
Abstract
Objectives:
The COVID-19 pandemic affected consumers’ access to oral health care. This study evaluated factors associated with teledentistry use among US adults from June 2019 through June 2020.
Methods:
We used data from a nationally representative survey of 3500 consumers. We estimated teledentistry use and adjusted associations with respondents’ concerns about the impacts of the pandemic on health and welfare and with their sociodemographic characteristics using Poisson regression models. We also analyzed teledentistry use across 5 teledentistry modalities (email, telephone, text, video conferencing, and mobile application).
Results:
Overall, 29% of respondents used teledentistry, and 68% of teledentistry users reported doing so for the first time because of the COVID-19 pandemic. First-time teledentistry use was positively associated with a high level of pandemic concerns (relative risk [RR] = 5.02; 95% CI, 3.49-7.20), age 35-44 years (RR = 4.22; 95% CI, 2.89-6.17), and annual household income $100 000-$124 999 (RR = 2.10; 95% CI, 1.55-2.84) and negatively associated with rural residence (RR = 0.68; 95% CI, 0.50-0.94). Having a high level of pandemic concerns (RR = 3.42; 95% CI, 2.30-5.08), young age (age 25-34 years: RR = 5.05; 95% CI, 3.23-7.90), and higher level of education (some college: RR = 1.59; 95% CI, 1.22-2.07) were strongly associated with teledentistry use for all “other” users (ie, existing or first-time use because of reasons unrelated to the pandemic). Most first-time teledentistry users used email (74.2%) and mobile applications (73.9%), whereas “other” teledentistry users used telephone communication (41.3%).
Conclusions:
Teledentistry use during the pandemic was higher in the general population than among those for whom teledentistry programs were originally designed (eg, low-income, rural populations). Favorable regulatory changes to teledentistry should be expanded to meet patient needs beyond the pandemic.
Oral health plays a strong role in determining systemic health and overall well-being, making it an essential service along with medical health and mental and behavioral health. 1 However, both patient and organizational-level access barriers persist for many in need of oral health care. 2 In response, various service delivery models, including teledentistry, have been introduced to open new points of entry to the oral health care system. Teledentistry allows for the remote provision of dental consultation including screening and diagnosis, treatment planning, and pre- and postoperative care. As with other alternative modes of service delivery, such as mobile and portable dentistry, teledentistry focuses on rural and other populations for whom structural and financial barriers often preclude access to oral health services. 3 Pre-pandemic use of teledentistry often occurred in conjunction with mobile and portable dentistry, allowing the itinerant provider to initiate the teledentistry visit or consultation and offer any recommended services to the patient. 4
Throughout the COVID-19 pandemic, many people delayed, avoided, or were prevented from obtaining dental treatment. International, federal, and state regulatory agencies and national and state dental societies recommended closure of dentistry practices in most states beginning in March 2020, with resumption of various services beginning in May 2020; some restrictions persisted in the types of services or the methods of treatment for various dental conditions. 5 Although the number of dental visits in the United States increased in late spring and summer 2020 as closure mandates were lifted, use varied consistent with county-level COVID-19 incidence rates, 6 suggesting that fears related to high incidence rates affected patients’ willingness to seek care. Historically, dental services are more likely than other essential health care services to be affected by income and employment rates. 7 It has been shown that social determinants of health (SDOH) such as financial stability, education, and health literacy also have a major impact on people’s health and well-being, including access to oral health care. 8 Reduced availability of oral health care during the pandemic combined with the loss of employment and health insurance and growing fears about COVID-19 were therefore likely to exacerbate disparities based on SDOH.
The temporary closure of dental offices and consumers’ pandemic-related fears reduced the number of dental visits but also promoted a period of natural experimentation in using teledentistry to fill new and existing gaps in access to oral health care. For example, the initial closures of dental practices drastically reduced the supply of oral health services. Subsequent to dental office closures, support for the use of teledentistry expanded across states and at the federal level. In response to the pandemic, regulators broadened the scope of supported services, expanded the populations who could access services, loosened privacy regulations to allow for communication on readily available web platforms, and allowed for reimbursement for teledentistry. 9 The experiences of both new and existing users of teledentistry during the early months of the pandemic could, therefore, be instrumental in crafting an effective expansion of future teledentistry initiatives.
While demand and use of teledentistry because of COVID-19 have been explored in international studies,10,11 few researchers have addressed nationwide use relative to consumers’ fears about the pandemic in the United States. Moreover, because of the novel impact of the pandemic on consumers’ perceptions and the availability of oral health services, the emergence of COVID-19 during early 2020 was a singular period in which interventions, such as teledentistry, to address public health emergencies could be implemented. In addition, in the absence of available vaccines and effective treatments, oral health knowledge and concerns about the pandemic likely had a heightened effect on consumers’ engagement with oral health services during this time. This study investigated consumers’ use of teledentistry from June 2019 through June 2020 and evaluated the association of teledentistry use with respondents’ level of anxiety or concern about various aspects and impacts of the pandemic and with their demographic and socioeconomic characteristics and geography.
Methods
Sampling and Data Collection
The data were collected by the Association of American Medical Colleges (AAMC) as part of its biannual Consumer Survey of Health Care Access. This survey obtains information on access to care including health insurance coverage, modes of care, patient–provider relationships, and demographic characteristics. 12 Survey respondents were recruited from a representative online panel of approximately 1.5 million adults in the United States.
Data from the June 2020 wave of the survey included responses from 3500 adults who needed health care in the past year. We assessed teledentistry use during the 12 months preceding survey completion, the primary outcome variable, based on the use of at least 1 of 5 modalities (email, telephone, text, video conferencing, and mobile application) to enable communication with dental providers. When survey participants indicated any teledentistry use, we asked them to indicate whether it was “for the first time because of COVID-19 or social distancing concerns.”
Survey items asking about pandemic-related concerns were included for the first time in the June 2020 instrument. Eight items focused on participants’ anxieties about financial and material security, access to technology, childcare, education, and the ability to care for one’s physical and mental health. These items were scored on a 5-point Likert scale ranging from 1 = not at all concerned to 5 = very concerned. We developed a composite score for overall concern by creating summed totals with a minimum of 8 and a maximum of 40 points. On the basis of the tertile distribution of composite scores, we categorized pandemic concerns as low (score of 8-18), medium (score of 19-30), or high (score of 31-40).
We conducted the study according to a research protocol that was reviewed and approved by the New York State Department of Health Institutional Review Board (IRB #1689715-1).
Data Analysis
We calculated descriptive statistics for respondents’ characteristics, pandemic concerns, and use of telehealth modalities. We tested differences between groups using the Pearson χ2 test for categorical variables and t tests for continuous variables.
We tested multivariable associations using modified Poisson regression (relative risks [RRs] and 95% CIs) with robust error variance estimates (also known as sandwich estimation). 13 We analyzed teledentistry use in 2 separate regression models: (1) for first-time users of teledentistry because of the pandemic compared with nonusers and (2) for “other” teledentistry users (ie, existing or first-time use because of reasons unrelated to the pandemic) compared with nonusers. Our primary predictor of interest was concerns related to the pandemic. Other predictors included respondents’ age, sex, race and ethnicity, education, annual household income, health insurance, self-reported area of residence, and geographic region.
The data were weighted by demographic, socioeconomic, and geographic characteristics to represent the US adult population. We used SPSS version 27.0 (IBM Corp) and R version 4.0.2 (R Foundation for Statistical Computing) for analyses. We considered P = .05 to be significant for all analyses.
Results
Analyses of both teledentistry users (n = 1021, 28.8%) and nonusers (n = 2526, 71.2%) yielded a total weighted sample of 3547 respondents (Table 1). Most respondents were aged ≥45 years (52.1%), male (53.6%), non-Hispanic White (63.3%), and married or living together (60.6%); had a college or postgraduate degree (43.1%), an annual household income ≥$100 000 (38.2%), and private health insurance (43.1%); lived in urban (42.5%) or suburban (41.9%) areas; and resided in the South (37.5%). Compared with nonusers, teledentistry users (first-time and “others”) were significantly more likely to be younger (18-44 years; 76.9% vs 36.2%), male (74.2% vs 45.2%), and married or living together (74.3% vs 55.1%); have a postgraduate degree (37.0% vs 12.5%), annual household income ≥$125 000 (44.5% vs 22.0%), and private health insurance (51.7% vs 39.6%); live in an urban area (65.8% vs 33.1%); and reside in the Northeast (22.1 vs 17.5) or West (28.3% vs 21.9%). We found no significant differences in teledentistry use by race and ethnicity.
Characteristics of respondents to the Consumer Survey of Health Care Access, by teledentistry use, United States, June 2019–June 2020 a
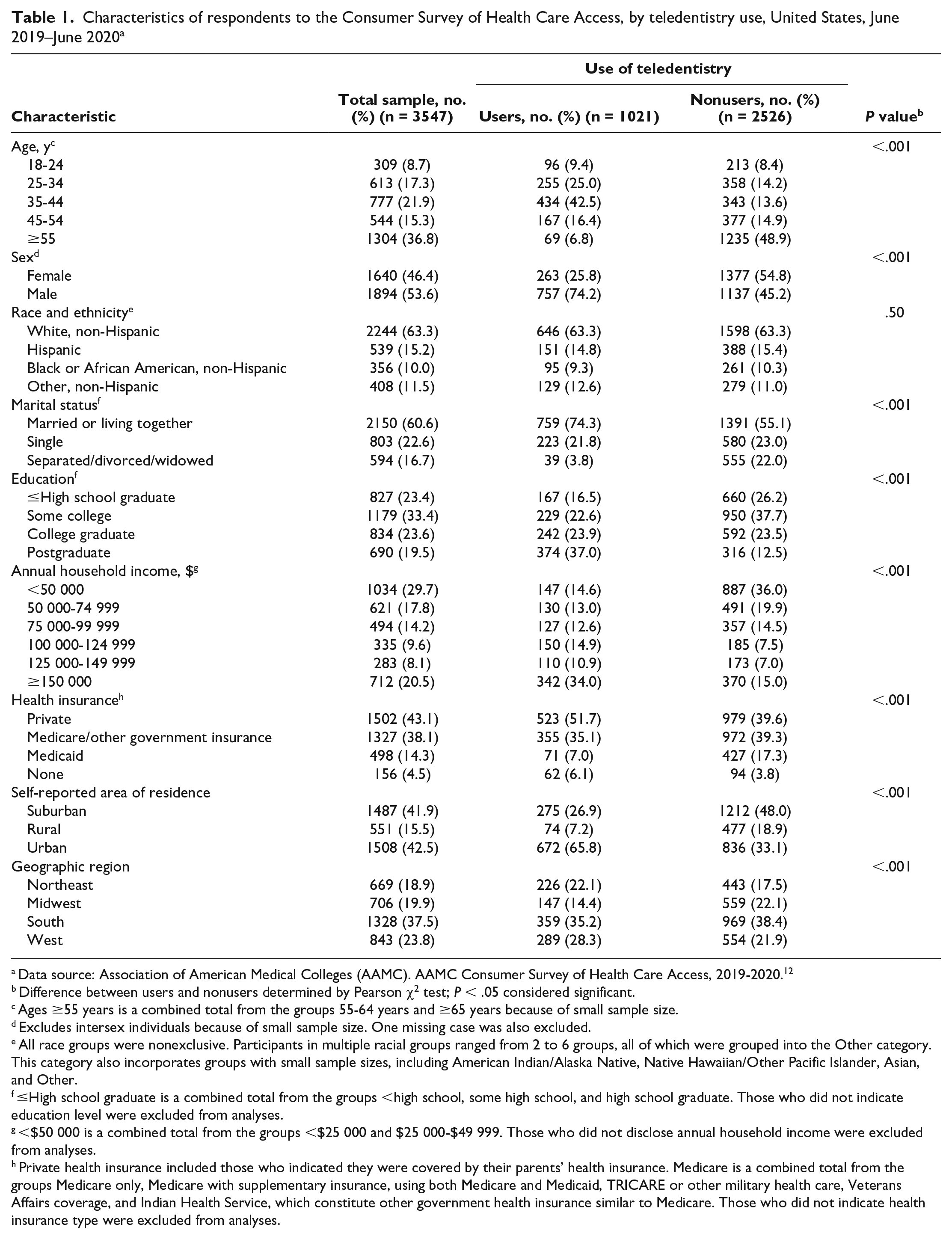
Data source: Association of American Medical Colleges (AAMC). AAMC Consumer Survey of Health Care Access, 2019-2020. 12
Difference between users and nonusers determined by Pearson χ2 test; P < .05 considered significant.
Ages ≥55 years is a combined total from the groups 55-64 years and ≥65 years because of small sample size.
Excludes intersex individuals because of small sample size. One missing case was also excluded.
All race groups were nonexclusive. Participants in multiple racial groups ranged from 2 to 6 groups, all of which were grouped into the Other category. This category also incorporates groups with small sample sizes, including American Indian/Alaska Native, Native Hawaiian/Other Pacific Islander, Asian, and Other.
≤High school graduate is a combined total from the groups <high school, some high school, and high school graduate. Those who did not indicate education level were excluded from analyses.
<$50 000 is a combined total from the groups <$25 000 and $25 000-$49 999. Those who did not disclose annual household income were excluded from analyses.
Private health insurance included those who indicated they were covered by their parents’ health insurance. Medicare is a combined total from the groups Medicare only, Medicare with supplementary insurance, using both Medicare and Medicaid, TRICARE or other military health care, Veterans Affairs coverage, and Indian Health Service, which constitute other government health insurance similar to Medicare. Those who did not indicate health insurance type were excluded from analyses.
Pandemic Concerns
Using a 5-point Likert scale, survey participants indicated being most concerned about the financial impact of the pandemic (mean = 3.6), being able to take care of their physical health (mean = 3.3), and having access to resources such as food (mean = 3.3) or other items expected to be in scarce supply (ie, toiletries) (mean = 3.4) (Table 2). Levels of concern about the pandemic were significantly higher among teledentistry users than among nonusers for all 8 items and for the categorical variable.
Concerns about impact of the COVID-19 pandemic among users and nonusers of teledentistry, Consumer Survey of Health Care Access, June 2019–June 2020 a
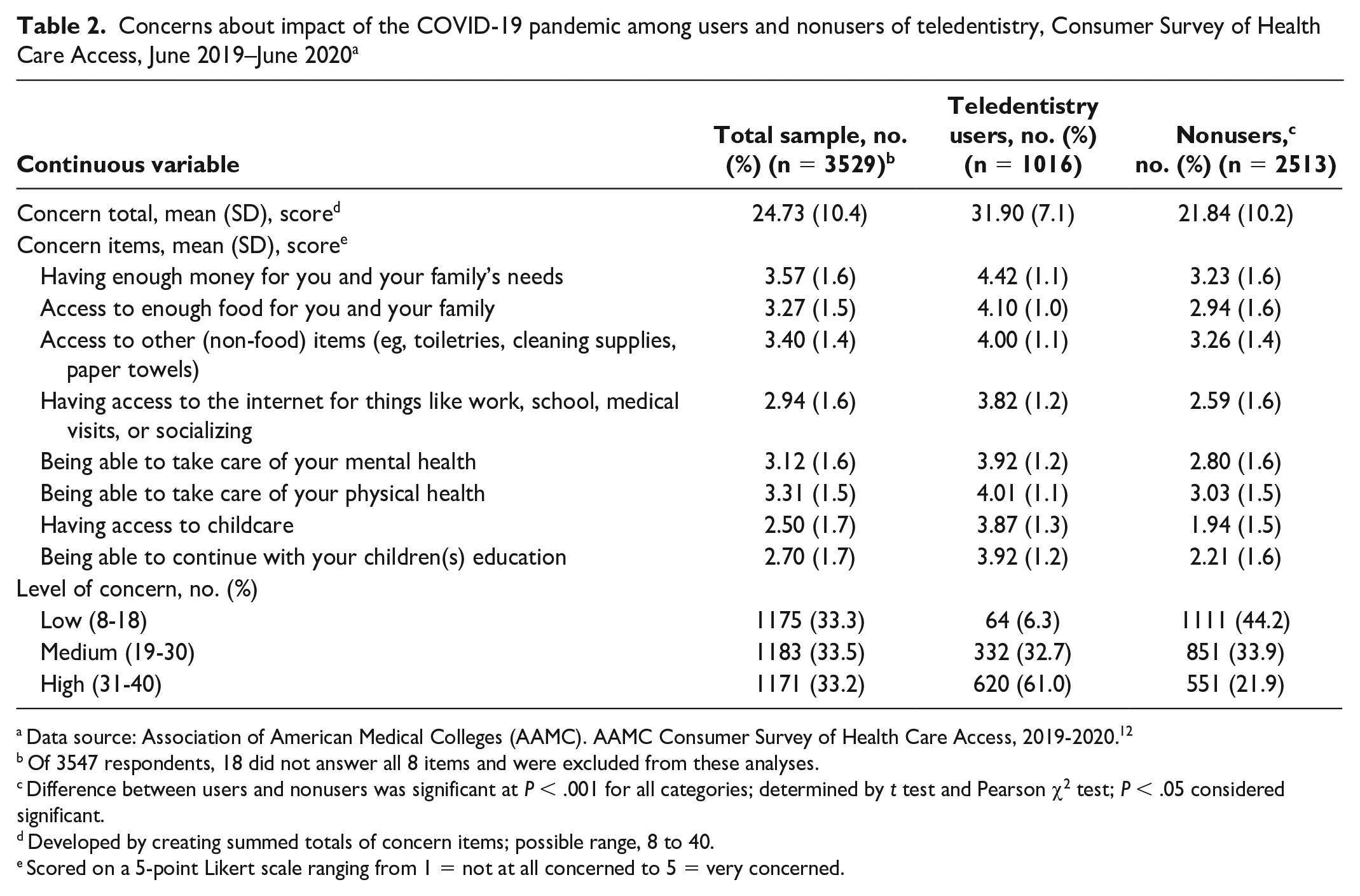
Data source: Association of American Medical Colleges (AAMC). AAMC Consumer Survey of Health Care Access, 2019-2020. 12
Of 3547 respondents, 18 did not answer all 8 items and were excluded from these analyses.
Difference between users and nonusers was significant at P < .001 for all categories; determined by t test and Pearson χ2 test; P < .05 considered significant.
Developed by creating summed totals of concern items; possible range, 8 to 40.
Scored on a 5-point Likert scale ranging from 1 = not at all concerned to 5 = very concerned.
On average, 68.4% of teledentistry use was for the first time because of the pandemic. All modalities were being used by most respondents for the first time because of the pandemic (Figure 1). Telephone use had the fewest first-time users (58.7%), whereas email (74.2%) and mobile applications (apps) (73.9%) had the most first-time users because of the pandemic. “Other” teledentistry users preferred telephone (41.3%) and text communication (33.5%) over email (25.8%) and mobile apps (26.1%).
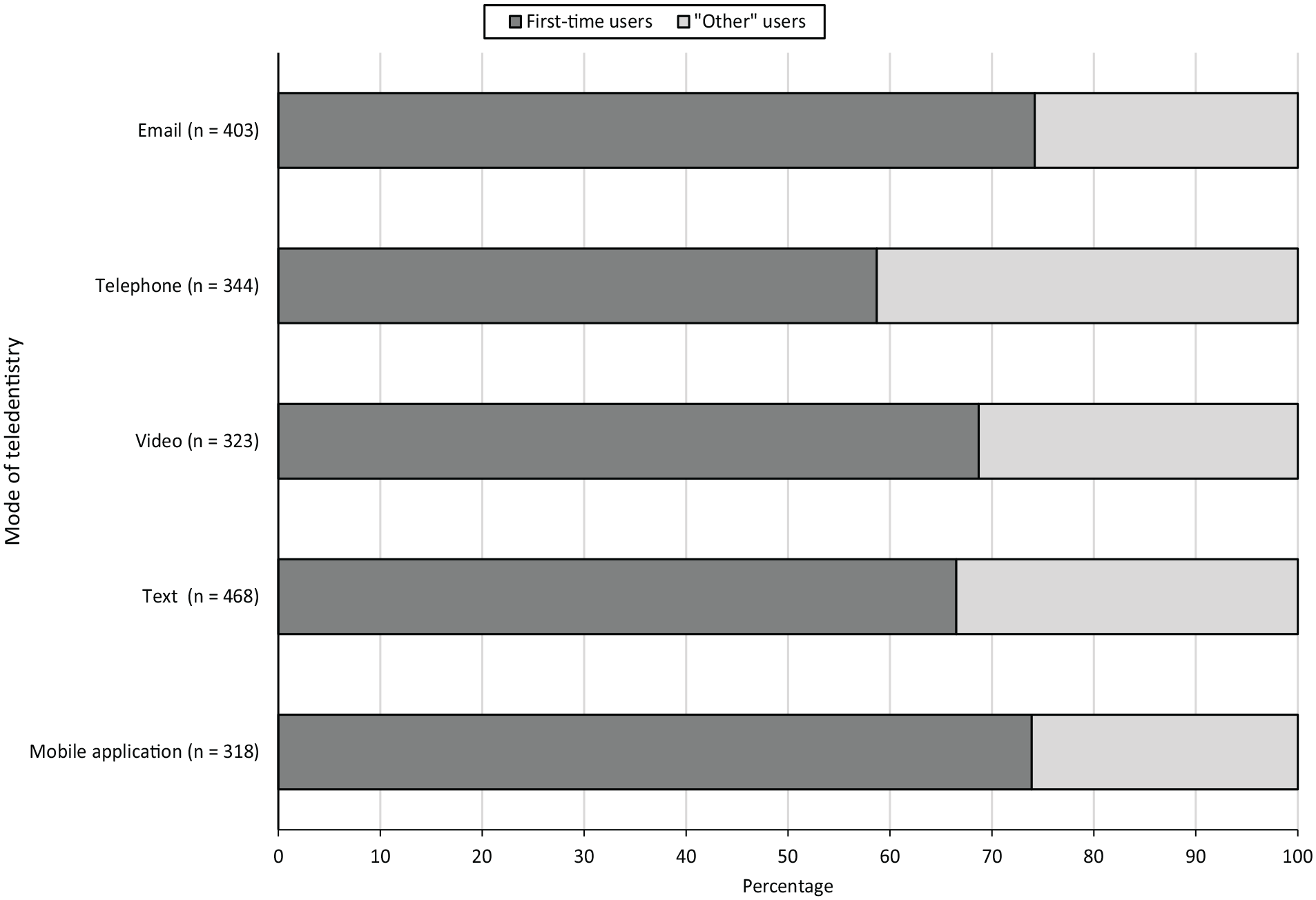
Percentage of teledentistry encounters across modalities by first-time users because of the COVID-19 pandemic and “other” users, June 2019–June 2020. “Other” users were defined as those who did not use teledentistry for the first time because of COVID-19. Teledentistry use consists of 5 modalities: emailing providers with questions, meeting with providers via telephone, meeting with providers via video conferencing (eg, Skype), using text communication or text-based chat functions with providers, and communicating with providers via mobile applications. Each teledentistry category was measured by a single item except for text communication, which consisted of 2 items asking about live text “chat” activity via a website and texting with a provider on a mobile phone.
Associations With Teledentistry Use
Respondents who used teledentistry for the first time because of the pandemic were significantly more likely than nonusers to have higher levels of pandemic concerns (medium concern: RR = 2.69; 95% CI, 1.87-3.87; high concern: RR = 5.02; 95% CI, 3.49-7.20) (Table 3). Concerns about the pandemic were also predictive of teledentistry use for “other” users (medium concern: RR = 3.30; 95% CI, 2.26-4.82; high concern: RR = 3.42; 95% CI, 2.30-5.08).
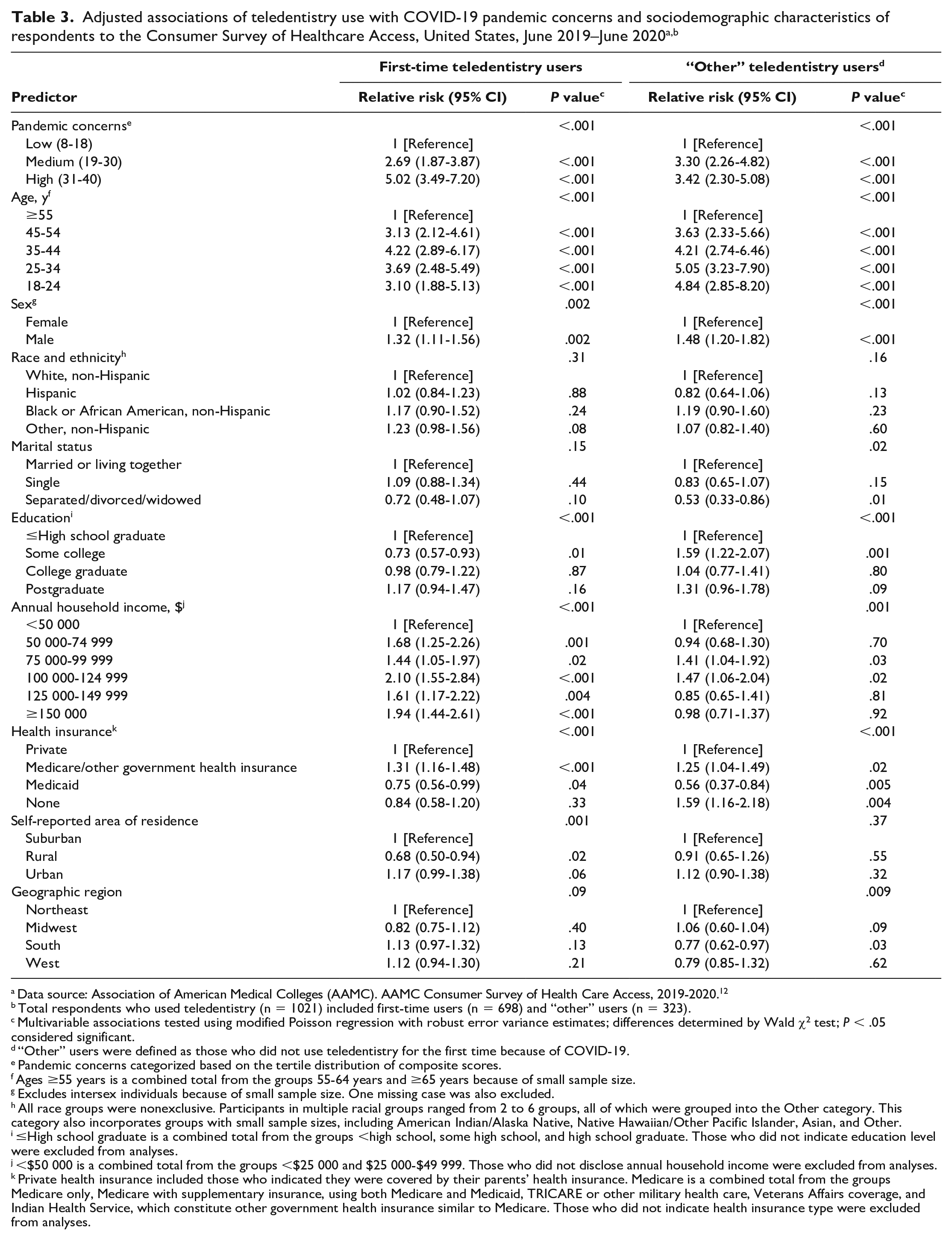
Data source: Association of American Medical Colleges (AAMC). AAMC Consumer Survey of Health Care Access, 2019-2020. 12
Total respondents who used teledentistry (n = 1021) included first-time users (n = 698) and “other” users (n = 323).
Multivariable associations tested using modified Poisson regression with robust error variance estimates; differences determined by Wald χ2 test; P < .05 considered significant.
“Other” users were defined as those who did not use teledentistry for the first time because of COVID-19.
Pandemic concerns categorized based on the tertile distribution of composite scores.
Ages ≥55 years is a combined total from the groups 55-64 years and ≥65 years because of small sample size.
Excludes intersex individuals because of small sample size. One missing case was also excluded.
All race groups were nonexclusive. Participants in multiple racial groups ranged from 2 to 6 groups, all of which were grouped into the Other category. This category also incorporates groups with small sample sizes, including American Indian/Alaska Native, Native Hawaiian/Other Pacific Islander, Asian, and Other.
≤High school graduate is a combined total from the groups <high school, some high school, and high school graduate. Those who did not indicate education level were excluded from analyses.
<$50 000 is a combined total from the groups <$25 000 and $25 000-$49 999. Those who did not disclose annual household income were excluded from analyses.
Private health insurance included those who indicated they were covered by their parents’ health insurance. Medicare is a combined total from the groups Medicare only, Medicare with supplementary insurance, using both Medicare and Medicaid, TRICARE or other military health care, Veterans Affairs coverage, and Indian Health Service, which constitute other government health insurance similar to Medicare. Those who did not indicate health insurance type were excluded from analyses.
Significant predictors were similar for first-time users and “other” teledentistry users; generally, differences across variable levels were stronger among “other” users than among first-time teledentistry users (Table 3). Younger respondents were 3 to 5 times more likely to use teledentistry than respondents aged ≥55 years, with stronger effects seen for “other” users (aged 25-34 years: RR = 5.05; 95% CI, 3.23-7.90). A consistent effect was also seen for both user groups, in which males were nearly 1.5 times more likely than females to use teledentistry. Race and ethnicity were not associated with teledentistry use. Respondents who were separated, divorced, or widowed were less likely than respondents who were married or living together to use teledentistry for reasons unrelated to the pandemic. Education also predicted teledentistry use. Compared with respondents with <high school education, respondents with some college were less likely to use teledentistry for the first time because of the pandemic but were 1.6 times more likely to use teledentistry for reasons unrelated to the pandemic (RR = 1.59; 95% CI, 1.22-2.07).
Respondents with higher annual household incomes were more likely to use teledentistry than respondents with lower annual household incomes (Table 3). We observed the largest effects among respondents with an annual household income ≥$100 000, who were about 2 times more likely to use teledentistry for the first time because of the pandemic (income $100 000-$124 999: RR = 2.10; 95% CI, 1.55-2.84) than respondents with annual household income <$50 000. Compared with respondents with private health insurance, respondents covered by Medicare or other government health insurance were about 1.3 times more likely to use teledentistry (ie, first-time users, “other users”) and Medicaid beneficiaries were less likely to use teledentistry. Rural respondents were less likely than suburban respondents to be first-time users of teledentistry (RR = 0.68; 95% CI, 0.50-0.94). We observed the effect of geographic region across “other” teledentistry users; respondents from the South were less likely than respondents from the Northeast to be teledentistry users (RR = 0.77; 95% CI, 0.62-0.97).
Discussion
Long before the interruption of dental services occasioned by the COVID-19 pandemic, teledentistry was recognized as a “disruptive innovation” driven by the unaffordability of oral health care and persistent gaps in access.14,15 Although teledentistry had some success in mitigating access issues for rural and other dentally underserved groups prior to the pandemic, it remained relatively unembraced. 2 The combined influence of fears related to the pandemic and the temporary closure of many points of service further exacerbated existing access gaps, increasing the need for innovation in promoting patient–dentist interactions, especially for urgent or emergent oral health problems.
The lack of access to dental care engendered by the COVID-19 pandemic, while severe, was not altogether novel. Teledentistry was originally introduced to address the lack of access to oral health care for rural and dentally underserved populations; as such, it was likewise poised to adapt to general demand during the pandemic. 16 Accordingly, regulations were broadened during 2020 to enable teledentistry use for consultations, diagnoses, and treatment planning for more patients in the general population. 17 Similarly, restrictions related to geographic region, requirements for types of interfaces (eg, video vs telephone), and HIPAA (Health Insurance Portability and Accountability Act) regulations were also loosened to increase access. 18 The American Dental Association also released guidelines on the coding and billing of virtual visits and personal protective equipment.19,20
Our results indicate that such measures improved availability of dental services for participants seeking access as the pandemic began. In our study, about 3 in 10 respondents used some type of information technology to contact their dental provider, and more than half indicated doing so for the first time because of the pandemic. In a recent study evaluating patient utilization data from 26 000 dental providers, Choi et al 21 found that demand for teledentistry services was 60 times greater in April 2020, when the pandemic necessitated practice closures, than before the COVID-19 outbreak. The authors also noted that demand for teledentistry services remained at approximately 10 times that of prepandemic levels even after dental offices reopened, suggesting that uptake and use of the modality may persist at higher rates than in the past.
The level of concerns among survey respondents about the impact of the pandemic also appears to have increased the use of teledentistry, with stronger associative relationships of its use than any other variable considered in our analysis. Interestingly, the level of concerns about concrete factors such as the availability of finances, childcare, and other essential resources was stronger for teledentistry users than for nonusers. Most prepandemic literature discussing barriers to accessing oral health services cites these factors as impediments to seeking care.2,22 However, these fears seemed to prompt rather than discourage teledentistry use during the pandemic. One important mitigating factor during the pandemic may be that teledentistry services were provided directly to patients at home, whereas visits to remote sites where teledentistry services could be initiated (eg, schools, mobile programs) were more commonly required prior to the pandemic. 3
Our results also showed that the stronger the most commonly cited financial concerns, the more likely participants were to engage in teledentistry use. One possible explanation is that our measures did not assess experienced barriers per se but rather the anticipation of need across various domains. As a result, concerns about the pandemic’s impact could be considered a measure of participants’ motivation to seek needed resources during the pandemic, which would positively predict their engagement with oral health services. Furthermore, as a period in which health concerns were particularly salient, the pandemic may have served to highlight existing patient needs and the necessity of providing secure pathways to needed health services. Our results suggest that concerns about the impact of the pandemic on various needs contributed uniquely to teledentistry use regardless of the occasion for its use. Increased patient motivation, awareness, and more accessible pathways to oral health services thus appear to have had a combined effect on teledentistry use during the pandemic.
One of the most compelling findings about the overall use of teledentistry, however, was the predominant use by majority population groups, especially in light of its original design objective to reach dentally underserved groups in rural areas. This study suggests that there may be enduring structural barriers to greater uptake of teledentistry across geographic areas, such as access to broadband networks, a necessary component for delivery of telehealth services. Similarly, low-income patients may have had variable access to broadband technologies required by prepandemic regulations to access teledentistry. Such results suggest that SDOH related to income, geography, or digital literacy may have hindered access to teledentistry.
While cell phone use is virtually ubiquitous across income levels, the use of email, mobile apps, and video technologies to reach dentists, which increased with pandemic-related use, may not have been as accessible in some households as in others. In the Federal Communications Commission’s 2020 report 23 describing the cellular and broadband marketplaces, 478 million connected mobile devices (cellular technology) were reported in the United States, a number greater than the population. In addition, in some states, a substantial portion of the population did not have access to a residential broadband connection. 23 Our study showed significantly lower use of teledentistry for reasons unrelated to the pandemic in the South. Deficits in required hardware technology, internet quality, and digital self-efficacy have also challenged remote learning efforts during COVID-19 in similar ways. 24
In addition, telephone consultations only became reimbursable after the regulatory changes affecting teledentistry were implemented during lockdown. 25 A survey in Nova Scotia, Canada, found that among the 181 dentists who provided any care to patients during the week of April 19, 2020, 93.4% provided only audio or virtual consultations. 26 These dentists indicated that 95% of their patient encounters occurred by telephone; 29.8% of patient encounters also or separately involved an email component or a video conference (7.7%). Policy makers may want to consider extending telephonic permissions to encourage uptake among all patients and increase funding for broadband technology, especially in rural areas. Indeed, while SDOH such as income and access to technology appeared to divide access to oral health care before the pandemic began (ie, among “other” users), executive orders expanding the application of teledentistry likely aided first-time use during the pandemic by Medicaid and low-income recipients. As an increasingly accessible pathway to oral health services, teledentistry represents a strong means by which to enhance and increase the number of professionals providing quality care in rural and other dentally underserved areas with a high demand for oral health care.
While the procedure-oriented nature of dentistry may appear to limit the potential of teledentistry for remote care delivery, robust uptake during the pandemic demonstrates that its use for consultations, diagnosis, treatment planning, pre- and postoperative care, and education is safe, effective, and desirable to patients. In addition, initial survey responses to dental video consultations during COVID-19 have been positive, with equal numbers preferring remote consultations over in-person equivalents. 27 Studies also show that consultations conducted remotely resulted in nearly 100% compliance, reflecting the effectiveness of teledentistry for determining and following through with dental planning. 28 As an alternate form of oral health care delivery, teledentistry can safely and effectively increase capacity in the dental delivery system to meet patient needs well beyond the COVID-19 pandemic.
Limitations
The study had several limitations. First, oral health literacy, dental need, and other variables related to seeking oral health care could not be measured. User and nonuser populations may therefore differ based on oral health need or other barriers and facilitators of dental service use not available in our data. Second, small sample sizes limited the analysis of groups that could not be merged with others (eg, people without health insurance). Lastly, self-reported data may be subject to recall bias. Given the short recall period of this study, however, this bias likely did not affect results.
Conclusion
The combined effect of increased patient need and concerns about the pandemic, more supportive regulatory restrictions, and dental providers’ participation in remote dental services all contributed to greater patient use of teledentistry. In addition, the populations using teledentistry during the pandemic were much broader than those for whom such programs were originally designed. The effects of COVID-19 will likely continue to have an impact on consumers’ perceptions and behaviors. The current study illustrates that the convergence of circumstances during the most uncertain months of the pandemic provided unique opportunities for teledentistry use to grow. Such outcomes are the result of a natural experiment brought on by the COVID-19 pandemic that demonstrates the utility of alternative forms of care delivery. The current findings thus reflect a precedent for using teledentistry to expand oral health workforce capacity and respond to future public health emergencies.
Footnotes
Acknowledgements
The authors acknowledge the contributions of the Association of American Medical Colleges (AAMC) and its staff, especially Michael Dill, MPA, director of workforce studies, and Natalie Felida, MPH, senior research analyst, for their input on survey design and conduct. Their expertise is greatly appreciated. This material is based upon data provided by AAMC. The views expressed herein are those of the authors and do not necessarily reflect positions or policies of AAMC.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Oral Health Workforce Research Center is supported by the Health Resources & Services Administration (HRSA) of the US Department of Health and Human Services (HHS) as part of an award totaling $449 915. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement by, HRSA, HHS, or the US government.