
Abstract
COVID-19 has disproportionately affected American Indian Tribes, including the San Carlos Apache Tribe, which resides on 1.8 million acres in Arizona and has 16 788 official members. High vaccination rates among American Indian/Alaska Native people in the United States have been reported, but information on how individual Tribes achieved these high rates is scarce. We describe the COVID-19 epidemiology and vaccine rollout in the San Carlos Apache Tribe using data extracted from electronic health records from the San Carlos Apache Healthcare Corporation (SCAHC). By mid-December 2020, 19% of the San Carlos Apache population had received a positive reverse transcription polymerase chain reaction test for SARS-CoV-2, the virus that causes COVID-19. The Tribe prioritized for vaccination population groups with the highest risk for severe COVID-19 outcomes (eg, those aged ≥65 years, who had a 46% risk of hospitalization if infected vs 13% overall). SCAHC achieved high early COVID-19 vaccination rates in the San Carlos community relative to the state of Arizona (47.6 vs 25.2 doses per 100 population by February 27, 2021). These vaccination rates reflected several strategies that were implemented to achieve high COVID-19 vaccine access and uptake, including advance planning, departmental vaccine education sessions within SCAHC, radio and Facebook postings featuring Tribal leaders in the Apache language, and pop-up community vaccine clinics. The San Carlos Apache Tribe’s vaccine rollout strategy was an early success story and may provide a model for future vaccination campaigns in other Tribal nations and rural communities in the United States.
COVID-19 has disproportionately affected American Indian Tribes, who often have risk factors for infection and severity, including poverty, multigenerational housing, and a high prevalence of comorbidities.1-4 The San Carlos Apache Tribe resides on 1.8 million acres in Arizona and has 16 788 members on and off the reservation. 5 Despite community mitigation measures, the Tribe experienced a rapid increase in COVID-19 cases in fall 2020.
Prior to the COVID-19 pandemic, American Indian/Alaska Native (AI/AN) populations had low rates of vaccination for diseases such as seasonal influenza, 6 pandemic H1N1 influenza, 7 human papillomavirus, 8 and routine childhood vaccinations 9 as compared with White populations. In contrast, AI/AN people had high overall early COVID-19 vaccination rates when compared with White people in the United States.10,11 This success has been attributed to coordinated action by Tribal governments and the Indian Health Service. 10 Considering AI/AN data in aggregate, however, may obscure differences in the partnerships, policies, and practices used to promote COVID-19 vaccination among Tribes. Additionally, given the high variability in COVID-19 morbidity and mortality according to age and presence or absence of other health conditions, it is important to consider not just raw vaccination rates but also how well vaccinations reached those with the greatest need.
Purpose
To mitigate the impact of COVID-19 in the community, the San Carlos Apache Healthcare Corporation (SCAHC), the Tribe’s Department of Health and Human Services, and the San Carlos Apache Tribal leadership planned an ambitious COVID-19 vaccine rollout. We describe the COVID-19 epidemic and vaccine rollout of the San Carlos Apache Tribe, including vaccine prioritization strategies and efforts to encourage vaccine uptake, supported by analyses of electronic health record data from SCAHC.
Methods
The San Carlos Apache Tribe and SCAHC began implementing culturally adapted COVID-19 vaccine educational efforts in the Apache language and English in November 2020, including radio education, Facebook posts, discussions at Tribal council meetings, and one-on-one conversations with community members. SCAHC received its first doses of the Pfizer-BioNTech vaccine from the Indian Health Service on December 16, 2020, and began administering vaccines the next day. The Moderna vaccine was introduced on January 4, 2021. Initially, COVID-19 vaccines were available only at SCAHC; however, community drive-through events, door-to-door campaigns, and pop-up clinics were added in mid-January 2021 after COVID-19 vaccine supply and vaccination capacity increased. SCAHC administered the vaccine in accordance with the Advisory Committee on Immunization Practices recommendations, 12 with categories informed by infection and hospitalization risks observed in the community as described hereinafter.
We extracted data from the Resource and Patient Management System at SCAHC to describe the Tribe’s COVID-19 epidemiology and vaccine rollout. 13 The intended population for these analyses included members of the San Carlos Apache Tribe and San Carlos community members living on the reservation. To exclude off-reservation non-Indian SCAHC employees and Tribal members outside the SCAHC catchment area, we limited the data to people with ≥1 visit at SCAHC in the past 3 years and not classified by the Resource and Patient Management System as “Caucasian” or “non-Indian or non–federally recognized Indian,” unless listed as “non-Indian members of Indian households” (N = 16 178). SCAHC was the only health facility offering SARS-CoV-2 reverse transcription polymerase chain reaction (RT-PCR) testing and COVID-19 vaccination on the reservation. SARS-CoV-2 infection was defined as a positive RT-PCR test result. Use of antigen testing was confined to limited community screening programs, and positive test results among Tribal or community members were confirmed by RT-PCR at SCAHC. SARS-CoV-2 infections and hospitalizations were calculated among groups stratified by age and the presence or absence of comorbidities. We defined “hospitalization” as “hospital admission or transfer from the emergency department” for COVID-19 or respiratory symptoms 3 days prior to 30 days after the specimen collection date for the first positive test result. We considered people with comorbidities to be those with any of the following system diagnosis tags (generated automatically by visit history and laboratory values): hypertension, obesity, diabetes, chronic obstructive pulmonary disease, chronic kidney disease, end-stage renal disease, cardiovascular disease, or asthma. We also calculated COVID-19 vaccination coverage over time and within categories of age and the presence or absence of comorbidities. We then compared population-adjusted SARS-CoV-2 infection rates and COVID-19 vaccination rates over time with publicly available data from the state of Arizona, 14 shown as infection rates per 100 000 people and cumulative vaccine doses administered per 100 people.
The San Carlos Tribal Council approved these analyses, and the project was reviewed by CDC and conducted consistent with applicable federal law and CDC policy—see, for example, 45 CFR part 46.102(l)(2), 21 CFR part 56, 42 USC §241(d), 5 USC §552a, and 44 USC §3501 et seq.
Outcomes
By December 12, 2020, the San Carlos Apache Tribe demonstrated cumulative per capita infection rates 3.4 times higher than overall rates in Arizona (3054 of 15 973 [19.1%] of San Carlos Apache Tribe members vs 402 589 of 7 189 020 [5.6%] in Arizona). The Tribe’s infection rate peaked in late November 2020. Infection rates in the community continued to fall after the introduction of COVID-19 vaccines in mid-December (369 cases occurred in the first 2 full weeks of December 2020 vs 10 in the first 2 full weeks of February 2021, a 97% decrease; Figure A). Overall infection rates in Arizona had also fallen by February 2021, but the decline was not as steep (89 331 cases occurred in the first 2 full weeks of December 2020 vs 27 065 cases in the first 2 full weeks of February 2021, a 70% decrease).
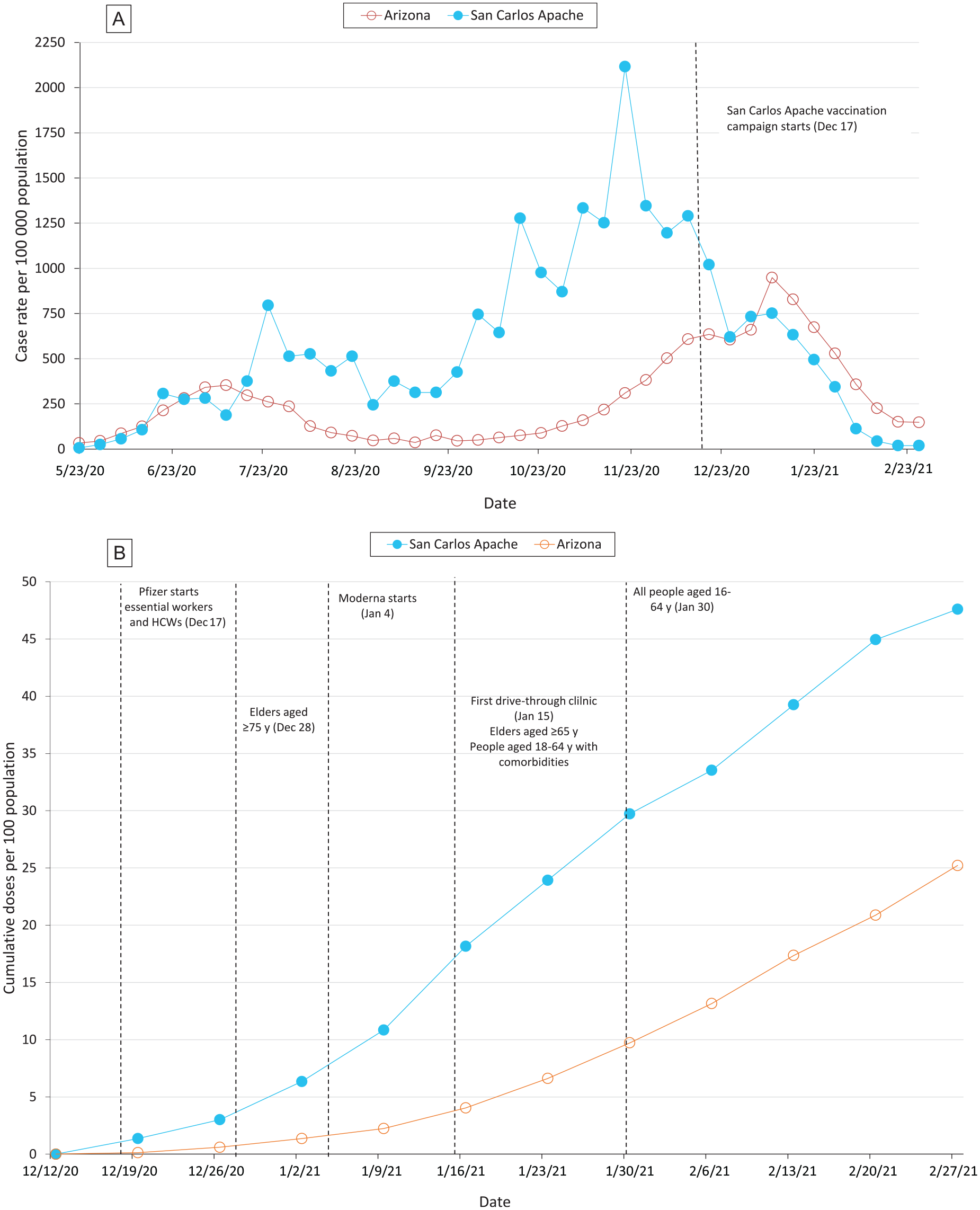
Comparison of (A) San Carlos Apache Tribe and Arizona COVID-19 epidemiologic curve from May 1, 2020, through February 27, 2021, and (B) COVID-19 vaccination coverage from December 12, 2020, through February 27, 2021. (A) New SARS-CoV-2 infections per 100 000 population diagnosed at the San Carlos Apache Healthcare Corporation (SCAHC) as compared with the state of Arizona per week, beginning May 23, 2020. Arizona cases reported from December 21-28, 2020, were averaged across all dates in that range because of inconsistent reporting. (B) Cumulative rate of weekly vaccine doses given per 100 population by SCAHC as compared with the state of Arizona, beginning December 2020. The population denominator includes the whole population, not just those eligible for the vaccine. Abbreviation: HCW, health care worker. Data sources: SCAHC and Arizona Department of Health Services COVID-19 data dashboard.
The risk of SARS-CoV-2 infection among the San Carlos Apache Tribe was similar across strata of age and presence of comorbidities, but the risk of hospitalization after infection was highest among those aged ≥75 years (38 of 71; 54%), 65-74 years (89 of 208; 43%), and 18-64 years with comorbidities (310 of 1746; 18%) as compared with 84 of 786 (11%) among healthy adults aged <65 years (Table). More than half of the adult San Carlos Apache population (6498 of 10 697; 61%) was in one of these high-risk categories. SCAHC sequentially prioritized COVID-19 vaccinations to health care and essential workers and people aged ≥75 years, 65-74 years, 18-64 years with comorbidities, and 16-64 years. As soon as 50% coverage was reached in one prioritization category, SCAHC made vaccines available to the next group while continuing outreach to higher-risk groups. As of February 9, 2021, 66% (726 of 1106) of people aged ≥65 years had received ≥1 dose of a COVID-19 vaccine, as opposed to 23% (949 of 4083) of adults aged <65 years with no comorbidities.
Risk of SARS-CoV-2 infection, COVID-19 hospitalization, and vaccine coverage by COVID-19 vaccine prioritization group among San Carlos Apache Tribe community members, Arizona, May 1, 2020–February 9, 2021
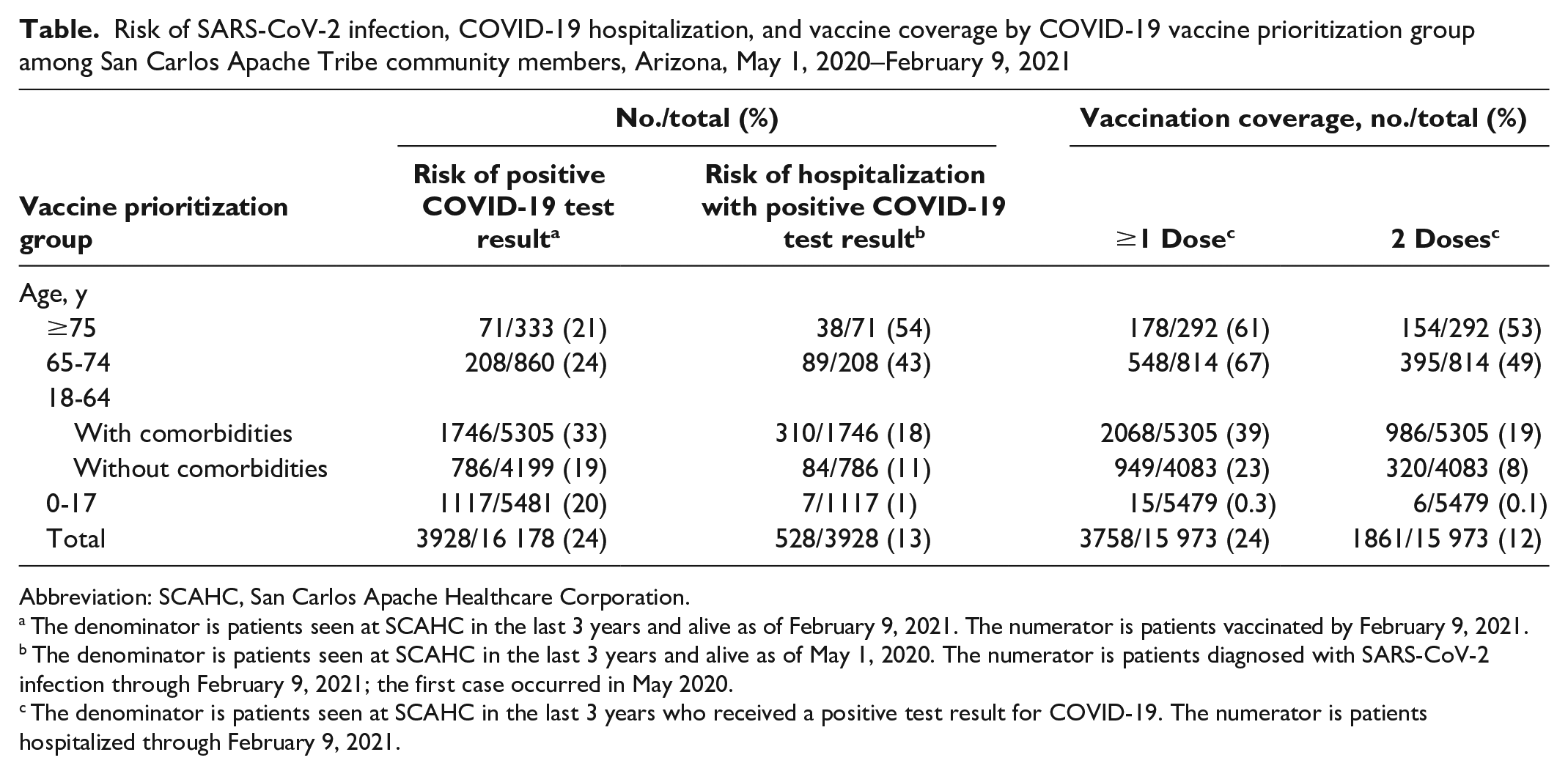
Abbreviation: SCAHC, San Carlos Apache Healthcare Corporation.
The denominator is patients seen at SCAHC in the last 3 years and alive as of February 9, 2021. The numerator is patients vaccinated by February 9, 2021.
The denominator is patients seen at SCAHC in the last 3 years and alive as of May 1, 2020. The numerator is patients diagnosed with SARS-CoV-2 infection through February 9, 2021; the first case occurred in May 2020.
The denominator is patients seen at SCAHC in the last 3 years who received a positive test result for COVID-19. The numerator is patients hospitalized through February 9, 2021.
Following the Tribe’s efforts to provide widespread education and access to the COVID-19 vaccine, per capita vaccine distribution was consistently higher in the San Carlos Apache Tribe than in Arizona (Figure B). By February 27, 2021, 4329 of 15 973 San Carlos Apache Tribe community members had received ≥1 dose of a COVID-19 vaccine, and 3273 had received 2 doses. In total, 47.6 doses per 100 people (7602 of 15 973) were administered to the San Carlos Apache Tribe through February 27, 2021, versus 25.2 doses per 100 people (1 812 565 of 7 189 020) in Arizona for the same period.
Lessons Learned
The San Carlos Apache Tribe implemented an aggressive COVID-19 vaccine rollout beginning in December 2020 to combat the high incidence of COVID-19 in its community, resulting in high COVID-19 vaccination rates relative to the state of Arizona. Several lessons were learned from this approach.
Advance Planning Supports Smoother Vaccine Rollout
The San Carlos Apache Tribe and SCAHC, in collaboration with the Indian Health Service, began planning for the vaccine rollout several months before any vaccine was approved. Key steps taken before vaccinations began included acquiring an ultra-cold freezer to store vaccines; developing a playbook for vaccine administration and a tiered approach based on Advisory Committee on Immunization Practices guidelines; identifying people in the high-priority vaccine groups; creating call lists for direct outreach; and communicating to the public information about COVID-19 signs and symptoms, risk factors, and, ultimately, vaccination. Careful planning allowed SCAHC to begin vaccinations the day after the first doses were received and allowed staff to focus their energy on operational issues that could not be anticipated in advance.
Community Education Improves Vaccine Uptake
Community educational efforts began 6 weeks prior to COVID-19 vaccine introduction and continued throughout the vaccine rollout, with the goal of addressing vaccine hesitancy. These efforts included showcasing Tribal leaders who received their COVID-19 vaccine via live video postings on Facebook, publishing frequently asked questions about COVID-19 vaccines, and providing education via radio in the Apache and English languages. Community members were also encouraged to share their personal stories and reasons for COVID-19 vaccination within their circles of influence. To understand the effectiveness of these approaches, the Tribe’s Department of Health and Human Services surveyed people receiving COVID-19 vaccines on January 15, 2021; most reported that they had heard about the vaccines via Facebook (45 of 133; 34%), the radio (44 of 133; 33%), and/or friends and family (49 of 132; 37%). SCAHC contacted all Tribal members believed to be at high risk based on their medical record history to ensure that no one missed an opportunity to hear about the vaccine. SCAHC also held internal staff educational sessions and routinely discussed vaccine recommendations at every Tribal council meeting to encourage consistency in the vaccine messages to the community. These outreach initiatives to improve the community’s understanding may have enabled optimal vaccine uptake.
Improving Access to Ensure Increased Vaccination
Originally, SCAHC offered only on-site vaccinations. Over time, drive-through vaccination events, pop-up vaccination events, and door-to-door vaccinations were added to ensure that all community members had access to the vaccine. Mass drive-through clinics had the biggest impact early in the vaccination campaign, with 512 people receiving the vaccine at a single drive-through event. By the end of March 2021, however, demand for the vaccine began to wane, and these events were no longer as effective. Community vaccination events were booths set up at swap meets, job fairs, education fairs, and other community events and would typically reach 15 to 20 doses in a single day. Door-to-door vaccinations were the most labor-intensive events, requiring teams of 4 or 5 people and generally reaching <10 people per day. However, door-to-door campaigns may still have a role in reaching people who would not leave their homes for other vaccine events. The biggest challenge to these types of events was the number of staff needed. Cross-training of staff and federal staff support from the Federal Emergency Management Agency made such an intensive effort feasible.
Comparisons With Other Literature
The San Carlos Apache Tribe’s COVID-19 vaccine rollout had similar features to successful mass vaccination campaigns for diseases in other settings, including a wide recognition of the negative impact of the disease in the community, the direct involvement of community members and leadership in the campaign, publicized social norms of acceptance, and ease of access to vaccination.15,16 The use of a combination of culturally adapted interventions also aligns with recognized best practices. 15 In particular, several aspects of this vaccine rollout were similar to those implemented by the Whiteriver Service Unit on the White Mountain Apache Tribe Reservation during the 2002-2003 influenza season. Similarities between these campaigns included their efforts to encourage health care worker vaccination, sharing of vaccine information on radio stations in English and the Apache language, and providing vaccinations at home visits and sites in the community. Differences included the phased aspect of the COVID-19 vaccine rollout, the setting of a global pandemic with widespread vaccine misinformation, and the San Carlos Apache Tribe’s use of social media and telephone calls to people at high risk of severe outcomes to encourage COVID-19 vaccination. 17
Community-based approaches to encouraging vaccine uptake may be especially important for groups with mistrust of the medical community stemming from historical or recent experiences, including American Indian Tribes.18,19 Although many of the efforts described here were labor intensive (including one-on-one telephone calls of people in high-priority vaccine groups, pop-up vaccination booths at community events, and door-to-door events), they allowed SCAHC to reach people who may have been overlooked by traditional vaccination campaigns. Similar strategies could be adapted by other communities when more efficient options (eg, mass media, large drive-in vaccine events) are insufficient, particularly when attempting to reach members of racial and ethnic minority and/or socioeconomically disadvantaged groups who may not have a telephone, lack the means for transportation to attend vaccination events, have minimal or no access to event information, and/or lack a stable housing situation.
Limitations of the Initial Vaccine Rollout and Next Steps
The initial vaccine rollout had some limitations. First, although advance planning was useful, the rollout plan required continuous and real-time adjustments to overcome challenges that arose (eg, staffing shortages, surges to the vaccine clinic, inconsistent VPN [virtual private network] wireless connection in the field for pop-up events). Second, engagement of religious leaders was limited during the early rollout. Earlier attempts to leverage their influence may have reduced vaccine hesitancy, limited vaccine misinformation from social media, and minimized political disagreements about the pandemic and the role of vaccines. Third, early in the vaccine rollout, COVID-19 vaccine educational materials had to be created by SCAHC, because they were not readily available in the Apache language or written for an American Indian population. This effort was time intensive and delayed the communications rollout. Finally, the SCAHC electronic health system facilitated identification of and outreach to large groups of people at risk, but this approach failed to reach people who had not accessed health care services in the past 3 years or whose contact information was not up-to-date.
Next steps include updating the current patient database and acquiring an electronic health record system that allows more robust data analytics. Vaccine efforts have continued since the analyses described in this article, with some strategies shifting as younger children and adolescents became eligible. As of March 2022, efforts included vaccine pop-up clinics at community events and school sports (up to 10 to 15 events per month), clinics at local elementary and high schools on and off the reservation, weekly visits to offer vaccines at the Tribal detention center, and home visits to people otherwise unable to access the vaccine.
Limitations of the Analysis
Our analyses had several limitations. First, all analyses used observational data from electronic health records, which may not have precisely reflected the intended population. Second, the definition of comorbidities may not have captured all people at risk. The hospitalization definition may have also captured some people with exacerbations to chronic respiratory conditions not directly caused by COVID-19, or it may have missed some patients who had COVID-19 with nonrespiratory symptoms. Third, all analyses combined data for the Pfizer-BioNTech and Moderna vaccines. Fourth, we did not compare COVID-19 vaccination rates based on first versus second dose for the San Carlos Apache Tribe and Arizona because these data were not reported for Arizona. Finally, although the steep decline in Tribal infection rates occurred during a similar time frame to the rapid vaccine rollout, the decline cannot be attributed to vaccination alone. Other mitigation efforts were in place to reduce infection rates—namely, shelter-in-place restrictions, Tribal curfews, and concerted contact tracing efforts leading to quarantine and/or isolation instructions. State and nationwide trends also reflected a declining number of cases around this time.
Data demonstrate the early success of the San Carlos Apache Tribe’s COVID-19 vaccination campaign. Increasing COVID-19 vaccination coverage and declining rates of new SARS-CoV-2 infections in December 2020–February 2021 allowed easing of some community mitigation strategies. Even as COVID-19 vaccinations have accelerated across the United States, disparities in access persist for certain groups, such as people living in rural communities. 20 The San Carlos Apache Tribe’s community-driven approach to vaccine education, logistics, and prioritization may provide a model for current and future vaccination campaigns in communities disproportionately affected by COVID-19 or other vaccine-preventable diseases.
Footnotes
Acknowledgements
The authors acknowledge the San Carlos Apache Tribal Council for its leadership and advocacy for COVID-19 vaccinations throughout the community; the San Carlos Apache Tribal Emergency Response Committee for its expertise in emergency management and being a liaison among the community entities; San Carlos Apache Healthcare Corporation Board of Directors for its leadership, engagement, and support of the San Carlos Apache Healthcare Corporation vaccine distribution efforts; and the Public Health Nursing Department of the San Carlos Apache Tribe Department of Health and Human Services and Aaron Tohtsoni for their efforts to conduct the vaccine hesitancy survey and follow-up.
Disclaimer
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.