
Abstract
Objectives:
The COVID-19 pandemic has led to severe mental health repercussions. We examined rates of anxiety and depression in the United States during the pandemic by demographic characteristics, individual stressors, and COVID-19 infection rates and policy contexts.
Methods:
We merged data from the April 2020–March 2021 US Household Pulse Survey with state-level data on COVID-19 rates and mitigation policies, including stay-at-home orders, face mask mandates, and restaurant closures. We estimated weighted logistic regression models to assess correlates of anxiety and depression.
Results:
Rates of anxiety and depression peaked in late 2020 at 39% and 32%, respectively. Food insecurity and disrupted medical care were associated with more than twice the odds of anxiety and depression (food insecurity: odds ratio [OR] = 2.58 for anxiety and 2.61 for depression; disrupted medical care: OR = 2.40 and 2.27). Being not employed (OR = 1.32 for anxiety and 1.45 for depression), uninsured (OR = 1.30 and 1.38), housing insecure (OR = 1.41 and 1.34), and experiencing disruptions in education (OR = 1.28 and 1.25) were linked to 25% to 45% increased odds of anxiety and depression. Increases in state COVID-19 infection rates were associated with significantly heightened odds of anxiety and depression (OR = 1.01 for anxiety and depression), but state mitigation policies were not.
Conclusions:
Levels of anxiety and depression rose during the pandemic, particularly among economically vulnerable individuals and those experiencing economic and service disruptions. Future research should assess the effectiveness of policies targeting COVID-19 economic and service disruptions.
COVID-19 has disrupted many facets of life since its emergence in the United States in early 2020. Beyond rising morbidity and mortality, COVID-19 led to widespread business shutdowns and rising rates of unemployment, as well as increases in economic, food, and housing insecurity.1-3 These stressors were particularly elevated among racial and ethnic minority groups, young adults, and less educated adults.3-6 The pandemic also led to widespread disruptions in educational and medical services.7,8 Likely in response to this array of stressors, the levels of psychological stress and mental health symptomatology among people in the United States rose during the COVID-19 pandemic.9-12 For example, recent evidence from the nationally representative Household Pulse Survey found that reports of anxiety and depression rose 4-fold in 2020, particularly among adults of Hispanic, non-Hispanic Black, and non-Hispanic other races and ethnicities, as well as those with less education, young adults, and parents.9,13,14
Yet, limited attention has been paid to how the economic and social stressors driven by the pandemic played a role in rising rates of mental health problems. As hypothesized by social determinants of health and social integration frameworks,15,16 research has found high rates of mental health conditions among economically insecure adults.11,17 Yet, rigorous analysis of the repercussions of rapidly shifting COVID-19–related economic and social stressors are only beginning to emerge.4,18,19 In addition, little attention has been paid to the role of government policies to stem the spread of COVID-19, termed nonpharmaceutical interventions (NPIs), such as stay-at-home orders and business closures, which may have exacerbated social isolation and economic and social stressors, 20 increased feelings of safety and control, 21 and affected mental health.
In this study, we used repeated cross-sectional surveys from 2 085 041 US adults to ask the following questions: How were economic and social stressors associated with mental health problems during the pandemic? Specifically, how were individual stressors and contextual forces derived from COVID-19 rates and NPIs associated with rates of mental health disorders? We hypothesized that anxiety and depression would be elevated among adults experiencing economic stressors and greater potential COVID-19 exposure, although we did not have hypotheses on the role of NPIs.
Methods
Survey Data
We drew survey data from the Household Pulse Survey, which is conducted by the US Census Bureau and partner agencies to provide rapid evidence on the social and economic impacts of COVID-19 on people in the United States. 22 For the Household Pulse Survey, the US Census Bureau conducted online surveys with repeated cross-sectional samples of adults in households in all 50 states and the District of Columbia. We included 2 085 041 respondents surveyed from April 23, 2020, through March 29, 2021 (phases 1-3), clustered into approximately 2-week groupings, which we term cohorts (including all cohorts available when we initiated data analysis). Our analytic sample included 21 cross-sectional cohorts of approximately 100 000 respondents each. We incorporated survey weights to adjust for sampling stratification and nonresponse and to produce estimates representative of the US adult population. 22 The Boston College Institutional Review Board reviewed this study and considered it exempt.
Respondents self-reported symptoms of anxiety and depression using the validated 2-item Generalized Anxiety Disorder Screener 23 (“feeling nervous, anxious, or on edge”; “not being able to stop or control worrying”) and the 2-item Patient Health Questionnaire 24 (“feeling down, depressed, or hopeless”; “having little interest or pleasure in doing things”). The 4 questions were all in reference to the past week and were scored from 0 (not at all) to 3 (nearly every day); scores ≥3 were clinically significant indicators of anxiety disorder and depressive disorder.23-25
Respondents reported individual characteristics, including age, sex, race and ethnicity, family structure, and educational attainment. Respondents also reported economic stressors and stressors in access to services, which we collectively refer to as individual stressors, coded as yes/no indicators. Economic stressors included being not employed (no work for pay or profit in the last 7 days), food insecurity (sometimes or often did not have enough to eat within the last 7 days), and housing insecurity (not current on rent or mortgage payments). Stressors in access to services included no health insurance, disrupted medical care (delayed or did not get medical care that was needed within the last 30 days because of the pandemic), and disrupted education (own, another household member’s, or child/children’s education plans changed, including shutdowns, transitioning to remote, or other changes).
Administrative Data
We assessed time-varying contextual factors, including COVID-19 rates and NPIs at the state level, and linked these variables to individual survey respondents based on state of residence and cohort. To ensure that state COVID-19 rates and NPIs had been experienced just before reports of mental health, we lagged state variables to the previous cohort period, on average 2 weeks prior to the survey for each respondent. We derived COVID-19 state-level case and death rates per 100 000 residents from USAFacts. 26 Because changing rates are highly publicized and hypothesized to be psychologically meaningful, we averaged daily rates during each cohort period and first differenced cohort rates (ie, subtracted t – 2 from t – 1) to identify a change in rates from the prior period. We derived state-level NPIs, specifically statewide stay-at-home/shelter-in-place orders, face mask mandates (requiring face masks in public settings), and restaurant closures (prohibiting indoor dining on the premises), from various databases27-29 and state government websites. We coded NPIs as yes/no variables to indicate whether each respondent was exposed to each policy before the survey. We selected these policies because they served to limit individuals’ personal freedoms and choices in daily activities and they were common NPIs directed toward the broadest swath of the population—in contrast to policies such as school closures, which directly affected only teachers and families with school-aged children, or eviction moratoria, which affected only those at risk of eviction.27,28
Missing Data
The US Census Bureau imputed missing demographic data using hot deck imputation before public release. No data were missing on COVID-19 infection rates, NPI variables, or state or cohort indicators. After data cleaning and bivariate correlations to check for multicollinearity, we imputed missing data on individual stressors, which ranged from 0% to 15%, except disruptions in education, which had 40% of data missing because of changes in survey questions. To do this, we used a bootstrap-based expectation–maximization algorithm (the Amelia II package in R) to impute 30 complete datasets to decrease bias from missing data and retain the nationally representative nature of the weighted sample.
Statistical Analyses
Using Stata version 17 (StataCorp), we estimated a series of logistic regression models predicting indicators of anxiety and depression. Descriptive models included only cohort fixed effects to track changing rates of positive screenings for anxiety and depression. Our main models included state and cohort fixed effects, individual characteristics, individual stressor indicators, and lagged contextual stressors, as follows:

where
After our main models, we estimated numerous additional model specifications to test the robustness of results. First, we estimated models without contextual stressors and then without individual stressors to assess whether the omission of each group altered the functioning of the other. Second, we estimated models including only 1 NPI variable at a time to ensure that the lack of significant associations with mental health outcomes was not driven by multicollinearity. Third, we substituted first-differenced measures of COVID-19 death rates per 100 000 state residents for COVID-19 case rates. Fourth, to ensure that the entry of COVID-19 vaccines did not alter our results, we reestimated models including only cohorts from 2020 (before availability of vaccines).
Results
Descriptive Results
Thirty-six percent of respondents screened positive for anxiety and 29% for depression (Table 1). Bivariate results indicated a higher prevalence of anxiety and depression among respondents who were younger, less educated, female, non-Hispanic Black, Hispanic, non-Hispanic Other, single parents, and experiencing each stressor. Rates of anxiety and depression were similar among respondents experiencing and not experiencing the 3 NPIs. Results from the logistic regression models including only cohort fixed effects found that anxiety and depression varied significantly among cohorts (Figure), rising from April to July, declining into September, and then peaking in November or December 2020 at 39% and 32%, respectively, before declining through March 2021.
Weighted imputed sample characteristics of Household Pulse Survey participants, April 23, 2020–March 29, 2021 (N = 2 085 041) a
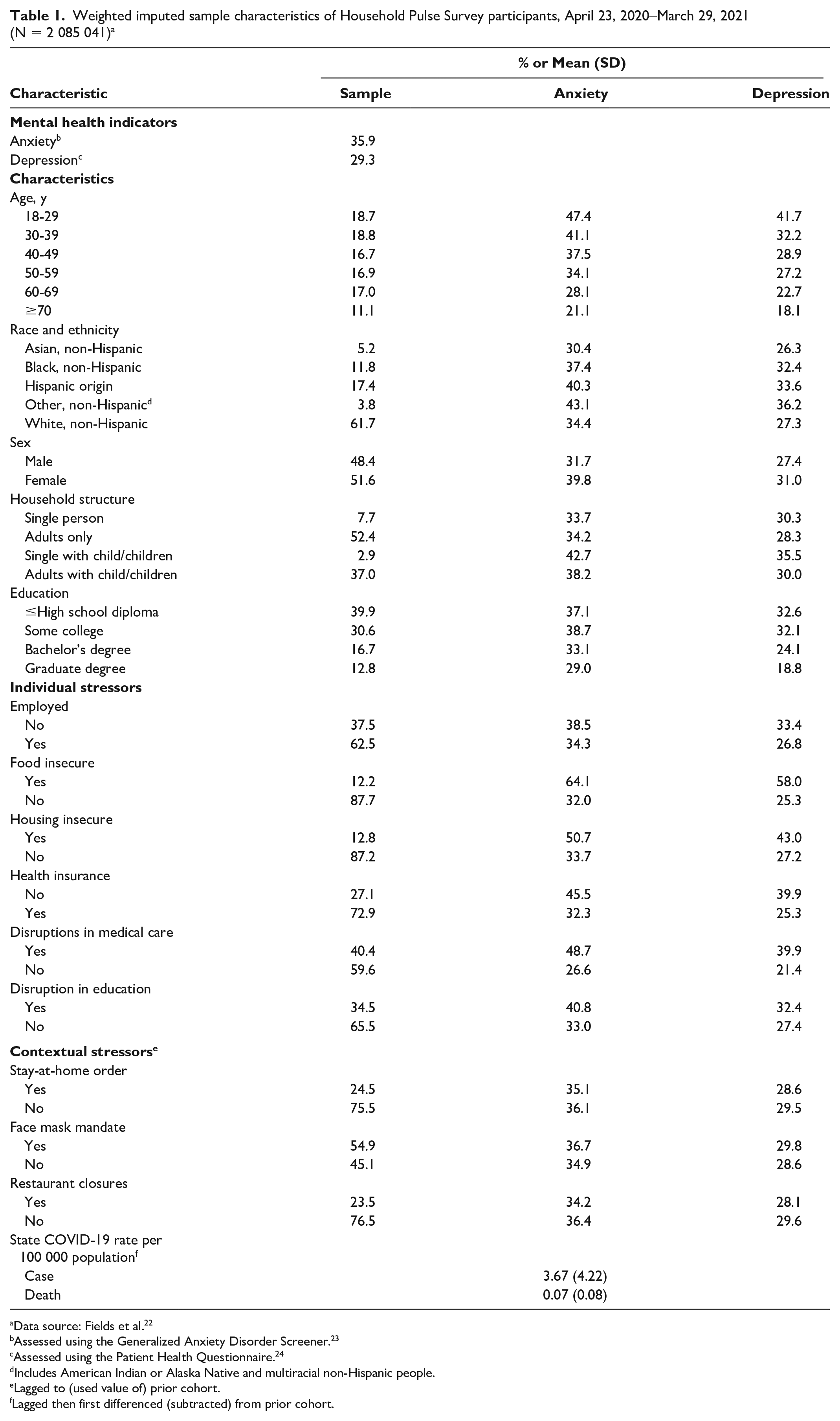
Data source: Fields et al. 22
Assessed using the Generalized Anxiety Disorder Screener. 23
Assessed using the Patient Health Questionnaire. 24
Includes American Indian or Alaska Native and multiracial non-Hispanic people.
Lagged to (used value of) prior cohort.
Lagged then first differenced (subtracted) from prior cohort.
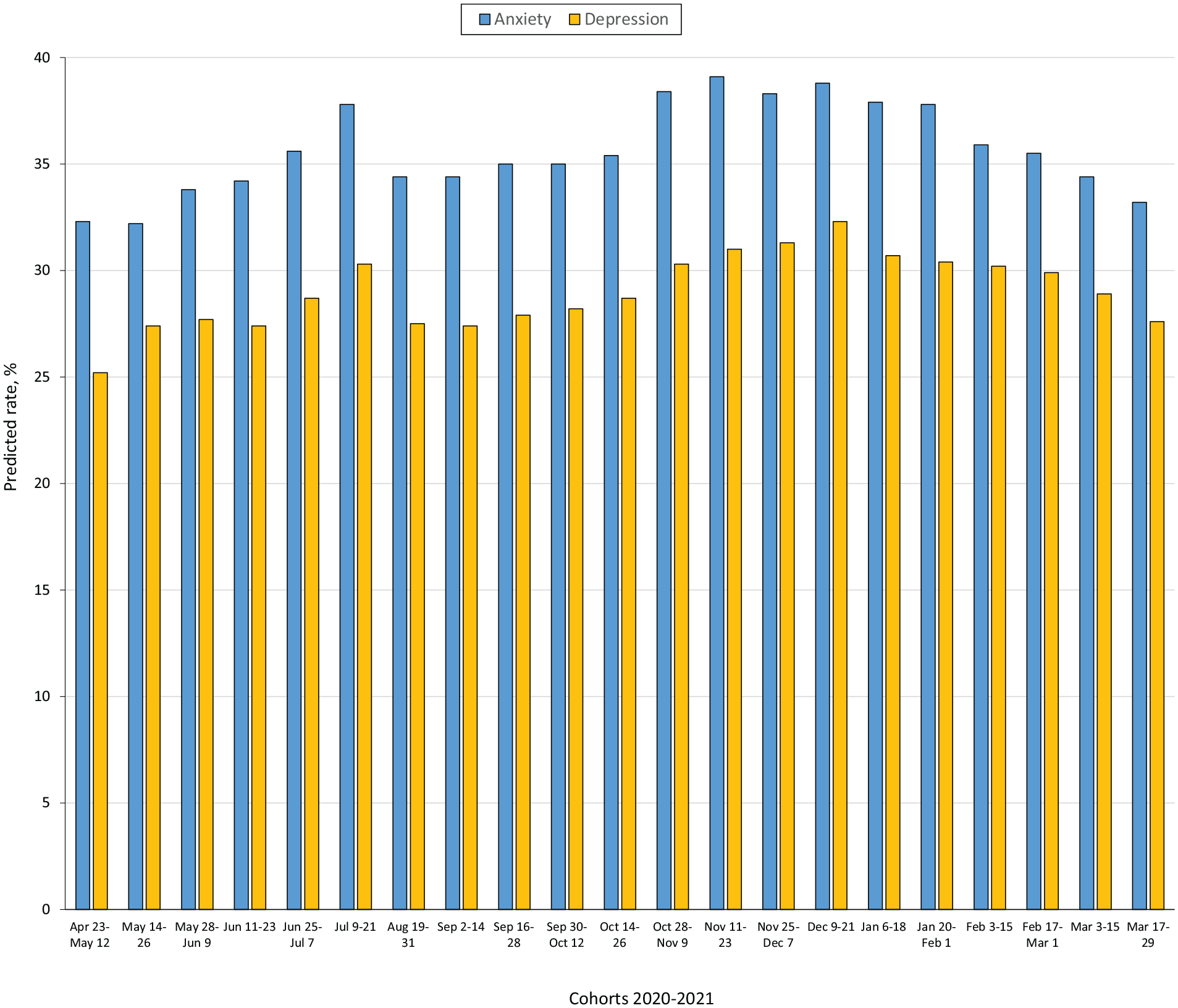
Predicted rates of anxiety and depression, derived from weighted data from Household Pulse Survey participants, April 23, 2020–March 29, 2021 (N = 2 085 041). Data source: Fields et al. 22 No surveys were collected on omitted dates (eg, July 22–August 18; December 22–January 5).
Differences in Levels of Anxiety and Depression by Demographic Characteristics
The likelihood of anxiety and depression was highest among the youngest adults, with 70% lower odds of screening positive for anxiety and 69% lower odds of screening positive for depression among respondents aged ≥70 years versus 18-29 years (Table 2). Odds of anxiety were 18% lower among non-Hispanic Black adults, 28% lower among non-Hispanic Asian adults, 11% lower among Hispanic adults, and 7% higher among non-Hispanic Other adults when compared with non-Hispanic White adults. Depression followed a similar pattern. Women reported 43% higher odds of anxiety and 17% higher odds of depression than men. Having additional people in the household was associated with better mental health: 6% and 18% lower odds of anxiety and depression, respectively, among those living with adults only, 18% and 30% lower odds among single parents, and 27% and 41% lower odds among those living with adults and children, when compared with single adults. Adults with a graduate degree had 12% lower odds of anxiety and 37% lower odds of depression than adults with a high school degree or less.
Weighted logistic regression models predicting anxiety and depression with demographic characteristics, individual stressors, and COVID-19 contextual stressors, using data from Household Pulse Survey participants, April 23, 2020–March 29, 2021 (N = 2 085 041) a
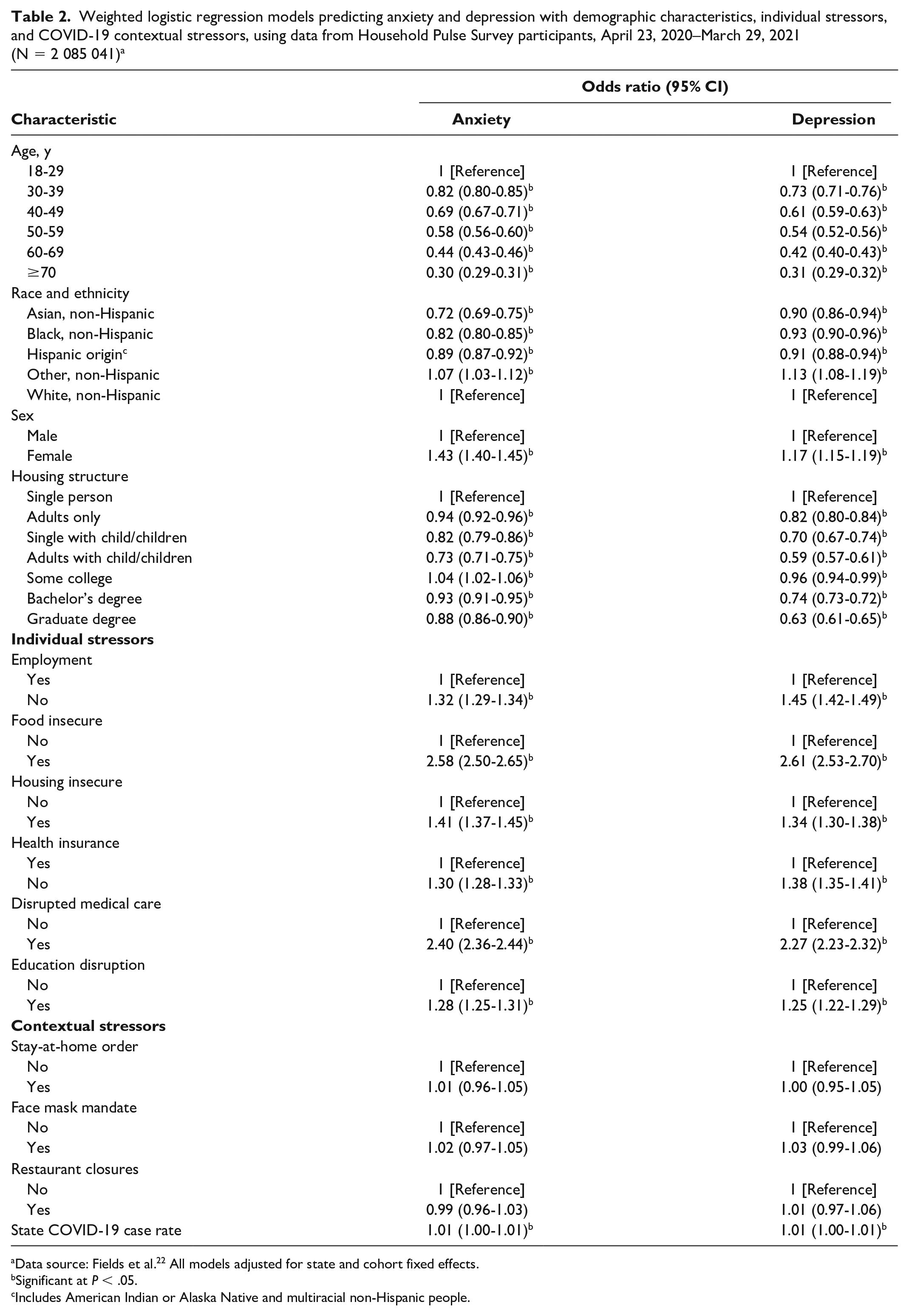
Data source: Fields et al. 22 All models adjusted for state and cohort fixed effects.
Significant at P < .05.
Includes American Indian or Alaska Native and multiracial non-Hispanic people.
Associations With Individual Stressors
Respondents who were not employed reported 32% higher odds of anxiety and 45% higher odds of depression than their employed counterparts (Table 2). Those experiencing food insecurity (vs not) reported 158% higher odds of anxiety and 161% higher odds of depression, while those experiencing housing insecurity (vs not) had 41% higher odds of anxiety and 34% higher odds of depression. Respondents who did not have health insurance (vs had health insurance) reported 30% higher odds of anxiety and 38% higher odds of depression. Having experienced disrupted medical care (vs not) was associated with 140% higher odds of anxiety and 127% higher odds of depression, while experiencing disrupted educational plans (vs not) was linked with 28% higher odds of anxiety and 25% higher odds of depression.
State-Level Contextual Stressors
Increases in COVID-19 case rates were associated with 0.5% increased odds of anxiety and 0.6% increased odds of depression for each additional COVID-19 case per 100 000 state population, translating to a 50% increase in the odds of anxiety and a 60% increase in the odds of depression for each additional case per 1000 residents. In contrast, COVID-19–related NPI policies, including stay-at-home orders, face mask mandates, and restaurant closures, had nonsignificant associations with indicators of anxiety and depression.
Alternate Model Specifications
Results from models excluding contextual stressors and then individual stressors were consistent with results in the full models, again finding no significant associations with NPI policies and similar ORs for COVID-19 rates and individual stressors. Models including only 1 state policy variable again found no significant links between NPIs and anxiety or depression. Models including first-differenced measures of COVID-19 death rates per 100 000 state residents in place of COVID-19 case rates found that coefficients for changing death rates were larger but less precise than those of case rates, with each additional COVID-19 death per 100 000 state residents associated with a significant 28% increase in the odds of depression (OR = 1.28; 95% CI, 1.07-1.54) and a nonsignificant 12% increase in the odds of anxiety (OR = 1.12; 95% CI, 0.95-1.32). Results from models including only cohorts from 2020 also found no substantive changes in results.
Discussion
In our study, we found tremendous growth and variability in positive screenings for anxiety and depression during the COVID-19 pandemic. Expanding prior research that tracked mental health concerns in the first few months of the pandemic,9,10,12,13,30 our results indicate that rates of positive screenings for anxiety and depression rose dramatically into the summer of 2020 before falling markedly in the fall and then peaking during November and December 2020. At this time, 39% of this nationally representative sample of US adults screened positive for anxiety disorder and 32% screened positive for depression, which is >4.5 times higher than rates reported in the nationally representative National Health Interview Survey sample drawn from January to June 2019 using the same measures (which reported rates of 8% for anxiety and 7% for depression). 31
Following prior research, 9,10,12,13,30,32 our results reiterate that certain demographic characteristics, including being female, younger, and less educated and living alone, corresponded to significantly amplified levels of anxiety and depression. These patterns may reflect the heightened stressors faced by adults who are most likely to work in service and forward-facing positions, which experienced the greatest pandemic disruptions, and the isolation faced by individuals living alone during a time of limited out-of-home social interactions. Adjusting for demographic characteristics and individual stressors, non-Hispanic Black and Hispanic adults had significantly lower levels of anxiety and depression than non-Hispanic White adults, suggesting that their elevated levels of mental health challenges, which emerged in bivariate descriptive results, were largely driven by their heightened likelihood of experiencing economic and service stressors.6,33 Non-Hispanic Asian adults also reported lower prevalence rates of anxiety and depression than non-Hispanic White adults, extending prior evidence showing fewer mental health conditions prior to and during the pandemic, as well as lower levels of pandemic stress among Asian American people.33-35
By systematically exploring economic and service access stressors, we found that economic, health, and educational disruptions all helped explain variability in positive anxiety and depression screenings. The most substantial variability was associated with food insecurity and having had to forgo or delay needed medical care because of COVID-19, each of which was associated with a more than doubling of odds of anxiety and depression. Smaller but substantial increases in the risk of anxiety and depression were linked to being not employed, uninsured, and housing insecure and experiencing educational disruptions, each of which was linked with 25% to 45% increased odds of anxiety and depression. The much stronger role of food insecurity versus housing insecurity might reflect the more direct physiologic and psychological stress caused by inadequate access to food, a daily necessity, in comparison with more global stress related to being behind on housing payments. This discrepancy may also have been associated with state and federal eviction and foreclosure moratoria, which afforded protections to many US residents through most of the pandemic,36,37 providing a buffer to the millions of people in the United States who were behind on their rent or mortgage.
A final contribution of this analysis was our assessment of the role of state contexts and policies on mental health. We found a higher prevalence of anxiety and depression among respondents living in states with growing rates of COVID-19 infection. The connection between COVID-19 deaths and depression was far stronger than the link with COVID-19 infection, with each additional death per 100 000 residents associated with 28% increased odds of depression, an effect that might represent fear for one’s personal safety and personal loss or trauma from the loss of loved ones.
In contrast, we found no evidence to suggest that state-level COVID-19 NPI policies limiting personal freedoms and social interactions were associated with anxiety and depression. One hypothesis would argue that such policies—primarily stay-at-home orders and restaurant closures—would inhibit economic activity for some, increase loneliness, and limit social interactions, thereby leading to rising mental health symptomatology. 20 Yet, such policies, as well as face mask mandates, have been shown to limit the spread of COVID-19, 38 and they may have provided a sense that the government was prioritizing public health, increasing respondents’ feelings of safety and security, and supporting mental health, as found in international samples of older adults. 21 The lack of significant connections with anxiety and depression may indicate that both these processes were at play, perhaps canceling each other out. The heightened polarization and politicization of such mandates certainly cannot be ignored, as policies may have different ramifications for psychological well-being depending on political ideology or individual beliefs in the role of government, 21 an issue to address in future research.
Strengths and Limitations
This study had several strengths, including the assessment of a large representative cohort of US adults from April 2020 through March 2021 and the use of validated short screeners of mental health conditions. However, this study also had several limitations. First, we included brief self-reported online surveys, which may have led to an omission of the most disadvantaged segments of the population (eg, those without internet access), underreporting of mental health conditions, and an inability to follow individuals over time. In addition, our analyses assessed correlational relationships between individual stressors and COVID-19–related contexts with individual mental health outcomes, and we could not identify causal effects. The COVID-19 rates and NPI policies also represented state-level factors, missing localized variability that may have been more strongly felt by survey respondents, and did not account for enforcement mechanisms or individual compliance with NPI policies, which may alter how people experience such policies. We did not assess other NPIs that may be relevant for certain populations, such as school closures and eviction moratoria.
Conclusions
Rates of positive screenings for anxiety and depression increased substantially during the COVID-19 pandemic, particularly among adults reporting economic and service disruptions and those living in states with increases in COVID-19 rates. Such information is essential for identifying groups at high risk of anxiety and depression most in need of supportive services and for informing economic and public health policies, which seek to support stability and well-being during the pandemic and beyond.
Results highlight dramatically elevated levels of anxiety and depression, which rose to >4.5 times higher than early 2019 national norms and varied with shifting state-level rates of COVID-19 infections and deaths. In contrast, state-level COVID-19 NPI policies, including stay-at-home orders, business closures, and face mask mandates, were not associated with mental health outcomes. Reflecting a social determinants of health framework, 15 this work identified the demographic, social, and economic characteristics linked to the highest risk of mental health concerns. Consistent with prior research, economically vulnerable individuals (including younger, less educated, and female adults) bore the brunt of heightened rates of anxiety and depression. Enhanced public health initiatives that provide mental health supports should be geared toward these groups.
Our results further highlight the elevated levels of mental health symptoms among adults experiencing economic duress and key life interruptions, including food and housing insecurity, lack of employment and health insurance, and disrupted access to health and educational services. Federal and state policy makers have implemented aggressive policies to address some of these needs, including expanded and extended unemployment benefits, eviction and foreclosure moratoria, and enhanced access to remote educational and health services. Although our results suggest that such policies may have helped to limit the mental health repercussions of the pandemic, research directly assessing policy effectiveness in lowering economic distress and supporting mental health is essential. Beginning in late 2020, COVID-19 vaccines began to be accessible to US residents, and a renewed sense of optimism emerged as case rates declined, COVID-19 restrictions were lifted, and vaccination rates grew. As these public health conditions again shift, it is essential to continue to monitor the mental health consequences of the COVID-19 pandemic and to identify the populations at highest risk of mental health disorders.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from Boston College, Data Analytics for Social Impact, to R.L.C., C.F.B., and S.S.H.