
Abstract
Objectives:
The association among psychiatric treatment history, HIV, and suicide reattempts among people starting treatment for substance use is not well understood. The objective of this study was to describe, by HIV status, the risk and protective factors associated with suicide reattempts among adults seeking treatment for substance use.
Methods:
The study included 340 390 US adult residents aged ≥18 years in the Addiction Severity Index–Multimedia Version network from January 1, 2014, through December 31, 2020. We used adjusted logistic regression models to estimate strength of association between prior psychiatric treatment, HIV status, and sociodemographic factors and suicide reattempts within 30 days of treatment evaluation.
Results:
Adults who had been prescribed psychiatric medication were less likely to have a recent suicide reattempt (adjusted odds ratio [aOR] = 0.8; 95% CI, 0.7-0.8) than adults with no prescription history. Adjusted models found similar protective effects between psychiatric treatment and suicide reattempts among adults reporting abuse, mental illness, injection drug use, and limited activity because of a medical condition. Conversely, the following were associated with recent suicide reattempts: being male (aOR = 1.4; 95% CI, 1.3-1.5), having a high school education/GED (General Educational Development) or less (aOR = 1.2; 95% CI, 1.1-1.2), being single (aOR = 1.2; 95% CI, 1.1-1.3), experiencing a pain problem (aOR = 1.2; 95% CI, 1.2-1.3), and not being referred to substance use treatment by court (aOR = 3.4; 95% CI, 3.2-3.7).
Conclusions:
A history of prescribed psychiatric medication is significantly associated with a reduced risk for suicide reattempts among adults seeking substance use treatment. Clinicians should consider incorporating mental health and suicide assessments into substance use treatment plans.
Keywords
In 2019, the suicide death rate was highest by age among US adults aged 45-54 years, and the drug poisoning (overdose) death rate was highest among US adults aged 30-39 years. 1 Even so, overdose rates increased faster among adults aged 25-44 years than among adults aged ≥45 years, 2 and during the COVID-19 pandemic, the rate of drug overdose deaths accelerated. 3 Furthermore, people exposed to suicide have an increased risk of suicidal ideation and behavior. 4
Substance misuse is a risk factor for suicide and unintentional death, particularly among people experiencing mental distress. 5 An underlying psychiatric condition, including mental illness or substance use disorder, has been found in approximately 90% of people who died by suicide. 6 Psychiatric conditions have also been associated with attempted suicide. 7 Adherence with psychiatric treatment is a protective factor for suicide reattempts among adults aged ≥18 years. 8
Increased rates of suicide have also been associated with people living with HIV/AIDS, in part but not solely because of associated mental distress and substance use. 9 Approximately 1.2 million people in the United States were living with HIV/AIDS in 2018, with an estimated 38 000 becoming newly infected in the 12 months before the 2018 estimate. 10 Although estimated rates of HIV infection among people with mental illness (eg, psychosis, mood disorders) in the United States vary by study cohort (1.0%-22.9%),11-14 they are higher than the estimated 0.4% rate of HIV infection among the US population aged 15-49 years. 15 Similarly, in the United States, the prevalence of HIV infection is also higher among people who inject drugs (an estimated 8.7%-22.4% 16 ) than among the general population. 15
Protective factors for suicide attempts and reattempts among people with HIV/AIDS have not been well defined. Préau et al identified family support as a protective factor for suicide attempts. 17 Bantjes and Kagee found that treatment for common mental disorders was associated with a reduction in suicidal ideation and planning, but not suicide attempts, among people living with HIV/AIDS. 18 The effect of psychiatric treatment on future suicide attempts among people with HIV/AIDS and substance use disorder is not well known.
Information on protective factors associated with suicide reattempts among people with HIV/AIDS is greatly needed because people who have attempted suicide are at a greater risk (than people who have not attempted suicide) for reattempts and subsequent death as a result of suicide. 19 Understanding the relationship among substance use, mental illness, HIV/AIDS, and suicide in the context of substance use treatment could identify opportunities for assessment, treatment, and prevention of future suicides. The objective of this study was to describe the risk and protective factors, by HIV status, associated with suicide reattempts among adults seeking treatment for substance use.
Methods
Data Source
Data were collected from adults being assessed for substance use and treatment planning by 968 treatment facilities located in 45 states and the District of Columbia during January 1, 2014, through December 31, 2020. Adults were evaluated using the Addiction Severity Index–Multimedia Version (ASI-MV), a component of the National Addictions Vigilance Intervention and Prevention Program (NAVIPPRO). 20 NAVIPPRO is a risk management system to monitor prescription opioids and other Schedule II and III therapeutic agents. 21 The NAVIPPRO ASI-MV, a modified version of the Addiction Severity Index, 21 is a self-administered computerized assessment tool used to collect patient-reported data (medical, employment, drug, alcohol, legal, family and social relationships, and mental illness) from adults aged ≥18 years who are entering substance treatment centers. 22 The NAVIPPRO ASI-MV performs well in test–retest reliability and criterion validity measures. 23 Because data in the ASI-MV system are deidentified and aggregated, this study was exempt from the Centers for Disease Control and Prevention (CDC) Institutional Review Board review and approval. The ethical integrity of the study was ensured by CDC’s National Center for HIV, Viral Hepatitis, STD, and TB Prevention ethics officials, who were not involved in the conduct of the study.
Analytic Sample Selection
The NAVIPPRO ASI-MV dataset comprised 406 216 observations; of these, 65 826 (16.2%) were repeated observations from the same individual (Figure). We analyzed the most recent observation for each of 340 390 unique individuals indicated by the most recent ASI-MV assessment date. We excluded from analysis individuals who (1) had missing values on HIV/AIDS problems, emotional or psychiatric treatment, suicide attempts >30 days before ASI-MV assessment date, and age at most recent ASI-MV assessment; (2) had no suicide attempts >30 days before the most recent ASI-MV assessment; or (3) were aged <18 years at most recent assessment (n = 286 220). The analytic sample consisted of 54 177 unique adults aged 18-90 years.
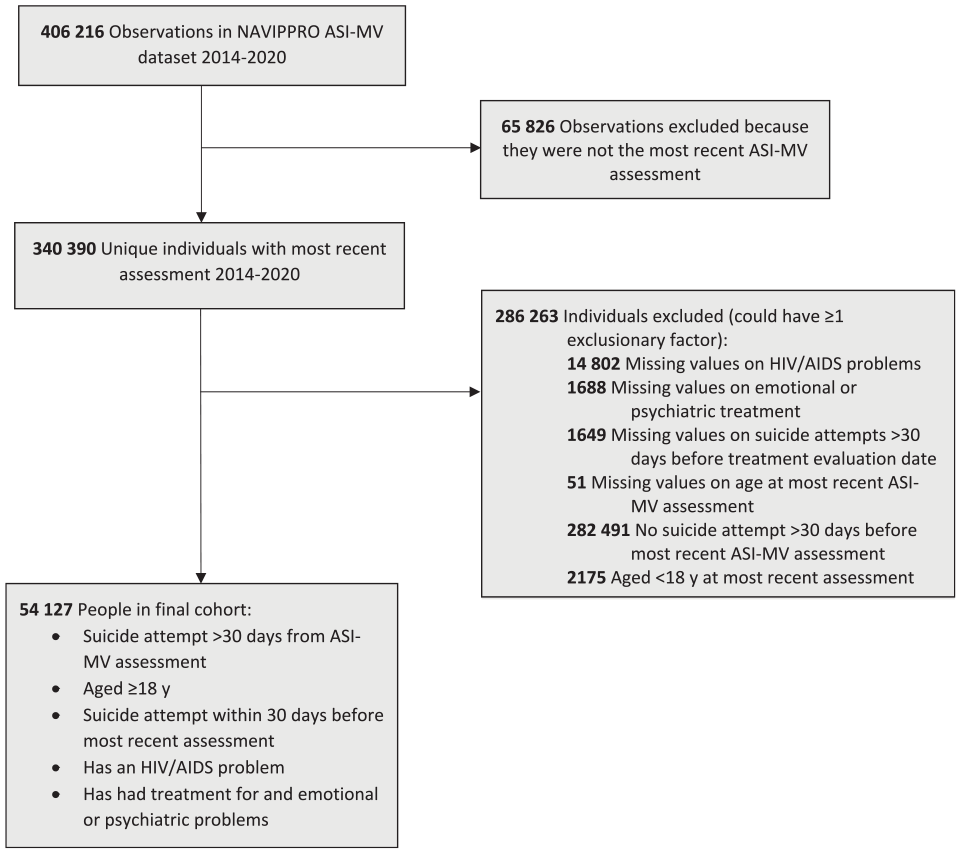
Flow of individuals in a cohort from the National Addictions Vigilance Intervention and Prevention Program (NAVIPPRO) Addiction Severity Index–Multimedia Version (ASI-MV) network. The NAVIPPRO ASI-MV is a self-administered computerized assessment tool used to collect patient-reported data (medical, employment, drug, alcohol, legal, family and social relationships, and mental illness) from adults aged ≥18 years who are entering substance treatment centers. The analytic sample consisted of 54 177 unique adults aged 18-90 years. Data source: NAVIPPRO. 20
Measures
The study outcome measure of interest was suicide reattempt (yes or no) within 30 days before ASI-MV assessment among people who had attempted suicide >30 days before ASI-MV assessment. We chose suicide attempts within 30 days before ASI-MV assessment because those attempts correspond to the high-risk category of the Columbia-Suicide Severity Rating Scale (C-SSRS). 24 We could not use the C-SSRS as the outcome measure because the NAVIPPRO dataset did not include information on suicidal ideation, planning, and lifetime attempts necessary to assign patients to the C-SSRS high-risk category.
We assessed HIV/AIDS-related concerns with responses to the yes/no question “Are you having problems with HIV or AIDS?” We assessed psychiatric treatment with responses to the yes/no question “In the past 30 days, were you prescribed medication for emotional or psychiatric problems?” We included the following information as potential effect modifiers and confounders: sociodemographic characteristics (age, race and ethnicity, sex/gender identity, education, employment status, marital status, and housing during previous 3 years), mental and behavioral health (history and type of abuse, diagnosis of a mental illness [depression or mood disorder, manic depression or bipolar disorder, posttraumatic stress disorder (PTSD)], injection drug use, court-suggested substance use treatment), and physical and medical information (pain problem, physical or medical problem interfering with or limiting daily activities).
Statistical Analyses
We conducted univariable, bivariable, and multivariable regression analyses with frequency tabulations and Wald χ2 tests to determine differences in the prevalence of a suicide attempt within 30 days before ASI-MV assessment. We measured collinearity through condition indices (<30) and variance inflation (<10). We used logistic regression analysis to examine the association of independent variables as potential confounders or effect modifiers with suicide attempt within 30 days before ASI-MV assessment and performed log likelihood ratio tests to assess interaction between the exposure variables (indicating effect modification). Interaction terms with a significant value (P < .05) were placed in the adjusted model that indicated independent association of each pair of exposure and outcome variables. We compared crude odds ratios (ORs) and adjusted odds ratios (aORs) to control for confounding among independent variables. We also conducted multivariable regressions with backward elimination based on log likelihood ratio tests (P < .05) to assess the association between prior psychiatric treatment and suicide attempt, controlling for demographic characteristics. For variables with >10% missing observations, we included a “missing” category in the univariate and multivariate analyses to identify any significant effects of missing values on ORs. We conducted separate analyses to account for the interaction between prescribed medication for an emotional or psychiatric problem and the exposure variables of abuse, depression diagnosis, manic depression/bipolar disorder diagnosis, PTSD diagnosis, injection drug use, and having a physical or medical problem interfering with or limiting daily activities. We conducted 1 model that excluded all variables that interacted with psychiatric treatment and 6 models that included only 1 of the 6 variables that interacted with psychiatric diagnosis. The Hosmer–Lemeshow goodness-of-fit test ensured model goodness of fit with P > .05. We used SAS version 9.4 (SAS Institute, Inc) for all analyses.
Results
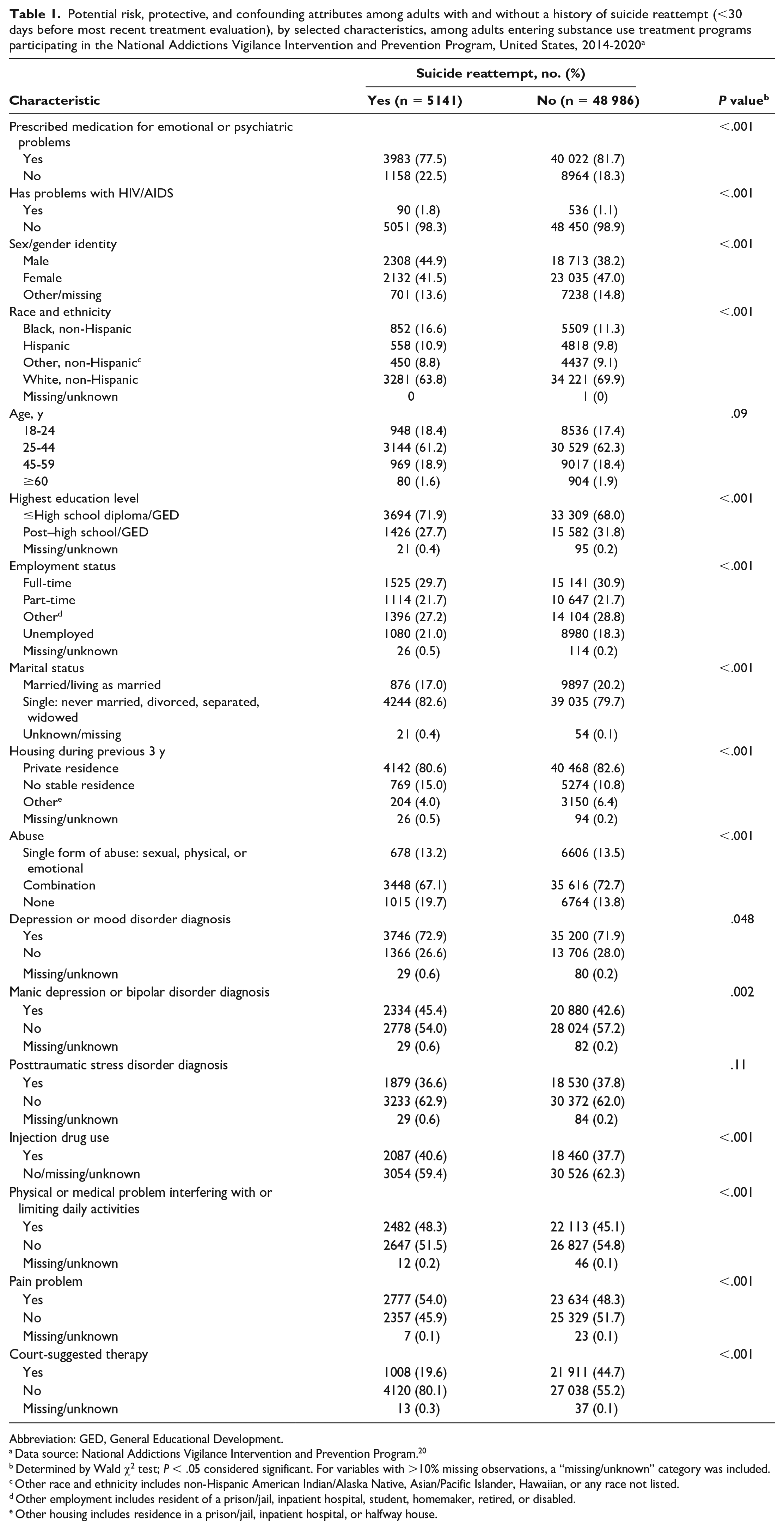
Approximately 10% (5128 of 54 077) of people had a suicide reattempt within 30 days before ASI-MV assessment. Regardless of suicide reattempt, most adults in the sample had been prescribed medication for emotional or psychiatric problems (Table 1). A smaller percentage of people who reattempted suicide were prescribed medication (77.5% [3983 of 5141]) when compared with those with no suicide reattempt (81.7% [40 022 of 48 986]). Except for age and PTSD history, each exposure characteristic assessed had a significantly different distribution when clients who reattempted suicide were compared with those who did not reattempt suicide.
Potential risk, protective, and confounding attributes among adults with and without a history of suicide reattempt (<30 days before most recent treatment evaluation), by selected characteristics, among adults entering substance use treatment programs participating in the National Addictions Vigilance Intervention and Prevention Program, United States, 2014-2020 a
Abbreviation: GED, General Educational Development.
Data source: National Addictions Vigilance Intervention and Prevention Program. 20
Determined by Wald χ2 test; P < .05 considered significant. For variables with >10% missing observations, a “missing/unknown” category was included.
Other race and ethnicity includes non-Hispanic American Indian/Alaska Native, Asian/Pacific Islander, Hawaiian, or any race not listed.
Other employment includes resident of a prison/jail, inpatient hospital, student, homemaker, retired, or disabled.
Other housing includes residence in a prison/jail, inpatient hospital, or halfway house.
Multivariable and Univariable Logistic Regression Modeling of Risk and Protective Factors for Suicide Reattempt
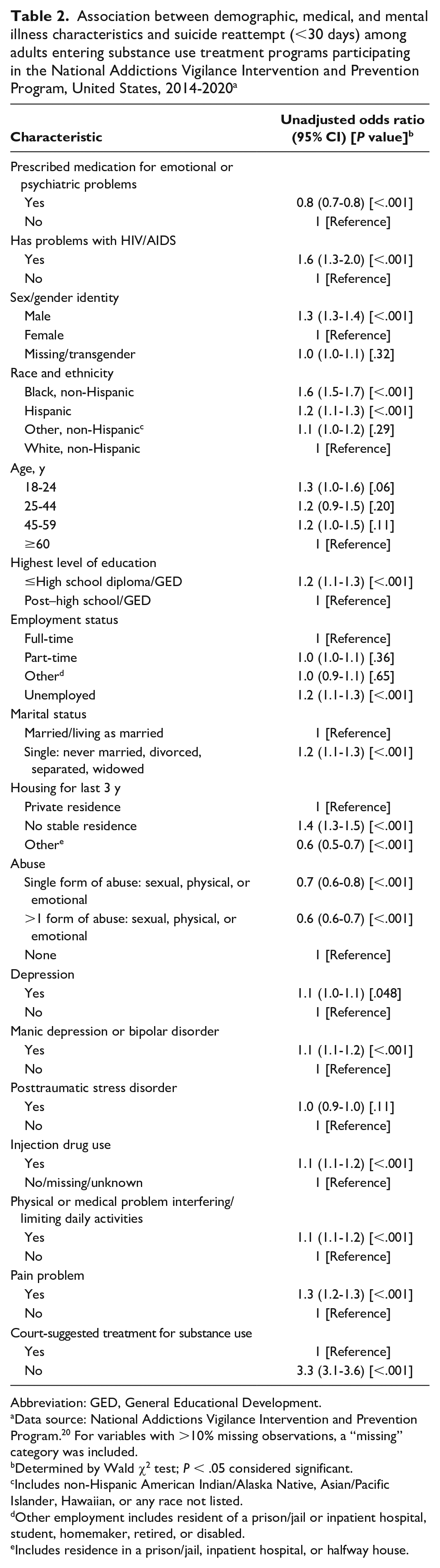
In our first model, which excluded the variables that interacted with our main exposure variable (prescribed medication for psychiatric or emotional problems), we found that people who were prescribed medication had lower odds of a suicide reattempt than people who were not prescribed medication (OR = 0.8; 95% CI, 0.7-0.8) (Table 2). Adjusted models found similar protective associations between interaction terms with receiving medication and the variables of emotional, physical, and sexual abuse; depression, bipolar disorder, and PTSD diagnosis; injection drug use; and a physical or medical problem interfering with or limiting daily activities (Table 3).
Association between demographic, medical, and mental illness characteristics and suicide reattempt (<30 days) among adults entering substance use treatment programs participating in the National Addictions Vigilance Intervention and Prevention Program, United States, 2014-2020 a
Abbreviation: GED, General Educational Development.
Data source: National Addictions Vigilance Intervention and Prevention Program. 20 For variables with >10% missing observations, a “missing” category was included.
Determined by Wald χ2 test; P < .05 considered significant.
Includes non-Hispanic American Indian/Alaska Native, Asian/Pacific Islander, Hawaiian, or any race not listed.
Other employment includes resident of a prison/jail or inpatient hospital, student, homemaker, retired, or disabled.
Includes residence in a prison/jail, inpatient hospital, or halfway house.
Adjusted association for prescribed medication for emotional or psychiatric problems, stratified by demographic, medical, and mental illness, and suicide reattempt (<30 days) among adults entering substance use treatment programs participating in the National Addictions Vigilance Intervention and Prevention Program, United States, 2014-2020 a
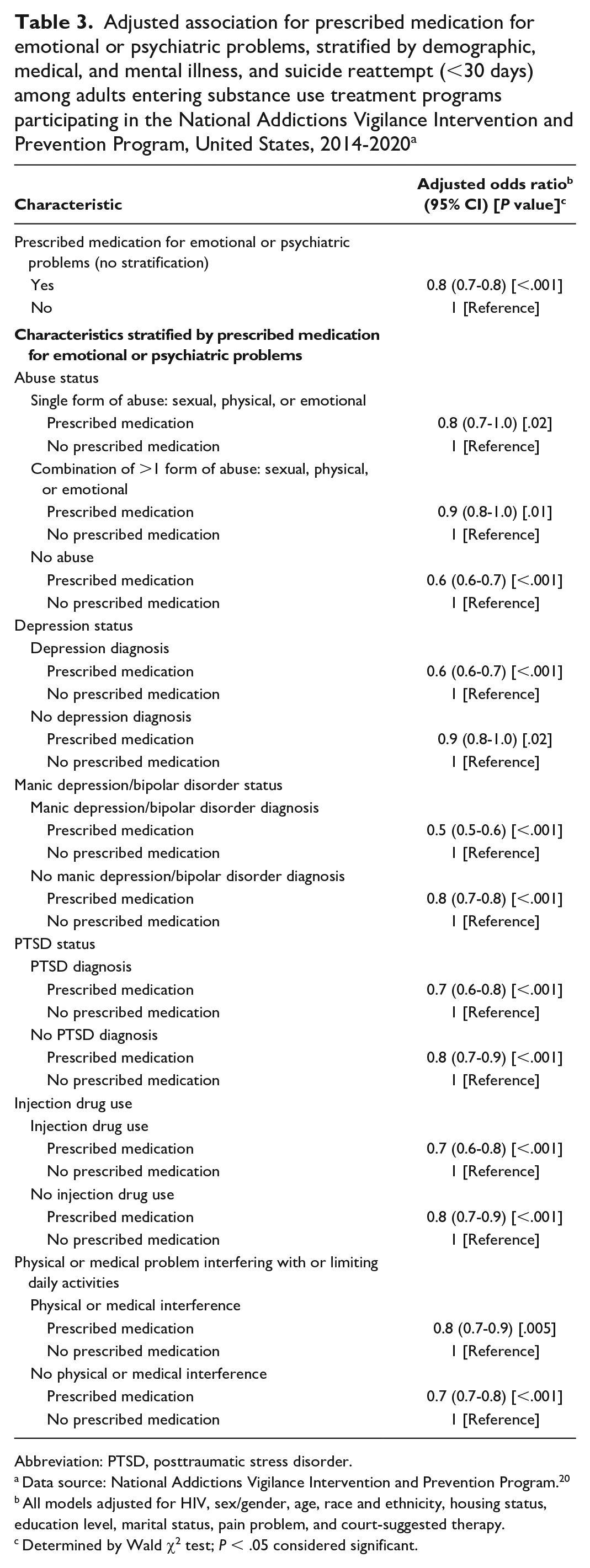
Abbreviation: PTSD, posttraumatic stress disorder.
Data source: National Addictions Vigilance Intervention and Prevention Program. 20
All models adjusted for HIV, sex/gender, age, race and ethnicity, housing status, education level, marital status, pain problem, and court-suggested therapy.
Determined by Wald χ2 test; P < .05 considered significant.
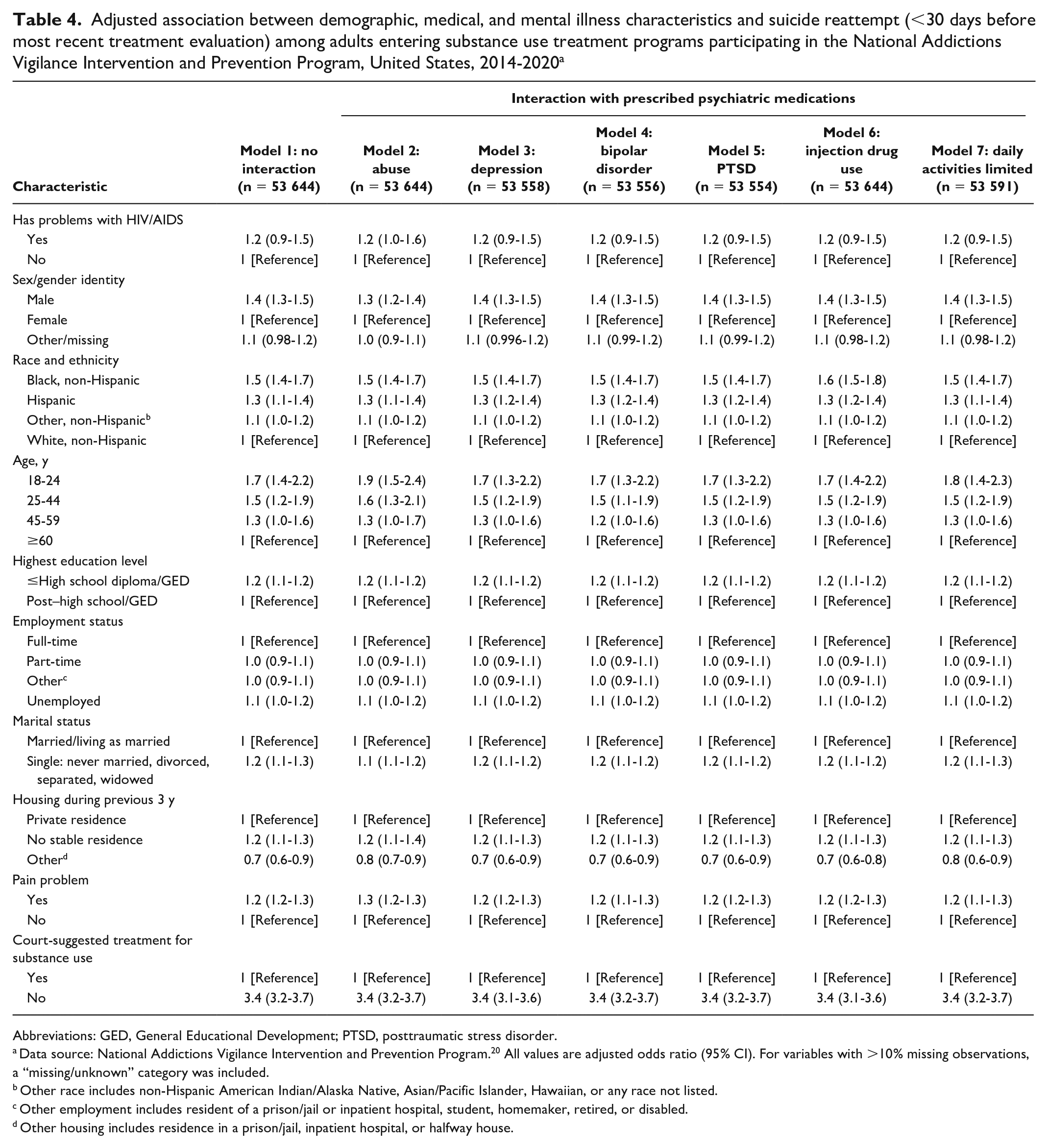
In our full model without interaction terms, we found that a self-reported problem with HIV/AIDS was not associated with a suicide reattempt (aOR = 1.2; 95% CI, 0.9-1.5) (Table 4). Among the exposure variables that modified the association between receiving medication for emotional or psychiatric problems and suicide reattempt, we found greater odds of suicide reattempt as follows: among men (aOR = 1.4; 95% CI, 1.3-1.5) than among women, among non-Hispanic Black and Hispanic people (aOR = 1.5 [95% CI, 1.4-1.7] and aOR = 1.3 [95% CI, 1.1-1.4], respectively) than among non-Hispanic White people, among people aged 18-24 years and 25-44 years (aOR = 1.7 [95% CI, 1.4-2.2] and aOR = 1.5 [95% CI, 1.2-1.9], respectively) than among people aged ≥60 years, among people with a high school diploma/GED (General Educational Development) or less (aOR = 1.2; 95% CI, 1.1-1.2) than among people with more education, among people who were single (aOR = 1.2; 95% CI, 1.1-1.3) than among people who were married or living as married, among people with no stable residence (aOR = 1.2; 95% CI, 1.1-1.3) than among people living in a private residence, among people with a pain problem (aOR = 1.2; 95% CI, 1.2-1.3) than among people without one, and among people not undergoing court-suggested treatment for substance use (aOR = 3.4; 95% CI, 3.2-3.7) than among those who were undergoing such treatment. We found similar results in the other models with interaction terms.
Adjusted association between demographic, medical, and mental illness characteristics and suicide reattempt (<30 days before most recent treatment evaluation) among adults entering substance use treatment programs participating in the National Addictions Vigilance Intervention and Prevention Program, United States, 2014-2020 a
Abbreviations: GED, General Educational Development; PTSD, posttraumatic stress disorder.
Data source: National Addictions Vigilance Intervention and Prevention Program. 20 All values are adjusted odds ratio (95% CI). For variables with >10% missing observations, a “missing/unknown” category was included.
Other race includes non-Hispanic American Indian/Alaska Native, Asian/Pacific Islander, Hawaiian, or any race not listed.
Other employment includes resident of a prison/jail or inpatient hospital, student, homemaker, retired, or disabled.
Other housing includes residence in a prison/jail, inpatient hospital, or halfway house.
Discussion
Because prior suicide attempt is one of the most important risk factors for future suicide 19 and substance use is also a risk factor for suicide, 5 we sought to identify potential risk and protective factors associated with suicide reattempts among US residents in substance use treatment centers. Similar to other studies,25-27 our study found that being prescribed medication for psychiatric or emotional problems was associated with a lower risk of suicide reattempt.
Our results were also in agreement with a previous study that found that receiving psychiatric treatment did not appear to reduce the odds of suicide attempts among people with a history of HIV/AIDS problems. 18 However, the size of the cohort with a history of HIV/AIDS problems who attempted suicide in that study was small (2% of 688 participants) and resulted in insufficient statistical power to determine associations. 18 Although we also had a small cohort (n = 90) of people with a history of HIV/AIDS problems who reattempted suicide within 30 days of ASI-MV assessment, we were able to determine in our adjusted models that no significant association existed between having a history of HIV/AIDS problems and a suicide reattempt within 30 days of ASI-MV assessment. Similar to other studies, 28 however, our study found that a history of HIV/AIDS problems was associated with suicide reattempt when our logistic regression model was unadjusted for other known risk factors for suicide reattempt.
One of the strongest risk factors for suicide reattempt in our study was entering treatment for reasons other than a court suggestion. Those who entered a participating substance use treatment facility without a court suggestion were >3 times as likely to have reported a suicide reattempt within 30 days before entering treatment as those who were in treatment because of a court suggestion. The recent suicide reattempt could be a contributing factor for seeking treatment. Increased levels of distress and suicidal ideation and attempts are associated with perceived need for professional help and help-seeking behavior, independent of substance use disorder or other mental health diagnoses. 29 It is also possible that other factors, such as encouragement from others or engagement in a cognitive appraisal process (ie, weighing the pros and cons of treatment), contributed to seeking substance use treatment. 30
Our adjusted models also found other factors associated with increased odds of suicide reattempts, such as age (18-44 years), race and ethnicity (non-Hispanic Black and Hispanic), sex (male), marital status (single), housing (experiencing homelessness), and pain (experiencing a pain problem). In models that included interaction terms with prescribed therapy and abuse, depression, PTSD, or medical interference, we found that experiencing unemployment was associated with reattempts as well. However, other studies did not find sociodemographic characteristics, including age, to be associated with suicide reattempt.8,31-33 A review found weak but nonsignificant associations between suicide reattempts and young adults, single people, and people experiencing unemployment, 32 similar to our significant results. Furthermore, 2 studies reported different associations between sex and suicide reattempts: one noted that the association was stronger among males than among females, 31 similar to our results, but another stated the opposite. 33 Even though the association between pain and suicide attempts is well documented, 34 the association with suicide reattempts is not. 35 Our results demonstrated that people who had a self-reported pain problem were more likely to report suicide reattempts than people who did not have a self-reported pain problem.
Limitations
Our study had at least 7 limitations. First, responses to the self-administered interview questions might have been biased in favor of socially desirable responses selectively recalled because of sensitive questions about suicide attempts, mental health diagnosis and therapy, abuse (physical, sexual, or emotional), and substance use. Second, we could not determine the type of prescribed medication for emotional or psychiatric problems, whether the treatment occurred during childhood or adulthood, adherence to or effectiveness of treatment, whether other psychological or psychiatric treatment was provided, or the frequency of treatment. Third, the measurement for “having problems with HIV/AIDs” in the questionnaire might not reliably measure HIV disease status. Fourth, we were unable to determine the frequency of prior suicide attempts or when the penultimate suicide attempt occurred. Most suicide reattempts or subsequent completed suicides occur within the first 2 years of follow-up, 36 suggesting that people in our analysis will reattempt or die by suicide without treatment. Fifth, we were unable to determine whether adults with a self-reported mental illness diagnosis had been experiencing symptoms while reattempting suicide or if their symptoms and signs were in remission after treatment. The interview did not ascertain when participants had been diagnosed with a mental health problem, only if they had been diagnosed. Sixth, we were unable to measure how long a person had been experiencing pain and whether pain and the most recent suicide attempt occurred during the same period. Lastly, although the analytic sample was large, it was not representative of the US resident population of people assessed for substance use treatment needs during 2014-2020.
Conclusion
Our results can assist clinicians and health care workers, particularly those providing psychiatric and psychological-related services to the approximately 340 000 people assessed for substance use and treatment needs in the NAVIPPRO ASI-MV network during 2014-2020. Our study examined associations between prescribed medication for emotional or psychiatric problems and suicide reattempts. A history of prescribed treatment might indicate a reduced risk for suicide reattempts among people seeking substance use treatment. However, other factors might increase risk, such as voluntarily seeking treatment, younger age, or experiencing homelessness, joblessness, or pain. Clinicians who are prescribing and implementing treatment plans for clients with ≥1 substance use disorder should consider assessing for suicide risk and referring people with recent suicide reattempts to mental health services to reduce possible suicidal ideation and future attempts. Furthermore, clinicians might consider screening for mental illness and suicide risk among patients living with HIV/AIDs and patients who have substance use disorders to decrease the number of suicide reattempts in this population.
Evidence-based strategies and standards address populations with elevated risk for suicidal behavior. In general, these strategies involve placing suicide prevention as a core component of all health care services and enhancing crisis care and care transitions. As outlined by CDC, 37 the National Action Alliance for Suicide Prevention, 38 and the US Department of Health and Human Services, 39 components of suicide prevention efforts include the following: improved clinical training in evidence-based suicide care; better suicide risk identification; enhanced safety planning for those with suicide risk; improved continuity of care in health care systems; increased use of caring contacts in diverse settings; improved local crisis care infrastructure; assurance that individuals at risk are connected to ongoing care; and upstream suicide prevention, focusing on connectedness, problem-solving skills, and economic support.
Longitudinal data are needed to understand how sociodemographic factors, chronic pain experiences, mental illness, and psychiatric treatment affect mental health and substance use treatment and suicide prevention. In addition, research is needed to determine optimal substance use and mental health treatments for those at risk for suicide reattempts.
Footnotes
Acknowledgements
The authors acknowledge the contributions of Akadia Kacha-Ochana, MPH, National Center for Injury Prevention and Control, CDC, and Caitlin Leach, MPH, National Center for HIV, Viral Hepatitis, STD, and TB Prevention, CDC, in acquiring the data. We gratefully acknowledge the editing contributions of Greta Tessman, MA, of the National Center for HIV, Viral Hepatitis, STD, and TB Prevention, CDC.
Authors’ Note
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of CDC.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.