
Abstract
Objectives:
In times of heightened population health needs, the health workforce must respond quickly and efficiently, especially at the state level. We examined state governors’ executive orders related to 2 key health workforce flexibility issues, scope of practice (SOP) and licensing, in response to the COVID-19 pandemic.
Methods:
We conducted an in-depth document review of state governors’ executive orders introduced in 2020 in all 50 states and the District of Columbia. We conducted a thematic content analysis of the executive order language using an inductive process and then categorized executive orders by profession (advanced practice registered nurses, physician assistants, and pharmacists) and degree of flexibility granted; for licensing, we indicated yes or no for easing or waiving cross-state regulatory barriers.
Results:
We identified executive orders in 36 states containing explicit directives addressing SOP or out-of-state licensing, with those in 20 states easing regulatory barriers pertaining to both workforce issues. Seventeen states issued executive orders expanding SOP for advanced practice nurses and physician assistants, most commonly by completely waiving physician practice agreements, while those in 9 states expanded pharmacist SOP. Executive orders in 31 states and the District of Columbia eased or waived out-of-state licensing regulatory barriers, usually for all health care professionals.
Conclusion:
Governor directives issued through executive orders played an important role in expanding health workforce flexibility in the first year of the pandemic, especially in states with restrictive practice regulations prior to COVID-19. Future research should examine what effects these temporary flexibilities may have had on patient and practice outcomes or on permanent efforts to relax practice restrictions for health care professionals.
In times of heightened population health needs, the health workforce must respond quickly and efficiently, and the onset of the COVID-19 pandemic was no different. The surge in patients brought with it shortages of medical staff, supplies, and space, leaving states to respond quickly.
Scope of practice (SOP) laws may reduce health care professionals’ ability to practice at the top of their education and license, and licensure requirements for out-of-state health care professionals can be administratively and financially burdensome. Because policies governing these issues are created at the state level, they vary across the country, even among neighboring states, and this patchwork system can hamper the health workforce’s response to emergencies. Among the groups most constrained by SOP laws are advanced practice registered nurses (APRNs) (nurse practitioners, certified nurse midwives, nurse anesthetists, and clinical nurse specialists) and physician assistants (PAs). Collectively referred to as advanced practice clinicians, APRNs and PAs perform as well as physicians do on health outcomes, are in some cases better at patient communication and chronic disease management, and meet the nation’s primary care needs by practicing in medically underserved and rural communities.1 -4
Yet, SOP restrictions—particularly collaborative practice and delegation agreements that require advanced practice clinicians to have a formal relationship with a supervisory physician to perform ≥1 component of clinical care—limit these clinicians’ autonomy and potential to expand the provision of health care services.5 -7 SOP restrictions can impede care by limiting advanced practice clinicians’ authority to prescribe medications, diagnose patients, and perform certain procedures and by constraining their potential to provide vital services in areas such as behavioral and women’s health that faced health workforce shortages prior to the pandemic.5 -7 Claims that SOP restrictions improve patient safety and quality of care are not supported by the evidence. 8
Pharmacists are also subject to SOP restrictions. 9 Pharmacists’ roles can be optimized when they are fully integrated into patient health care teams and can provide expanded services, including medication adjustment, disease management, patient education, and health promotion.9,10 Although there is a growing trend of allowing pharmacists to provide services beyond dispensing and advising on prescriptions, state-specific SOP barriers often stand in the way of allowing pharmacists to perform the full spectrum of services that they are educated and trained to offer, the settings in which services may be provided, or the populations for which they can provide care. 9 Given the accessibility of community pharmacists to the patients whom they serve, especially in otherwise medically underserved areas, they have the potential to serve as vital health care extenders during public health emergencies such as COVID-19, if given the regulatory authority to do so. 11
States regulate the education, training, and examinations that all health care professionals must complete before working in a particular state. This regulation presents barriers to interstate mobility for health care professionals, which in turn constrains health systems’ ability to increase health workforce capacity during a health emergency. 12 Existing occupational licensure compacts, which enable professional licensure reciprocity among states, allow for some flexibility in movement across state lines for health care professionals, but they vary in the ease of reciprocity, the professions to which they apply, and the number of participating states. 13
The COVID-19 pandemic exposed health care systems’ needs for greater flexibility in SOP and interstate mobility areas of health workforce regulation. The lack of a coordinated national response and minimal coordination between federal and state policies early in the pandemic left the onus on states—particularly on state governors—to determine how to deploy their health workforce to combat COVID-19. Organizations such as the National Governors Association provided guidance to governors suggesting that some of the most effective strategies that they could use were expanding clinicians’ SOP and easing licensing barriers for out-of-state practitioners. 14 Both strategies serve to expand the pool of health workers available to provide clinical care at a time of surging demand. The former strategy provides the flexibility needed for the health workforce to task shift when health care facilities are overwhelmed or understaffed, and it increases the pool of health care providers able to offer full-spectrum health care services. Additionally, when SOP restrictions are relaxed to allow advanced practice clinicians more autonomy, supervisory tasks are also reduced or eliminated for physicians, thus allowing them to shift their focus to providing specialized care to address the complex needs of patients with and without COVID-19. 14 Easing regulations to allow out-of-state practitioners to provide services has long been a strategy used by states to boost health workforce capacity in times of public health emergencies and may be particularly important in states already facing health professional shortages. 15
One policy lever available to governors is issuing executive orders, which allow them to circumvent the legislative process by creating laws that fall under a state’s purview of gubernatorial authority. 16 Governors have used executive orders to address a range of public health issues, but they are particularly critical policy tools in times of emergency.16 -19 When a state declares an emergency, as all states did in response to COVID-19, it triggers emergency powers that the governor may use to mitigate the threat, which may include the temporary removal of laws or regulations that present barriers to an effective state response. 20 The main advantage to expanding the governor’s executive power in emergencies is the speed with which executive orders take effect; traditional legislative methods are not suited to immediately address urgent matters.
An emergency declaration can change the legal and operational landscape in which governments, private organizations, and the public operate during an emergency. If they occur at multiple levels (federal, state, local), emergency declarations can spur a cascade of activities and guidance that may be confusing for organizations and individuals. Therefore, clear directives from governors are especially important in times of emergency. This study examined governor-issued executive orders containing explicit directives that (1) expanded SOP for APRNs, PAs, or pharmacists or (2) permitted health care professionals with out-of-state licenses to provide care during the COVID-19 pandemic. Previous research has examined many aspects of the COVID-19 pandemic, but to our knowledge, no studies to date have reviewed the content of governors’ executive orders across the United States as they relate to these 2 key health workforce issues. We examined state governors’ actions related to 2 key health workforce issues, SOP and licensing, in response to the COVID-19 pandemic.
Methods
We conducted an in-depth document review of the text of state governors’ executive orders related to SOP and licensing in all 50 states and the District of Columbia that were introduced in 2020. Document review is well established as a qualitative research method that can elicit meaning and gain in-depth understanding of a particular topic. 21 We used state governments’ webpages containing the executive orders themselves as our primary data source, as well as secondary sources that referenced primary source material.22 -24
We included executive orders containing explicit authorizations from the governor easing out-of-state licensing or SOP regulations for APRNs, PAs, or pharmacists. We excluded executive orders that delegated authority to state agencies, such as departments of health, for health workforce regulatory oversight or that cross-referenced preexisting legislation without including explicit directives from the governor to ease health workforce restrictions. We also excluded executive orders related to reentry of retired professionals or early entry of students as well as policies not directly issued by the governor (eg, administrative policies promulgated by state agencies). We determined that these actions were beyond the scope of this project.
Once we gathered the policy data (ie, text of executive orders), we followed a 3-step process commonly used in document review: skimming, reading, and interpretation. 21 For the interpretation step, 3 authors (M.Z., J.S., M.K.) and a research assistant conducted a thematic content analysis of the policy language using an inductive process. We did not identify themes a priori and instead developed a set of key themes that we refined throughout the analytic process through group discussion and consensus. For all states that issued executive orders, we categorized them within 4 types: SOP for APRNs, SOP for PAs, SOP for pharmacists, and licensing for all professions. Within each category, we created and refined a set of themes that described how a governor’s executive order addressed workforce flexibility. Another author (P.P.) reviewed and refined the themes; we then reviewed these themes with content experts from professional associations representing APRNs, PAs, and pharmacists and refined them again according to their input. We next created a ranked category for each profession’s SOP, with a score of 1 indicating the maximized flexibility and a score of 2 indicating increased but less-than-maximum flexibility; if a state fell into both categories (eg, because of content related to multiple professions), we categorized them according to the highest degree of flexibility allowed in the executive order.
Lastly, we indicated the change from pre–COVID-19 policy based on these categories. To determine pre–COVID-19 policy, we relied on existing categorization by professional societies. The American Association of Nurse Practitioners categorizes states in 1 of 3 ways for nurse practitioners: full SOP, reduced SOP, or restricted SOP. Full SOP states for nurse practitioners do not require a collaborative practice agreement (CPA). 25 The primary mechanism for physician supervision of PAs is a supervision or delegation agreement, and PAs are subject to additional restrictions or allowances in their SOP, as outlined in the “6 Key Elements of a Modern PA Practice Act” by the American Academy of Physician Associates (previously the American Academy of Physician Assistants). 26 For pharmacists, we used the National Conference of State Legislatures’ determination on pharmacists’ prescription adaptation. 27 Using these 3 sources, we determined that before March 2020, 23 states were full SOP for nurse practitioners, 24 states had at least 5 of the 6 key elements for PAs, and 3 states allowed prescription adaptation for pharmacists. For licensing, we considered whether states were party to the Nurse Licensure Compact (NLC), the occupational interstate licensure compact for the nursing workforce, at the beginning of the pandemic in the United States. We used NLC participation as an indicator of states’ pre–COVID-19 openness to licensure flexibility across health professions, with nonparticipating states designated as being more restrictive than participating states. Thirty-two states were determined to be party to the NLC as of March 2020. 28 We followed the guidelines of the George Washington University Human Subjects Research Determination and concluded that this study did not require institutional review board review per federal regulations under 45 CFR 46. 29
Results
National Landscape
We identified executive orders in 35 states and the District of Columbia that contained explicit directives addressing SOP and/or out-of-state licensing, with executive orders in 20 states easing regulatory barriers pertaining to both areas of workforce policy (Table 1). Of those that addressed only 1 of these areas, the District of Columbia and 11 states (Alaska, California, Colorado, Florida, Hawaii, Massachusetts, Minnesota, New Hampshire, New Mexico, North Carolina, and Wyoming) issued executive orders explicitly granting licensing flexibilities to out-of-state health care professionals but did not issue executive orders pertaining to SOP. Four states (Arizona, Kentucky, New Jersey, and Washington) issued executive orders pertaining to SOP but not licensing.
Governor-issued executive orders containing explicit directives expanding the scope of practice or easing regulatory barriers for out-of-state health care professionals during the COVID-19 pandemic, United States, 2020
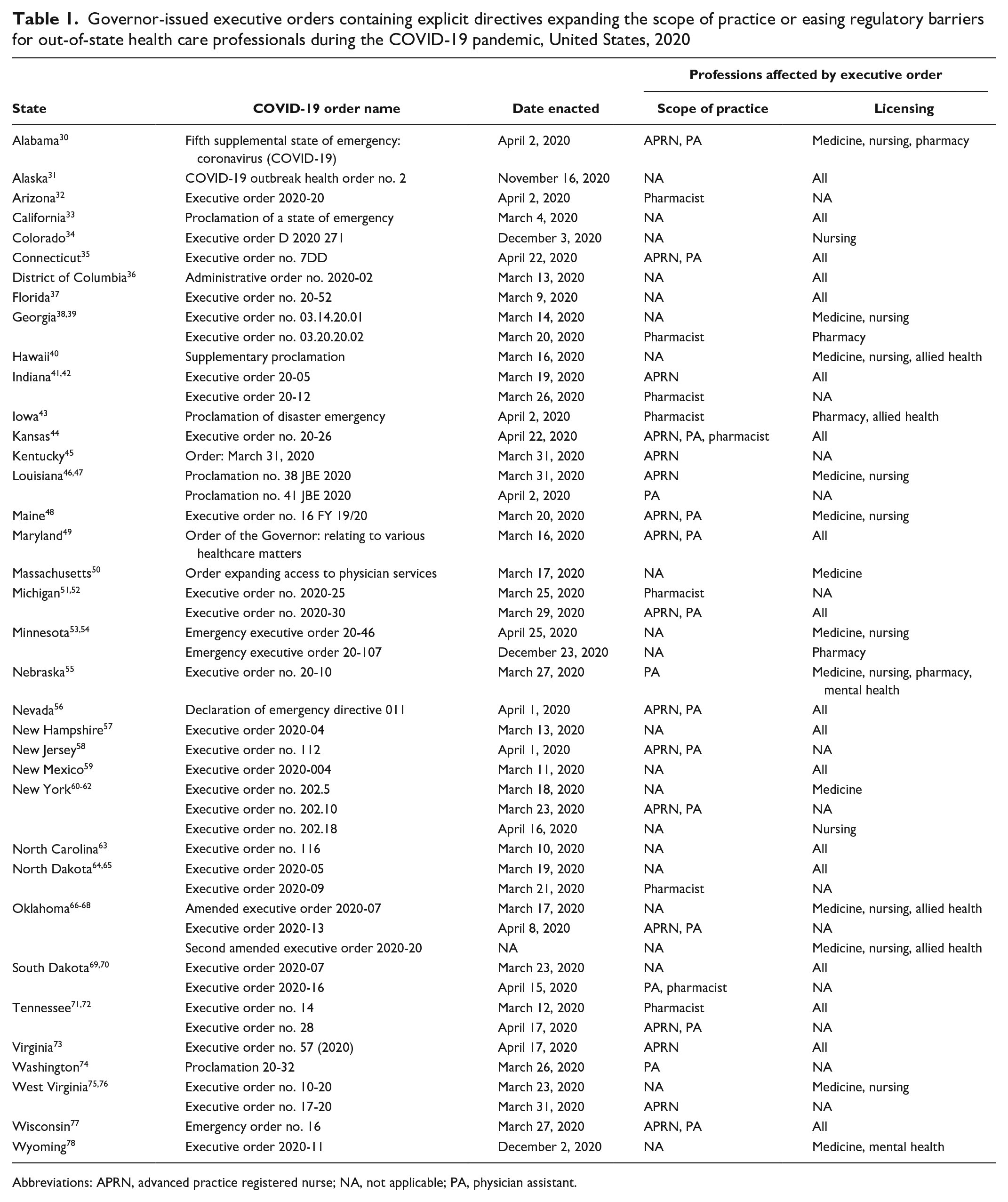
Abbreviations: APRN, advanced practice registered nurse; NA, not applicable; PA, physician assistant.
Scope of Practice: APRNs
We identified executive orders in 17 states that included explicit directives from the governor that reduced regulatory barriers related to SOP for APRNs and categorized them by thematic content for the extent of workforce flexibility that they authorized.
We defined the category 1 executive orders as those that maximized APRN workforce flexibility by either completely waiving CPAs between APRNs and a supervising physician or broadly removing limits on the services that could be provided under an APRN’s SOP (Table 2). Executive orders waived CPAs in 9 states (Kansas, Louisiana, Maine, Michigan, New Jersey, New York, Tennessee, Virginia, and Wisconsin), 3 of which had restricted practice environments prior to COVID-19 (Michigan, Tennessee, and Virginia) and only 1 of which (Maine) was already a full practice authority state, although just for APRNs with 2 years of practice. Executive orders in 2 states (Maryland and Nevada), while not specific to APRNs, authorized health care professionals to engage in services outside the scope of their specialization or license. In total, 11 states were in category 1.
Governor-issued directives in executive orders expanding the scope of practice (SOP) for APRNs during the COVID-19 pandemic, United States, 2020
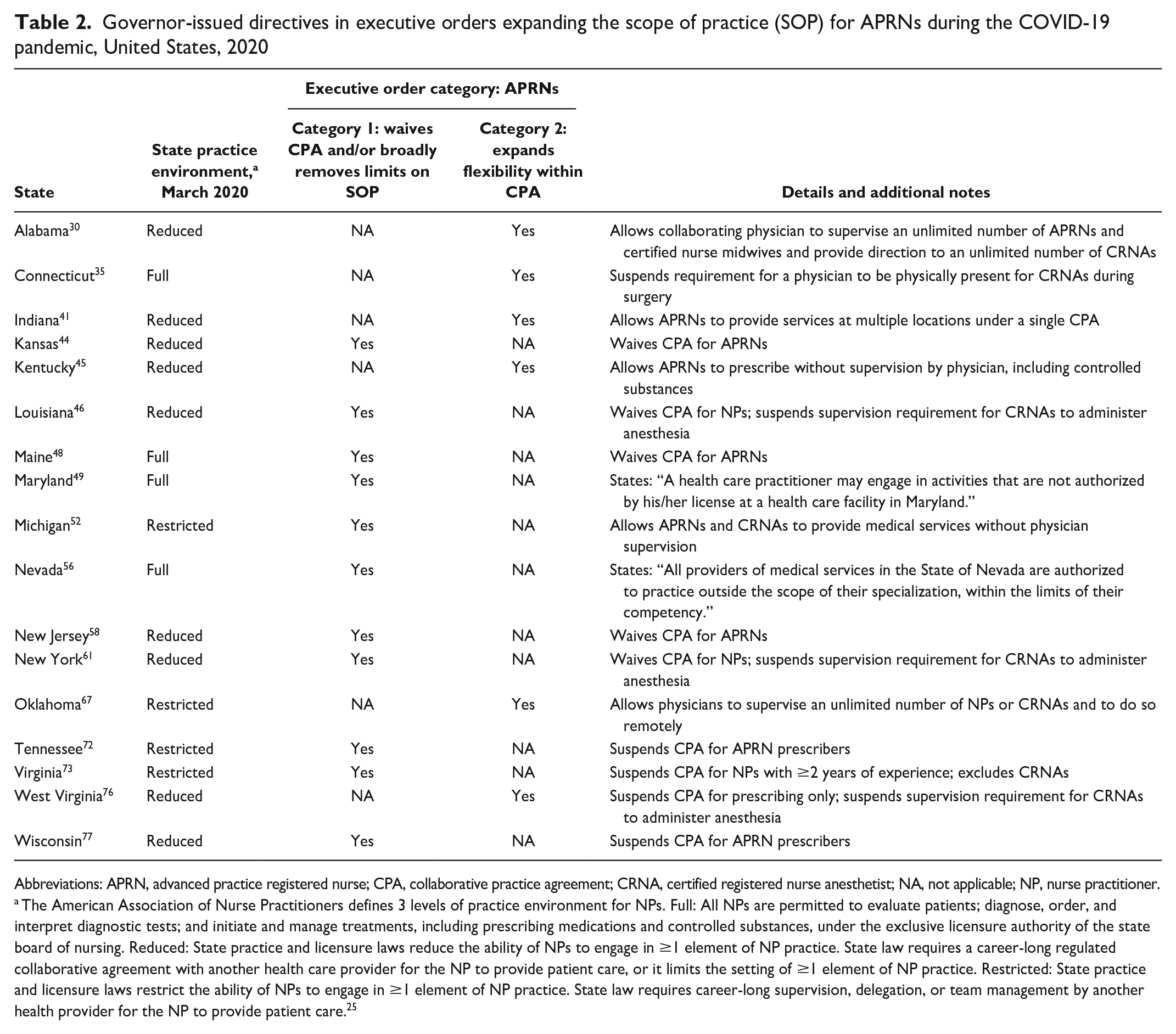
Abbreviations: APRN, advanced practice registered nurse; CPA, collaborative practice agreement; CRNA, certified registered nurse anesthetist; NA, not applicable; NP, nurse practitioner.
The American Association of Nurse Practitioners defines 3 levels of practice environment for NPs. Full: All NPs are permitted to evaluate patients; diagnose, order, and interpret diagnostic tests; and initiate and manage treatments, including prescribing medications and controlled substances, under the exclusive licensure authority of the state board of nursing. Reduced: State practice and licensure laws reduce the ability of NPs to engage in ≥1 element of NP practice. State law requires a career-long regulated collaborative agreement with another health care provider for the NP to provide patient care, or it limits the setting of ≥1 element of NP practice. Restricted: State practice and licensure laws restrict the ability of NPs to engage in ≥1 element of NP practice. State law requires career-long supervision, delegation, or team management by another health provider for the NP to provide patient care. 25
Category 2 of executive order directives comprised those that expanded practice flexibilities by easing supervisory restrictions or administrative burdens but stopped short of waiving CPAs. For example, executive orders issued in Connecticut and West Virginia authorized certified registered nurse anesthetists to administer anesthesia or other medications without physician supervision, while executive orders in Alabama and Oklahoma authorized physician supervision of an unlimited number of APRNs (Table 2). We identified 6 states (Alabama, Connecticut, Indiana, Kentucky, Oklahoma, and West Virginia) that issued executive orders in category 2 SOP policy provisions.
Scope of Practice: PAs
We identified executive orders in 17 states that included explicit directives from the governor reducing regulatory barriers related to SOP for PAs (Table 3).
Governor-issued directives in executive orders expanding scope of practice (SOP) for PAs, United States, 2020
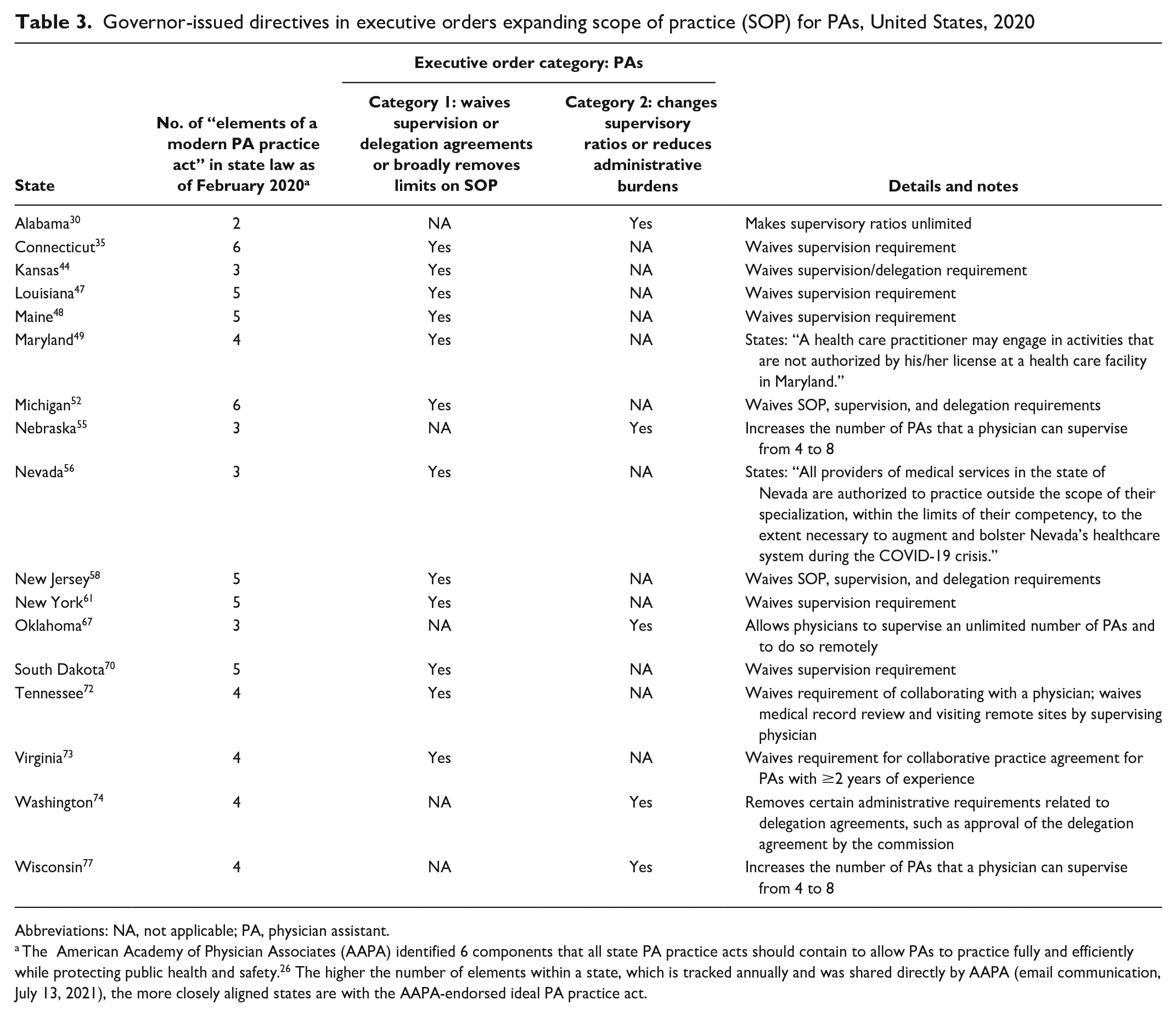
Abbreviations: NA, not applicable; PA, physician assistant.
The American Academy of Physician Associates (AAPA) identified 6 components that all state PA practice acts should contain to allow PAs to practice fully and efficiently while protecting public health and safety. 26 The higher the number of elements within a state, which is tracked annually and was shared directly by AAPA (email communication, July 13, 2021), the more closely aligned states are with the AAPA-endorsed ideal PA practice act.
Category 1 executive orders included those that maximized PA flexibility by completely waiving PA supervision or delegation agreements or broadly removing limits on the services that could be provided by PAs (Table 3). Executive orders in 12 states fell into this category, with those from 10 states (Connecticut, Kansas, Louisiana, Maine, Michigan, New Jersey, New York, South Dakota, Tennessee, and Virginia) waving supervisory requirements altogether. Of the 10 states that waived supervision requirements through executive order directives, 7 had already maintained a highly flexible PA practice environment, with 5 or 6 key elements (of 6 possible) of modern PA practice codified. As with APRNs, we included 2 states (Maryland and Nevada) in category 1 that broadly expanded SOP for all health care professionals.
Category 2 comprised executive orders that relieved PAs from administrative burdens or eased supervisory restrictions. We identified executive orders in 5 states (Alabama, Nebraska, Oklahoma, Washington, and Wisconsin) that fell in this category, most of which increased supervisory ratios or made them unlimited.
Scope of Practice: Pharmacists
We identified executive orders in 9 states that included explicit directives from the governor expanding SOP for pharmacists and classified them under 1 of 2 policy categories: those that expanded prescriptive authority or those that extended practice authority (Table 4). We classified executive orders issued in 2 states (Kansas and Michigan) as category 1 by authorizing pharmacists to provide care for routine health maintenance and chronic conditions. We classified 8 states (Arizona, Georgia, Indiana, Iowa, Michigan, North Dakota, South Dakota, and Tennessee) as category 2 because they permitted pharmacists to dispense emergency refills or substitute therapeutics without physician authorization. Michigan was the only state that we identified where an executive order was issued authorizing expanded prescriptive authority (emergency refills and therapeutic substitution) and extended practice authority for pharmacists.
Governor-issued directives in executive orders expanding scope of practice for pharmacists, United States, 2020
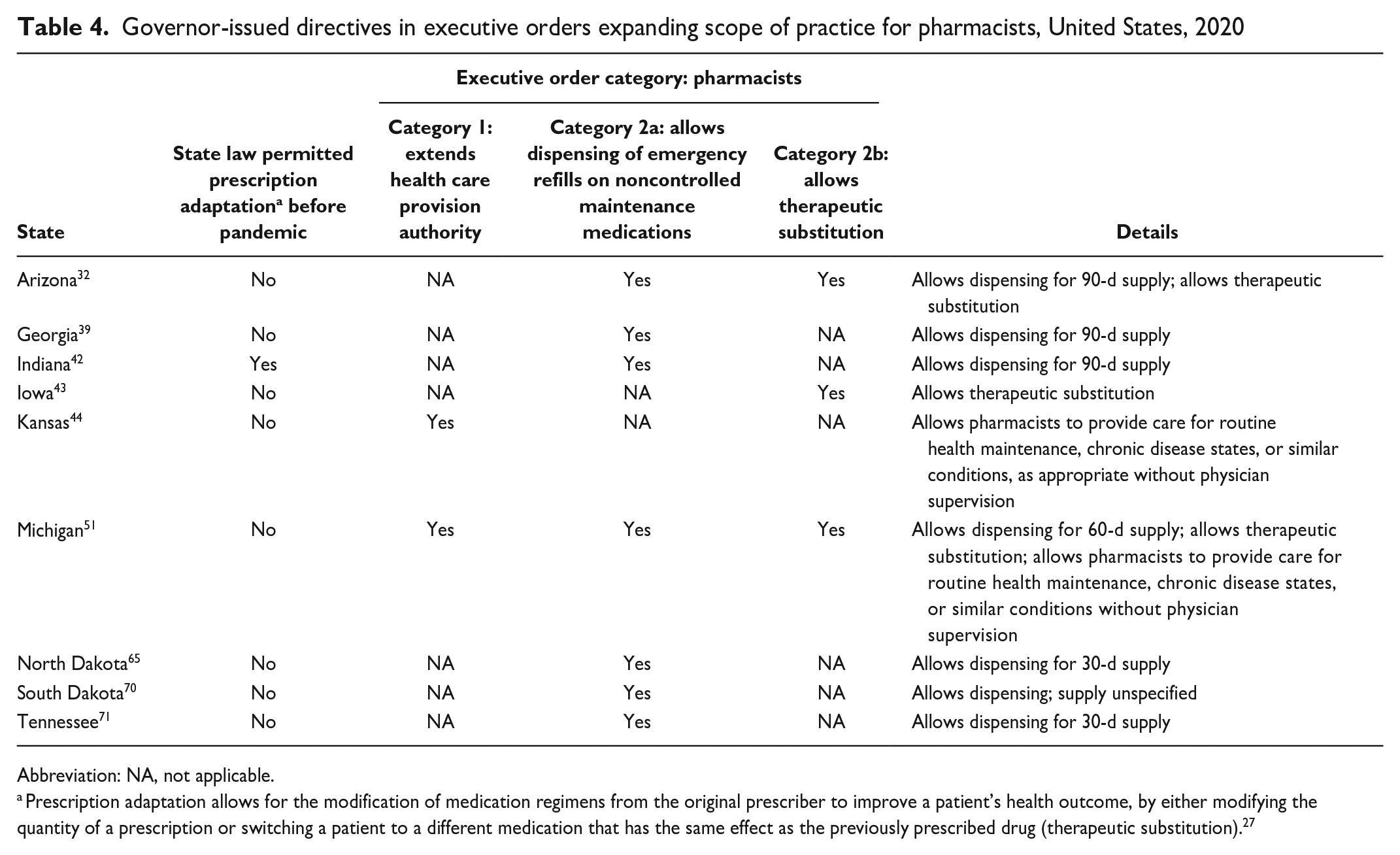
Abbreviation: NA, not applicable.
Prescription adaptation allows for the modification of medication regimens from the original prescriber to improve a patient’s health outcome, by either modifying the quantity of a prescription or switching a patient to a different medication that has the same effect as the previously prescribed drug (therapeutic substitution). 27
Licensing
We identified executive orders in 31 states and the District of Columbia that included explicit directives easing or waiving licensing regulatory barriers for out-of-state health care professionals during the declared state of emergency, through either reciprocal or expedited licensing arrangements (Table 5). Among these, executive order directives in 18 states referred to “health care providers” or “medical personnel” collectively when granting out-of-state licensing flexibility. In the remaining states, executive order directives specified that this licensing flexibility applied to specific professions, most frequently medicine (12 states) and nursing (11 states). Less frequently, pharmacists (5 states), allied professionals (3 states), and mental health professionals (2 states) were specified in executive order directives easing regulatory barriers to allow health care providers to practice across state lines.
State executive orders containing directives explicitly granting licensing flexibility to out-of-state health care professionals, by profession, United States, 2020
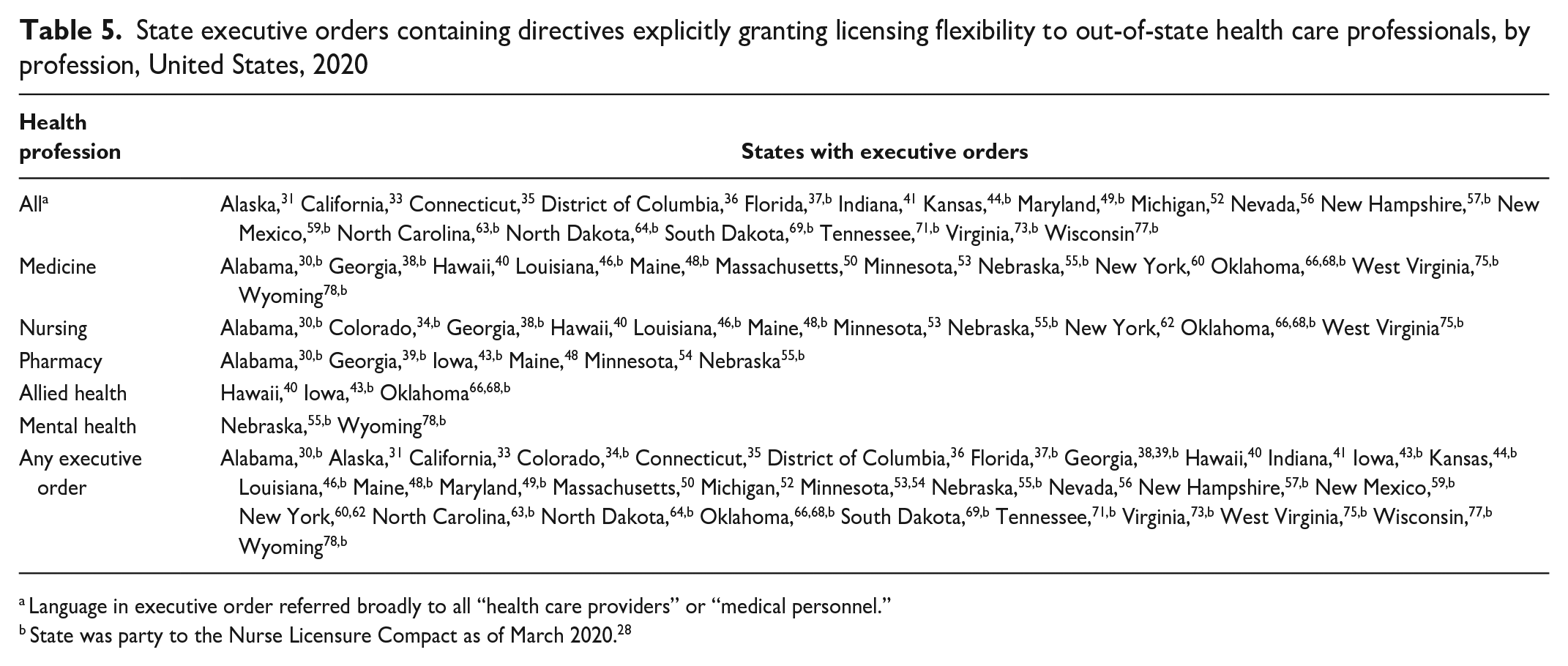
Language in executive order referred broadly to all “health care providers” or “medical personnel.”
State was party to the Nurse Licensure Compact as of March 2020. 28
Of the 31 states and the District of Columbia with executive orders explicitly granting out-of-state licensing flexibility to at least 1 type of health care professional, 21 were party to the NLC at the beginning of the COVID-19 pandemic (Table 5).
Discussion
Governors’ responses to the COVID-19 pandemic provided an opportunity to examine the ways in which policies could temporarily expand health care workforce flexibilities and thereby improve public health response during a period of intense health care service demand. Of particular interest were executive orders that waived CPAs or supervision requirements issued by governors in states that had the most restrictive APRN and PA practice environments before the COVID-19 pandemic, temporarily overhauling the practice environment for advanced practice clinicians in states such as Michigan, Tennessee, and Virginia. We posit that these sweeping regulatory changes were enacted out of necessity because existing regulations and statutes did not embed flexibilities that would have allowed for a sufficient workforce response to the pandemic. In these and other states, the pandemic likely disrupted the traditional power balance, with some advocates hoping that it was the needed catalyst to help convince policy makers that such restrictions are not only unnecessary but constitute barriers to care in regions already experiencing health workforce shortages. 79 However, in many states, the emergency declaration has since expired and, with it, the concomitant provisions waiving practice agreements for advanced practice clinicians. 80 In Michigan, Tennessee, and Virginia, no permanent legislation has been enacted to replace the temporary waivers easing regulatory flexibility.
Throughout the pandemic, pharmacists have played a key role in testing and providing vaccines in the community, the latter of which was federally authorized.81,82 However, our research suggests that states did not fully leverage pharmacists’ competencies to respond to population health needs during the early months of the pandemic. Only Kansas and Michigan authorized pharmacists to provide care for routine health maintenance, chronic disease states, or similar conditions. Expanding pharmacists’ roles would allow them to integrate more fully with health care teams and contribute to public health during nonemergency times and during emergencies.
Directives permitting out-of-state health care professionals to provide care were issued in more states than those expanding SOP. One potential explanation is related federal policy. A Centers for Medicare & Medicaid Services waiver issued early in the pandemic temporarily allowed professionals to be eligible for Medicare and Medicaid reimbursement in states outside their licensed state. 83 However, this federal action did not waive state law, necessitating that states align their licensing requirements for the waiver to apply in practice. Furthermore, the growing number of states party to the NLC and other occupational licensure compacts may represent political acceptance of the need for interstate collaboration to mitigate the challenges presented by a patchwork of state licensing policies in a nation of increasingly mobile workers. 13
While executive orders temporarily easing health workforce regulations in response to COVID-19 present the opportunity to study the effects of policy changes on the workforce, what, if any, impact they will have on permanent efforts to relax practice restrictions for health care professionals is a needed area of future research. Similarly, it may still be too early to fully assess the effects of these temporary policies on workforce and patient outcomes. One early study found that out-of-state licensing flexibilities in response to COVID-19 expanded the respiratory therapist and nurse workforce in New Jersey, 84 while another study suggests that emergency SOP expansions did not always result in practice changes for nurse practitioners. 85
Underlying this study is the idea that explicit directives issued by the governor are important. In some states, a governor’s initial emergency declaration automatically triggers a delegation of authority over workforce regulation to state agencies or departments, ostensibly negating the need for detailed directives in executive orders. 86 While it was beyond the scope of this study for us to assess state agency administrative orders stemming from the COVID-19 public health emergency, this regulatory mechanism could have been a policy lever used by states that needed to expand workforce capacity due to restrictive practice environments yet had no explicit directive issued through an executive order to do so and, thus, were not captured in our analysis (eg, Missouri, Texas, California). 25 This deferral of regulatory oversight may place the emergency workforce policy response in the hands of the state bodies that regulate health care professionals, but it also provides governors with a way to sidestep some of the political responsibility for explicitly taking action on contentious practice issues. Conversely, in some states governors took explicit action but could have relied on existing authorities in state agencies, as in the 8 states where a governor-issued executive order explicitly authorized nurses holding out-of-state licenses to practice, despite the state already being party to the NLC. This duplication of policy efforts suggests that clear directives issued by governors serve an important role in lending visibility, intentionality, and reinforcement to state health workforce policies in times of emergency.
Limitations
This study had several limitations. First, while this work comprehensively examined the status of governors’ executive orders during a critical time in state policy, it did not capture all policies, such as legislation, and did not address policy mechanisms that may have had the same de facto effect on the workforce (ie, state agency regulations). Second, each state has a unique structure for its agencies, executive orders, and emergency response, and comparing them across states would result in an “apples to oranges” comparison, whereas every state has a governor who can issue executive orders. Third, relevant executive orders may have been issued after 2020. We intentionally limited our data collection period to 2020 to examine executive orders issued in the immediate aftermath of the pandemic’s onset. Lastly, as with any qualitative study, the determinations made on each state’s policy and policy category are subjective. We increased rigor by involving expert opinion, but we acknowledge that different researchers and/or interested parties may have classified any particular finding differently.
Conclusion
States with restrictive health workforce practice environments and licensing requirements may be limited in their ability to meet public health and patient care needs in response to a crisis. Governor directives issued through executive orders played an important role in expanding health workforce flexibility in the first year of the pandemic, especially in states with restrictive practice regulations prior to COVID-19. The effects that these temporary flexibilities may have had on patient and practice outcomes or on permanent efforts to relax practice restrictions for health care professionals is an area in need of ongoing research.
Footnotes
Acknowledgements
The authors thank Noah Westfall, MPH, for the research support that he provided for this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Resources and Services Administration, US Department of Health and Human Services (grant no. U81HP26493).