2.6- to 12-times higher mortality rates27 -29 from COVID-19 as compared with non–NH/PI people. Thus, by March 2021, NH/PI people appeared to have the highest per capita COVID-19 death rate in 90% of states that reported deaths among these individuals. 1
However, despite this initial evidence showing the disproportionate impact of the COVID-19 pandemic on NH/PI communities, almost no studies have examined or described this negative impact as perceived and reported by the NH/PI residents of these communities. Instead, existing data have almost exclusively relied on raw numbers of NH/PI infections, hospitalizations, and deaths as reported by clinics, hospitals, testing sites, and other secondary government or health care sources—likely underrepresenting COVID-19’s true impact on NH/PI communities. Accordingly, in 2020, the National Institute on Alcohol Abuse and Alcoholism and the National Institute on Drug Abuse funded a detailed community-based study to obtain a comprehensive picture of COVID-19’s effects on the health of diverse NH/PI communities in the United States.
The present analysis is based in part on this community-based study, and this article reports on 3 core objectives of the study. The first was to assess the patterns of COVID-19 outcomes affecting NH/PI communities, including levels of COVID-19 vaccine uptake and psychosocial distress. The second was to evaluate general health in NH/PI communities with health indicators defined by the Centers for Disease Control and Prevention as linked to increased risk of chronic disease: obesity, sleep, and cigarette smoking. 30 The third was to model which COVID-19 outcomes and health indicators predicted COVID-19 distress and vaccine uptake in NH/PI communities. We particularly sought to identify predictors of COVID-19 vaccine uptake because of the importance of promoting repeated vaccine/booster uptake in NH/PI communities to counteract COVID-19’s growing endemicity31 -33 and evolving variants that elude prior immunity.34,35
Methods
Study Sample and Recruitment
The institutional review board at the University of California, Riverside approved the study protocols. To obtain a diverse sample across NH/PI ethnicities, ages, and sex/genders, trained NH/PI staff from partner organizations recruited 319 NH/PI adults (aged ≥18 years) from April through November 2021 in 5 US states with sizable NH/PI populations: Arkansas, California, Oregon, Utah, and Washington. To recruit the sample, we used established best practices for capturing nonprobabilistic data from medically underserved populations36,37; these practices resulted in the successful recruitment of hundreds of NH/PI participants in our previous National Institutes of Health–funded studies.38 -40 That is, NH/PI staff from our partner organizations recruited participants by distributing study advertisements to NH/PI residents in their communities via email, telephone, in-person visits, and neighborhood organizations (eg, churches, cultural centers). To ensure that people of diverse ages and generations could participate in this exploratory study, staff administered informed consent and a 30- to 45-minute survey either online via Qualtrics (by sending a personalized study link to each participant’s email address) or in person or by telephone via staff using paper-and-pencil survey packets. Although 86% of NH/PI people are English proficient, 41 for NH/PI participants with lower English proficiency, staff administered the survey by orally translating items into participants’ preferred language. Participants received $20 for survey completion.
Measures
Demographic characteristics and health
Demographic variables were age, sex/gender, education, annual household income, marital status, and NH/PI ethnicity (Polynesian, Micronesian, Melanesian). General health was assessed by using the well-established item “In general, would you say your health is excellent, very good, good, fair, or poor?” Overweight and obesity were determined by calculating participants’ body mass index as weight in kilograms divided by height in meters squared. Overweight was defined as 25.0 to <30.0 kg/m2 and obesity as ≥30.0 kg/m2 by using self-reported height and weight. Current smoking was identified through affirmative responses of “some days” or “every day” to the query “Do you now smoke cigarettes every day, some days, or not at all?” 42 To assess sleep behavior, participants were asked, “In the past 2 weeks, on average, how many hours of sleep did you get in a 24-hour period?” Some participants were also asked, “Before the pandemic, on average, how many hours of sleep did you get in a 24-hour period?”
COVID-19 outcomes
To assess COVID-19 outcomes, we adapted items from the Coronavirus Health Impact Survey version 0.3—a survey jointly developed by the National Institute of Mental Health and leading medical institutions 43 —using feedback from our NH/PI community partners. Specifically, we queried whether participants had contracted COVID-19. We then asked whether participants had a close family member who had symptoms or was diagnosed with COVID-19, was hospitalized for COVID-19, or died of COVID-19. 43 To assess COVID-19–related distress, participants were asked to rate their distress by answering the question “Overall, how much distress have you experienced related to COVID-19 during the crisis?” Response options ranged from 1 (no distress) to 10 (extreme distress).
COVID-19 and influenza vaccine uptake
COVID-19 vaccine uptake was assessed by using the yes/no item “I have taken a vaccine for COVID-19.” Influenza vaccine uptake was assessed via the yes/no item “Did you get a flu vaccine this season (in the last year)?” We inquired about influenza vaccine uptake because influenza is another respiratory illness with an available and well-established adult vaccine that must be repeatedly used—providing us with a close analogue for evaluating NH/PI uptake of COVID-19 vaccines. 44
Statistical Analyses
We conducted study analyses in SPSS version 27 (IBM Corp). Descriptive statistics analyzed frequencies, means, and SDs. We used Pearson χ2 tests and independent t tests to examine significant differences in sex/gender (female, male, transgender, nonbinary) in frequencies and mean scores, and we used paired t tests to examine significant differences in average hours of sleep before versus during the COVID-19 pandemic. We performed linear regression to determine which demographic variables, chronic disease–related health indicators, and COVID-19 outcomes were significantly associated with increased COVID-19 distress. To identify potential avenues for promoting COVID-19 vaccine/booster uptake among NH/PI adults, we performed logistic regression to determine which demographic characteristics, health indicators, and COVID-19 outcomes were associated with COVID-19 vaccine uptake. For both exploratory models, the independent variables were as follows: age, sex/gender, education, annual household income, and marital status (demographic variables); general health, obesity, sleep hours, and current cigarette smoking (health indicators); and COVID-19 for self or close family member and family member hospitalized or died of COVID-19 (COVID-19 outcomes). For the COVID-19 vaccine uptake model, we included COVID-19 distress and influenza vaccine uptake as additional independent variables. All tests used a minimum significance level of P < .05.
Results
Sample Demographic Characteristics and Health Indicators
Of the 319 survey participants, 55% (n = 177) were women, 30% (n = 97) were men, and 14% (n = 45) identified as transgender or nonbinary; the average age was 35.2 years (Table 1). Fifty-four percent were of Polynesian heritage (eg, Native Hawaiian, Samoan, Tongan), 38% were of Micronesian heritage (eg, Marshallese, Chuukese), and 2% were of Melanesian heritage (eg, Fijian).
Characteristics of participants aged ≥18 years, by sex/gender, in a survey of Native Hawaiian/Pacific Islander people (N = 319) about the impact of COVID-19 on Native Hawaiian/Pacific Islander people in 5 US states, April–November 2021 a
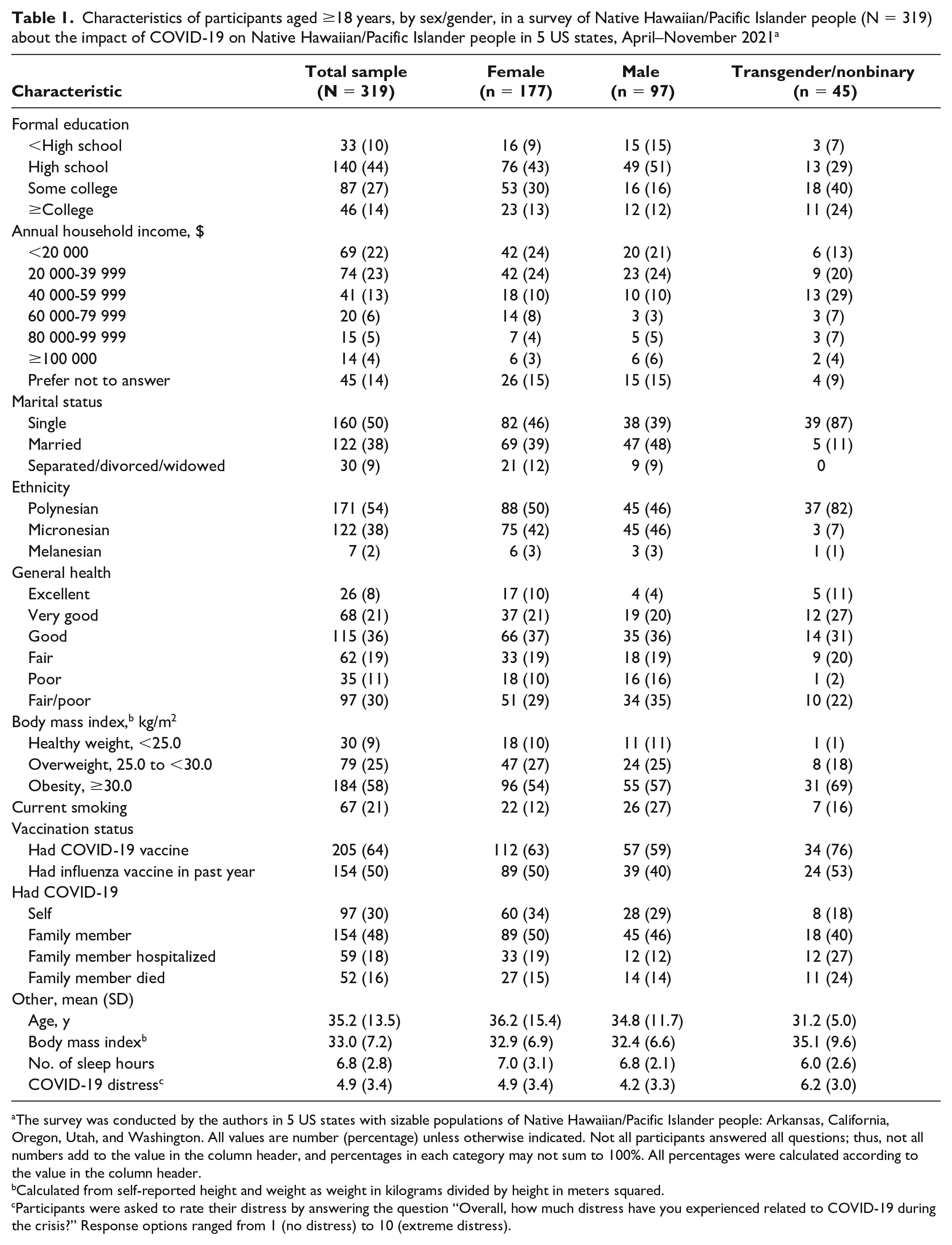
The survey was conducted by the authors in 5 US states with sizable populations of Native Hawaiian/Pacific Islander people: Arkansas, California, Oregon, Utah, and Washington. All values are number (percentage) unless otherwise indicated. Not all participants answered all questions; thus, not all numbers add to the value in the column header, and percentages in each category may not sum to 100%. All percentages were calculated according to the value in the column header.
Calculated from self-reported height and weight as weight in kilograms divided by height in meters squared.
Participants were asked to rate their distress by answering the question “Overall, how much distress have you experienced related to COVID-19 during the crisis?” Response options ranged from 1 (no distress) to 10 (extreme distress).
Assessing health during the pandemic, 30% (n = 97) of participants cited fair/poor health and only 8% reported excellent health; 58% and 25% of participants had body mass indexes indicating obesity and overweight, respectively; and 21% of participants were current cigarette smokers (Table 1). Men had a significantly higher current smoking rate than women (27% vs 12%, χ21, 190 = 5.0, P = .03). Participants had a mean (SD) 6.8 (2.8) hours of sleep per night during the pandemic, which was a significant decrease from the 7.6 (3.0) hours of sleep before the pandemic among the 136 participants who reported their average prepandemic sleep hours (t135 = 4.28, P < .001).
COVID-19 Outcomes and Vaccine Uptake
Thirty percent of survey participants indicated being diagnosed with COVID-19 (Table 1). Approximately one-half of participants reported having a close family member with COVID-19; 18% had a close family member who was hospitalized with COVID-19 and 16% had a close family member who died of COVID-19. Elevated levels of COVID-19 distress were noted among participants; the mean (SD) COVID-19 distress score was 4.9 (3.4).
Sixty-four percent of participants reported taking the COVID-19 vaccine, and 48% indicated getting the influenza vaccine in the past year. We found no significant differences by sex in COVID-19 vaccine uptake, but women had significantly higher rates than men of past-year influenza vaccine uptake (50% vs 40%, χ21, 262 = 4.1, P = .04).
Linear Regression of COVID-19 Distress
We found several significant associations in the linear regression performed to determine which demographic variables, chronic disease–related health indicators, and COVID-19 outcomes were significantly associated with increased COVID-19 distress in our study sample (Table 2). Among the demographic variables examined, identifying as transgender/nonbinary gender (vs female) was significantly associated with greater COVID-19 distress (β = .21, P = .007). For our health indicators, better general health was significantly associated with lower COVID-19 distress (P = .04), while fewer sleep hours per night (P = .02) and obesity (P < .001) were significantly associated with greater COVID-19 distress. Also, having a close family member die of COVID-19 was significantly associated with greater COVID-19 distress (P = .04).
Linear regression for COVID-19 distress by demographic characteristics, health indicators, and COVID-19 outcomes from a survey of Native Hawaiian/Pacific Islander people (N = 319) aged ≥18 years about the impact of COVID-19 on Native Hawaiian/Pacific Islander people in 5 US states, April–November 2021 a
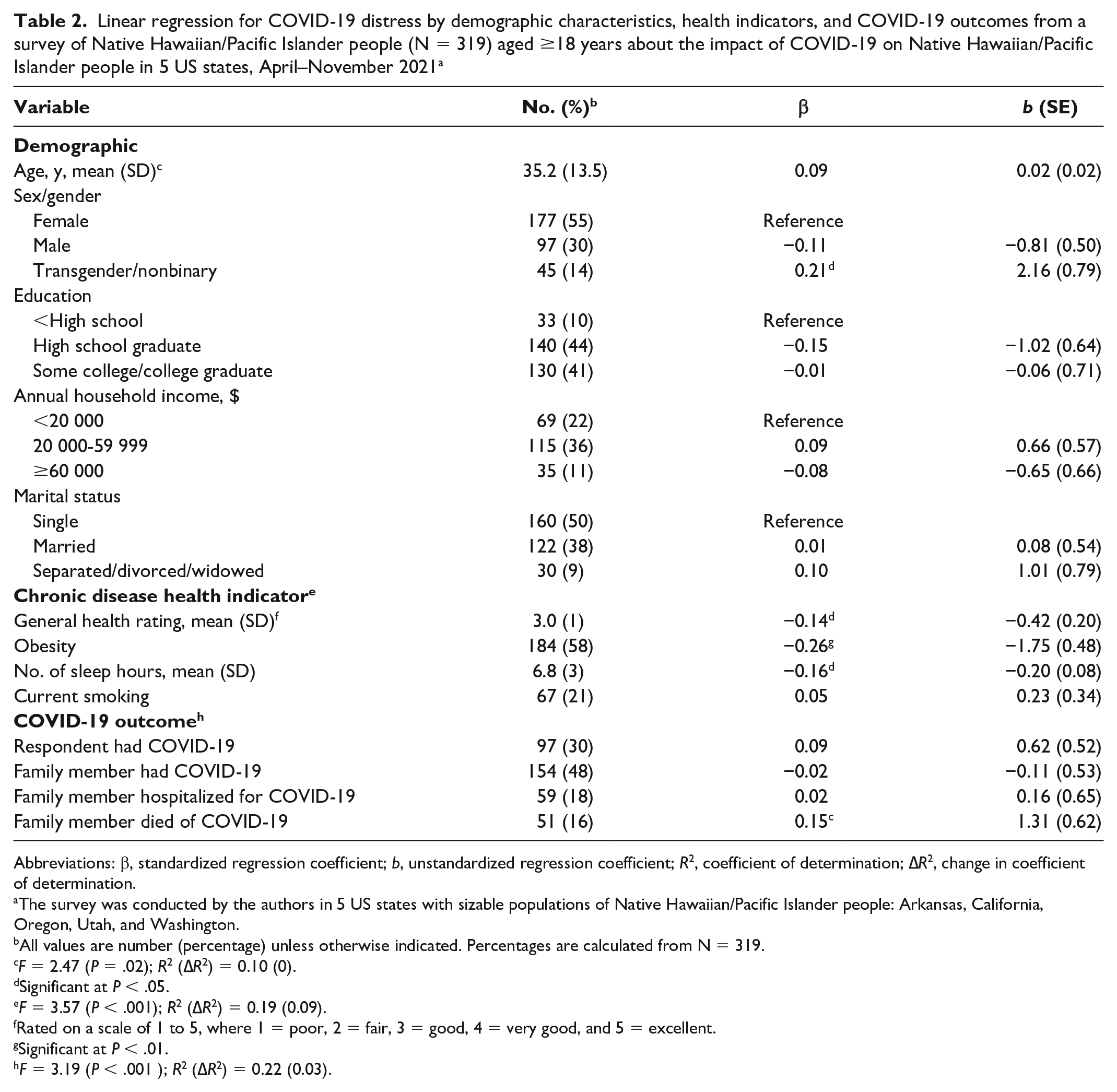
Abbreviations: β, standardized regression coefficient; b, unstandardized regression coefficient; R2, coefficient of determination; ∆R2, change in coefficient of determination.
The survey was conducted by the authors in 5 US states with sizable populations of Native Hawaiian/Pacific Islander people: Arkansas, California, Oregon, Utah, and Washington.
All values are number (percentage) unless otherwise indicated. Percentages are calculated from N = 319.
F = 2.47 (P = .02); R2 (∆R2) = 0.10 (0).
Significant at P < .05.
F = 3.57 (P < .001); R2 (∆R2) = 0.19 (0.09).
Rated on a scale of 1 to 5, where 1 = poor, 2 = fair, 3 = good, 4 = very good, and 5 = excellent.
Significant at P < .01.
F = 3.19 (P < .001 ); R2 (∆R2) = 0.22 (0.03).
Logistic Regression of COVID-19 Vaccine Uptake
We found several significant associations in the logistic regression conducted to determine which demographic characteristics, health indicators, and COVID-19 outcomes were associated with COVID-19 vaccine uptake (Table 3). A 1-year increase in age was significantly associated with 1.06-times greater odds of COVID-19 vaccine uptake (P = .01), and a 1-point increase in COVID-19 distress was significantly associated with 1.18-times greater odds of COVID-19 vaccine uptake (P = .01). In contrast, being married (vs single) was significantly associated with 0.17-times lower odds of COVID-19 vaccine uptake (P < .001), and having a close family member hospitalized with COVID-19 was significantly associated with 0.24-times lower odds (P = .01). Finally, participants who received an influenza vaccine in the past year (vs did not) had 7.58-times greater odds of COVID-19 vaccine uptake (P < .001).
Logistic regression for COVID-19 vaccine uptake by demographic characteristics, health indicators, and COVID-19 outcomes from a survey of Native Hawaiian/Pacific Islander people (N = 319) aged ≥18 years about the impact of COVID-19 on Native Hawaiian/Pacific Islander people in 5 US states, April–November 2021 a
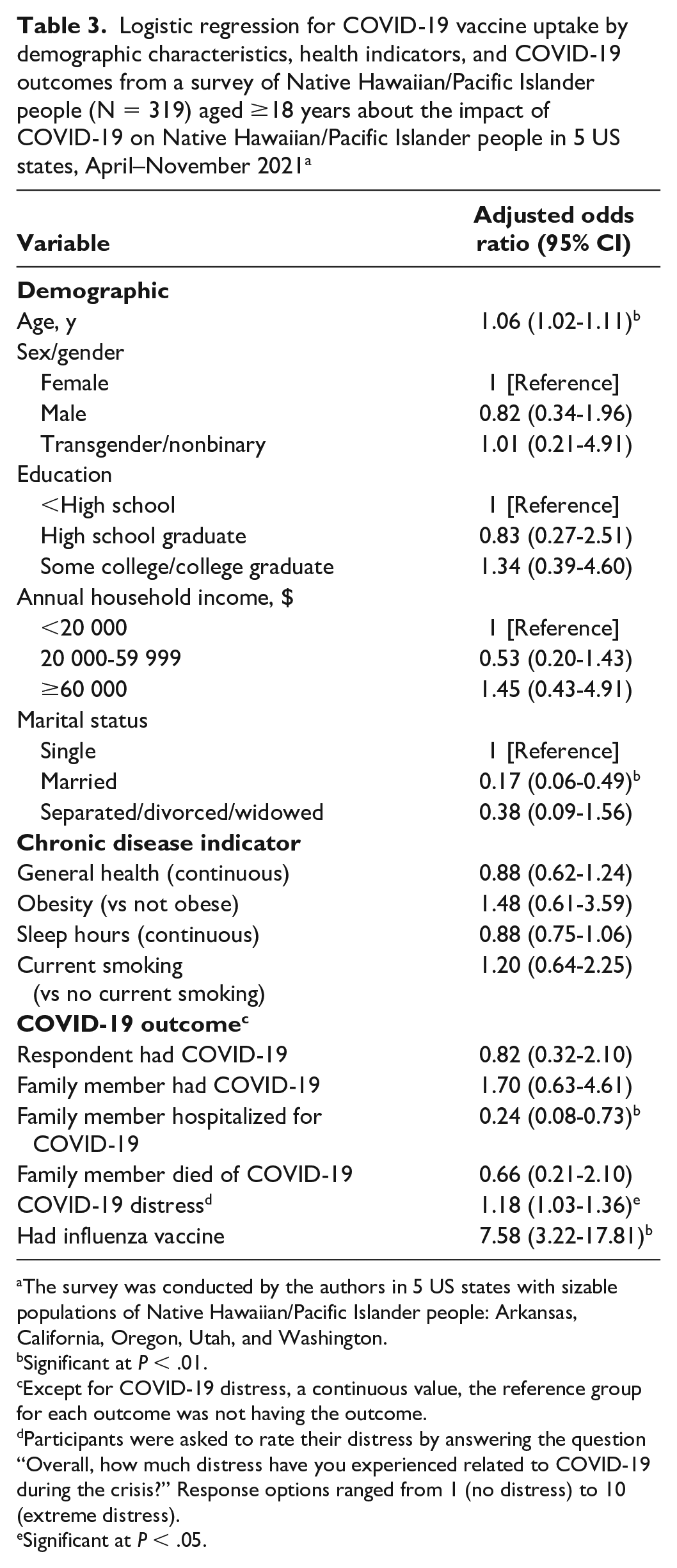
The survey was conducted by the authors in 5 US states with sizable populations of Native Hawaiian/Pacific Islander people: Arkansas, California, Oregon, Utah, and Washington.
Significant at P < .01.
Except for COVID-19 distress, a continuous value, the reference group for each outcome was not having the outcome.
Participants were asked to rate their distress by answering the question “Overall, how much distress have you experienced related to COVID-19 during the crisis?” Response options ranged from 1 (no distress) to 10 (extreme distress).
Significant at P < .05.
Discussion
To our knowledge, our study is one of the first empirical studies to collect, analyze, and report data on the health of the NH/PI population in the United States during COVID-19. Our multistate findings show that NH/PI people have been deeply affected by COVID-19: almost one-third of our sample contracted COVID-19, and one-half had a close family member who contracted it. Additionally, nearly 1 in 5 NH/PI people in our sample stated that a close family member died of COVID-19, suggesting that COVID-19 mortality may be disproportionately concentrated in NH/PI communities, given the overall US COVID-19 mortality rate of 250 deaths per 100 000 people. 45
These empirical findings cohere with (1) limited US state/county data that report elevated COVID-19 infection and mortality rates among NH/PI people 1 and (2) numerous community reports received by our team and broadcast in the news media indicating that COVID-19 funerals have become commonplace in NH/PI communities during the pandemic. 46 Because NH/PI funerals are culturally vital social gatherings that involve prolonged close contact, singing, and communal consumption of food and drink, they can increase the risk of exposure to COVID-19 and may act as superspreader events in NH/PI communities.47,48
When we examined NH/PI health during the COVID-19 pandemic, nearly one-third of participants cited fair or poor health, and 83% met criteria for overweight or obesity, a major risk factor for severe COVID-19.49,50 On average, participants reported sleeping less than the 7 hours per night recommended by the American Academy of Sleep Medicine—placing NH/PI people at increased risk for impaired immune function and adverse health outcomes, such as obesity, diabetes, hypertension, cardiovascular disease, and early mortality. 51 Additionally, 21% of participants were current cigarette smokers, substantially exceeding the current US adult smoking rate of 14%. 52 Because smoking-related diseases are the leading causes of NH/PI mortality13,53,54 and a major risk factor for severe COVID-19,19,55 this finding underscores the need to develop effective culturally targeted smoking cessation interventions to prevent and reduce heightened risk for tobacco-related diseases and COVID-19 morbidity and mortality among NH/PI people—especially because they are less likely than people in other racial and ethnic groups to quit smoking56,57 and rarely use services or interventions that have not been culturally adapted to their population.38,58,59
On a positive note, our data revealed that 64% of NH/PI participants had received the COVID-19 vaccine at assessment (April–November 2021). Although this rate was taken from a large nonprobability sample, it is higher than rates of other population groups who had received at least 1 COVID-19 vaccine dose as of December 13, 2021: 58% among White people, 56% among Latina/Latino people, and 51% among African American people. 60 Thus, while NH/PI people have been noted to consistently underutilize health care services,58,61 our data suggest that they may be generally receptive to receiving COVID-19 vaccines.
When we explored which factors were associated with COVID-19–related vaccination among NH/PI people, regression results revealed that older age, experiencing COVID-19 distress, and receiving a past-year influenza vaccine were positively associated with COVID-19 vaccination after accounting for demographic characteristics, health indicators, and COVID-19 outcome variables. Receiving the influenza vaccine was the strongest predictive factor and was associated with >7 times greater likelihood of receiving the COVID-19 vaccine. Thus, health professionals may be aided in increasing COVID-19 vaccine and booster uptake in NH/PI communities by designing health communications messaging that (1) is targeted to young NH/PI people, who appear less likely than older NH/PI people to receive COVID-19 vaccines, and (2) increases NH/PI awareness and uptake of the influenza vaccine, which could serve as a bridge to COVID-19 vaccine acceptance and use among vaccine-hesitant NH/PI people.
On average, in our survey, NH/PI participants reported experiencing substantial COVID-19–related distress (scoring 5 on a 10-point scale), which was independently predicted by 3 of our study’s 4 health indicators after accounting for demographic characteristics, health indicators, and COVID-19 outcomes. Most notably, poorer general health and fewer sleep hours were significantly associated with greater COVID-19 distress, revealing a possible connection among general health, sleep, and psychosocial distress among NH/PI people during COVID-19. 62
Limitations
Our study had several potential limitations. First, we used nonprobability sampling. However, traditional probability sampling methods typically have great difficulty capturing representative sampling frames from medically underserved communities,63,64 necessitating the use of community-engaged and community-accepted nonprobabilistic approaches. 65 Accordingly, to mitigate potential bias and strengthen study generalizability in this nonprobabilistic study, we obtained a diverse sample of NH/PI ethnicities, ages, and sex/genders by (1) recruiting diverse NH/PI participants from multiple states in the western and southern United States (the continental US regions with the largest NH/PI populations 66 ) and (2) using multiple survey formats (eg, online, telephone, in-person) to accommodate the survey preferences of diverse NH/PI participants. Second, the current study did not assess NH/PI adults living in the Pacific region, limiting the generalizability of our study findings to US-dwelling NH/PI adults. Thus, although many Pacific Island nations (eg, Marshall Islands, American Samoa) experienced low rates of COVID-19 infection, hospitalization, and death relative to rates in the United States (eg, 17 confirmed cases and 0 deaths in the Marshall Islands 67 as of May 2022), because of extensive and prolonged emergency mitigation efforts (eg, travel bans, COVID-19 lockdowns), there is a need to investigate the impact of COVID-19 on NH/PI populations throughout the Pacific.
Third, because of the absence of psychometrically validated measures of COVID-19–related distress at the time of our study, our COVID-19 distress item lacked psychometric validation. Fourth, our linear regression model did not apply nonlinear approaches, particularly with response to age. Finally, because our study was a community-based study uniquely focused on illuminating the COVID-19–related challenges experienced by NH/PI communities during the pandemic, we did not include a comparison racial or ethnic group (eg, non-Hispanic White adults). Future studies may wish to compare the findings of our NH/PI-focused study with findings from studies of other racial and ethnic groups in the United States, particularly the non-Hispanic White population, by using large epidemiologic datasets to identify and isolate the precise scope of racial and ethnic differences (NH/PI vs White) on our key COVID-19–related variables (eg, distress, vaccine uptake). Despite these limitations and given the absence of empirical data to date about the negative impact of COVID-19 on NH/PI communities—in part caused by the small size of the NH/PI population, which renders it challenging to assess with traditional health survey methods (eg, random-digit dial)—we contend that our study findings may serve as a useful initial step toward understanding and eventually lessening the deleterious effects of COVID-19 on NH/PI populations in the United States.
Conclusions
Our study results are among the first to empirically demonstrate that despite receiving scant COVID-19–related research and attention, NH/PI communities have elevated rates of COVID-19 infection and COVID-19–related loss, distress, and poor health. Our novel findings reinforce calls from policy makers and researchers for greater attention and funding for research to prevent and reduce the health disparities among NH/PI people, 68 including funding efforts to disaggregate existing datasets and dashboards to address harmful gaps in reporting on COVID-19 among NH/PI people,69,70 as mandated by the US Office of Management and Budget. 25 Additionally, given the endemic nature of COVID-19 and the high levels of COVID-19 exposure, distress, and loss experienced by NH/PI communities, it is vital that future studies monitor and evaluate not only COVID-19–related health but also the mental health and substance use issues facing NH/PI communities to better understand how to address the ongoing mental and physical health consequences of this pandemic, thereby improving the health of this neglected racial population.
Footnotes
Acknowledgements
We express our deepest appreciation to our community partners, the National Tongan American Society, the Arkansas Coalition of the Marshallese, the United Territories of Pacific Islanders Alliance, and the Office of Samoan Affairs, for their hard work and support for this project during the COVID-19 pandemic.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Institutes of Health: the National Institute on Drug Abuse (R34 DA049989) and the National Institute on Alcohol Abuse and Alcoholism (R21 AA026689-S1). The content is solely the responsibility of the authors and does not represent the official views of the National Institutes of Health, National Institute on Drug Abuse, or National Institute on Alcohol Abuse and Alcoholism.