
Abstract
Limited studies are available on how decisions and perceptions on SARS-CoV-2 vaccination have changed since the start of vaccination availability. We performed a qualitative study to identify factors critical to SARS-CoV-2 vaccination decision making and how perspectives evolved among African American/Black, Native American, and Hispanic communities disproportionately affected by COVID-19 and social and economic disadvantage. We conducted 16 virtual meetings, with 232 participants in wave 1 meetings (December 2020) and with 206 returning participants in wave 2 meetings (January and February 2021). Wave 1 vaccine concerns in all communities included information needs, vaccine safety, and speed of vaccine development. Lack of trust in government and the pharmaceutical industry was influential, particularly among African American/Black and Native American participants. Participants showed more willingness to get vaccinated at wave 2 than at wave 1, indicating that many of their information needs had been addressed. Hesitancy remained greater among African American/Black and Native American participants than among Hispanic participants. Participants in all groups indicated that conversations tailored to their community and with those most trustworthy to them would be helpful. To overcome vaccine hesitancy, we propose a model of fully considered SARS-CoV-2 vaccine decision making, whereby public health departments supply information, align with community values and recognize lived experiences, offer support for decision making, and make vaccination easy and convenient.
Keywords
People from racial and ethnic minority groups have experienced increased infection, hospitalization, and mortality from COVID-19.1 -5 High vaccine coverage against SARS-CoV-2 is critical to control COVID-19. Surveys conducted before6 -10 and after 11 authorization of SARS-CoV-2 vaccines from the US Food and Drug Administration noted considerable hesitancy, particularly among non-Hispanic African American/Black participants.10,11 Survey results are limited in explaining reasons for vaccine hesitancy. In addition, although repeated surveys can measure how point estimates of intent or the frequency of specific concerns change, information gained from surveys generally do not explain why these changes occur.
In this qualitative study, we aimed to identify concerns about SARS-CoV-2 vaccines and factors critical to vaccination decision making, as well as how perspectives evolved among African American/Black, Native American, and Hispanic communities from shortly before the availability of SARS-CoV-2 vaccines through when >20 million vaccinations had been administered in the United States. We use the term vulnerable to describe communities in which COVID-19 has had disproportionate health burden, which has been associated with social and economic disadvantage and racial and ethnic minority populations affected by structural racism.12,13 This investigation addresses the need for a deeper understanding of factors associated with vaccination intent and decision making and describes a model for authentic community engagement and support for decision making.
Methods
We identified a convenience sample of
African American/Black people in Baltimore, Maryland; New Orleans, Louisiana; and Howard County, Maryland
Hispanic people in Fairfax County, Virginia; Harris County, Texas; Glenwood Springs/Garfield County, Colorado; and Howard County, Maryland
Native American people—1 tribe each from the Great Plains and the Northern Plains
Collaborators in each community recruited meeting participants using snowball sampling, engagement with community and faith-based organizations, and local advertisements. All participants received compensation for their time participating. Selection was independent of prior COVID-19 infection or vaccination intent. The Johns Hopkins University Bloomberg School of Public Health Committee on Human Research determined that this work was public health surveillance and not human subjects research with identifiable information and, thus, waived formal review.
Each group participated in 2 virtual 90- to 180-minute conversations. We conducted wave 1 conversations December 1-15, 2020, and wave 2 conversations January 26–February 15, 2021. A trained facilitator who was of similar race and ethnicity as participants led the conversations. The same people were invited to participate in both waves. Conversations with Hispanic groups were held in Spanish. Facilitators followed a written discussion guide adapted for their community. At each session, facilitators reminded participants that conversations were not about persuading them to get vaccinated but to understand their decision making and changes over time.
Wave 1 conversations focused on participants’ pandemic experiences, perception of vaccination benefits and concerns, logistical barriers, and vaccination intent. Wave 2 conversations explored concerns from wave 1, whether perceptions and experiences had changed, the importance for decision making, sources of information about SARS-CoV-2 vaccines, and vaccination intent. At several points during each meeting, facilitators used the polling feature of the virtual platform to collect information from participants who chose to respond. This information provided the sense of the group and was used to focus further discussion.
Up to 4 public health and academic team members took extensive notes during each conversation and characterized themes. Those team members also reviewed recordings of the sessions to confirm accuracy of expressed themes. Given our focus on rapidly sharing findings with community leaders and public health agencies, we did not transcribe sessions and, therefore, cannot provide direct quotes in this article. Spanish-language meetings were translated in real time for note takers listening in English.
Results
Wave 1 conversations included 232 participants, and wave 2 conversations included 206 participants (88.8% retention). All participants at the 16 meetings in each wave were from the racial and ethnic groups of interest. Of the participants, 135 of 197 (69%) who provided their demographic information were women, and ages ranged from 18 to ≥60 years (Table). Of 208 participants who reported previous COVID-19 experience, 65% (n = 135) indicated that they or a family member had been diagnosed with COVID-19.
Characteristics of participants from African American/Black, Native American, and Hispanic communities who participated in 2 conversations on SARS-CoV-2 vaccination, United States, December 2020 and January–February 2021 a
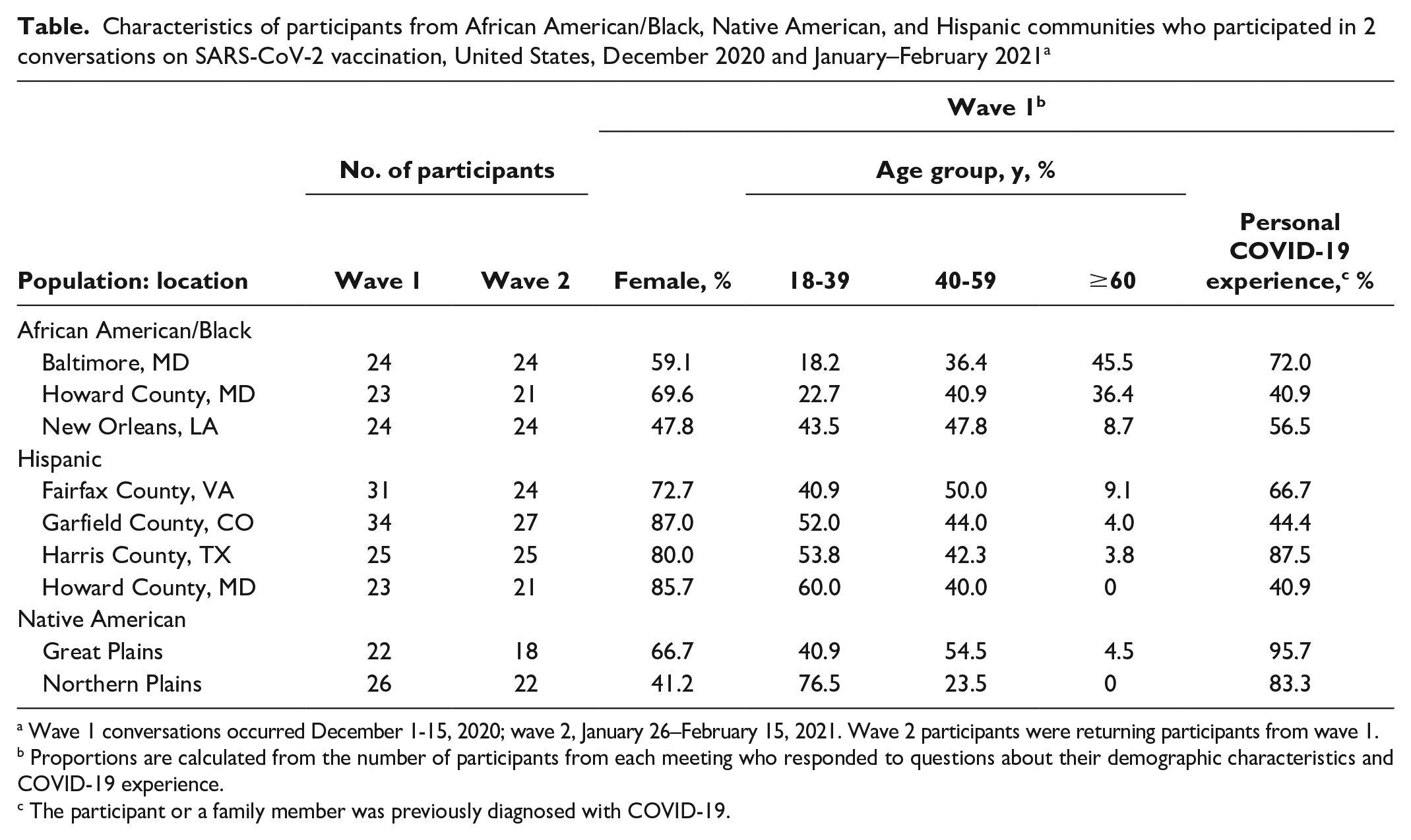
Wave 1 conversations occurred December 1-15, 2020; wave 2, January 26–February 15, 2021. Wave 2 participants were returning participants from wave 1.
Proportions are calculated from the number of participants from each meeting who responded to questions about their demographic characteristics and COVID-19 experience.
The participant or a family member was previously diagnosed with COVID-19.
Many wave 1 participants identified health experiences and pandemic challenges of job loss and difficulty paying rent or affording food. When asked why they might get vaccinated, in addition to protecting health and mitigating economic effects, Hispanic participants more commonly than other groups mentioned getting vaccinated to benefit others in their community. When polled, 72 of 88 Hispanic participants (82%) indicated that they felt a responsibility to get vaccinated to protect their community and “were happy to do their part,” as compared with 31 of 66 African American/Black participants (47%) and 16 of 38 Native American participants (42%).
Concerns included the need for more information about the vaccines and vaccine safety, the speed of vaccine development, and a lack of trust in government and the pharmaceutical industry. A sentiment expressed by many Native American participants was wanting data on vaccine efficacy and safety specific to people who are Native American. When asked by the facilitator, participants in each population group expressed the belief that researchers and pharmaceutical companies experiment on people like them. Participants also mentioned concerns such as a lack of trust in the health care system and public health, systemic racism in health care, and the racialized politics of the Trump administration. Several African American/Black participants indicated that the push for vaccination seemed self-serving given the long-standing health care inequities affecting their community that had not elicited the same concern. The most common logistical concerns were the hours and locations of vaccination clinics. When compared with African American/Black and Native American participants, Hispanic participants more commonly expressed concerns about the need to share personal information to be vaccinated.
By wave 2, among African American/Black, Hispanic, and Native American participants who were vaccine eligible, 65%, 64%, and 47%, respectively, had received ≥1 dose. Among those not yet vaccinated, in each population, the proportion who indicated intent to definitely/probably be vaccinated had increased since wave 1. Many whose attitudes shifted from wave 1 to wave 2, particularly Hispanic participants, indicated that their most important information needs had been met.
The speed of vaccine development was considered a less important issue by wave 2. Among vaccine safety issues, participants in each group often indicated that possible long-term side effects would make them less likely to be vaccinated, while few indicated concerns with short-term reactions. Some Native American participants tied their concerns to the intergenerational well-being of their tribe, describing how the potential loss of an elder or effects on fertility would add to the loss of people, culture, and language.
Many participants stated that they needed more than information to make a vaccination decision, indicating the value of conversations with those most trustworthy to them. Consistent with distrust of government and the pharmaceutical industry, Native American and African American/Black participants were less likely than Hispanic participants to seek information from a physician or public health expert and more likely than Hispanic participants to seek information from other health professionals, community or faith leaders, and friends or family. Participants from all communities were interested in more conversations in their community led by people they know and trust. Logistical concerns were less prominent during wave 2 than in wave 1. The need to provide personal information for vaccination continued to be a larger issue for Hispanic and Native American participants than for African American/Black participants.
Discussion
As SARS-CoV-2 vaccinations have increased, it has been easy to lose sight of the hesitancy that remains, particularly among vulnerable communities. Understanding the reasons for vaccine hesitancy and developing approaches to support decision making are crucial for public health.
More participants in wave 1 than wave 2 had a wait-and-see attitude or a probable or definite intent to not get vaccinated in all participating communities. Shifting attitudes likely resulted from the severity and longevity of the pandemic, the high levels of efficacy documented in clinical trials of the vaccines authorized by the US Food and Drug Administration,14,15 additional experience derived from the millions of people who were vaccinated, and the desire to “return to normal.” For some participants, vaccine safety concerns remained but did not determine whether they received or intended to receive the SARS-CoV-2 vaccine.
Although additional information and experience with SARS-CoV-2 vaccines will be sufficient for some to support a decision to be vaccinated, for others, distrust in government and the pharmaceutical industry continues to underlie hesitancy, particularly among African American/Black and Native American communities, which have experienced historical trauma and ongoing racism.16 -23 The current interest by public health departments in achieving equity in SARS-CoV-2 vaccination is viewed by some participants as inauthentic in the context of unaddressed inequities in health and health care. Distrust of the health care system also has implications for the sources that people turn to for information. Medical providers are often cited as the best source of information on vaccinations; however, information from elders in Native American communities and from faith leaders in African American/Black communities may have a greater influence than that from medical providers. 24 Word of mouth on the vaccination experience of family and others in their community may also be influential. 25
Our study had several limitations. First, participants were not selected randomly and numbers are relatively small; thus, participants likely do not completely reflect the racial or ethnic group in their communities or the diversity of each population. Second, we analyzed qualitative information by characterizing key themes rather than transcribing each meeting, identifying keywords, and providing illustrative quotes.
While public health practitioners often speak of “informed decision making,” factors beyond information contribute to people’s decisions about vaccination. We propose that public health practitioners focus instead on fully considered SARS-CoV-2 vaccine decision making (Figure). This approach has 4 components. One component is providing information that people describe as influential for them. Another component is recognizing the effects of people’s values and lived experience on decisions. For African American/Black and Native American communities, this component would include acknowledging limited trust and engaging with communities to address the underlying causes that engender mistrust in health care and government. Attempts to persuade people to get vaccinated will likely be less effective than engagement and dialogue. A third component is providing support for decision making, including the public as contributors and not just targets for persuasion. Rather than pursuing a transactional approach, where counting vaccinations is the measure of success, public health departments should pursue a relational approach, where success derives in part from bridges built with the community and trustworthiness demonstrated over time. The final component is making vaccination easy. Although decision making and implementation often are considered separately, decisions are influenced by how hard it is to act. Making vaccinations easily accessible, using culturally appropriate communications, limiting what personal information is collected, and explaining why personal information is needed will contribute to vaccination decisions.
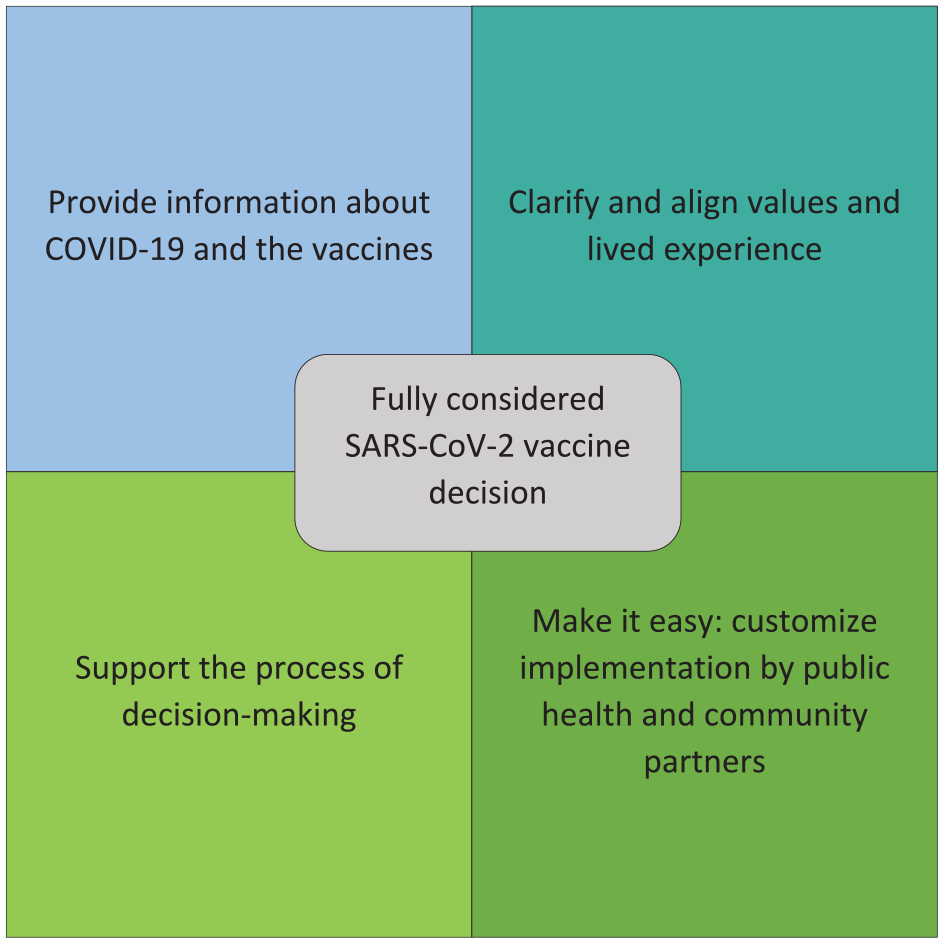
Suggested framework for public health departments to engage with communities and more effectively address the full range of needs leading to a decision on SARS-CoV-2 vaccination.
Effective and ongoing engagement with vulnerable communities can help overcome barriers to SARS-CoV-2 vaccination and achieve other public health priorities. Given the interest and pandemic-associated resources available for public health, opportunities exist to build more effective ways of partnering with and meaningfully engaging vulnerable communities that can reduce disparities and positively affect attitudes and behaviors.
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Daniel A. Salmon has received research support from Merck and serves on advisory boards for Merck and Janssen. Matthew Z. Dudley has received research support from Merck.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant funding for this work came from the Robert Wood Johnson Foundation and the Horizon Foundation.