
Abstract
Public health emergencies impact the well-being of people and communities. Long-term emotional distress is a pervasive and serious consequence of high levels of crisis exposure and low levels of access to mental health care. At highest risk for mental health trauma are historically medically underserved and socially marginalized populations and frontline health care workers (HCWs). Current public health emergency response efforts provide insufficient mental health services for these groups. The ongoing mental health crisis of the COVID-19 pandemic has implications for the resource-strained health care workforce. Public health has an important role in delivering psychosocial care and physical support in tandem with communities. Assessment of US and international public health strategies deployed during past public health emergencies can guide development of population-specific mental health care. The objectives of this topical review were (1) to examine scholarly and other literature on the mental health needs of HCWs and selected US and international policies to address them during the first 2 years of the pandemic and (2) to propose strategies for future responses. We reviewed 316 publications in 10 topic areas. Two-hundred fifty publications were excluded, leaving 66 for this topical review. Findings from our review indicate a need for flexible, tailored mental health outreach for HCWs after disasters. US and global research emphasizes the dearth of institutional mental health support for HCWs and of mental health providers who specialize in helping the health care workforce. Future public health disaster responses must address the mental health needs of HCWs to prevent lasting trauma.
The COVID-19 pandemic has devastated the health of communities on a global scale. Frontline health care workers (HCWs) are at greatest risk of its lasting consequences because of inequitable access to health care and limitations on mental health resources. The HCWs who serve in decision-making, caregiving, and counseling roles bear the burdens of the population’s trauma as well as their own. To our knowledge, no published research has examined national and international strategies to address the mental health needs of HCWs during the COVID-19 pandemic. This topical review examined the occurrence of mental health disorders in the US HCW population during the pandemic, summarizes public health strategies used in and outside the United States to address HCW mental health needs, and proposes systemic changes to better support this critical workforce during current and future public health emergencies.
Impact of the COVID-19 Pandemic on the Health Care Workforce
Historically, exposure to traumatic events has had ramifications on mental health.1,2 The COVID-19 pandemic is a global public health disaster that has caused once-in-a-generation physical and mental stress, with widespread economic hardship, social distancing protocols, and increased unemployment rates. 2 Emerging research indicates sharp increases in the prevalence of posttraumatic stress disorder (PTSD), mood and dissociative disorders, and stress disorders, with the most severe psychological harm occurring among HCWs treating COVID-19 patients and in medically underserved populations.3 -5 Chronic burnout among HCWs is a major concern as health care systems continue to operate under challenging conditions. 4
The adverse effects of public health emergencies demonstrate that the mental health of HCWs must be addressed as part of disaster response. Identification of strengths and gaps in past US and international public health emergency responses can guide development of future activities to address postdisaster mental health needs. Specifically, augmentation of public health emergency responses to address the unique mental health needs of HCWs will be imperative for preventing this population from disproportionate harm during and after future disasters.
Methods
The objective of this topical review was to examine scholarly and other literature on the mental health needs of HCWs during the COVID-19 pandemic. Search topics included the following: (1) trends in public health emergencies in the United States; (2) current prevalence and incidence of mental health and substance use disorders during the COVID-19 pandemic; (3) long-term implications of the COVID-19 pandemic on the mental health of HCWs, those infected with COVID-19, and medically vulnerable adult and child populations; (4) mental health training for HCWs in the United States; (5) US public health/mental health response during the COVID-19 pandemic; (6) US telehealth expansion during the COVID-19 pandemic; (7) changes in US health care, billing, and reimbursement regulations during COVID-19; (8) US financial health aid during the COVID-19 pandemic; (9) international public health/mental health workforce strategies during the COVID-19 pandemic; and (10) international public health/mental health workforce strategies during epidemiological emergencies.
The literature search focused on data from the gray literature, news articles, empirical studies, conference presentations, and government documents using databases such as Medline [OVID], PubMed, Google Scholar, and EBSCOhost. Examples of search terms included the following: mental health or psychological or psychiatric providers, professionals, educators, and health workers; occupational stress, emotional health, burnout, anxiety, and distress; regulatory or institutional or organizational mental health policy or policies; site of services (ie, remote or virtual, in-office, in clinic, telehealth, telebehavioral health, telemedicine); and pandemic-related terms (eg, pandemic, COVID-19). The search focused on the period April 1, 2020, through April 30, 2022, to focus on efforts to support HCW mental health during these 2 years of the COVID-19 pandemic. We also searched for literature on past epidemiological outbreaks (eg, severe acute respiratory syndrome coronavirus [SARS-CoV] during 2002-2003 and the H1N1 influenza outbreak of 2009).
We identified 316 articles as meeting topical criteria for initial manual review by 2 reviewers (M.G., J.B.). We applied review and exclusion criteria (ie, non–English language, no supporting data, sample size <5, did not address the topic area) after deduplicating documents using Endnote. A total of 250 articles were excluded, leaving 66 publications for further analysis, which included classification (theme, setting, study population, study methods, sample size) and extraction of findings and implications by category.
Outcomes
Prior research documents the prevalence of psychopathology among HCWs after disasters, with few unified public health solutions designed to meet this population’s mental health needs. 6 No cohesive public health and mental health planning exists to address unmet needs arising from long-term crises. This section describes findings of this topical review on the burden of mental health disorders observed among HCWs in the United States and the lack of response to their rising mental health needs during the pandemic. Actions taken by other countries to meet the needs of their HCWs are summarized and presented as examples for future planning in the United States.
Long-term Mental Health Effects of Past US Disasters on HCWs
The long-term effects of disasters on mental wellness are pronounced. Past emergencies uncovered weaknesses in the ability of the US public health infrastructure to deploy an integrated, unified, and large-scale response to mental health crises.7 -12 The evidence for long-term treatment of mental illness among HCWs after past disasters is sparse. Research has predominantly focused on assessing the prevalence or incidence of disorders such as bipolar I and II depression rather than on the people with the conditions or on the patterns of use of services and barriers to access rather than on how and when to deliver the care when it matters to the person. This dearth of literature on mental health support for HCWs suggests the need for increased research on how to meet the unique mental health needs of HCWs.
Research on the impact of pandemic-related stress on HCWs provides evidence of increasing mental health symptoms. 13 An early 2020 study of 1119 HCWs in the United States found that 93% experienced stress, 86% experienced anxiety, 76% experienced exhaustion, and 75% were overwhelmed because of the pandemic. 14 Of 1685 HCWs who participated in a subsequent survey, 39% reported PTSD, 33% reported anxiety, 17% reported depressive symptoms, and 5% reported suicidal ideation during the pandemic. 15 Mental health concerns among HCWs persisted beyond the first wave of COVID-19 infections in the United States. A late-2020 state-level study of 605 HCWs reported that 43% experienced mild or higher levels of anxiety, 32% any sleep disturbance, 22% PTSD symptoms, 23% lower levels of resilience, and 14% depression 8 months after the initial surge. 16 Risk factors associated with poor mental health among HCWs include higher frequency of exposure to patients infected with COVID-19, being female, younger age, and having a previous psychiatric history. 16
Maldistribution and the shortage of mental health providers across the United States create barriers to accessing care for HCWs. 17 Research conducted during prior pandemics indicates that HCWs are less likely than non-HCWs to actively seek out or accept emotional help despite showing signs of psychological distress. 18 HCWs may self-isolate out of fear of infecting close contacts, preventing them from seeking mental health care. 19 These detrimental mental and physical health effects are likely to diminish the size of the health care workforce over time. 20 A 2020-2021 American Medical Association survey of health care organizations found that half of all respondents reported at least some burnout symptoms, including 16% who reported persistent, nonsubsiding symptoms. 21 An additional contributor to burnout may be leadership turnover, as indicated by a growing number of health official resignations caused by the politicization of public health, the negative response to the use of public health emergency powers, and the implementation of disease control measures. 22
US Systemic Responses to the COVID-19 Pandemic
The COVID-19 pandemic is likely to have both short- and long-term implications for the mental health of US HCWs.3,21 National support for HCWs is shown by efforts to expand the capacity of workers and broaden their ability to practice. Emergency funding at the national level to augment mental health facilities and service provision modalities, particularly telehealth services, continues to support the delivery of care. The Coronavirus Aid, Relief, and Economic Security (CARES) Act of 2020 provided $425 million for the Substance Abuse and Mental Health Services Administration, including $250 million for certified community behavioral health clinics, $50 million for suicide prevention programs, $100 million for emergency response spending, and $15 million for tribal communities.23,24 Additionally, the Centers for Disease Control and Prevention (CDC) activated a cooperative agreement for emergency response, awarding approximately $2 billion in CARES Act funding to expand, establish, and sustain a public health workforce. 25
The American Rescue Plan Act of 2021 (ARPA), a $1.9 trillion package intended to mitigate the public health and economic impacts of the COVID-19 pandemic, provided nearly $2.5 billion in funding for states and territories to address the mental health crisis, reduce burnout among HCWs, and support training efforts.25,26 This package directed $1.65 billion in funding to the Substance Abuse and Mental Health Services Administration for community block grant programs for delivery of mental health and substance use disorder services; behavioral health training for health care professionals, paraprofessionals, and safety officers; and a behavioral health education and awareness campaign.27 -29 Some ARPA allocations, such as funding to provide access to mental health care for children, include language that explicitly allows organizations and institutions that are awarded funding to provide workforce development opportunities such as teleconsultation and training. 30 While the block grants do not share this permitting language, allowable services include expanding capacity and training of the behavioral health workforce to meet mental health needs.28,29 These funding streams offer a key opportunity for investing in education and fostering resilience building among the health care workforce.
Additional efforts to support HCWs include establishment of the Physician Support Line for physicians in the United States to access care from licensed psychiatrists (https://www.physiciansupportline.com). Online mental health resources may be useful for some HCWs, although many are unlikely to make contact with a mental health provider, heightening the risk of long-term moral injury. 31 A 2020 survey of US HCWs indicated that many report their employers as “falling short” in providing adequate paid sick leave that could be used for mental health care, highlighting the need for supportive workplace benefits such as time off and enhanced health insurance coverage. 3 Institutions that receive ARPA funding will be positioned to take the lead on creating local partnerships and resources to directly support HCWs and provide HCW training for management of high levels of exposure to occupational stress. 29
To address the disruption in service delivery during the COVID-19 pandemic, HCWs rapidly expanded the use of telehealth. 32 Policy changes at the state and federal levels allowed for expansion of telehealth authorization, payment parity, and reimbursement across insurers; waived requirements for written consent to receive treatment; and provided service delivery through video or audio-only methods, including methods not in compliance with the Health Insurance Portability and Accountability Act. 33 The CARES Act allocation provided expansion of telehealth for people insured by Medicare, private health insurance, and other federally funded programs.3,34 The prohibition of online form–only prescribing of controlled substances in the Ryan Haight Online Pharmacy Consumer Protection Act of 2008 was temporarily suspended in March 2020 during the pandemic to allow health care providers to prescribe medication-assisted treatment through telehealth.35,36 The Centers for Medicare & Medicaid Services expanded telehealth coverage to allow provision of services in a wider range of facilities and broaden the number and types of providers eligible for payments. 37 The Coronavirus Preparedness and Response Supplemental Appropriations Act of 2020 included a waiver that removed rural restrictions on Medicare providers, allowing them to offer beneficiaries telehealth services regardless of whether the beneficiary was located in a rural community. 38 Widespread adoption of telehealth services continues to allow HCWs in rural and urban areas to provide services such as triage, screening, monitoring, and counseling through telehealth. 39 Although many of these federal and state government–implemented policies were issued as temporary, many legislators are calling for them to be made permanent, and continued expansion of these services may allow for greater access to mental health care for HCWs. 40
The need to prepare the public health workforce amid the challenges of the pandemic prompted rapid changes to practice, education, and training standards. Before the COVID-19 pandemic, many of the health occupations that would become in high demand during the pandemic were regulated in a way that limited the flow of professionals across state lines. 41 The Uniform Emergency Volunteer Health Practitioner Act is model legislation enacted in 2007 by a committee appointed by and representing the National Conference of Commissioners on Uniform State Laws. 42 Adopting states can recognize out-of-state licensure for various health practitioners during a state of declared emergency; several states enacted this mechanism during the COVID-19 pandemic, allowing volunteer workers from other states to practice without having to obtain a state-specific license and ensuring a greater portion of HCWs could meet high service demands. 43 Additionally, some states authorized practice without supervision for recent HCW graduates and lowered the number of required on-site clinical hours in health care facilities, allowing them to enter the workforce immediately after graduating. 44 Other changes included state government suspension of continuing education requirements and a reduction of inactivation fees, boosting the number of HCWs eligible to practice, and lowering capacity strain. 45
Government, educational, and health care organizations are using various strategies to meet mental health needs in the United States, including telehealth policy changes, increased funding for certified community behavioral health clinics, expansion of health care provider capacity, and relaxation of education and training requirements (Box).
Federal and state legislative and policy efforts to expand the mental health workforce in response to COVID-19
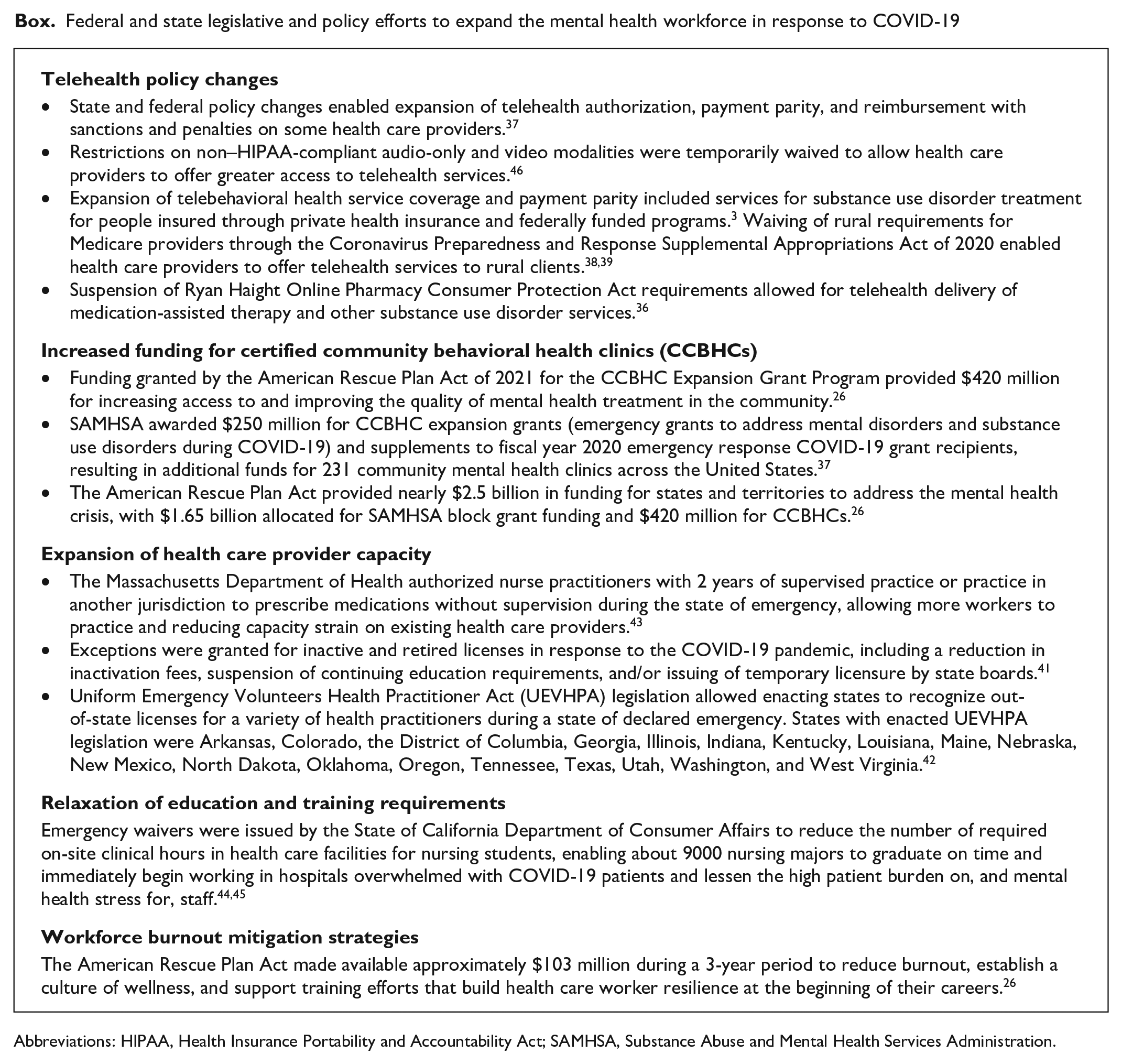
Abbreviations: HIPAA, Health Insurance Portability and Accountability Act; SAMHSA, Substance Abuse and Mental Health Services Administration.
International Disaster Responses During the COVID-19 Pandemic
Research on the public health responses of other countries to rising mental health needs in the wake of the pandemic is limited. However, experiences of HCWs in China, the first country hardest hit by the pandemic, generated a large body of research. 47 This research demonstrates effective deployment of emergency services to meet mental health service demands. Summaries of public health workforce expansion efforts in China are presented as examples to inform workforce strategies for the United States.
Increased mental health needs of HCWs treating COVID-19 patients have prompted local Chinese governments and hospitals to establish support mechanisms to help staff safeguard their health. The government has implemented interventions that include activating mental health teams to serve in coordination with local health authorities. 48 Hospitals across China have developed psychological intervention teams available via hotline to provide support to HCWs and offer online education to HCWs on coping strategies. 48 Academic and government agencies in China are also promoting telemental health services for HCWs and people diagnosed with COVID-19 along with their families. 49 The overlap in the characteristics of China’s emergency response to the SARS outbreak of 2003 and the COVID-19 pandemic, including regular clinical screenings for HCWs and the addition of psychiatrists to medical assistance teams, highlights China’s HCW support strategies as a potential model for public health emergency planning in the United States.
Little published research from other countries beyond China on HCW-focused mental health interventions is available. Findings on the implementation of Compassion, REsilience And TEam-building (CREATE), a team-based support intervention implemented at a tertiary teaching hospital in Canada, suggest that rapid mobilization of organization-level interventions during a pandemic can ameliorate the mental health burden on HCWs 50 ; however, these findings have not been replicated or tested elsewhere. A systematic review of the literature on electronic mental health solutions deployed to support HCWs during the COVID-19 pandemic, such as a tele-peer-to-peer psychological support program and an evidence-based digital learning package on psychological well-being for HCWs, found that most identified interventions targeted China’s workforce. Additional countries assessed included Canada, Iran, Malaysia, the United Kingdom, and the United States. 51
Public Health Implications
Trauma in populations overwhelmed by large-scale emergencies can trigger an increase in mental health problems among HCWs, who face high levels of exposure to disaster and low levels of access to care. 52 Unlike elements of emergency response provided through organizations such as the National Guard, which offer physical assistance, no standard aid exists to address mental health needs during a disaster. Evidence indicates that perceived or clinically diagnosed need for mental health care does not translate to an increased use of services.9,53 When coupled with existing workforce shortages and health care provider scarcity in many areas of the United States, the surge in mental health needs caused by increasingly occurring disasters will only further strain HCWs. Development of population-specific interventions is proposed as a viable solution to fill the absence of a nationally unified public health response to mental health crises after disasters.
Systemic Changes to Support the US Health Care Workforce
Strategies to support HCWs in the United States and mitigate burnout are needed. Evidence suggests that systemic integration of interventions tailored to the needs of HCWs should be implemented on a national scale. Policy makers and health care leaders can play a critical role in designing, funding, and implementing mental health initiatives for HCWs. Studies investigating the management of moral injury and mental health sequelae among HCWs suggest a tiered approach of anticipating, recognizing, and managing signs of mental illness. 54 We recommend that health care leaders implement and encourage supportive “buddy” relationships, managerial debriefs, environmental well-being supports, and rapid access to brief mental health interventions for HCWs. Greater access to mental health services that operate both within and outside of typical business hours, as well as effective screening and referral programs for HCWs, may be necessary to reach HCWs. 55 Implementation of mental health awareness training for HCWs could also help HCWs recognize their own mental health needs and prioritize their own and their colleagues’ mental well-being. 56 Potential structural barriers to implementing mental health supports for HCWs include service provision costs, HCW scheduling and time limitations, insufficient hours of mental health provider availability, and waitlists for services. 53 These changes will require the government, health care systems, and HCW employers to act in concert to overcome these potential barriers. 57 Without them, hospitals and health systems will continue to face mounting staffing shortages that could jeopardize access to and quality of care. Future research could identify mental health support such as that delivered under pandemic conditions for HCWs with limited access to care.
Health Care Workforce Planning
Greater training and resources to support HCWs are imperative for addressing the mental health needs of HCWs. Wait times for mental health services increased during the pandemic because of a rise in referrals to primary and specialty care settings that are likely to result in more patients with psychiatric disorders in both primary and secondary care. 54 Strategies to manage the increase in demand include closer liaisons between mental health practitioners and primary care colleagues to foster mental health integration into medical treatment settings. 17 Existing research suggests there may be value in implementing mental health first aid training programs, a public health intervention strategy that equips individuals with the skills to recognize and respond appropriately to signs of mental health problems, for primary care providers and the emergency department workforce. 56 Provision of mental health first aid training can also foster peer-to-peer support for HCWs in preparation for future disasters. 57 Additionally, the National Institute for Occupational Safety and Health is expanding its Total Worker Health program to advance the well-being of HCWs. 58 Total Worker Health programs are designed to be voluntary and participatory and aim to give employees a voice in their work conditions by designing work schedules to reduce stress and cultivating leaders and values that encourage healthy supervision and respect for workers. 59 Lastly, surveys to track trends in HCW stress levels can be deployed by health care organizations to monitor the impact of workload and burnout on their workforce. 60
Conclusions
HCWs are facing substantial mental health stressors, burdens, and challenges in the wake of the COVID-19 pandemic. Continued attention among policy makers and health care managers to mental health risk for capacity-strained HCWs is necessary. 61 Although ARPA funding allocations are not universally designated for workforce development and training, funding can be used by organizations that employ HCWs to implement resiliency training and workforce development efforts. Continued federal and state funding awards to institutions that educate and train future HCWs are, therefore, needed for development of adaptive, flexible curricula and culturally sensitive resilience interventions that optimize well-being in workplaces with high levels of stress due to emotional exhaustion, increased demands on limited time, longer and higher-intensity work hours, low autonomy, and few work breaks. 58 Extended funding to organizations that employ HCWs ensures adequate staffing, paid time off, and availability of mental health resources will be a critical mechanism for reducing burnout. Lastly, HCW leadership training in mental health symptom recognition and destigmatization of mental health will create a foundation for building a culture of wellness.
Footnotes
Acknowledgements
The authors thank the Behavioral Health Workforce Research Center for its contributions to this article. Victoria Schoebel, MPH, contributed to the authors’ responses to reviewer comments. Caitlyn Wayment, MPH, Jackson Bensley, MPH, Brittany Jullie, MPH, and Isabella Ginsberg, MSW, contributed to the literature review.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Health Resources and Services Administration (HRSA) of the US Department of Health and Human Services (HHS) as part of an award totaling $3 546 763 with zero percentage financed with nongovernmental sources. The contents are those of the authors and do not necessarily represent the official views of, nor an endorsement, by HRSA, HHS, or the US government.